

Mechanisms and Comparative Treatments of Allergic Rhinitis including Phototherapy
Research Centre, Warwickshire College University Centre, Warwick New Road, Leamington Spa, Warwickshire CV32 5JE, UK
Allergies 2024, 4(1), 17-29; https://doi.org/10.3390/allergies4010002
Submission received: 24 October 2023
/
Revised: 12 January 2024
/
Accepted: 2 February 2024
/
Published: 16 February 2024
(This article belongs to the Special Issue Feature Papers 2023)
Abstract
:The treatment of allergic conditions presents a challenge for both seasonal allergic rhinitis and perennial rhinitis sufferers. The increasing prevalence of both of these types of allergic responses requires the use of a range of treatments which can provide relief. The treatment of allergic rhinitis has been considered under the ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines. Current treatment options include medication and avoidance for those with reduced responses, but more expensive treatments include immunotherapy and the use of monoclonal antibodies (mAb). All treatments target specific parts of the inflammatory response which includes mast cells, eosinophils and basophils. Phototherapy can be a useful addition to these treatments, and combinations of UV-B (5%), UV-A (25%) and visible light (70%) in phototherapy treatments have been shown to reduce the severity of symptoms. Phototherapy consisting of visible wavelengths and infrared light (660 nm 940 nm) was shown to be particularly effective in treating perennial rhinitis. The use of a range of wavelengths in the control of allergic responses is described in this paper. Phototherapy can form part of an effective treatment regime for allergic rhinitis sufferers which can exploit synergies in the control of the condition elicited through several pathways.
1. Introduction
Allergic rhinitis symptoms include rhinorrhea, nasal obstruction, nasal itching and sneezing. Allergic reactions that are IgE-mediated occur where the allergen is, for example, an outdoor pollen. Seasonal allergic rhinitis (SAR) is the term used by many physicians and research workers to describe these reactions [1]. The nasal symptoms of pollen allergy occur because, due to their size, pollen grains are predominantly deposited in the nasal cavities [2]. There are various indoor allergens which also cause allergic rhinitis. The occurrence of SAR is low in children but increases in late adolescents/young adults, which is the age at which SAR is frequently described. The impact of SAR can decline as sufferers become older.
2. Background to the Mechanism of Allergic Rhinitis
2.1. Symptoms of Allergic Rhinitis
Some symptoms of allergic rhinitis including rhinorrhea, nasal obstruction, nasal itching, and sneezing are reversible spontaneously or under treatment [1]. Allergic rhinitis usually peaks in teenagers and those in their twenties. The condition is heritable due to gene-based determinants of total IgE and specific allergic sensitization. The form of specific sensitivities is therefore as heritable as simple genetic traits. An association has been reported between genetic traits, such as the GATA3 gene, which encodes a protein belonging to the GATA family of transcription factors, and the subsequent risk of developing allergic rhinitis [1]. This observation was reported in a study using children suffering from atopic allergic rhinitis followed up until the age of 10. Further studies have identified candidate genes associated with allergic rhinitis [3,4]
2.2. Potential for Phototherapy-Mediated Early and Late Phase Allergic Responses
Activated Th2 lymphocytes produce cytokines (interleukins ILs) such as IL-4 [5]. Interleukin-4 (IL-4), which is a member of the γ-chain receptor cytokine family, is produced mainly by Th2 lymphocytes, basophils, and mast cells in response to receptor-mediated activation [6]. Light from 380 to 660 nm applied to cultures of human keratinocytes and macrophage/dendritic cells identified IL-4 as a key effector cytokine released in these cultures. However, it is not clear whether light from 380 to 660 nm applied to cultures changes/decreases the production of IL-4 in these cultures. IL-4 was identified as the first cytokine to be produced by mast cells and is responsible for promoting mast cell IL-13 production. During the allergic response, IL-4 is produced in vivo and rapidly made in mast cells to stimulate inflammatory responses. Although other pathways exist, IL 4 and IL 13 are also the most common cytokines associated with the regulation of B lymphocyte function [7]. B lymphocyte cells play a pivotal role in IgE-mediated allergies as a result of their unique ability to produce allergen-specific IgE antibodies that sensitize mast cells and basophils by binding to their high-affinity IgE receptors (FcεRI) [8].
2.3. Characteristics of Early Phase Responses
Sensitized individuals exhibit an early/immediate phase response which lasts for about 2–3 h after minimum exposure to the allergen. The early phase response comprises the degranulation of mast cells, which in sensitized individuals are abundant in the epithelial surfaces in the nose and eyes. They are particularly abundant in the nasal mucosa. When cross linkage between the allergen-specific IgE and the specific allergen occurs, mast cells degranulate (release substances). Histamine is a major component of these substances. This is the classic form of the early phase response. Histamine stimulates the sensory nerve endings and induces sneezing. Histamine can also stimulate the mucous glands, resulting in the secretion of mucous (rhinorrhea) and histamine, leukotrienes and prostaglandins, which act on the blood vessels causing nasal congestion [9].
2.4. Characteristics of Late Phase Responses
The late phase response occurs 4–6 h after antigen stimulation. The late phase has prolonged symptoms such as sneezing, rhinorrhea and nasal congestion which last for about 18–24 h. The late phase response is characterized by the inflammation of tissues and a cellular uptake of T lymphocytes, basophils and eosinophils [9]. Other components released by these cells include leukotrienes, kinins and histamine, all of which result in the continuation of the symptoms.
The activity of cytokines and chemokines like IL-4 and IL-13 that are secreted from mast cells is a key aspect of the late phase allergic response [10,11]. The cytokine IL-4 is particularly important as it regulates the differentiation of CD4+ T cells into Th-2 effector cells. This represents a marker of type II inflammatory responses. Cytokines also upregulate the expression systems of vascular cell adhesion molecules such as VCAM-1 on endothelial cells. This enables the infiltration of eosinophils, lymphocytes and basophils into the nasal mucosa. Physical inhibition resulting from phototherapy can reduce this infiltration and reduce the late phase allergic responses. Chemokines (TARC) released from epithelial cells [12,13] can function as chemo-attractants for eosinophils, basophils and T lymphocytes [14,15]. Granulocyte macrophage colony-stimulating factors (GM-CSF) released by epithelial cells prolong the survival of the infiltrated eosinophils in the nasal mucosa [16].
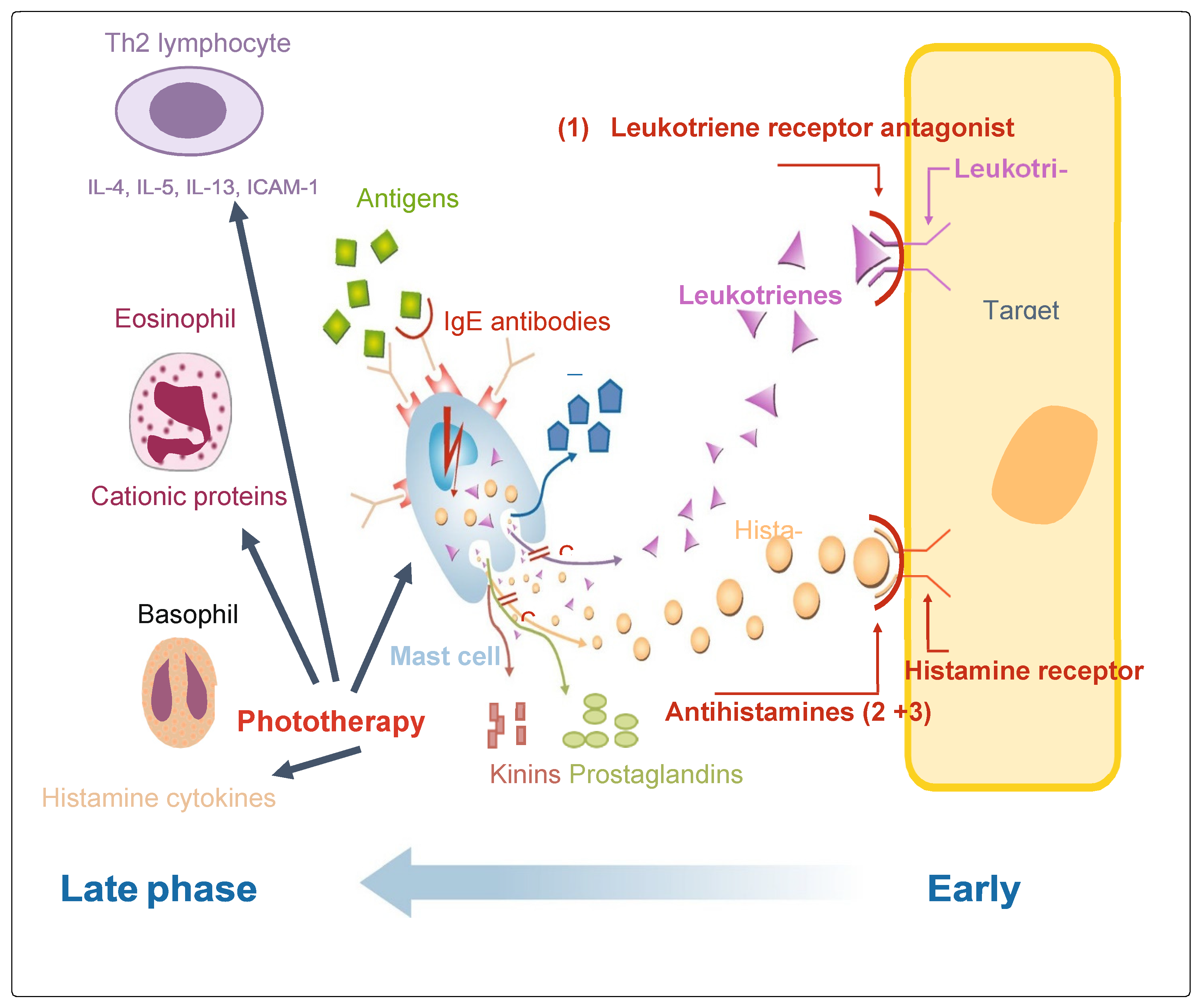
Other parts of the late phase response include mast cells, which have been found to contribute to the late phase response through histamine/tryptase-induced upregulation in nasal epithelial cells. Other mediators released such as eosinophil cationic protein (ECP) and platelet-activating factor are part of the late phase response. A summary of the early and late phase responses is shown in Figure 1.
2.5. AR Treatment According to ARIA (Allergic Rhinitis and Its Impact on Asthma) Guidelines
The ARIA guidelines form an important part of decisions regarding the treatment of AR. These guidelines cover a range of treatment types [18]. Self-management strategies are an important part of the ARIA guidelines. A system was proposed for a step-up or step-down of AR treatments from self-administration to emergency hospital admission. The guideline group aimed to adapt this approach to real-world evidence and the availability of medicines and resources [19]. Self-administration of AR treatments including phototherapy forms part of the ARIA guidelines. Pharmacotherapy and other treatments for AR patients are considered effective in the control of the disease. A range of considerations which include patient empowerment and preferences, symptom severity and multi-morbidity determine treatment. Other factors which are included in treatment decisions are efficacy and safety of the treatment, patient history in response to treatments and quality of life [20]. Applicability of treatment guidelines in the routine care of patients can be adapted based on the results of randomized control trials (RCTs). This is, however, limited by the methods used in the clinical trials [21]. Therefore, information from real-world evidence (RWE) is increasingly being considered in the creation of practice-oriented guidelines. Ideally, both RCT and RWE approaches will be merged.
3. Phototherapy Treatment of AR
3.1. Phototherapy Treatment of AR Using Visible Wavelengths
Limitations in the conventional therapies mean that alternative treatments for AR are required. Intranasal phototherapy has received growing interest as an alternative treatment to relieve the symptoms of AR patients. AR is often treated using pharmacological products alone or in combination, depending on the symptoms suffered. Many affected by AR would like to reduce the requirement for medicines or may have other conditions where there are other side effects of the medicines. Many allergic rhinitis sufferers wish to reduce the amount of medication that they take. Many find that medication does not control their symptoms adequately.
Considerable evidence exists which shows that phototherapy is an effective treatment for allergic rhinitis. Phototherapy can be used on all AR sufferers as a replacement therapy or concurrent with traditional medication. It can be an effective treatment for inflammatory and immune-mediated diseases. Phototherapy has an immunosuppressive effect, and ultraviolet (UV) and visible light treatment are used as a therapy for inflammatory skin diseases [22]. Flashed light also induces absorbance changes in cytochrome c oxidase. This can result in reductions in inflammation associated with mitochondrial dysfunction [23]. The wavelengths used in phototherapy were studied for their effects on antimicrobial peptides. Antimicrobial peptides such as LL37 can condense with DNA and are then retained within endosomal compartments. Epidermal expression of antimicrobial peptides (AMPs) such as cathelicidin LL-37 is downregulated in atopic eczema. UV radiation (100–400 nm) has no effect on the keratinocyte production of LL37; however, radiation of 280 nm UV induces LL37 formation. This explains why narrowband UVB (280–315 nm) is more effective against psoriasis compared to broadband UVB treatment.
Combining 25% UV-A, 5% UV-B and 70% visible light as UVAB is a therapeutic alternative in patients with AR. Apoptosis (programmed cell death) of these cells after phototherapy could be the underlying mechanism of decreased IL-5 production. T cells perpetuate and maintain allergic processes. Cell death after phototherapy has a long-term beneficial effect. Phototherapy treatment decreases eosinophil numbers and eosinophil cationic protein (ECP) levels in the nasal fluid. This could be attributed to the direct proapoptotic effect of UVAB on eosinophils and to the decreased IL-5 levels [22]. UV-A light significantly inhibits histamine release from basophils and mast cells. UV-B light has also an inhibitory effect on mast cells [24]. Phototherapy has therefore a role to play in the effective treatment of AR as it has effects on different inflammatory and immune-mediated mucosal symptoms [25]. It is also shown to be effective where AR symptoms persist.
Like many AR treatments, phototherapy cannot be applied directly to the nasal mucosa, which is the major limiting factor in this treatment. Clinical results may improve when UVAB is applied to a larger area of nasal mucosa. UV-B laser treatment in combination with UV-A (25%), UV-B (5%) and visible light (70%) inhibited wheal formation in skin tests [22,26,27]. Total nasal scores from allergen challenges were also reduced after application of both mUV/VIS combined with low-intensity visible light (mUV/VIS without UV) in treated groups [27]. The results were highly significant in the mUV/VIS-treated group in comparison with the visible light-treated cohort.
3.2. Phototherapy Effects of Red and Infrared Wavelengths
Many studies have been published showing the effect of light therapy as a therapeutic treatment for tissue repair, as well as its biochemical, cellular, histological and functional effects on tissues. Allergic symptoms depend on oxygen radical formation, which was suppressed after red light illumination. Red light or NIR wavelengths with different mechanisms of action from UV and visible light could be considered as treatments for AR. Far-infrared irradiation (FIR) therapy can improve blood flow and reduce inflammation [28]. Applying FIR to the nasal region of AR-affected patients has been shown to reduce symptoms such as eye itching, nasal itching/stuffiness and rhinorrhea [29]. Phototherapeutic devices which combine wavelengths as a treatment are therefore more likely to have a greater impact on allergic rhinitis. Recent studies using the allergy reliever device [30] showed significantly improved nasal symptoms of allergic rhinitis while using the device during exposure to indoor and outdoor allergens. The allergy reliever uses 660 nm and 940 nm wavelengths of light. This study was conducted using allergy sufferers but at the time of year when additional allergen exposure from pollens was absent. This demonstrated that the reduced allergic reactions resulted from using the allergy reliever, as all patients in the study were not using pharmacological interventions.
3.3. Evidence for Phototherapy as a Successful Treatment for Allergic Rhinitis
The effectiveness of phototherapy on allergic symptoms has been documented previously [22,24,25,26]. The main trials where effects are reported are listed in Table 1. It is not possible to list all trials in summary as over 2000 trials/reports have been published on the beneficial effects of phototherapy. Many wavelengths of light used in phototherapy studies have been shown to be effective. These studies showed that phototherapy (UV-A, UV-B, visible light wavelengths and near-red and infra-red wavelengths) suppresses the clinical symptoms of allergic rhinitis. Most trials combined different wavelengths in treatments and this was shown to have a synergistic effect on the suppression of allergic rhinitis. Most treatments combined UVA and UVB with visible light; however, some treatments combined UV and infrared light. This has certain advantages due to the differences in the mechanism of activity between different wavelengths. Applying a wavelength of 660 nm and infrared light (940 nm) therapy improved the clinical symptoms of eye itching, nasal itching, nasal stuffiness, rhinorrhea and sneezing significantly during the period of therapy. Trials combining these wavelengths resulted in greater control of AR in comparison to pharmacological interventions [31]. These extensive trials demonstrated that due to the combination of wavelengths used, there was a greater controlling effect on allergic rhinitis symptoms (Table 2).
3.4. Safety of Visible and NIR Wavelengths Used in Phototherapy
The evidence shows that nostril-based application of phototherapy improves blood rheology and cerebral blood flow without needing to puncture blood vessels, indicating that this treatment may have equivalent results to peripheral intravenous laser irradiation. A potential problem of NIR light being in contact with skin is the heating effect. NIR light from an LED produces two types of energy, radiated NIR light energy which is absorbed by the skin and energy conducted as heat
Radiated energy increases when quantified temperature is less than 0.5 °C [36]. NIR sources of radiating light are LEDs and lasers. Safety regulations of laser applications are applied to LED sources [37]. Radiated light energy has a high potential to cause serious injuries. This property is beneficial in surgical operations. The skin damage threshold depends on the wavelength, spot size and pulse length of the light used [37]. Light absorption by tissues depends on the wavelength of the light radiated. This effect results from the absorption of light by water. Wavelengths longer than 950 nm are strongly absorbed by water. Water is virtually transparent to the light in the NIR range. The constant circulation of blood means that deep tissues do not heat up, as blood pigments mostly absorb NIR light. NIR light does not present the risk of tissue damage that occurs at wavelengths longer than 950 nm.
LED light diverges as it leaves the source, and so, it is difficult to focus all energy into one spot [38]. Spot sizes can be produced by means of additional optics. Therefore, spot size is not an issue in LED safety considerations [38]. Short time durations cannot be achieved by LEDs because of the slow response time of the semiconductor junction [39]. For this reason, LEDs do not carry the risk caused by short powerful bursts. It is clear that the methods of application of these wavelengths is safe and effective for the treatment of allergic rhinitis. The effects of these wavelengths for the treatment of allergic rhinitis have been reported by [30,35]. Recently, it has been reported [40] that light of 650 nm administered to the nasal area was safe and effective for the control of allergic rhinitis when assessed as part of a clinical trial.
3.5. Use of Phototherapy as a Reliever of Symptoms in Allergic Rhinitis
Combining wavelengths has been shown to be effective not only as background treatment but also as a reliever [30]. It was also effective in clinical trials conducted by Emberlin and Lewis [35]. The combination of 660 nm light with visible spectra has been shown to decrease IL-5 production. This interleukin is a key cytokine in triggering the AR response (Figure 1). Light (660 nm) has an effect on memory T cells, which is important as these maintain the allergic process. Decreased numbers of eosinophils and levels of eosinophil cationic protein (ECP) were observed in nasal lavage after phototherapy. This is explained by a proapoptotic outcome after treatment with 660 nm/visible light on eosinophils, with decreases in local IL-5 levels [35]. The allergy reliever is effective in treating AR because of these effects. Additionally, the allergy reliever utilizes light with a similar wavelength to 940 nm. Far-infrared irradiation (FIR) therapy (approx. 940 nm) improves blood circulation and reduces inflammation resulting from thermal and non-thermal effects [30]. For this reason, a combination of wavelengths used in the allergy reliever is more effective as a treatment for AR.
4. Treatments for Allergic Rhinitis Using Pharmacological Intervention
4.1. Approaches to the Use of Allergic Rhinitis Pharmacotherapies
Pharmacotherapies are commonly used to suppress allergic rhinitis. A phased approach to the treatment of allergic rhinitis was recommended by ARIA, including the use of second-generation antihistamines and topical nasal corticosteroids. The European Academy of Allergy and Clinical Immunology (EAACI) collaborated with ARIA to define a framework of requirements for the pharmacology, efficacy and safety of antihistamines and nasal corticosteroids [41]. Antihistamine/antileukotriene treatment is effective in AR suppression. Antihistamines may prevent AR symptoms, while the prophylactic activity of antileukotrienes remains unclear. When these pharmacotherapies are combined, as in a 6-week pretreatment with montelukast (oral antileukotriene) and cetirizine (oral antihistamine), patients suffered significantly less from sneezing, eye and nose itching, nasal congestion and rhinorrhea than those in whom the treatment was started at the beginning of the pollen season [42]. The majority of AR drugs, such as many antihistamines, intranasal corticosteroids, or alpha sympathomimetics or low-effective mast cell stabilizers, are non-prescription drugs. Nevertheless, there are side effects to the use of these treatments. Antihistamines can be quite sedating due to their ability to cross the blood–brain barrier. Leukotriene receptor antagonists are not as effective as other treatments and are often used in combination with other pharmacological interventions [43]. There was 86% agreement among patients who prefer “not to take any medicine if they can avoid it”, showing that non-pharmacotherapies were favored by patients [44]. This emphasizes the need for alternative treatments which are effective for allergic rhinitis.
Phototherapy and other alternatives are considered as complimentary treatments to pharmacotherapies treatments. However, care must be taken to select complimentary treatments that have different modes of action compared to pharmacotherapies. Most pharmacotherapies usually interact with the allergic pathophysiological pathways and reflect modes of action (Figure 1).
4.2. Leukotriene Receptors (LTRAs)
LTRAs interfere with the activity and secretion of cysteinyl leukotrienes (CysLTs). CysLTs are powerful inflammatory mediators which affect nasal congestion, mucus production and inflammatory reactions in the cell [45,46,47,48]. They have anti-inflammatory activities by inhibiting eosinophil migration/adhesion to vascular endothelial cells [49]. Additionally, LTRAs under some circumstances can inhibit reactive oxygen species’ generation and the release of protease and elastase from human eosinophils and neutrophils [50].
4.3. Oral Antihistamines (OAHs)
Oral antihistamines inhibit the interaction of histamine with H1 receptors. OAHs at elevated concentrations may inhibit histamine-stimulated cytokine release [51,52,53,54,55,56]. One problem in using these drugs is that elevated concentrations are not easy to achieve in the nasal mucosa, which is a common problem with treatments.
4.4. Intranasal Antihistamines (INAH)
One advantage of the application of antihistamines ensures that the drug reaches directly the nasal mucosa. This enhances antiallergic/inflammatory effects locally while reducing systemic exposure [57]. These compounds are effective for the treatment of AR. Mast cells can be stabilized by the application of INAH, which block calcium channels on mast cells, with positive effects on the release of tryptase, prostaglandins, kinins and interleukins [58,59]. Intranasal antihistamines reduce inflammatory reactions and mediators such as tumor necrosis factor (TNF)α ([60], granulocyte-stimulating factor (GM-CSF), cytokines (e.g., interleukin [IL]-1β, IL-4, and IL-8) [36,61] and adhesion molecules (e.g., intercellular adhesion molecule-1 [62]. These stimulate inflammatory responses and induce the late-phase responses [58].
4.5. Intranasal Corticosteroids (INSs)
Intranasal glucocorticosteroids (INCSs) are considered the gold standard in the pharmacological therapy of AR, as outlined in the results of the 2016 ARIA conference [63]. INSs inhibit the activation of many allergenic pathways and cellular responses. This prevents these cells from finding their way into the nasal mucosa [64,65,66,67]. The effect is due to reduction in ICAM-1 expression on nasal epithelial cells, in both allergenic phases and after allergen challenge. Experimental studies indicate that INSs reduce IL-13 production in mitogen-stimulated cells and reduce the production of GM-CSF, TNFα, IL-6 and IL-8 generated by in vitro cultured nasal epithelial cells [68,69]. The anti-inflammatory action of INSs may affect hyper-reactivity in chronic AR. Treatment with an INS reduces nasal congestion and nasal histamine hyper-reactivity in sufferers with perennial AR [70].
5. Other Treatments for Allergic Rhinitis Using Non-Pharmacological Interventions
5.1. Avoidance
Avoiding triggering allergic rhinitis has always been an effective treatment for these reactions. This may be difficult to achieve because avoiding allergens from pollens may not be possible at certain times of the year. Many sufferers also have mixed allergic and non-allergic rhinitis, making avoidance difficult. The severity of rhinitis can correlate with the levels of allergens in indoor and outdoor environments [71]. Using allergen-impermeable bedding covers for the mattress and pillow can be a useful protection against dust mite, while vacuums with high-HEPA air filters are also effective. Other precautions include washing bedclothes and bed sheets in hot water (60 °C).
No one method can provide effective treatment, and sufferers should use combinations of avoidance methods. Animal allergies require removal of the pet from the home, with careful vacuuming of all carpets and mattresses. Using these methods may take 20 weeks to reduce cat dander levels to that of cat free homes. Inconsistent results have been shown for reducing cat dander by regular bathing of cats [63,72]. Reduced numbers of pets correlate with lower dander levels; however, keeping cats outside does not significantly reduce the presence of Fel d 1 (the major allergen in cat dander). Reducing the access of dogs to the home and bedroom correlates with lower amounts of Can f, which is an allergen produced by dogs [73,74]. Fungal allergen levels in homes can also be reduced by controlling moisture levels. The control of food debris decreases cockroach infestations, but it may take over 6 months to remove residual cockroach allergen.
5.2. Pollen Barriers and Non-Pharmacotherapies
Pollen barriers are available as a remedy for allergic responses such as hay fever. These barriers are applied to the nasal cavity and act to reduce the amount of allergens and allergen carries entering the nasal mucosa [75]. The mechanism includes trapping pollen grains entering the nostrils. This reduces the amount of allergen in contact with the nose. Investigations into the numbers of grass pollen grains/total pollen grains collected in the nostrils coated with pollen barriers showed higher numbers collected on the uncoated nostrils (Table 1). These studies gave no indication of the amount of reduction in allergens entering the nose, as many particles including pollen would enter the nose unimpeded. However, they may have some effect, especially at lower allergen levels.
Artificial tears and compress therapy are often advised for the treatment of seasonal allergic conjunctivitis. Their efficacy in relieving the signs and symptoms of the ocular allergic response has been demonstrated [76]. The study demonstrated that artificial tears and cold compresses were effective in relieving the signs and symptoms of the ocular allergic responses, each individually equivalent to epinastine and superior when combined. The efficacy of epinastine was enhanced by the addition of cold compress treatments.
6. Allergen Immunotherapy (AIT)
Immunotherapy is used to treat AR and commonly involves the repeated application of allergen extracts as infections or sublingual applications [77]. Subcutaneous immunotherapy (SCIT) can result in successful outcomes for allergic rhinitis patients where IgE mediates the onset of symptoms. SCIT has some advantages over other types of treatment because it can result in long-term control for years, with the prevention and development of new allergen sensitivities. Immunotherapy is underutilized, although there are benefits for the control of allergenic reactions triggered by pollen, animal particles and dust mites. However, localized adverse reactions can occur around the area where the injection was administered and severe systemic reactions can occur during subcutaneous immunotherapy. One percent of those receiving immunotherapy experience these adverse reactions [78]. The two main risk factors for adverse reactions were high pollen levels and dosing errors.
Patients should receive immunotherapy injections in a clinical environment so that anaphylaxis can be treated if it occurs. Patients must be observed for 30 min after each treatment injection to avoid this possibility [79]. Other problems include discomfort, the frequency of injections and the high cost of treatment. Immunotherapy can modify the disease and is cost-effective, as shown when there is a comparison of the direct costs of treating allergic rhinitis. Indirect costs mean that immunotherapy may be much more economic compared to other treatments. Immunotherapy is commonly delivered subcutaneously, but sublingual immunotherapy (SLIT) can also be used. Some disadvantages of SLIT include oral itching [78]. However, these effects seem to be the same as those observed in the placebo cohort of trials and may be due to the delivery mechanism.
Standardization in SLIT is another issue as timothy grass pollen extract supply is limited commercially. SLIT carries a low risk of anaphylaxis and using it means that therapy can begin at the maintenance dose without a build-up phase. SLIT treatments for dust mite allergy are effective in reducing symptom scores. Anaphylaxis is not very common in studies with SLIT, but it can occur during prolonged treatment. SLIT is not as common a treatment as SCIT, but further work is required to determine the optimal dose and the selection of patients.
7. Conclusions
Medications and applications of a range of treatments have been used with good results in the management of AR, but complete resolution of symptoms cannot be guaranteed and so cases prove difficult to treat. Drug-based medication is not suitable for some sufferers, especially pregnant and breast-feeding women. The use of phototherapy as a therapeutic treatment for AR is a safe and promising treatment which could be useful. The evidence suggests that phototherapy suppresses the effector phase of AR, which produces a significant suppression of clinical symptoms. Phototherapy has been used as a treatment for inflammatory skin diseases and is considered a new and alternative treatment in allergic rhinitis [80]. Allergic rhinitis and atopic dermatitis have many similar pathways which result in the conditions and as such, are similar [25]. Phototherapy is attributed to a local immunosuppressive and immunomodulant action. Therefore, phototherapy could inhibit other aspects of effector phases of allergic reactions. This includes the inhibition of antigen presentation by dendritic cells, which induces apoptosis of immune cells. Other types of inhibition resulting from phototherapy include the synthesis and release of pro-inflammatory mediators from eosinophils, mast cells, basophils and T cells. Phototherapy could therefore become another key treatment for use by allergic rhinitis sufferers.
Funding
European Union ERDF Open Call: Priority Axis 3, Project OC38R17P0534.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bousquet, J.; van Cauwenberge, P.; Khaltaev, N.; Aria Workshop Group; World Health Organization. Allergic Rhinitis and Its Impact on Asthma. J. Allergy Clin. Immunol. 2001, 108, S147–S334. [Google Scholar] [CrossRef]
- D’Amato, G.; Spieksma, F.T.M.; Liccardi, G.; Jager, S.; Russo, M.; Kontou-Fili, K.; Nikkels, H.; Wuthrich, B.; Bonini, S. Pollen related allergy in Europe. Allergy 1998, 53, 567–578. [Google Scholar] [CrossRef]
- North, M.L.; Ellis, A.K. The role of epigenetics in the developmental origins of allergic disease. Ann. Allergy Asthma Immunol. 2011, 106, 355–361. [Google Scholar] [CrossRef]
- Moodycliffe, A.M.; Kimber, I.; Norval, M. The effect of ultraviolet B irradiation and urocanic acid isomers on dendritic cell migration. Immunology 1992, 77, 394–399. [Google Scholar]
- Hollingsworth, J.W.; Maruoka, S.; Boon, K.; Garantziotis, S.; Li, Z.; Tomfohr, J.; Bailey, N.; Potts, E.N.; Whitehead, G.; Brass, D.M.; et al. In utero supplementation with methyl donors enhances allergic airway disease in mice. J. Clin. Investig. 2008, 118, 3462–3469. [Google Scholar] [CrossRef]
- Silva-Filho, J.L.; Caruso-Neves, C.; Pinheiro, A.A.S. IL-4: An important cytokine in determining the fate of T cells. Biophys. Rev. 2014, 6, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.; Candotti, F.; Smith, S.; O’Shea, J.J.; Weinberg, K.; Johnston, J.A. Interleukin-4 Signalling in B Lymphocytes from Patients with X-linked Severe Combined Immunodeficiency Open Access. Cell Biol. Metab. 1997, 272, 7314–7319. [Google Scholar] [CrossRef]
- Satitsuksanoa, P.; Daanje, M.; Akdis, M.; Boyd, S.D.; van de Veen, W. Allergy Biology and dynamics of B cells in the context of IgE-mediated food allergy. Allergy 2021, 76, 1707–1717. [Google Scholar] [CrossRef]
- Naclerio, R.M. Allergic rhinitis. N. Engl. J. Med. 1991, 325, 860–869. [Google Scholar] [PubMed]
- Bradding, P.; Feather, I.H.; Wilson, S.; Bardin, P.; Heusser, C.H.; Holgate, S.T.; Howarth, P.H. Immuno-localization of cytokines in the nasal mucosa of normal and perennial rhinitic subjects. The mast cell as a source of IL- 4, IL-5, and IL-6 in human allergic mucosal inflammation. J. Immunol. 1993, 151, 3853–3865. [Google Scholar] [CrossRef] [PubMed]
- Pawankar, R.U.; Okuda, M.; Hasegawa, S.; Suzuki, K.; Yssel, H.; Okubo, K.; Okumura, K.; Ra, C. Interleukin-13 expression in the nasal mucosa of perennial allergic rhinitis. Am. J. Respir. Crit. Care Med. 1995, 152, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Xia, Y.; Nguyen, A.; Lai, Y.H.; Feng, L.; Mosmann, T.R.; Lo, D. Effects of Th2 cytokines on chemokine expression in the lung: IL-13 potently induces eotaxin expression by airway epithelial cells. J. Immunol. 1999, 162, 2477–2487. [Google Scholar] [CrossRef] [PubMed]
- Sekiya, T.; Miyamasu, M.; Imanishi, M.; Yamada, H.; Nakajima, T.; Yamaguchi, M.; Fujisawa, T.; Pawankar, R.; Sano, Y.; Ohta, K.; et al. Inducible expression of a Th2- type CC chemokine thymus- and activation-regulated chemokine by human bronchial epithelial cells. J. Immunol. 2000, 165, 2205–2213. [Google Scholar] [CrossRef] [PubMed]
- Ozu, C.; Pawankar, R.; Takizawa, R.; Yamagishi, S.; Yagi, T. Regulation of mast cell migration into the allergic nasal epithelium by RANTES and not SCF. J. Allergy Clin. Immunol. 2004, 113, S28. [Google Scholar] [CrossRef]
- Lilly, C.M.; Nakamura, H.; Kesselman, H.; Nagler-Anderson, C.; Asano, K.; Garcia-Zepeda, E.A.; Rothenberg, M.E.; Drazen, J.M.; Luster, A.D. Expression of eotaxin by human lung epithelial cells: Induction by cytokines and inhibition by glucocorticoids. J. Clin. Investig. 1997, 99, 1767–1773. [Google Scholar] [CrossRef]
- Pawankar, R.; Ra, C. Heterogeneity of mast cells and T cells in the nasal mucosa. J. Allergy Clin. Immunol. 1996, 98, S248–S262. [Google Scholar] [CrossRef] [PubMed]
- Bjermer, L.; Westman, M.; Holmström, M.; Wickman, M.C. The complex pathophysiology of allergic rhinitis: Scientific rationale for the development of an alternative treatment option. Allergy Asthma Clin. Immunol. 2019, 15, 24. [Google Scholar] [CrossRef]
- Klimek, L.; Bachert, C.; Pfaar, O.; Becker, S.; Bieber, T.; Brehler, R.; Buhl, R.; Casper, I.; Chaker, A.; Czech, W.; et al. ARIA guideline 2019: Treatment of allergic rhinitis in the German health system. Allergo J. Int. 2019, 28, 255–276. [Google Scholar] [CrossRef]
- Sherman, R.E.; Anderson, S.A.; Dal Pan, G.J.; Gray, G.W.; Gross, T.; Hunter, N.L.; LaVange, L.; Marinac-Dabic, D.; Marks, P.W.; Robb, M.A.; et al. Real-world evidence—What is it and what can it tell us? N. Engl. J. Med. 2016, 375, 2293–2297. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Wallace, D.; Dykewicz, M.; Shneyer, L. Minimal clinically important difference (MCID) in allergic rhinitis: Agency for Healthcare Research and quality or anchor-based thresholds? J. Allergy Clin. Immunol. Pract. 2016, 4, 682–688. [Google Scholar] [CrossRef]
- Oyinlola, J.O.; Campbell, J.; Kousoulis, A.A. Isreal world evidence influencing practice? Asystematic review of CPRD research in NICE guidances. BMC Health Serv. Res. 2016, 16, 299. [Google Scholar] [CrossRef]
- Koreck, A.I.; Csoma, Z.; Bodai, L.; Ignacz, F.; Kenderessy, A.S.; Kadocsa, E.; Szabo, G.; Bor, Z.; Erdei, A.; Szony, B.; et al. Rhinophototherapy: A new therapeutic tool for the management of allergic rhinitis. Allergy Clin. Immunol. 2005, 115, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Hallen, S.; Oliveberg, M.; Brzezinski, P. Light-induced Structural Changes in Cytochrome c Oxidase. Measurements of Electrogenic Events and Absorbance Changes. FEBS Lett. 1993, 318, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Koreck, A.; Csoma, Z.; Ignácz, F.; Bodai, L.; Kadocsa, E.; Szabó, G.; Bor, Z.; Nékám, K.; Dobozy., A.; Kemény, L.; et al. Intranasal phototherapy for the treatment of allergic rhinitis. Orvosi Hetil. 2005, 146, 965–969. [Google Scholar] [CrossRef]
- Kemeny, L.; Koreck, A. Ultraviolet light phototherapy for allergic rhinitis. J. Photochem. Photobiol. B 2007, 87, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Csoma, Z.; Koreck, A.; Ignacz, F.; Bor, Z.; Szabo, G.; Bodai, L.; Dobozy, A.; Kemeny, L.J. PUVA treatment of the nasal cavity improves the clinical symptoms of allergic rhinitis and inhibits the immediate-type hypersensitivity reaction in the skin. Photochem. Photobiol. B 2006, 83, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Cingi, C.; Yaz, A.; Cakli, H.; Ozudogru, E.; Kecik, C.; Bal, C. The effects of phototherapy on quality of life in allergic rhinitis cases. Eur. Arch. Otorhinolaryngol. 2009, 266, 1903–1908. [Google Scholar] [CrossRef] [PubMed]
- Norihero, I.; Katsuura, T.; Kikuchi, Y.; Miwa, E. Effect of far infrared radiation on forearm skin blood flow. Ann. Physiol. Anthropol. 1987, 6, 31–32. [Google Scholar]
- Hu, K.-H.; Li, W.-T. Clinical Effects of Far-Infrared Therapy in Patients with Allergic Rhinitis. In Proceedings of the 29th Annual International Conference of the IEEE EMBS, Lyon, France, 23–26 August 2007; pp. 1479–1482. [Google Scholar]
- Kennedy, R.; Robertson, L. Study on the effect of phototherapy for inhibition of symptoms associated with allergic rhinitis. Eur. Ann. Allergy Clin. Immunol. 2020, 52, 66–73. [Google Scholar] [CrossRef]
- Hu, K.-H.; Li, W.-T. Phototherapy for the Treatment of Allergic Rhinitis; Allergic Rhinitis; Kowalski, M., Ed.; InTech: London, UK, 2012; ISBN 978-953-51-0288-5. Available online: http://www.intechopen.com/books/allergic-rhinitis/photoherapy-for-allergic-rhinitis (accessed on 30 September 2023).
- Brehmer, D. Endonasal phototherapy with Rhinolight for the treatment of allergic rhinitis. Expert. Rev. Med. Devices 2010, 7, 21–26. [Google Scholar] [CrossRef]
- Neuman, I.; Finkelstein, Y. Narrow-band Red Light Phototherapy in Perennial Allergic Rhinitis and Nasal Polyposis. Ann. Allergy Asthma Immunol. 1997, 78, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Tatar, E.Ç.; Korkmaz, H.; Sürenoğlu, U.A.; Saylam, G.; Ozdek, A. Effects of rhinophototherapy on quality of life in persistant allergic rhinitis. Clin. Exp. Otorhinolaryngol. 2013, 6, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Emberlin, J.C.; Lewis, R.A. Pollen challenge study of a phototherapy device for reducing the symptoms of hay fever. Curr. Med. Res. Opin. 2009, 25, 1635–1644. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Nakamura, Y.; Takagi, S.; Sakai, K. Effects of azelastine on the level of serum interleukin-4 and soluble CD23 antigen in the treatment of nasal allergy. Arzneimittelforschung 1998, 48, 1143–1147. [Google Scholar]
- Sliney, D.; Wolbarsht, M. Optical Radiation Hazards to the Skin. In Safety with Lasers and Other Optical Sources; Springer: Boston, MA, USA, 1980. [Google Scholar] [CrossRef]
- Bozkurt, A.; Onaral, B. Safety assessment of near infrared light emitting diodes for diffuse optical measurements. Biomed. Eng. Online 2004, 3, 9. [Google Scholar] [CrossRef]
- Bhattacharya, P.; Fornari, R.; Kamimura, H. Comprehensive Semiconductor Science and Technology, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2011; pp. 154–167, ISBN 9780444531438, eBook ISBN 9780080932286. [Google Scholar]
- Kang, J.-I.; Min, K.-J.; Lee, D.-H. Intranasal Phototherapy for Allergic Rhinitis: A systematic review. J. Korean Med. Ophthalmol. Otolaryngol. Dermatol. 2020, 33, 55–73. [Google Scholar] [CrossRef]
- Bousquet, J.; Van Cauwenberge, P.; Bachert, C.; Canonica, G.W.; Demoly, P.; Durham, S.R.; Fokkens, W.; Lockey, R.J.; Meltzer, E.O.; Mullol, J.; et al. Requirements for medications commonly used in the treatment of allergic rhinitis. European Academy of Allergy and Clinical Immunology (EAACI), Allergic Rhinitis and its Impact on Asthma. Allergy 2003, 58, 165–263. [Google Scholar] [CrossRef] [PubMed]
- Kurowski, M.; Kuna, P.; Górski, P. Montelukast plus cetirizine in the prophylactic treatment of seasonal allergic rhinitis: Influence on clinical symptoms and nasal allergic inflammation. Allergy 2004, 59, 280–288. [Google Scholar] [CrossRef]
- Akhouri, S.; House, S.A. Allergic Rhinitis. [Updated 16 July 2023]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023; Available online: https://www.ncbi.nlm.nih.gov/books/NBK538186/ (accessed on 30 September 2023).
- Britten, N.; Ukoumunne, O.C.; Boulton, M.G. Patients’ attitudes to medicines and expectations for prescriptions. Health Expect. 2002, 5, 256–269. [Google Scholar] [CrossRef]
- Peters-Golden, M.; Gleason, M.M.; Togias, A. Cysteinyl leukotrienes multi-functional mediators in allergic rhinitis. Clin. Exp. Allergy. 2006, 36, 689–703. [Google Scholar] [CrossRef]
- Ramires, R.; Caiaffa, M.F.; Tursi, A.; Haeggstrom, J.Z.; Macchia, L. Novel inhibitory effect on 5-lipoxygenase activity by the anti-asthma drug montelukast. Biochem. Biophys. Res. Commun. 2004, 324, 815–821. [Google Scholar] [CrossRef]
- Anderson, R.; Theron, A.J.; Gravett, C.M.; Steel, H.C.; Tintinger, G.R.; Feldman, C. Montelukast inhibits neutrophil pro-inflammatory activity by a cyclic AMP-dependent mechanism. Br. J. Pharmacol. 2009, 156, 105–115. [Google Scholar] [CrossRef]
- Woszczek, G.; Chen, L.Y.; Alsaaty, S.; Nagineni, S.; Shelhamer, J.H. Concentration-dependent noncysteinyl leukotriene type 1 receptormediated inhibitory activity of leukotriene receptor antagonists. J. Immunol. 2010, 184, 2219–2225. [Google Scholar] [CrossRef]
- Robinson, A.J.; Kashanin, D.; O’Dowd, F.; Williams, V.; Walsh, G.M. Montelukast inhibition of resting and GM-CSF-stimulated eosinophil adhesion to VCAM-1 under flow conditions appears inde-pendent of cysLT(1)R antagonism. J. Leukoc. Biol. 2008, 83, 1522–1529. [Google Scholar] [CrossRef]
- Meliton, A.Y.; Munoz, N.M.; Leff, A.R. Blockade of avidity and focal clustering of beta 2-integrin by cysteinyl leukotriene antagonism attenuates eosinophil adhesion. J. Allergy Clin. Immunol. 2007, 120, 1316–1323. [Google Scholar] [CrossRef]
- Weimer, L.K.; Gamache, D.A.; Yanni, J.M. Histamine-stimulated cytokine secretion from human conjunctival epithelial cells: Inhibition by the histamine H1 antagonist emedastine. Int. Arch. Allergy Immunol. 1998, 115, 288–293. [Google Scholar] [CrossRef]
- Dobashi, K.; Iizuka, K.; Houjou, S.; Sakai, H.; Watanabe, K.; Mori, M.; Nakazawaet, T. Effect of cetirizine on antigen-induced tracheal contraction of passively sensitized guinea pigs. Ann. Allergy Asthma Immunol. 1996, 77, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Anthes, J.C.; Gilchrest, H.; Richard, C.; Eckel, S.; Hesk, D.; West, R.E., Jr.; Williams, S.M.; Greenfeder, S.; Billah, M.; Kreutner, W.; et al. Biochemical characterization of desloratadine, a potent antagonist of the human histamine H(1) receptor. Eur. J. Pharmacol. 2002, 449, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Kanei, A.; Asano, K.; Kanai, K.; Furuta, A.; Sasaki, K.; Suzaki, H. Inhibitory action of levocetirizine on the production of eosinophil chemoattractants RANTES and eotaxin in vitro and in vivo. In Vivo 2014, 28, 657–666. [Google Scholar] [PubMed]
- Kusters, S.; Schuligoi, R.; Huttenbrink, K.B.; Rudert, J.; Wachs, A.; Szelenyi, I.; Peskar, B.A. Effects of antihistamines on leukotriene and cytokine release from dispersed nasal polyp cells. Arzneimittelforschung 2002, 52, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Canonica, G.W.; Blaiss, M. Antihistaminic, anti-inflammatory, and antiallergic properties of the nonsedating second-generation antihistamine desloratadine: A review of the evidence. World Allergy Organ. J. 2011, 4, 47–53. [Google Scholar] [CrossRef]
- Horak, F.; Zieglmayer, U.P. Azelastine nasal spray for the treatment of allergic and nonallergic rhinitis. Expert. Rev. Clin. Immunol. 2009, 5, 659–669. [Google Scholar] [CrossRef]
- Van Hoecke, H.; Vandenbulcke, L.; Van Cauwenberge, P. Histamine and leukotriene receptor antagonism in the treatment of allergic rhinitis: An update. Drugs 2007, 67, 2717–2726. [Google Scholar] [CrossRef]
- Kempuraj, D.; Huang, M.; Kandere-Grzybowska, K.; Basu, S.; Boucher, W.; Letourneau, R.; Athanassiou, A.; Theoharides, T.C. Azelastine inhibits secretion of IL-6, TNF-alpha and IL-8 as well as NF-kappaB activation and intracellular calcium ion levels in normal human mast cells. Int. Arch. Allergy Immunol. 2003, 132, 231–239. [Google Scholar] [CrossRef]
- Matsuo, S.; Takayama, S. Influence of the anti-allergic agent, azelastine, on tumor necrosis factor-alpha (TNF-alpha) secretion from cultured mouse mast cells. In Vivo 1998, 12, 481–484. [Google Scholar] [PubMed]
- Yoneda, K.; Yamamoto, T.; Ueta, E.; Osaki, T. Suppression by azelastine hydrochloride of NF-kappa B activation involved in generation of cytokines and nitric oxide. Jpn. J. Pharmacol. 1997, 73, 145–153. [Google Scholar] [CrossRef]
- Ciprandi, G.; Pronzato, C.; Passalacqua, G.; Ricca, V.; Grogen, J.; Mela, G.S. Topical azelastine reduces eosinophil activation and intercellular adhesion molecule-1 expression on nasal epithelial cells: An antiallergic activity. J. Allergy Clin. Immunol. 1996, 98 Pt 1, 1088–1096. [Google Scholar] [CrossRef]
- Wallace, D.V.; Dykewicz, M.S.; Bernstein, D.I.; Blessing-Moore, J.; Cox, L.; Khan, D.A.; Lang, D.M.; Nicklas, R.A.; Oppenheimer, J.; Portnoy, J.M.; et al. The diagnosis and management of rhinitis: An updated practice parameter. J. Allergy Clin. Immunol. 2008, 122, S1–S84. [Google Scholar] [CrossRef] [PubMed]
- Holm, A.; Dijkstra, M.; Kleinjan, A.; Severijnen, L.A.; Boks, S.; Mulder, P.; Fokkens, W. Fluticasone propionate aqueous nasal spray reduces inflammatory cells in unchallenged allergic nasal mucosa: Effects of single allergen challenge. J. Allergy Clin. Immunol. 2001, 107, 627–633. [Google Scholar] [CrossRef]
- Alvarado-Valdes, C.A.; Blomgren, J.; Weiler, D.; Gleich, G.J.; Reed, C.E.; Field, E.A.; Wisniewski, M.E.; Pobinert, B.F. The effect of fluticasone propionate aqueous nasal spray on eosinophils and cytokines in nasal secretions of patients with ragweed allergic rhinitis. Clin. Ther. 1997, 19, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Weido, A.J.; Reece, L.M.; Alam, R.; Cook, C.K.; Sim, T.C. Intranasal fluticasone propionate inhibits recovery of chemokines and other cytokines in nasal secretions in allergen-induced rhinitis. Ann. Allergy Asthma Immunol. 1996, 77, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Rak, S.; Jacobson, M.R.; Sudderick, R.M.; Masuyama, K.; Juliusson, S.; Kay, A.B.; Hamid, Q.; Löwhagen, O.; Durham, S.R. Influence of prolonged treatment with topical corticosteroid (fluticasone propionate) on early and late phase nasal responses and cellular infiltration in the nasal mucosa after allergen challenge. Clin. Exp. Allergy 1994, 24, 930–939. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, M.; Takizawa, R.; Yokoshima, K.; Okubo, K.; Okuda, M.; Yagi, T. Generation of tumor necrosis factor alpha by human nasal epithelial cells and inhibition by fluticasone propionate. Arerugi 1995, 44, 1216–1222. [Google Scholar] [PubMed]
- Ohnishi, M.; Takizawa, R.; Ohkubo, K.; Yokosima, K.; Okuda, M.; Yagi, T. Fluticasone propionate reduced the production of GM-CSF, IL-6 and IL-8 generated from cultured nasal epithelial cells. Arerugi 1994, 43, 441–447. [Google Scholar]
- Wandalsen, G.F.; Mendes, A.I.; Sole, D. Objective improvement in nasal congestion and nasal hyperreactivity with use of nasal steroids in persistent allergic rhinitis. Am. J. Rhinol. Allergy. 2010. [CrossRef]
- Tovey, E.R.; Liu-Brennan, D.; Garden, F.L.; Oliver, B.G.; Perzanowski, M.S.; Marks, G.B. Time-Based Measurement of Personal Mite Allergen Bioaerosol Exposure over 24 Hour Periods. PLoS ONE 2016, 11, e0153414. [Google Scholar] [CrossRef]
- Van Cauwenberge, P.; Bachert, C.; Passalacqua, G.; Bousquet, J.; Canonica, G.W.; Durham, S.R.; Fokkens, W.J.; Howarth, P.H.; Lund, V.; Malling, H.J.; et al. Consensus statement on the treatment of allergic rhinitis. European Academy of Allergology and Clinical Immunology. Allergy 2000, 55, 116–134. [Google Scholar] [CrossRef]
- Nicholas, C.; Wegienka, G.; Havstad, S.; Ownby, D.; Johnson, C.C. Influence of cat characteristics on Fel d 1 levels in the home. Ann. Allergy Asthma Immunol. 2008, 101, 47–50. [Google Scholar] [CrossRef]
- Nicholas, C.; Wegienka, G.; Havstad, S.; Zoratti, E.; Ownby, D.; Johnson, C.C. Dog characteristics and allergen levels in the home. Ann. Allergy Asthma Immunol. 2010, 105, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Kenney P Hilberg O Laursen AC Peel RG Sigsgaard T Preventive effect of nasal filters on allergic rhinitis: A randomized, double-blind, placebo-controlled crossover park study. J. Allergy Clin. Immunol. 2015, 136, 1566–1572. [CrossRef] [PubMed]
- Wolffsohn, J.S.; Naroo, S.A.; Bilkhu, P.S.; Kennedy, R.; Robertson, L.A. Investigating ocular allergy: Can we determine a better measurement? Clin. Exp. Allergy 2013, 43, 1441. [Google Scholar]
- Dhami, S.; Kakourou, A.; Asamoah, F.; Agache, I.; Lau, S.; Jutel, M.; Muraro, A.; Roberts, G.; Akdis, C.A.; Bonini, M.; et al. Allergen immunotherapy for allergic asthma: A systematic review and meta-analysis. Allergy 2017, 72, 1825–1848. [Google Scholar] [CrossRef] [PubMed]
- Wise, S.K.; Schlosser, R.J. Subcutaneous and sublingual immunotherapy for allergic rhinitis: What is the evidence? Am. J. Rhinol. Allergy 2012, 26, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.; Li, T.; Nelson, H.; Lockey, R. Allergen immunotherapy: A practice parameter second update. J. Allergy Clin. Immunol. 2007, 120, S25–S85. [Google Scholar] [CrossRef]
- Kennedy, R. Phototherapy as a Treatment for Dermatological Diseases, Cancer, Aesthetic Dermatologic Conditions and Allergenic Rhinitis in Adult and Paediatric Medicine. Life 2023, 13, 196. [Google Scholar] [CrossRef]
Figure 1.
Allergenic phases and potential sites for intervention [17].
Figure 1.
Allergenic phases and potential sites for intervention [17].


{kind=link}
Table 1.
Average number of pollen grains in the nostrils (N = 18).
| Uncoated Nostril | Nostril with Pollen Barrier | % Increase | |
|---|---|---|---|
| Grass pollen | 67.3 | 185.7 | 64 |
| Other pollen | 5.7 | 20.3 | 72 |
| Total pollen | 102.4 | 376.9 | 73 |
Table 2.
Main clinical trials showing the effect of phototherapy on allergic rhinitis.
| Study Criteria | Wavelength | Main Effects | Main References |
|---|---|---|---|
| Randomized, single-blind, placebo-controlled study | UVAB (UV-A and UV-B, visible light) | Decrease in the severity of symptoms of nasal obstruction, nasal itching, nasal discharge and sneezing variables (p < 0.001). | [27] |
| Double-blind, placebo-controlled study | UV-B (5%), UV-A (25%) and visible light (70%) | Decrease in severity of allergic rhinitis. | [32] |
| Randomized, double-blind study (49 patients) | mUV/VIS irradiation | Improvement in clinical symptoms of sneezing (p < 0.016), rhinorrhea (p < 0.007), nasal itching (p < 0.014) and total nasal score (p < 0.004). | [22] |
| A blind, placebo-controlled study | Visible light (mUV/VIS) and infrared light (660 nm 940 nm) | Significantly improved nasal symptoms of allergic rhinitis arising from exposure to indoor and outdoor allergens. | [30] |
| Double-blind, randomized prospective study (50 patients) | Intranasal illumination at 660 nm for 4.4 min three times a day for 14 days | Improvement in symptoms was reported by 72% of the allergic rhinitis patients. | [33] |
| Randomized study (65 Patients) | Visible light, ultraviolet A and ultraviolet B | Improvements in all variables of the quality of life—nasal symptom scores and VAS were statistically significant. | [34] |
| Randomized, double-blind study | Low-dose UVB, low-dose UVA and visible light | Reduced symptom scores for sneezing, rhinorrhea, nasal itching and the total nasal score in ragweed allergic patients. | [25] |
| Randomized into the treatment group (phototherapy was performed once a day for 7 days) and control group (antihistamine once a day for 7 days) | Phototherapy with LEDs consisting of two wavelengths, 660 and 850 nm | Significant improvements were observed in all of the symptoms of AR patients. | [31] |
| Double-blind, placebo-controlled grass pollen challenge | Red and infrared spectra: 652 nm and 940 nm | Significant reductions in severity of symptom scores were found for sneezing, running nose, running eyes and itchy mouth/palate (p < or =0.05). | [35] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kennedy, R. Mechanisms and Comparative Treatments of Allergic Rhinitis including Phototherapy. Allergies 2024, 4, 17-29. https://doi.org/10.3390/allergies4010002
AMA Style
Kennedy R. Mechanisms and Comparative Treatments of Allergic Rhinitis including Phototherapy. Allergies. 2024; 4(1):17-29. https://doi.org/10.3390/allergies4010002
Chicago/Turabian StyleKennedy, Roy. 2024. "Mechanisms and Comparative Treatments of Allergic Rhinitis including Phototherapy" Allergies 4, no. 1: 17-29. https://doi.org/10.3390/allergies4010002