

Highlighting Hemodynamic Risks for Bioresorbable Stents in Coronary Arteries

Abstract
:1. Introduction
2. Methods
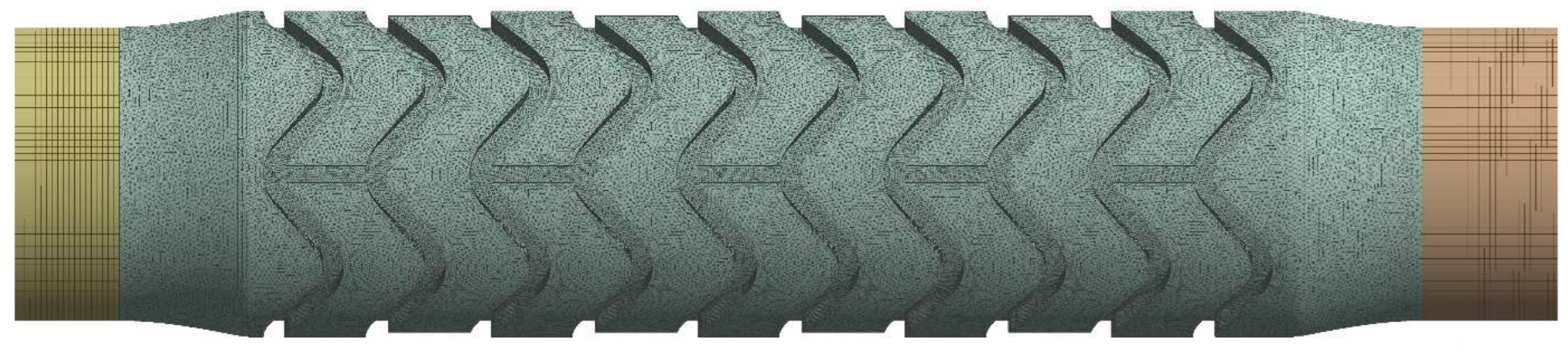
2.1. Fluid Domain Geometry
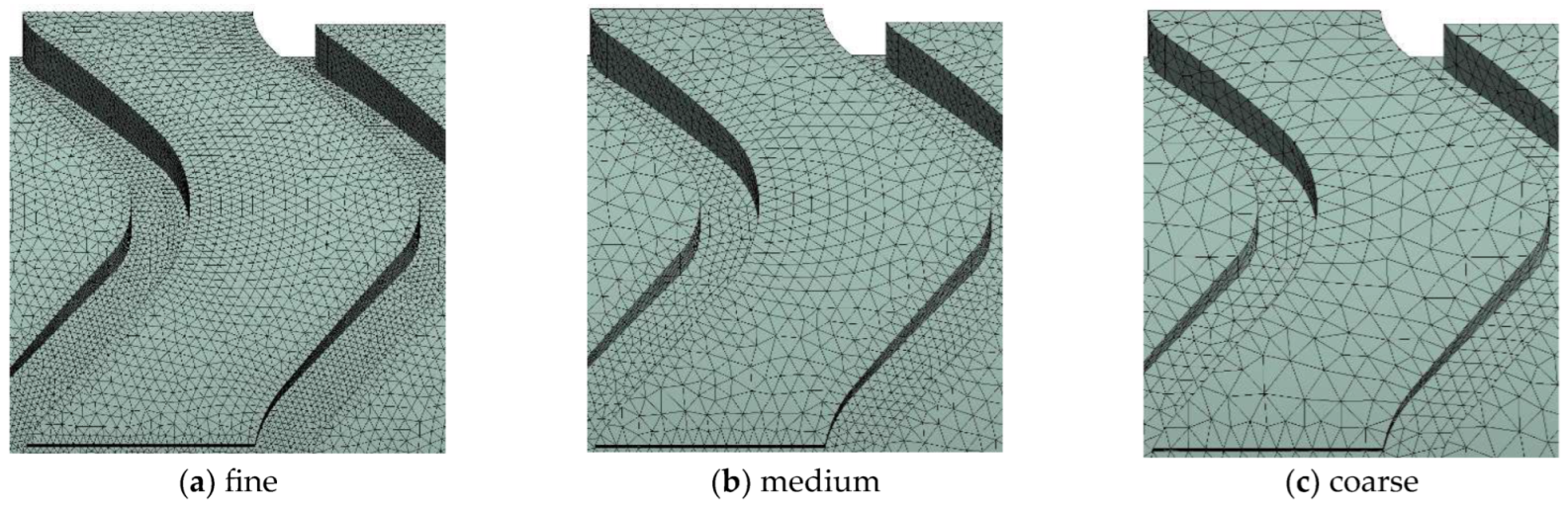
2.2. Mesh Generation
Grid Convergence Analysis
2.3. Fluid Properties
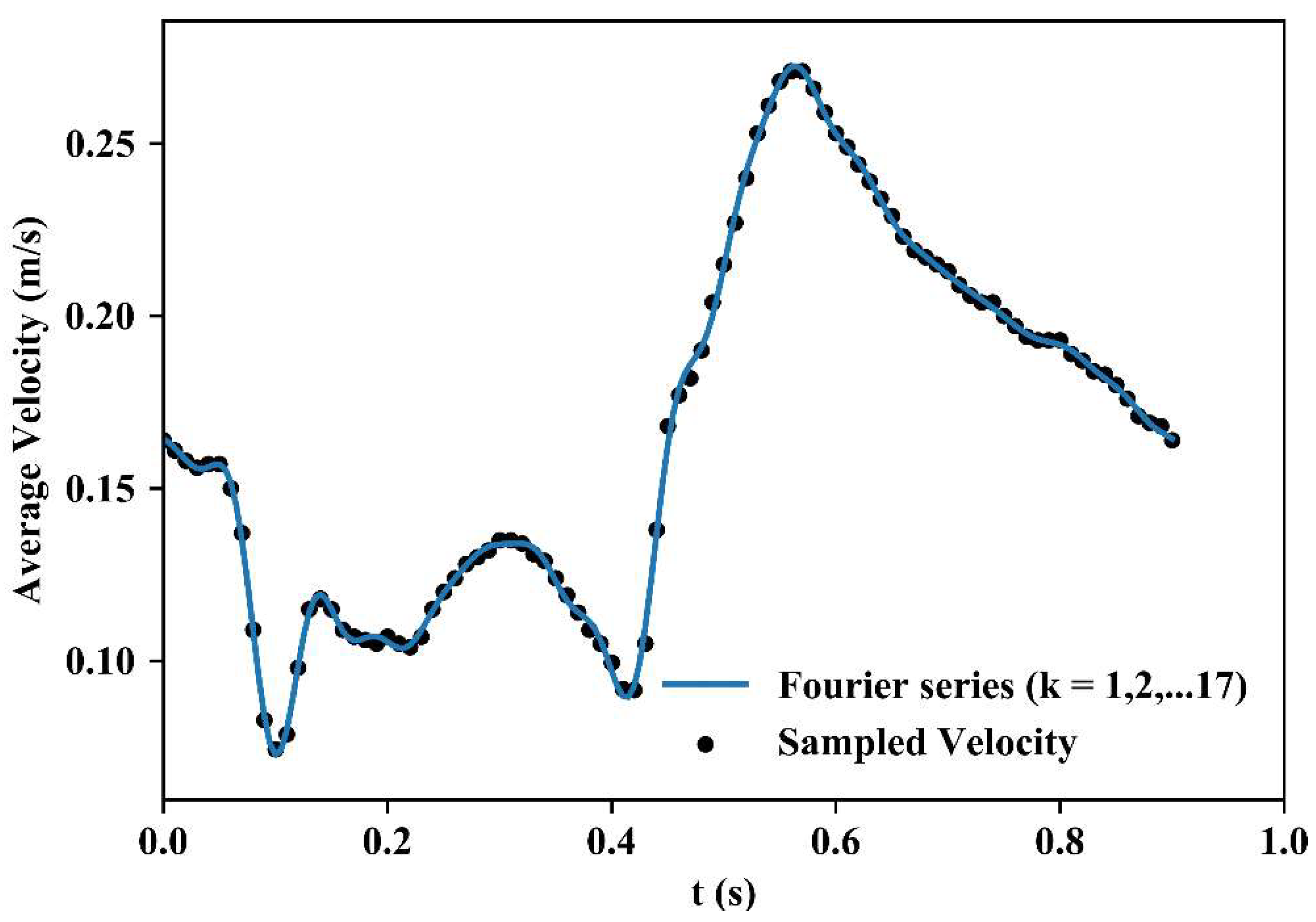
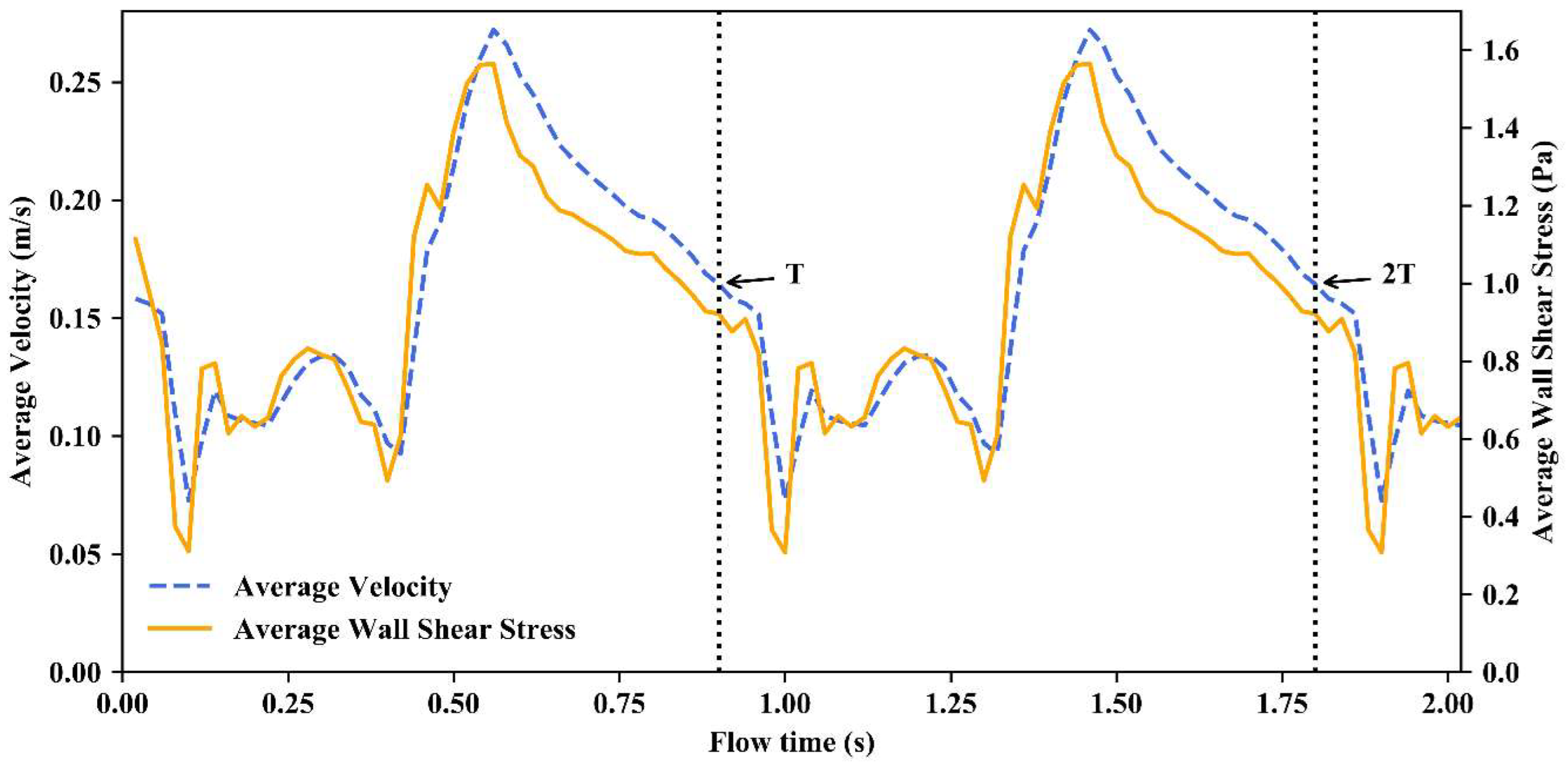
2.4. Boundary Conditions
2.5. Simulation
2.6. Calculation of Parameters to Evaluate Risk
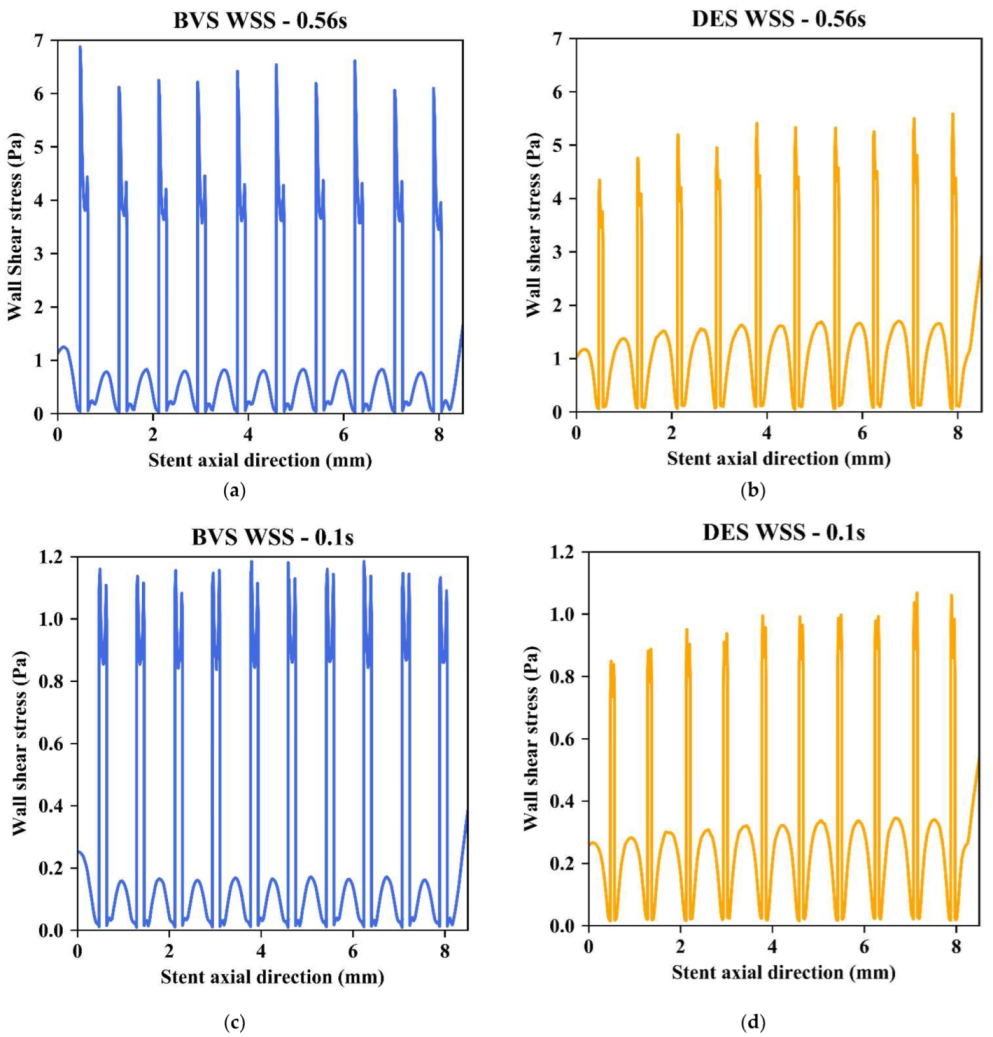
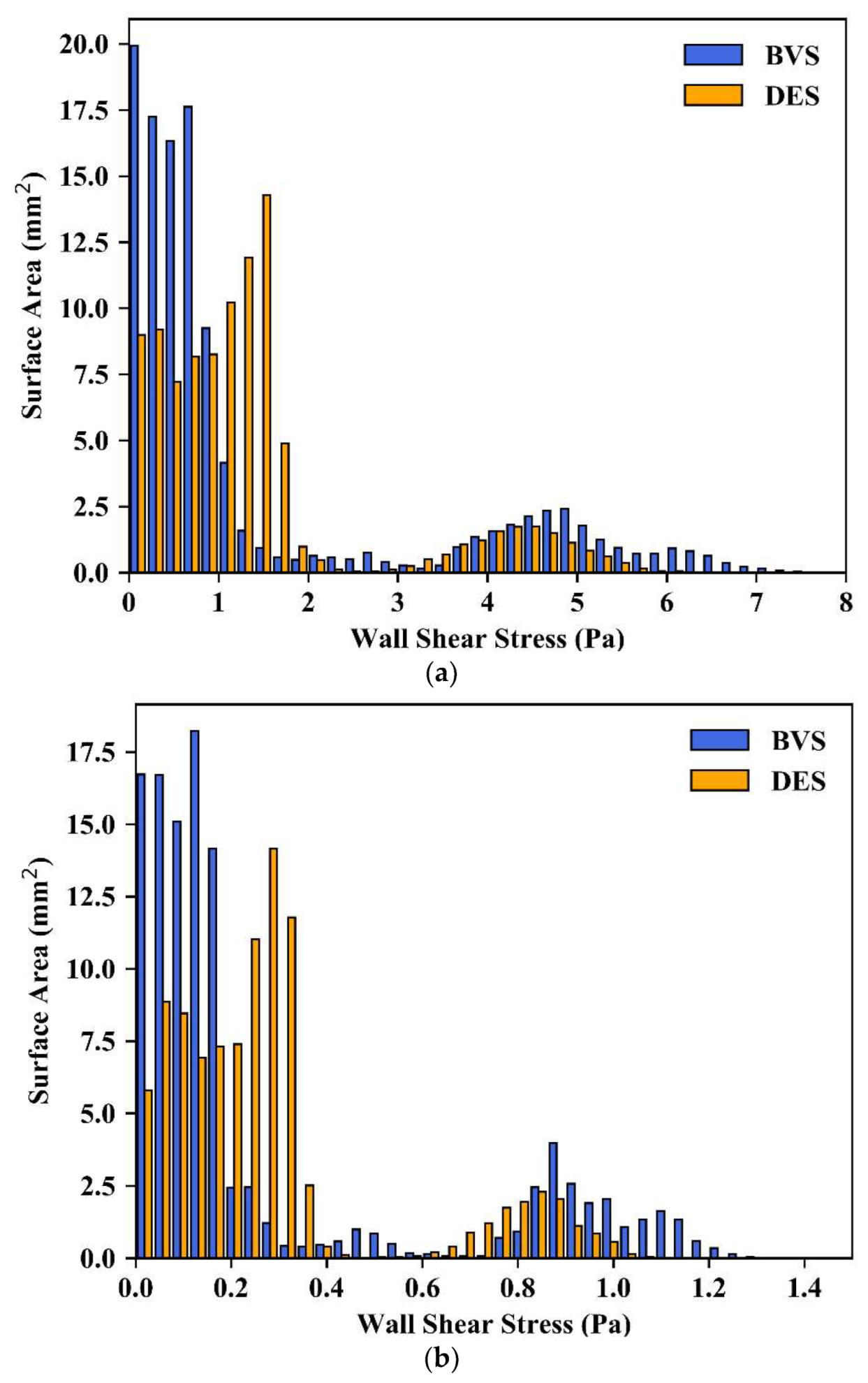
2.6.1. Instantaneous Wall Shear Stress
2.6.2. Time-Averaged Wall Shear Stress
2.6.3. Oscillatory Shear Index
2.6.4. Relative Residence Time
2.6.5. Shear Rate
3. Results
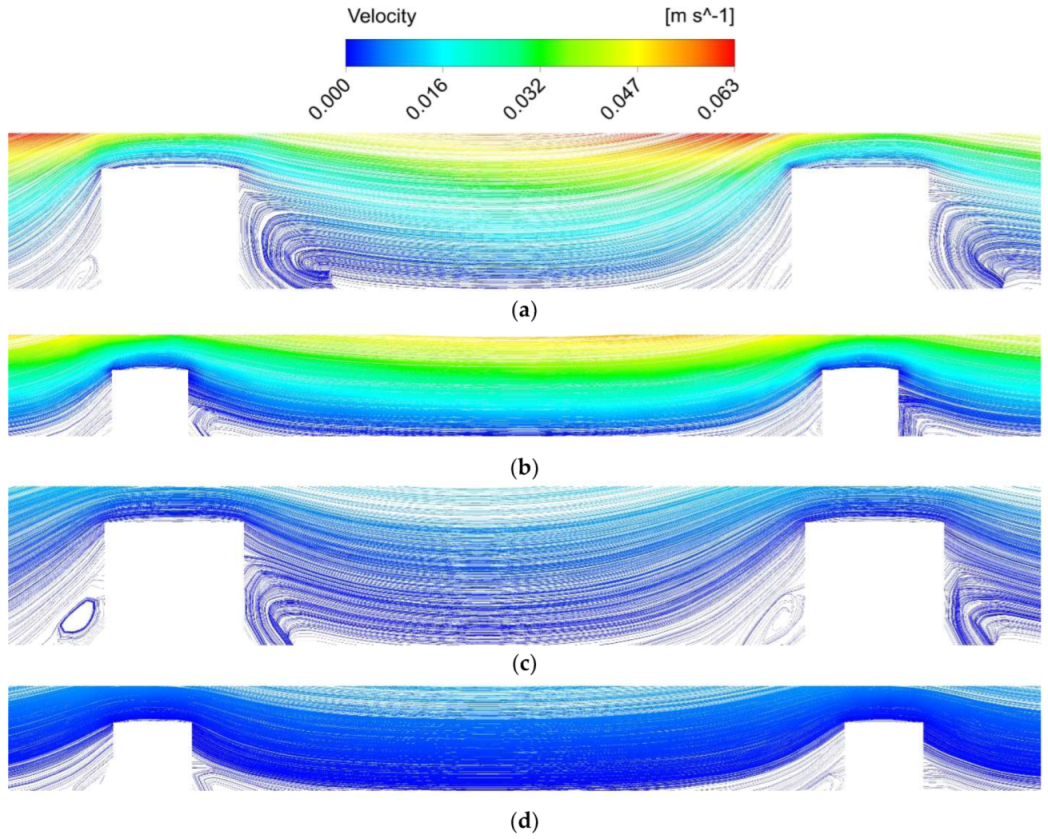
3.1. Instantaneous Flow Characteristics
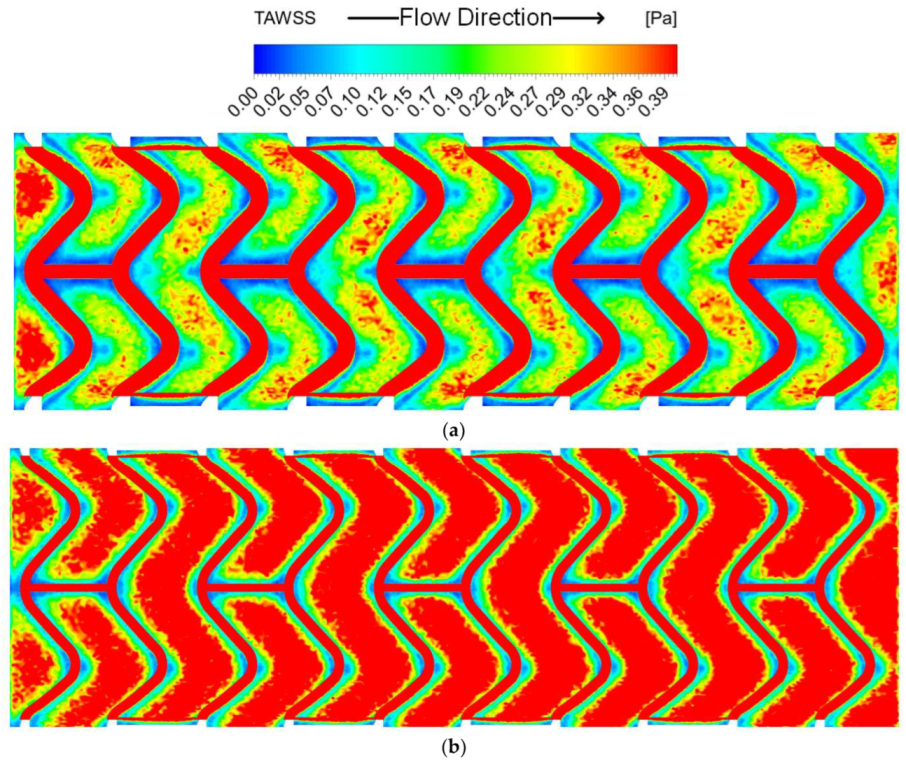
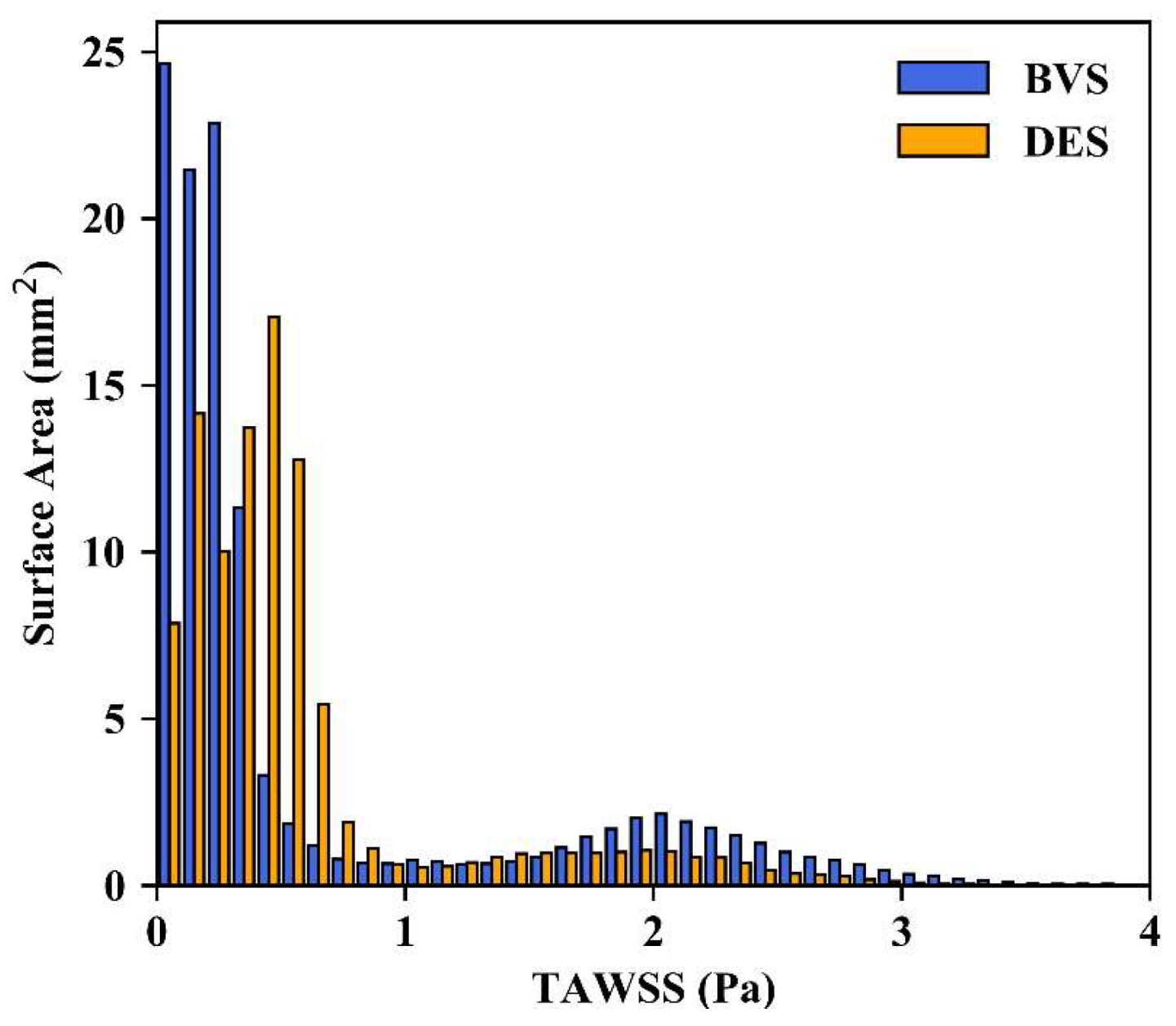
3.2. Time-Averaged Wall Shear Stress
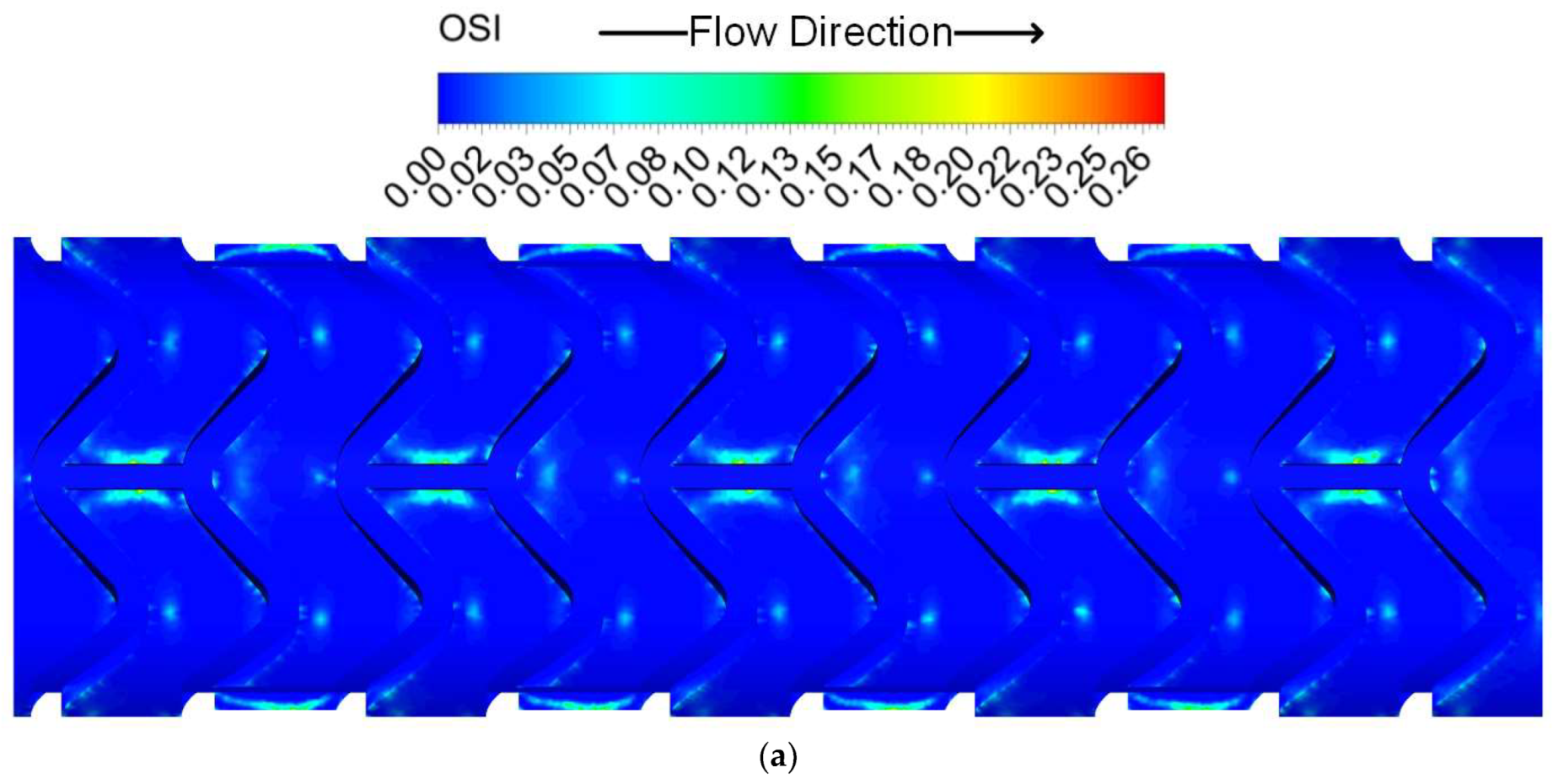
3.3. Oscillatory Shear Index
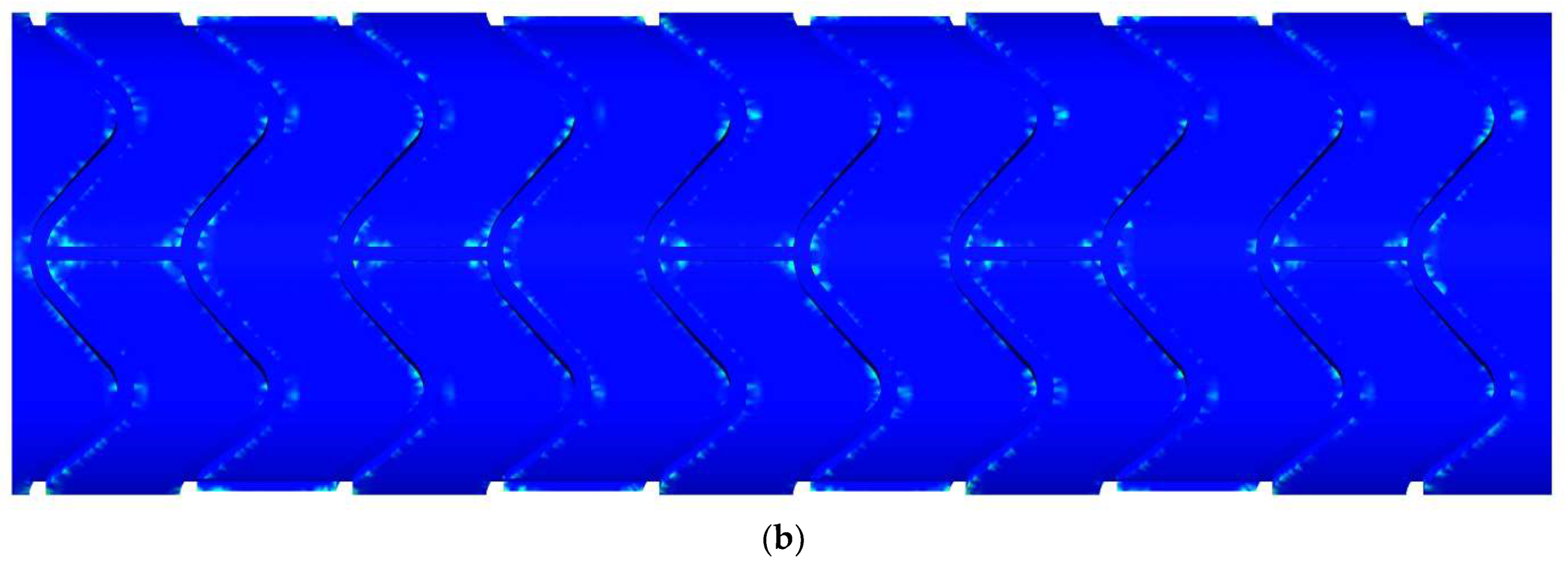
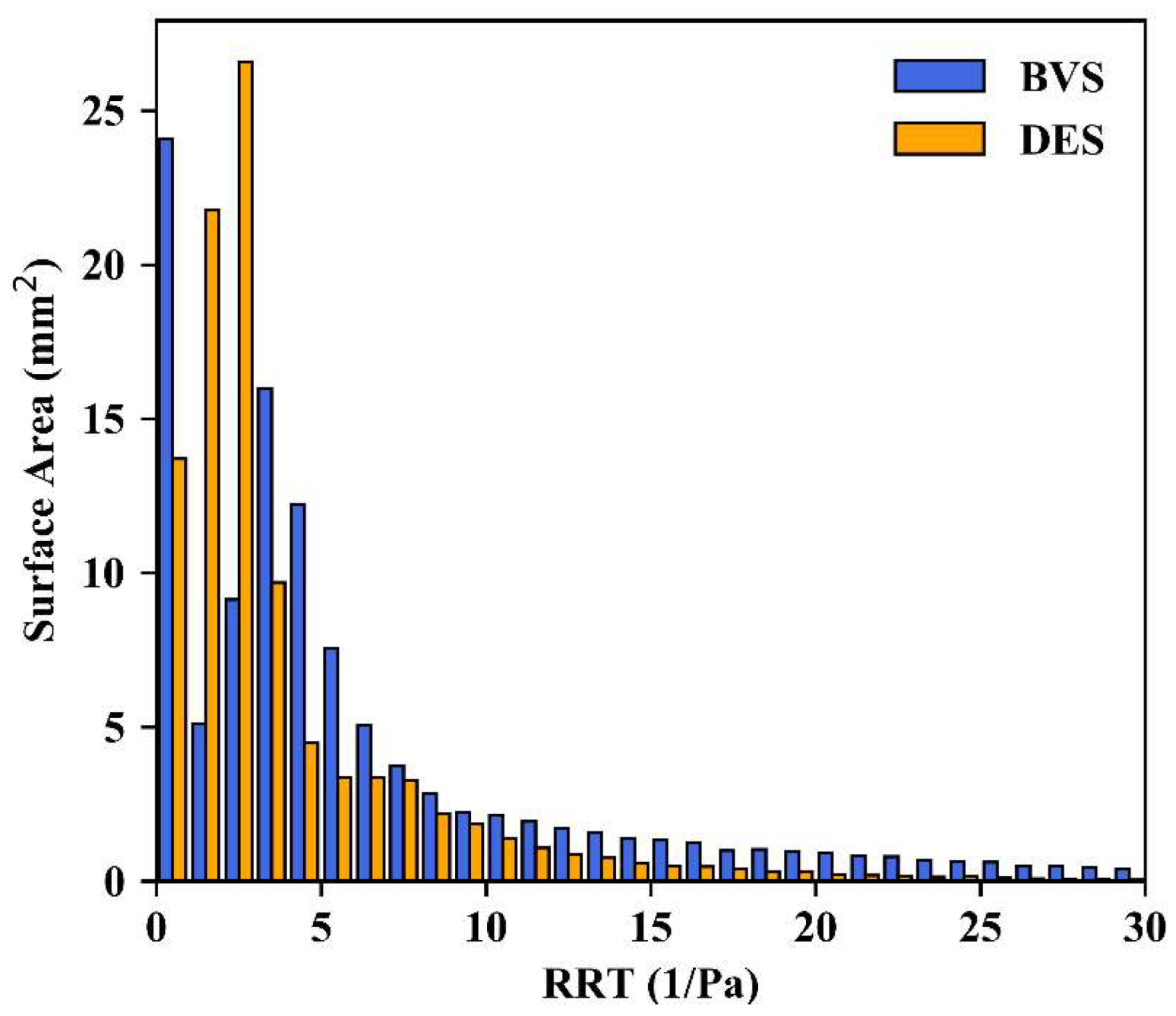
3.4. Relative Residence Time
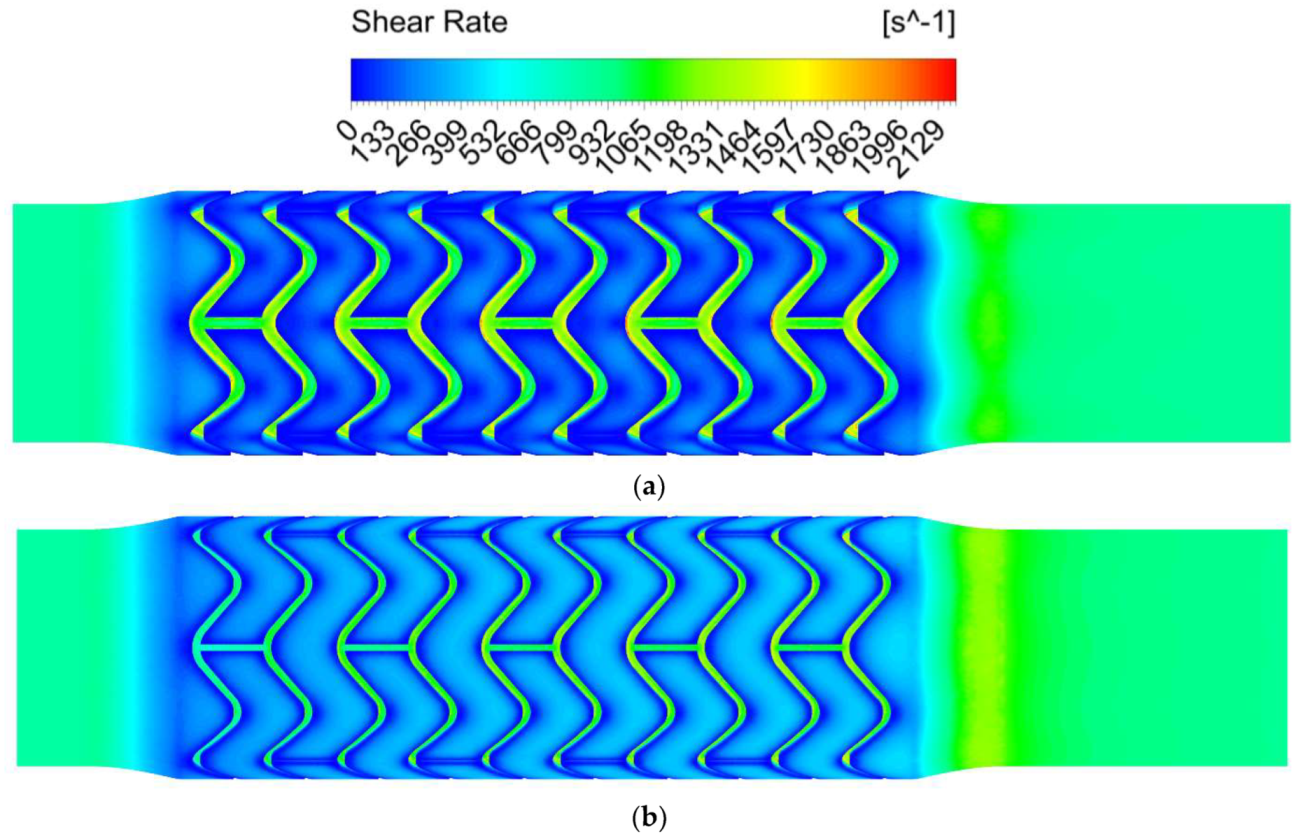
3.5. Shear Rate
4. Discussion
Comparison of Simulation Results with Existing Work
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Falk, E. Pathogenesis of atherosclerosis. J. Am. Coll. Cardiol. 2006, 47, C7–C12. [Google Scholar] [CrossRef] [PubMed]
- British Heart Foundation. Heart and Circulatory Disease Statistics 2023. Available online: https://www.bhf.org.uk/what-we-do/our-research/heart-statistics/heart-statistics-publications/cardiovascular-disease-statistics-2023 (accessed on 9 August 2023).
- Verdonck, P. Advances in Biomedical Engineering, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Stone, G.W.; Moses, J.W.; Ellis, S.G.; Schofer, J.; Dawkins, K.D.; Morice, M.-C.; Colombo, A.; Schampaert, E.; Grube, E.; Kirtane, A.J.; et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N. Engl. J. Med. 2007, 356, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Kereiakes, D.J.; Onuma, Y.; Serruys, P.W.; Stone, G.W. Bioresorbable vascular scaffolds for coronary revascularization. Circulation 2016, 134, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Onuma, Y.; Serruys, P.W. Bioresorbable scaffold: The advent of a new era in percutaneous coronary and peripheral revascularization? Circulation 2011, 123, 779–797. [Google Scholar] [CrossRef] [PubMed]
- Ormiston, J.A.; Serruys, P.W.S. Bioabsorbable coronary stents. Circ. Cardiovasc. Interv. 2009, 2, 255–260. [Google Scholar] [CrossRef]
- Indolfi, C.; De Rosa, S.; Colombo, A. Bioresorbable vascular scaffolds—basic concepts and clinical outcome. Nat. Rev. Cardiol. 2016, 13, 719–729. [Google Scholar] [CrossRef]
- Ali, Z.A.; Gao, R.; Kimura, T.; Onuma, Y.; Kereiakes, D.J.; Ellis, S.G.; Chevalier, B.; Vu, M.-T.; Zhang, Z.; Simonton, C.A.; et al. Three-year outcomes with the Absorb bioresorbable scaffold: Individual-patient-data meta-analysis from the ABSORB randomized trials. Circulation 2018, 137, 464–479. [Google Scholar] [CrossRef]
- Capodanno, D.; Buccheri, S.; Romano, S.; Capranzano, P.; Francaviglia, B.; Tamburino, C. Decision analytic Markov model weighting expected benefits and current limitations of first-generation bioresorbable vascular scaffolds. Circ. Cardiovasc. Interv. 2018, 11, e005768. [Google Scholar] [CrossRef]
- Bangalore, S.; Bezerra, H.G.; Rizik, D.G.; Armstrong, E.J.; Samuels, B.; Naidu, S.S.; Grines, C.L.; Foster, M.T.; Choi, J.W.; Bertolet, B.D.; et al. The state of the Absorb bioresorbable scaffold: Consensus from an expert panel. J. Am. Coll. Cardiol. Interv. 2017, 10, 2349–2359. [Google Scholar] [CrossRef]
- Serruys, P.W.; Revaiah, P.C.; Onuma, Y. Bioresorbable scaffolds: Is there still light at the end of the tunnel? J. Am. Coll. Cardiol. 2023, 82, 196–199. [Google Scholar] [CrossRef]
- Wang, P.-J.; Ferralis, N.; Conway, C.; Grossman, J.C.; Edelman, E.R. Strain-induced accelerated asymmetric spatial degradation of polymeric vascular scaffolds. Proc. Natl. Acad. Sci. USA 2018, 115, 2640–2645. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.-J.; Nezami, F.R.; Gorji, M.B.; Berti, F.; Petrini, L.; Wierzbicki, T.; Migliavacca, F.; Edelman, E.R. Effect of working environment and procedural strategies on mechanical performance of bioresorbable vascular scaffolds. Acta Biomater. 2018, 82, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Bangalore, S.; Edelman, E.R.; Bhatt, D.L. First-generation bioresorbable vascular scaffolds. Disappearing stents or disappearing evidence? J. Am. Coll. Cardiol. 2017, 69, 3067–3069. [Google Scholar] [CrossRef] [PubMed]
- Lafont, A.; Mennuni, M.G. What happened to the bioresorbable scaffold concept? Circ. Cardiovasc. Interv. 2018, 11, e006283. [Google Scholar] [CrossRef] [PubMed]
- Glagov, S.; Zarins, C.K.; Giddens, D.P.; Ku, D.N. Hemodynamics and atherosclerosis. Insights and perspectives gained from studies of human arteries. Arch. Pathol. Lab. Med. 1988, 112, 1018–1031. [Google Scholar] [PubMed]
- Asakura, T.; Karino, T. Flow patterns and spatial distribution of atherosclerotic lesions in human coronary arteries. Circ. Res. 1990, 66, 1045–1066. [Google Scholar] [CrossRef]
- Kohler, T.R.; Kirkman, T.R.; Kraiss, L.W.; Zierler, B.K.; Clowes, A.W. Increased blood flow inhibits neointimal hyperplasia in endothelialized vascular grafts. Circ. Res. 1991, 69, 1557–1565. [Google Scholar] [CrossRef]
- Wentzel, J.J.; Krams, R.; Schuurbiers, J.C.H.; Oomen, J.A.; Kloet, J.; van der Giessen, W.J.; Serruys, P.W.; Slager, C.J. Relationship between neointimal thickness and shear stress after wallstent implantation in human coronary arteries. Circulation 2001, 103, 1740–1745. [Google Scholar] [CrossRef]
- LaDisa, J.F.; Olson, L.E.; Molthen, R.C.; Hettrick, D.A.; Pratt, P.F.; Hardel, M.D.; Kersten, J.R.; Warltier, D.C.; Pagel, P.S. Alterations in wall shear stress predict sites of neointimal hyperplasia after stent implantation in rabbit iliac arteries. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H2465–H2475. [Google Scholar] [CrossRef]
- Gay, M.; Zhang, L.T. Numerical studies on fluid-structure interactions of stent deployment and stented arteries. Eng. Comput. 2009, 25, 61–72. [Google Scholar] [CrossRef]
- Sakariassen, K.S.; Orning, L.; Turitto, V.T. The impact of blood shear rate on arterial thrombus formation. Future Sci. OA 2015, 1, FSO30. [Google Scholar] [CrossRef] [PubMed]
- Casa, L.D.C.; Deaton, D.H.; Ku, D.N. Role of high shear rate in thrombosis. J. Vasc. Surg. 2015, 61, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Caiazzo, G.; Kilic, I.D.; Fabris, E.; Serdoz, R.; Mattesini, A.; Foin, N.; de Rosa, S.; Indolfi, C.; di Mario, C. Absorb bioresorbable vascular scaffold: What have we learned after 5 years of clinical experience? Int. J. Cardiol. 2015, 201, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Chiastra, C.; Migliavacca, F.; Martínez, M.A.; Malve, M. On the necessity of modelling fluid-structure interaction for stented coronary arteries. J. Mech. Behav. Biomed. Mater. 2014, 34, 217–230. [Google Scholar] [CrossRef]
- Abbott Vascular. Absorb GT1TM Bioresorbable Vascular Scaffold (BVS) System, Instructions for Use; Abbott Vascular: Santa Clara, CA, USA, 2016. [Google Scholar]
- Brugaletta, S.; Gomez-Lara, J.; Diletti, R.; Farooq, V.; van Geuns, R.J.; de Bruyne, B.; Dudek, D.; Garcia-Garcia, H.M.; Ormiston, J.A.; Serruys, P.W. Comparison of in vivo eccentricity and symmetry indices between metallic stents and bioresorbable vascular scaffolds: Insights from the ABSORB and SPIRIT trials. Catheter. Cardiovasc. Interv. 2012, 79, 219–228. [Google Scholar] [CrossRef]
- Kolandaivelu, K.; Swaminathan, R.; Gibson, W.J.; Kolachalama, V.B.; Nguyen-Ehrenreich, K.-L.; Giddings, V.L.; Coleman, L.; Wong, G.K.; Edelman, E.R. Stent thrombogenicity early in high-risk interventional settings is driven by stent design and deployment and protected by polymer-drug coatings. Circulation 2011, 123, 1400–1409. [Google Scholar] [CrossRef]
- Hsiao, H.-M.; Lee, K.-H.; Liao, Y.-C.; Cheng, Y.-C. Cardiovascular stent design and wall shear stress distribution in coronary stented arteries. Micro Nano Lett. 2012, 7, 430–433. [Google Scholar] [CrossRef]
- Stiehm, M.; Brede, M.; Quosdorf, D.; Martin, H.; Leder, A. A sensitivity analysis of stent design parameters using CFD. Biomed. Tech. 2013, 58, SI-1-Track-N. [Google Scholar] [CrossRef]
- Briguori, C.; Sarais, C.; Pagnotta, P.; Liistro, F.; Montorfano, M.; Chieffo, A.; Sgura, F.; Corvaja, N.; Albiero, R.; Stankovic, G.; et al. In-stent restenosis in small coronary arteries: Impact of strut thickness. J. Am. Coll. Cardiol. 2002, 40, 403–409. [Google Scholar] [CrossRef]
- Foin, N.; Lee, R.D.; Torii, R.; Guitierrez-Chico, J.L.; Mattesini, A.; Nijjer, S.; Sen, S.; Petraco, R.; Davies, J.E.; di Mario, C.; et al. Impact of stent strut design in metallic stents and biodegradable scaffolds. Int. J. Cardiol. 2014, 177, 800–808. [Google Scholar] [CrossRef]
- Kays, W.M.; Crawford, M.E. Convective Heat and Mass Transfer, 3rd ed.; McGraw-Hill: New York, NY, USA, 1993. [Google Scholar]
- Chiastra, C.; Morlacchi, S.; Pereira, S.; Dubini, G.; Migliavacca, F. Computational fluid dynamics of stented coronary bifurcations studied with a hybrid discretization method. Eur. J. Mech. B Fluids 2012, 35, 76–84. [Google Scholar] [CrossRef]
- Roache, P.J. Quantification of uncertainty in computational fluid dynamics. Annu. Rev. Fluid Mech. 1997, 29, 123–160. [Google Scholar] [CrossRef]
- Oberkampf, W.L.; Roy, C.J. Verification and Validation in Scientific Computing, 1st ed.; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Slater, J.W. Examining Spatial (Grid) Convergence. Available online: http://www.grc.nasa.gov/WWW/wind/valid/tutorial/spatconv.html (accessed on 25 October 2018).
- Merrill, E.W. Rheology of blood. Physiol. Rev. 1969, 49, 863–888. [Google Scholar] [CrossRef] [PubMed]
- Soulis, J.V.; Giannoglou, G.D.; Chatzizisis, Y.S.; Seralidou, K.V.; Parcharidis, G.E.; Louridas, G.E. Non-Newtonian models for molecular viscosity and wall shear stress in a 3D reconstructed human left coronary artery. Med. Eng. Phys. 2008, 30, 9–19. [Google Scholar] [CrossRef]
- Davies, J.E.; Whinnett, Z.I.; Francis, D.P.; Manisty, C.H.; Aguado-Sierra, J.; Willson, K.; Foale, R.A.; Malik, I.S.; Hughes, A.D.; Parker, K.H.; et al. Evidence of a dominant backward-propagating “suction” wave responsible for diastolic coronary filling in humans, attenuated in left ventricular hypertrophy. Circulation 2006, 113, 1768–1778. [Google Scholar] [CrossRef] [PubMed]
- Ni, M.-J.; Abdou, M.A. Temporal second-order accuracy of simple-type methods for incompressible unsteady flows. Numer. Heat Transf. Part B 2004, 46, 529–548. [Google Scholar] [CrossRef]
- Ku, D.N.; Giddens, D.P.; Zarins, C.K.; Glagov, S. Pulsatile flow and atherosclerosis in the human carotid bifurcation. Positive correlation between plaque location and low and oscillating shear stress. Arteriosclerosis 1985, 5, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Himburg, H.A.; Grzybowski, D.M.; Hazel, A.L.; LaMack, J.A.; Li, X.-M.; Friedman, M.H. Spatial comparison between wall shear stress measures and porcine arterial endothelial permeability. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H1916–H1922. [Google Scholar] [CrossRef]
- Suess, T.; Anderson, J.; Danielson, L.; Pohlson, K.; Remund, T.; Blears, E.; Gent, S.; Kelly, P. Examination of near-wall hemodynamic parameters in the renal bridging stent of various stent graft configurations for repairing visceral branched aortic aneurysms. J. Vasc. Surg. 2016, 64, 788–796. [Google Scholar] [CrossRef]
- Morbiducci, U.; Gallo, D.; Massai, D.; Consolo, F.; Ponzini, R.; Antiga, L.; Bignardi, C.; Deriu, M.A.; Redaelli, A. Outflow conditions for image-based hemodynamic models of the carotid bifurcation: Implications for indicators of abnormal flow. J. Biomech. Eng. 2010, 132, 091005. [Google Scholar] [CrossRef]
- Barstad, R.M.; Roald, H.E.; Cui, Y.; Turitto, V.T.; Sakariassen, K.S. A perfusion chamber developed to investigate thrombus formation and shear profiles in flowing native human blood at the apex of well-defined stenosis. Arterioscler. Thromb. 1994, 14, 1984–1991. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Kereiakes, D.J.; Gori, T.; Metzger, D.C.; Stein, B.; Erickson, M.; Torzewski, J.; Kabour, A.; Piegari, G.; Cavendish, J.; et al. 5-year outcomes after bioresorbable coronary scaffolds implanted with improved technique. J. Am. Coll. Cardiol. 2023, 82, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Ding, Z.; Piana, R.N.; Gehrig, T.R.; Friedman, M.H. Cataloguing the geometry of the human coronary arteries: A potential tool for predicting risk of coronary artery disease. Int. J. Cardiol. 2009, 135, 43–52. [Google Scholar] [CrossRef]
- de Nisco, G.; Kok, A.M.; Chiastra, C.; Gallo, D.; Hoogendoorn, A.; Migliavacca, F.; Wentzel, J.J.; Morbiducci, U. The atheroprotective nature of helical flow in coronary arteries. Ann. Biomed. Eng. 2019, 47, 425–438. [Google Scholar] [CrossRef] [PubMed]
- de Nisco, G.; Hoogendoorn, A.; Chiastra, C.; Gallo, D.; Kok, A.M.; Morbiducci, U.; Wentzel, J.J. The impact of helical flow on coronary atherosclerotic plaque development. Atherosclerosis 2020, 300, 39–46. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter Stent Design | Fine | Medium | Coarse | |||
|---|---|---|---|---|---|---|
| BVS | DES | BVS | DES | BVS | DES | |
| Mesh elements | 2,681,415 | 2,695,283 | 659,490 | 646,258 | 196,442 | 193,516 |
| Mesh nodes | 1,354,050 | 1,344,475 | 346,514 | 339,487 | 108,203 | 106,269 |
| 1 | 1 | 1.575 | 1.582 | 1.474 | 1.473 | |
| Global element size | 0.045 mm | 0.0719 mm | 0.11 mm | |||
| Stent region element size | 0.0375 mm | 0.0625 mm | 0.1 mm | |||
| Stent face element size | 0.0188 mm | 0.0313 mm | 0.05 mm | |||
| Mesh | AWA WSS (Pa) | %Decrease in AWA WSS as Mesh Refined | GCI | |||
|---|---|---|---|---|---|---|
| BVS | DES | BVS | DES | BVS | DES | |
| Fine | 1.365 | 1.349 | 0.51% | 1.24% | 0.483% | 1.58% |
| Medium | 1.372 | 1.366 | 0.94% | 1.94% | 1.121% | 3.118% |
| Coarse | 1.385 | 1.393 | NA | NA | NA | NA |
| Parameter | Risk Threshold |
|---|---|
| /TAWSS | <0.4 Pa |
| OSI | >0.3 |
| RRT | >10 Pa−1 |
| Shear rate | >5000 s−1 |
| Finding | %Occurrence | Random-Effect RR (95% Confidence Interval) | |
|---|---|---|---|
| Absorb BVS | Xience DES | ||
| Target lesion failure | 11.7% | 8.1% | 1.37 (1.09–1.72) |
| Target vessel myocardial infarction | 7.8% | 4.2% | 1.68 (1.23–2.29) |
| Ischaemia-driven target lesion revascularisation | 6.6% | 4.4% | 1.41 (1.03–1.93) |
| Device thrombosis | 2.4% | 0.6% | 2.83 (1.27–6.31) |
| Parameter | At-Risk Area (mm2) | %Increase in Risk Area | ||
|---|---|---|---|---|
| BVS | DES | ∆ | ||
| < 0.4 Pa—minimum velocity | 88.1 | 84.5 | 3.6 | 4.3% |
| < 0.4 Pa—maximum velocity | 37.2 | 18.2 | 19 | 104% |
| TAWSS < 0.4 Pa | 80.4 | 44.1 | 36.3 | 82.3% |
| OSI > 0.3 | 0 | 0 | 0 | 0% |
| RRT > 10 Pa−1 | 25.5 | 7.5 | 18 | 240% |
| Shear rate > 5000 s−1 | 0 | 0 | 0 | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elliott, M.S.; Cole, J.S.; Blair, R.W.; Menary, G.H. Highlighting Hemodynamic Risks for Bioresorbable Stents in Coronary Arteries. Fluids 2023, 8, 241. https://doi.org/10.3390/fluids8090241
Elliott MS, Cole JS, Blair RW, Menary GH. Highlighting Hemodynamic Risks for Bioresorbable Stents in Coronary Arteries. Fluids. 2023; 8(9):241. https://doi.org/10.3390/fluids8090241
Chicago/Turabian StyleElliott, Marcus S., Jonathan S. Cole, Ross W. Blair, and Gary H. Menary. 2023. "Highlighting Hemodynamic Risks for Bioresorbable Stents in Coronary Arteries" Fluids 8, no. 9: 241. https://doi.org/10.3390/fluids8090241