


Dead Bodybuilders Speaking from the Heart: An Analysis of Autopsy Reports of Bodybuilders That Died Prematurely
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
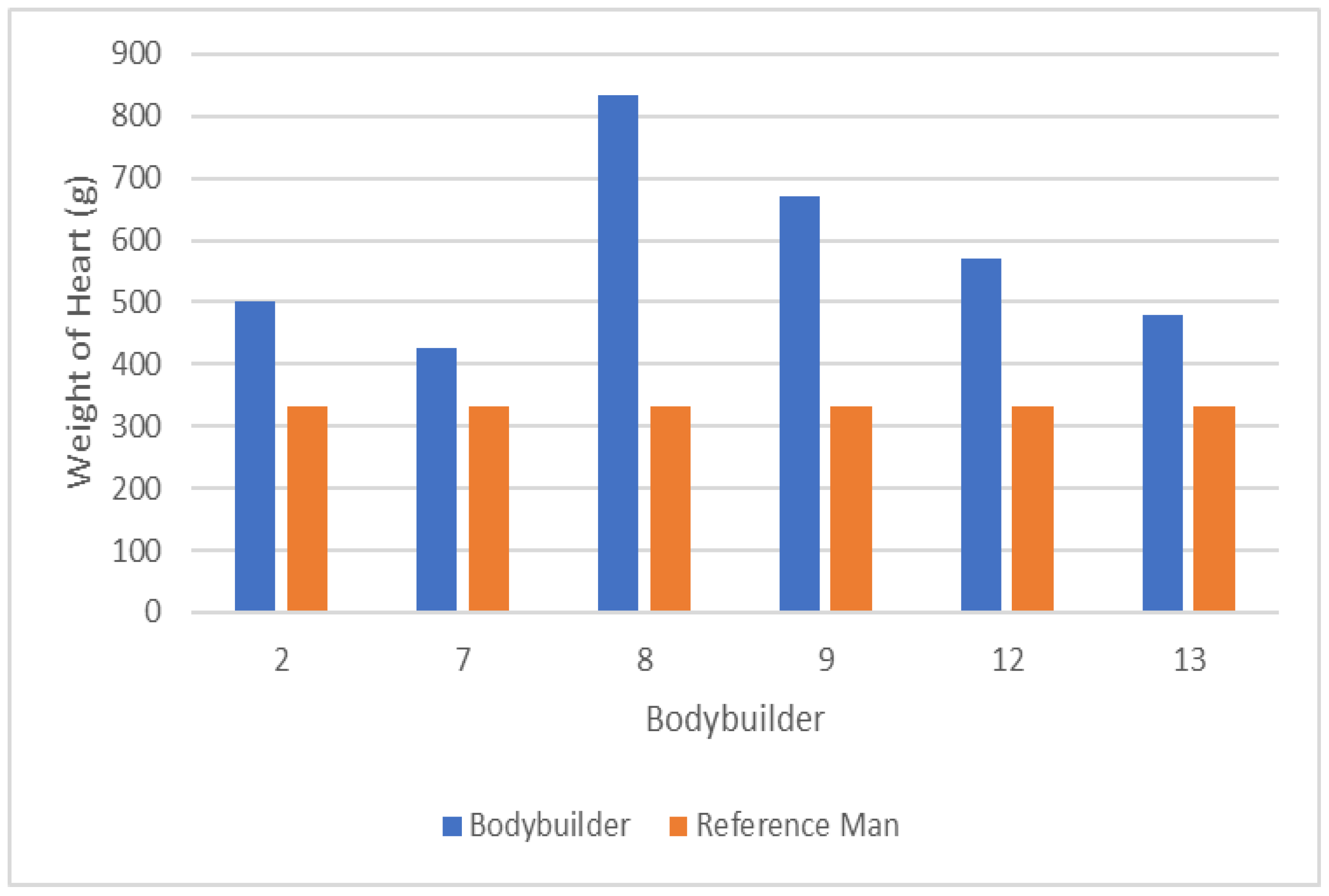
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sagoe, D.; Molde, H.; Andreassen, C.S.; Torsheim, T.; Pallesen, S. The Global Epidemiology of Anabolic-Androgenic Steroid Use: A Meta-Analysis and Meta-Regression Analysis. Ann. Epidemiol. 2014, 24, 383–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berning, J.M.; Adams, K.J.; Stamford, B.A. Anabolic Steroid Usage in Athletics: Facts, Fiction, and Public Relations. J. Strength Cond. Res. 2004, 18, 908–917. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Collins, R.; Darkes, J.; Gwartney, D. A League of Their Own: Demographics, Motivations and Patterns of Use of 1,955 Male Adult Non-Medical Anabolic Steroid Users in the United States. J. Int. Soc. Sports Nutr. 2007, 4, 12. [Google Scholar] [CrossRef] [Green Version]
- Kanayama, G.; Pope, H.G., Jr. History and Epidemiology of Anabolic Androgens in Athletes and Non-Athletes. Mol. Cell. Endocrinol. 2018, 464, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Adami, P.E.; Koutlianos, N.; Baggish, A.; Bermon, S.; Cavarretta, E.; Deligiannis, A.; Furlanello, F.; Kouidi, E.; Marques-Vidal, P.; Niebauer, J.; et al. Cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids in relation to sports: A position statement of the sport cardiology and exercise nucleus of the European Association of Preventative Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 559–575. [Google Scholar] [CrossRef]
- Hackett, D.A. Training, Supplementation, and Pharmacological Practices of Competitive Male Bodybuilders Across Training Phases. J. Strength Cond. Res. 2022, 36, 963–970. [Google Scholar] [CrossRef]
- Fijan, A.; Eftekhari, M.H.; Dashtabi, A. The Prevalence of Anabolic Androgenic Steroid Misuse and Its Associated Factors among Bodybuilders in Shiraz, Iran. Int. J. Food Sci. Nutr. 2018, 3, 151–156. [Google Scholar]
- de Siqueira Nogueira, F.R.; de Freitas Brito, A.; de Oliveira, C.V.C.; Vieira, T.I.; Gouveia, R.L.B. Anabolic-Androgenic Steroid Use among Brazilian Bodybuilders. Subst. Use Misuse 2014, 49, 1138–1145. [Google Scholar] [CrossRef]
- Haerinejad, M.J.; Ostovar, A.; Farzaneh, M.R.; Keshavarz, M. The Prevalence and Characteristics of Performance-Enhancing Drug Use Among Bodybuilding Athletes in the South of Iran, Bushehr. Asian J. Sports Med. 2016, 7, e35018. [Google Scholar] [CrossRef] [Green Version]
- Razavi, Z.; Moeini, B.; Shafiei, Y.; Bazmamoun, H. Prevalence of Anabolic Steroid Use and Associated Factors among Body-Builders in Hamadan, West Province of Iran. J. Res. Health Sci. 2014, 14, 163–166. [Google Scholar]
- Steele, I.; Pope, H.; Ip, E.J.; Barnett, M.J.; Kanayama, G. Is Competitive Body-Building Pathological? Survey of 984 Male Strength Trainers. BMJ Open Sport Exerc. Med. 2020, 6, e000708. [Google Scholar] [CrossRef] [PubMed]
- Iraki, J.; Fitschen, P.; Espinar, S.; Helms, E. Nutrition Recommendations for Bodybuilders in the Off-Season: A Narrative Review. Sports 2019, 7, 154. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.M.; Helms, E.R.; Trexler, E.T.; Fitschen, P.J. Nutritional Recommendations for Physique Athletes. J. Hum. Kinet. 2020, 71, 79–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, R.C.; Prestes, J.; Enes, A.; de Moraes, W.M.A.; Trindade, T.B.; de Salles, B.F.; Aragon, A.A.; Souza-Junior, T.P. Training Programs Designed for Muscle Hypertrophy in Bodybuilders: A Narrative Review. Sports 2020, 8, 149. [Google Scholar] [CrossRef]
- Manore, M.M.; Thompson, J.; Russo, M. Diet and Exercise Strategies of a World-Class Bodybuilder. Int. J. Sport Nutr. 1993, 3, 76–86. [Google Scholar] [CrossRef] [Green Version]
- Alway, S.E.; Grumbt, W.H.; Stray-Gundersen, J.; Gonyea, W.J. Effects of Resistance Training on Elbow Flexors of Highly Competitive Bodybuilders. J. Appl. Physiol. 1992, 72, 1512–1521. [Google Scholar] [CrossRef]
- Gentil, P.; de Lira, C.A.B.; Paoli, A.; Dos Santos, J.A.B.; da Silva, R.D.T.; Junior, J.R.P.; da Silva, E.P.; Magosso, R.F. Nutrition, Pharmacological and Training Strategies Adopted by Six Bodybuilders: Case Report and Critical Review. Eur. J. Transl. Myol. 2017, 27, 6247. [Google Scholar] [CrossRef]
- Achar, S.; Rostamian, A.; Narayan, S.M. Cardiac and Metabolic Effects of Anabolic-Androgenic Steroid Abuse on Lipids, Blood Pressure, Left Ventricular Dimensions, and Rhythm. Am. J. Cardiol. 2010, 106, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Barbosa Neto, O.; da Mota, G.R.; De Sordi, C.C.; Resende, E.A.M.R.; Resende, L.A.P.R.; Vieira da Silva, M.A.; Marocolo, M.; Côrtes, R.S.; de Oliveira, L.F.; Dias da Silva, V.J. Long-Term Anabolic Steroids in Male Bodybuilders Induce Cardiovascular Structural and Autonomic Abnormalities. Clin. Auton. Res. 2018, 28, 231–244. [Google Scholar] [CrossRef]
- Baggish, A.L.; Weiner, R.B.; Kanayama, G.; Hudson, J.I.; Picard, M.H.; Hutter, A.M., Jr.; Pope, H.G., Jr. Long-Term Anabolic-Androgenic Steroid Use Is Associated with Left Ventricular Dysfunction. Circ. Heart Fail. 2010, 3, 472–476. [Google Scholar] [CrossRef] [Green Version]
- Smit, D.L.; de Ronde, W.; Voogel, B.J.; den Heijer, M. Anabolic Androgenic Steroids Induce Reversible Left Ventricular Hypertrophy and Cardiac Dysfunction. Echocardiography Results of the HAARLEM Study. Front. Reprod. Health 2021, 58, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hall, D. Kali Muscle Gives Heart Attack Update, Sends Warning to Bodybuilders. Available online: https://fitnessvolt.com/kali-muscle-heart-attack-update/ (accessed on 12 February 2022).
- Stewart, B. Dead Bodybuilders. Available online: https://www.heartwise.com/whatsnew/2021/11/30/dead-bodybuilders (accessed on 11 February 2022).
- Hornik, C. How Mr Olympia Bodybuilders like Shawn Rhoden and George Peterson Are Dying in an Industry under Fire. Available online: https://www.the-sun.com/sport/3446217/heart-attacks-overdoses-bodybuilding-stars-perfection-sports/ (accessed on 11 February 2022).
- Evolution of Bodybuilding. Available online: https://www.evolutionofbodybuilding.net/tag/death/ (accessed on 11 February 2022).
- Magnante, M. Remembering 28 Bodybuilders Who Passed Away (2017–2020). Available online: https://fitnessvolt.com/bodybuilders-passed-away/ (accessed on 12 February 2022).
- 10 Bodybuilders Who Died Young and Rocked the Fitness Industry. Available online: https://playcrazygame.com/2021/11/22/10-bodybuilders-who-died-young-and-rocked-the-fitness-industry/ (accessed on 12 February 2022).
- Chris Colucci, T.N. Big Dead Bodybuilders. Available online: https://www.t-nation.com/pharma/big-dead-bodybuilders/ (accessed on 12 February 2022).
- Merritt, G. Do pro Bodybuilders Die Younger than Average? (Updated). Available online: https://www.thebarbell.com/do-pro-bodybuilders-die-younger-than-average/ (accessed on 12 February 2022).
- Keats, T.E. A Report Prepared by a Task Group of Committee 2 of the International Commission on Radiological Protection Reference Man. Radiology 1975, 117, 584. [Google Scholar] [CrossRef]
- Walpot, J.; Juneau, D.; Massalha, S.; Dwivedi, G.; Rybicki, F.J.; Chow, B.J.W.; Inácio, J.R. Left Ventricular Mid-Diastolic Wall Thickness: Normal Values for Coronary CT Angiography. Radiol. Cardiothorac. Imaging 2019, 1, e190034. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.K. Obesity and Coronary Heart Disease. Am. J. Med. Sci. 2001, 321, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Bamman, M.M.; Hunter, G.R.; Newton, L.E.; Roney, R.K.; Khaled, M.A. Changes in Body Composition, Diet, and Strength of Bodybuilders during the 12 Weeks prior to Competition. J. Sports Med. Phys. Fitness 1993, 33, 383–391. [Google Scholar] [PubMed]
- Schoenfeld, B.J.; Alto, A.; Grgic, J.; Tinsley, G.M.; Trexler, E.T. Alterations in Body Composition, Resting Metabolic Rate, Muscular Strength, and Eating Behavior in Response to Natural Bodybuilding Competition Preparation: A Case Study. J. Strength Cond. Res. 2020, 34, 3124–3138. [Google Scholar] [CrossRef]
- Jacobson, B.H.; Cook, D.; Redus, B. Correlation between Body Mass Index and Percent Body Fat of Trained Body Builders. Percept. Mot. Skills 2003, 96, 931–932. [Google Scholar] [CrossRef]
- Kouri, E.M.; Pope, H.G., Jr.; Katz, D.L.; Oliva, P. Fat-Free Mass Index in Users and Nonusers of Anabolic-Androgenic Steroids. Clin. J. Sport Med. 1995, 5, 223–228. [Google Scholar] [CrossRef]
- Esposito, M.; Licciardello, G.; Privitera, F.; Iannuzzi, S.; Liberto, A.; Sessa, F.; Salerno, M. Forensic Post-Mortem Investigation in AAS Abusers: Investigative Diagnostic Protocol. A Systematic Review. Diagnostics 2021, 11, 1307. [Google Scholar] [CrossRef]
- Dickerman, R.D.; Schaller, F.; McConathy, W.J. Left Ventricular Wall Thickening Does Occur in Elite Power Athletes with or without Anabolic Steroid Use. Cardiology 1998, 90, 145–148. [Google Scholar] [CrossRef]


{kind=link}
| Website (Accessed on 11 February 2022) | Reference |
|---|---|
| www.heartwise.com | [23] |
| www.the-sun.com | [24] |
| www.evolutionofbodybuilding.net | [25] |
| www.fitnessvolt.com | [26] |
| www.playcrazygame.com | [27] |
| www.t-nation.com | [28] |
| www.thebarbell.com | [29] |
| Bodybuilder | Unofficial Reported Cause of Death | Birth Year | Date of Death | Place of Death |
|---|---|---|---|---|
| 1 | Myocardial infarction | 1975 | 11/6/2021 | Nevada |
| 2 | Sudden cardiac arrest | 1984 | 10/6/2021 | Florida |
| 3 | Pulmonary embolism/ Myocardial infarction | 1972 | 8/8/2021 | Ohio |
| 4 | Natural causes | 1983 | 5/21/2020 | Alabama |
| 5 | Unknown | 1985 | 6/3/2020 | New Jersey |
| 6 | Heart failure | 1985 | 5/30/2019 | Oregon |
| 7 | Natural via cardiomyopathy | 1989 | 8/22/2017 | California |
| 8 | Myocardial infarction | 1991 | 8/22/2017 | Florida |
| 9 | Enlarged organs | 1970 | 8/25/2017 | Florida |
| 10 | Undisclosed | 1970 | 1/24/2015 | California |
| 11 | Myocardial infarction/heart failure | 1965 | 8/16/2014 | California |
| 12 | Myocardial infarction | 1972 | 2/20/2013 | Georgia |
| 13 | Accidental drowning/ Myocardial infarction | 1973 | 9/11/2011 | Texas |
| 14 | Myocardial infarction | 1966 | 2/19/2011 | Nevada |
| Sources: [23,24,25,26,27,28,29] | ||||
| Bodybuilder | Age (Years) | Height (m) | Weight (kg) | Body Mass Index kg/m2 |
|---|---|---|---|---|
| 2 | 37 | 1.68 | 93.2 | 33 |
| 7 | 30 | 1.7 | 93.2 | 32.2 |
| 8 | 26 | 1.83 | 120 | 35.8 |
| 9 | 46 | 1.83 | 100 | 29.9 |
| 12 | 40 | 1.83 | 127.3 | 38 |
| 13 | 37 | 1.8 | 107.5 | 33.2 |
| Mean ± SD | 36 ± 7.1 | 1.82 ± 0.02 | 103.8 ± 5.3 | 31.6 ± 2.3 |
| Bodybuilder | Coroner Summary of Findings |
|---|---|
| 2 | Sudden cardiac dysrhythmia due to hypertensive cardiovascular disease. Cardiomegaly with ventricular hypertrophy. Anabolic steroid use noted as a contributory factor. The coronary arteries are patent and have no arteriosclerosis. The atrial and ventricular chambers are not dilated. The papillary muscles and chordae tendineae are thickened. |
| 7 | The cause of death is steroid-induced cardiomyopathy. There is segmental atherosclerosis with up to 50% stenosis of the major arteries. Left ventricular dilation is present. |
| 8 | Bodybuilder with a history of dyslipidemia (low HDL, elevated LDL), elevated aminotransferases, and a chronic cough with some episodes of associated shortness of breath. Family history of early-onset atherosclerosis and hypertension. He collapsed during a period of ongoing respiratory symptoms. Follow-up evaluation showed abnormal electrocardiogram that met criteria for left ventricular hypertrophy. Severe cardiomegaly with concentric left ventricular hypertrophy. Coronary artery atherosclerosis. |
| 9 | Cardiomegaly with mild coronary atherosclerosis. The heart was enlarged with the myocardium of the left and right ventricles hypertrophied. The coronary arteries were normally developed and had mild atherosclerotic disease. The chambers were not dilated and the atrial and ventricular septae were intact. |
| 12 | The deceased died as a result of cardiac dysrhythmia associated with cardiomegaly and left ventricular hypertrophy. |
| 13 | Hypertensive and arteriosclerotic cardiovascular disease. Cardiomegaly with left ventricular hypertrophy. Coronary artery disease. Remote scar of myocardium. Generalized atherosclerosis. There are hypertensive changes of myocytes. A section of coronary artery reveals complicated atherosclerotic plaque with recanalization. The heart has four chamber dilation. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escalante, G.; Darrow, D.; Ambati, V.N.P.; Gwartney, D.L.; Collins, R. Dead Bodybuilders Speaking from the Heart: An Analysis of Autopsy Reports of Bodybuilders That Died Prematurely. J. Funct. Morphol. Kinesiol. 2022, 7, 105. https://doi.org/10.3390/jfmk7040105
Escalante G, Darrow D, Ambati VNP, Gwartney DL, Collins R. Dead Bodybuilders Speaking from the Heart: An Analysis of Autopsy Reports of Bodybuilders That Died Prematurely. Journal of Functional Morphology and Kinesiology. 2022; 7(4):105. https://doi.org/10.3390/jfmk7040105
Chicago/Turabian StyleEscalante, Guillermo, Dillon Darrow, V. N. Pradeep Ambati, Daniel L. Gwartney, and Rick Collins. 2022. "Dead Bodybuilders Speaking from the Heart: An Analysis of Autopsy Reports of Bodybuilders That Died Prematurely" Journal of Functional Morphology and Kinesiology 7, no. 4: 105. https://doi.org/10.3390/jfmk7040105