
CFD to Quantify Idealized Intra-Aneurysmal Blood Flow in Response to Regular and Flow Diverter Stent Treatment


Abstract
:1. Introduction
2. Materials and Methods
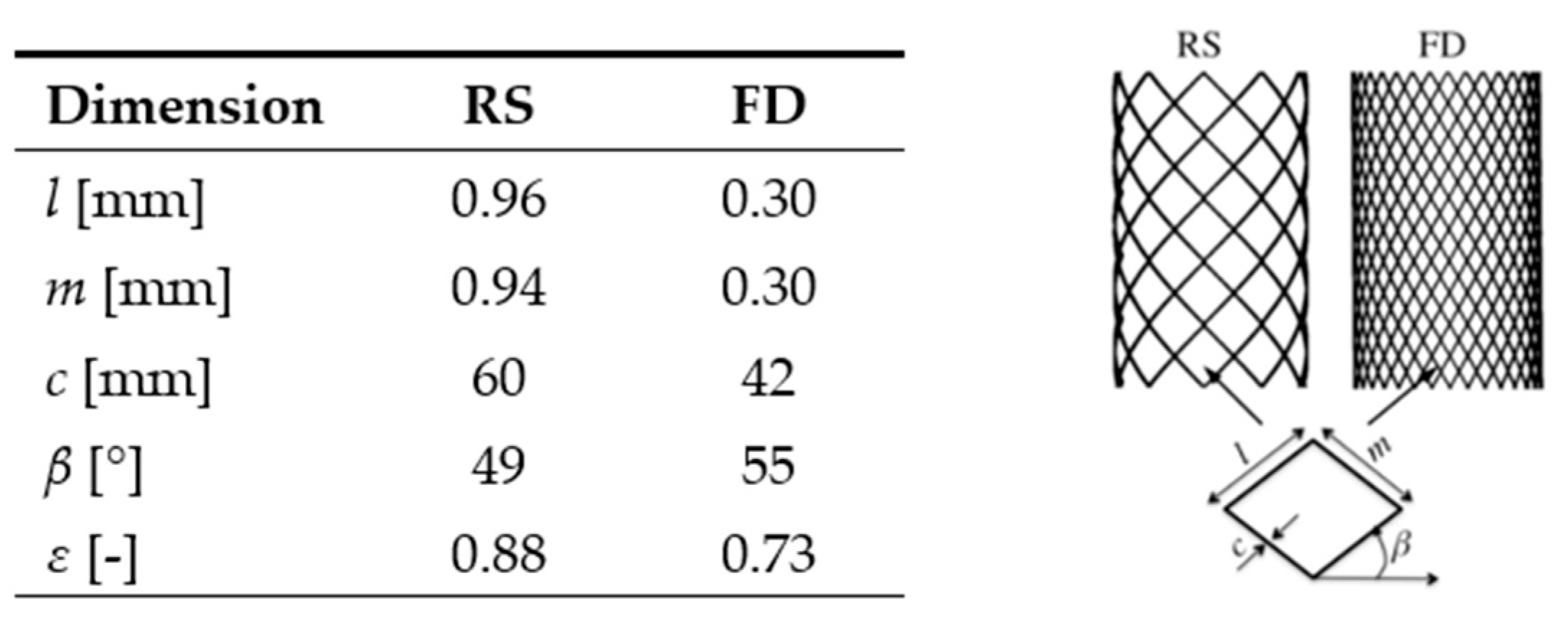
2.1. Vascular Modeling and Stent Geometry
2.2. Numerical Grid and Mathematical Model
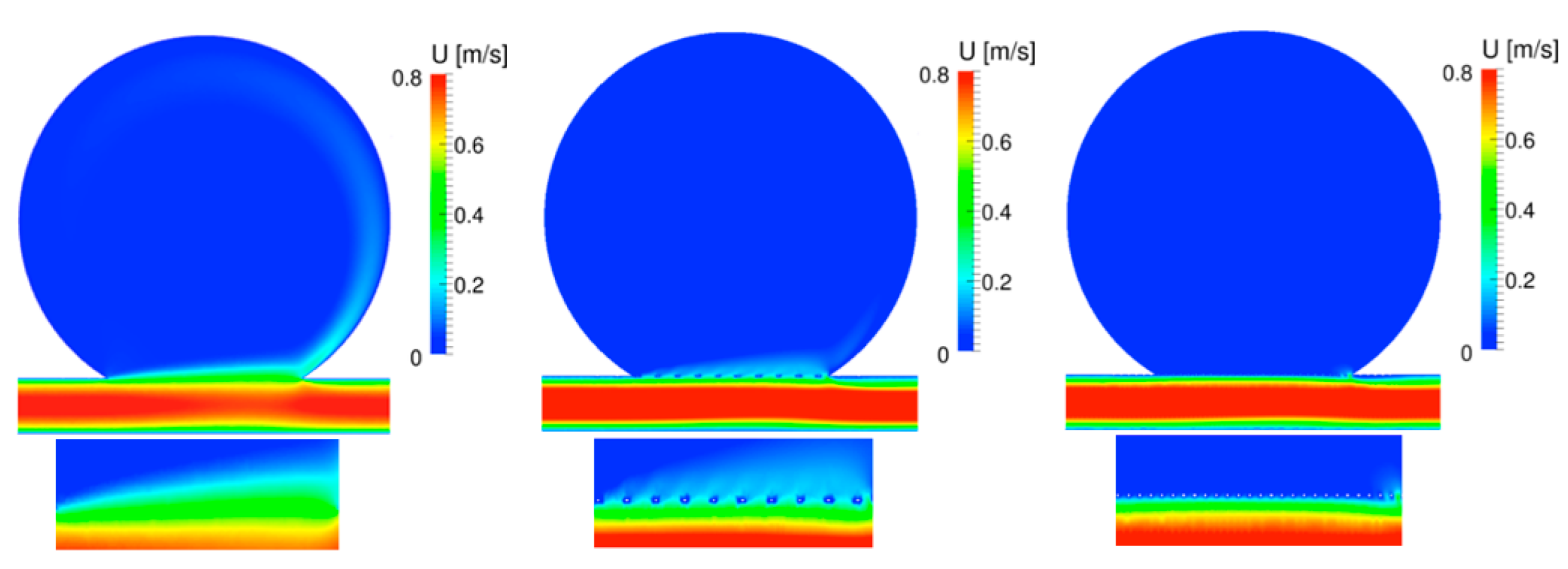
3. Results and Discussion
4. Limitations and Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willis, T. The Anatomy of the Brain and the Nerves, Tercentenary ed.; Feindel, W., Ed.; McGill University Press: Montreal, QB, Canada, 1965. [Google Scholar]
- Dennis, K.D.; Rossman, T.L.; Kallmes, D.F.; Dragomir-Daescu, D. Intra-aneurysmal flow rates are reduced by two flow diverters: An experiment using tomographic particle image velocimetry in an aneurysm model. J. NeuroIntervent. Surg. 2015, 7, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Augsburger, L.; Reymond, P.; Rüfenacht, D.A.; Stergiopulos, N. Intracranial stents being modeled as a porous medium: Flow simulation in stented cerebral aneurysms. Ann. Biomed. Eng. 2010, 39, 850–863. [Google Scholar] [CrossRef] [PubMed]
- Möhlenbruch, M.; Herweh, C.; Jestaedt, L.; Stampfl, S.; Schönenberger, S.; Ringleb, P.; Bendszus, M.; Pham, M. The FRED flow-diverter stent for intracranial aneurysms: Clinical study to assess safety and efficacy. Am. J. Neuroradiol. 2015, 36, 1155–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, M.; Becske, T.; Sahlein, D.; Babb, J.; Nelson, P. Stent-supported aneurysm coiling: A literature survey of treatment and follow-up. Am. J. Neuroradiol. 2012, 33, 159–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coley, S.; Sneade, M.; Clarke, A.; Mehta, Z.; Kallmes, D.; Cekirge, S.; Saatci, I.; Roy, D.; Molyneux, A. Cerecyte coil trial: Procedural safety and clinical outcomes in patients with ruptured and unruptured intracranial aneurysms. Am. J. Neuroradiol 2012, 33, 474–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alderazi, Y.J.; Shastri, D.; Kass-Hout, T.; Prestigiacomo, C.J.; Gandhi, C.D. Flow diverters for intracranial aneurysms. Stroke Res. Treat. 2014, 2014, 1–12. [Google Scholar] [CrossRef]
- Becske, T.; Kallmes, D.F.; Saatci, I.; McDougall, C.G.; Szikora, I.; Lanzino, G.; Moran, C.J.; Woo, H.H.; Lopes, D.K.; Berez, A.L.; et al. Pipeline for uncoilable or failed aneurysms: Results from a multicenter clinical trial. Radiology 2013, 267, 858–868. [Google Scholar] [CrossRef]
- Girdhar, G.; Li, J.; Kostousov, L.; Wainwright, J.; Chandler, W.L. In-vitro thrombogenicity assessment of flow diversion and aneurysm bridging devices. J. Thromb. Thromboly 2015, 40, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Sadasivan, C.; Cesar, L.; Seong, J.; Rakian, A.; Hao, Q.; Tio, F.O.; Wakhloo, A.K.; Lieber, B.B. An original flow diversion device for the treatment of intracranial aneurysms: Evaluation in the rabbit elastase-induced model. Stroke 2009, 40, 952–958. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Peng, T.; Wu, J.; Huang, C.; Jiang, Y.; Chen, L. Outflow vessel in the plane of main vortex of large cerebral aneurysms: A study of hemodynamic analyses. Neurosc. Med. 2015, 6, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Tremmel, M.; Xiang, J.; Natarajan, S.K.; Hopkins, L.N.; Siddiqui, A.H.; Levy, E.I.; Meng, H. Alteration of intra-aneurysmal hemody-namics for flow diversion using enterprise and vision stents. World Neurosurg. 2010, 74, 306–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jou, L.-D.; Lee, D.; Morsi, H.; Mawad, M. Wall shear stress on ruptured and unruptured intracranial aneurysms at the internal carotid artery. Am. J. Neuroradiol. 2008, 29, 1761–1767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shojima, M.; Oshima, M.; Takagi, K.; Torii, R.; Hayakawa, M.; Katada, K.; Morita, A.; Kirino, T. Magnitude and role of wall shear stress on cerebral aneurysm computational fluid dynamic study of 20 middle cerebral artery aneurysms. Stroke 2004, 35, 2500–2505. [Google Scholar] [CrossRef] [PubMed]
- Cebral, J.R.; Castro, M.A.; Burgess, J.E.; Pergolizzi, R.S.; Sheridan, M.J.; Putman, C.M. Characterization of cerebral aneurysms for assessing risk of rupture by using patient-specific computational hemodynamics models. Am. J. Neuroradiol. 2005, 26, 2550–2559. [Google Scholar] [PubMed]
- Wong, G.K.; Kwan, M.C.; Ng, R.Y.; Simon, C.H.; Poon, W.S. Flow diverters for treatment of intracranial aneurysms: Current status and ongoing clinical trials. J. Clin. Neuroradiol. 2011, 18, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Steinman, D.A.; Milner, J.S.; Norley, C.J.; Lownie, S.P.; Holdsworth, D.W. Image-based computational simulation of flow dynamics in a giant intracranial aneurysm. Am. J. Neuroradiol. 2003, 24, 559–566. [Google Scholar] [PubMed]
- Kojima, M.; Irie, K.; Masunaga, K.; Sakai, Y.; Nakajima, M.; Takeuchi, M.; Fukuda, T.; Arai, F.; Negoro, M. Hybrid stent device of flow-diverting effect and stent-assisted coil embolization formed by fractal structure. Med. Biol. Eng. Comput. 2016, 54, 1–11. [Google Scholar] [CrossRef]
- Ley, D.; Mühl-Benninghaus, R.; Yilmaz, U.; Körner, H.; Cattaneo, G.F.M.; Mailänder, W.; Kim, Y.-J.; Scheller, B.; Reith, W.; Simgen, A. The derivo embolization device, a second-generation flow diverter for the treatment of intracranial aneurysms, evaluated in an elastase-induced aneurysm model. J. Clin. Neurol. 2017, 3, 335–343. [Google Scholar] [CrossRef]
- O’kelly, C.J.; Spears, J.; Chow, M.; Wong, J.; Boulton, M.; Weill, A.; Willinsky, R.A.; Kelly, M.; Marotta, T.R. Canadian experience with the pipeline embolization device for repair of unruptured intracranial aneurysms. Am. J. Neuroradiol. 2013, 34, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; You, Z.; Peach, T.; Byrne, J.; Rizkallah, R.R. A new flow diverter stent for direct treatment of intracranial aneurysm. J. Biomech. 2015, 48, 4206–4213. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.E.; Gomori, J.M.; Moscovici, S.; Leker, R.R.; Itshayek, E. Delayed complications after flow-diverter stenting: Reactive in-stent stenosis and creeping stents. J. Clin. Neuros. 2014, 21, 1116–1122. [Google Scholar] [CrossRef]
- Kuzmik, G.A.; Williamson, T.; Ediriwickrema, A.; Andeejani, A.; Bulsara, K.R. Flow diverters and a tale of two aneurysms. J. NeuroIntervent Surg. 2013, 5, e23. [Google Scholar] [CrossRef]
- Hampton, T.; Walsh, D.; Tolias, C.; Fiorella, D. Mural destabilization after aneurysm treatment with a flow-diverting device: A report of two cases. J. NeuroIntervent. Surg. 2011, 3, 167–171. [Google Scholar] [CrossRef]
- Kulcsár, Z.; Houdart, E.; Bonafé, A.; Parker, G.; Millar, J.; Goddard, A.J.; Renowden, S.; Gál, G.; Turowski, B.; Mitchell, K.; et al. Intra-aneurysmal thrombosis as a possible cause of delayed aneurysm rupture after flow-diversion treatment. Am. J. Neuroradiol 2011, 32, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Goubergrits, L.; Schaller, J.; Kertzscher, U.; Woelken, T.; Ringelstein, M.; Spuler, A. Hemodynamic impact of cerebral aneurysm endovascular treatment devices: Coils and flow diverters. Expert Rev. Med. Devices 2014, 11, 361–373. [Google Scholar] [CrossRef]
- Jou, L.D.; Mawad, M.E. Timing and size of flow impingement in a giant intracranial aneurysm at the internal carotid artery. Med. Biol. Eng. Comput. 2011, 49, 891–899. [Google Scholar] [CrossRef]
- Chien, A.; Tateshima, S.; Castro, M.; Sayre, J.; Cebral, J.; Vinueala, F. Patient-specific flow analysis of brain aneurysms at a single location: Comparison of hemodynamic characteristics in small aneurysms. Med. Biol. Eng. Comput. 2008, 46, 1113–1120. [Google Scholar] [CrossRef]
- Bouillot, P.; Brina, O.; Ouared, R.; Yilmaz, H.; Lovblad, K.-O.; Farhat, M.; Pereira, V.M. Computational fluid dynamics with stents: Quantitative comparison with particle image velocimetry for the three commercials off the shelf intracranial stents. J. NeuroIntervent. Surg. 2016, 8, 309–315. [Google Scholar] [CrossRef]
- Boussel, L.; Rayz, V.; McCulloch, C.; Martin, A.; Acevedo-Bolton, G.; Lawton, M.; Higashida, R.; Smith, W.S.; Young, W.L.; Saloner, D. Aneurysm growth occurs at region of low wall shear stress patient- specific correlation of hemodynamics and growth in a longitudinal study. Stroke 2008, 39, 2997–3002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouillot, P.; Brina, O.; Ouared, R.; Lovblad, K.-O.; Farhat, M.; Pereira, V.M. Hemodynamic transition driven by stent porosity in sidewall aneurysms. J. Biomech. 2015, 48, 1300–1309. [Google Scholar] [CrossRef]
- Gambaruto, A.; Janela, J.; Moura, A.; Sequeira, A. Sensitivity of hemodynamics in a patient specific cerebral aneurysm to vascular geometry and blood rheology. Math. Biosc. Eng. 2011, 8, 409–423. [Google Scholar]
- Cebral, J.; Castro, M.; Appanaboyina, S.; Putman, C.; Millan, D.; Frangi, A. Efficient pipeline for image-based patient-specific analysis of cerebral aneurysm hemodynamics: Technique and sensitivity. IEEE Trans. Med. Imaging 2005, 24, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Tremmel, M.; Kolega, J.; Levy, E.I.; Natarajan, S.K.; Meng, H. Newtonian viscosity model could overestimate wall shear stress in intracranial aneurysm domes and underestimate rupture risk. J. NeuroIntervent. Surg. 2012, 4, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Gambaruto, A.; Janela, J.; Moura, A.; Sequeira, A. Shear-thinning effects of hemodynamics in patient-specific cerebral aneurysms. Math. Biosc. Eng. 2013, 10, 649–665. [Google Scholar]
- Reymond, P.; Merenda, F.; Perren, F.; Rüfenacht, D.; Stergiopulos, N. Validation of one-dimensional model of the systemic arterial tree. Am. J. Physiol Heart Circ. Physiol. 2009, 297, H208–H222. [Google Scholar] [CrossRef] [Green Version]
- Valencia, A.; Morales, H.; Rivera, R.; Bravo, E.; Galvez, M. Blood flow dynamics in patient-specific cerebral aneurysm models: The relationship between wall shear stress and aneurysm area index. Med. Eng. Phys. 2008, 30, 329–379. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.; Tutino, V.M.; Xiang, J.; Siddiqui, A. High WSS or low WSS? Complex interactions of hemodynamics with intracranial aneurysm initiation, growth, and rupture: Toward a unifying hypothesis. Am. J. Neuroradiol. 2014, 35, 1254–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallmes, D.F.; Ding, Y.H.; Dai, D.; Kadirvel, R.; Lewis, D.A.; Cloft, H.J. A new endoluminal, flow-disrupting device for treatment of saccular aneurysms. Stroke 2007, 38, 2346–2352. [Google Scholar] [CrossRef] [Green Version]
- Lieber, B.B.; Sadasivan, C. Endoluminal scaffolds for vascular reconstruction and exclusion of aneurysms from the cerebral circulation. Stroke 2010, 41, S21–S25. [Google Scholar] [CrossRef] [Green Version]
- Wootton, D.M.; Ku, D.N. Fluid mechanics of vascular systems, diseases, and thrombosis. Ann. Rev. Biomed. Eng. 1999, 1, 299–329. [Google Scholar] [CrossRef]
- Meng, H.; Wang, Z.; Kim, M.; Ecker, R.D.; Hopkins, L.N. Saccular aneurysms on straight and curved vessels are subject to different hemodynamics: Implications of intravascular stenting. Am. J. Neuroradiol. 2006, 27, 1861–1865. [Google Scholar] [PubMed]
- Bouillot, P.; Brina, O.; Ouared, R.; Lovblad, K.-O.; Farhat, M.; Pereira, V.M. Particle imaging velocimetry evaluation of intracranial stents in sidewall aneurysm: Hemodynamic transition related to the stent design. PLoS ONE 2014, 9, e113762. [Google Scholar] [CrossRef]
- Kerl, H.U.; Boll, H.; Fiebig, T.; Figueiredo, G.; Förster, A.; Nölte, I.S.; Nonn, A.; Groden, C.; Brockmann, M.A. Implantation of pipeline flow-diverting stents reduces aneurysm inflow without relevantly affecting static intra-aneurysmal pressure. Neurosurgery 2014, 4, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Larrabide, I.; Aguilar, M.; Morales, H.G.; Geers, A.; Kulcsar, Z.; Rüfenacht, D.; Frangi, A. Intra-aneurysmal pressure and flow changes induced by flow diverters: Relation to aneurysm size and shape. Am. J. Neuroradiol. 2013, 34, 816–822. [Google Scholar] [CrossRef] [Green Version]
- Xiang, J.; Ma, D.; Snyder, K.V.; Levy, E.I.; Siddiqui, A.H.; Meng, H. Increasing flow diversion for cerebral aneurysm treatment using a single flow diverter. Neurosurgery 2014, 75, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Gholampour, S.; Mehrjoo, S. Effect of bifurcation in the hemodynamic changes and rupture risk of small intracranial aneurysm. Neurosurg. Rev. 2021, 44, 1703–1712. [Google Scholar] [CrossRef] [PubMed]
- Hajirayat, K.; Gholampour, S.; Sharif, I.; Bizaria, D. Biomechanical Simulation to Compare the Blood Flow Hemodynamics and Cerebral Anurysm Rupture Risk in Patients with Different Aneurysms Necks. J. Appl. Mech. Tech. Phys. 2017, 58, 968–974. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
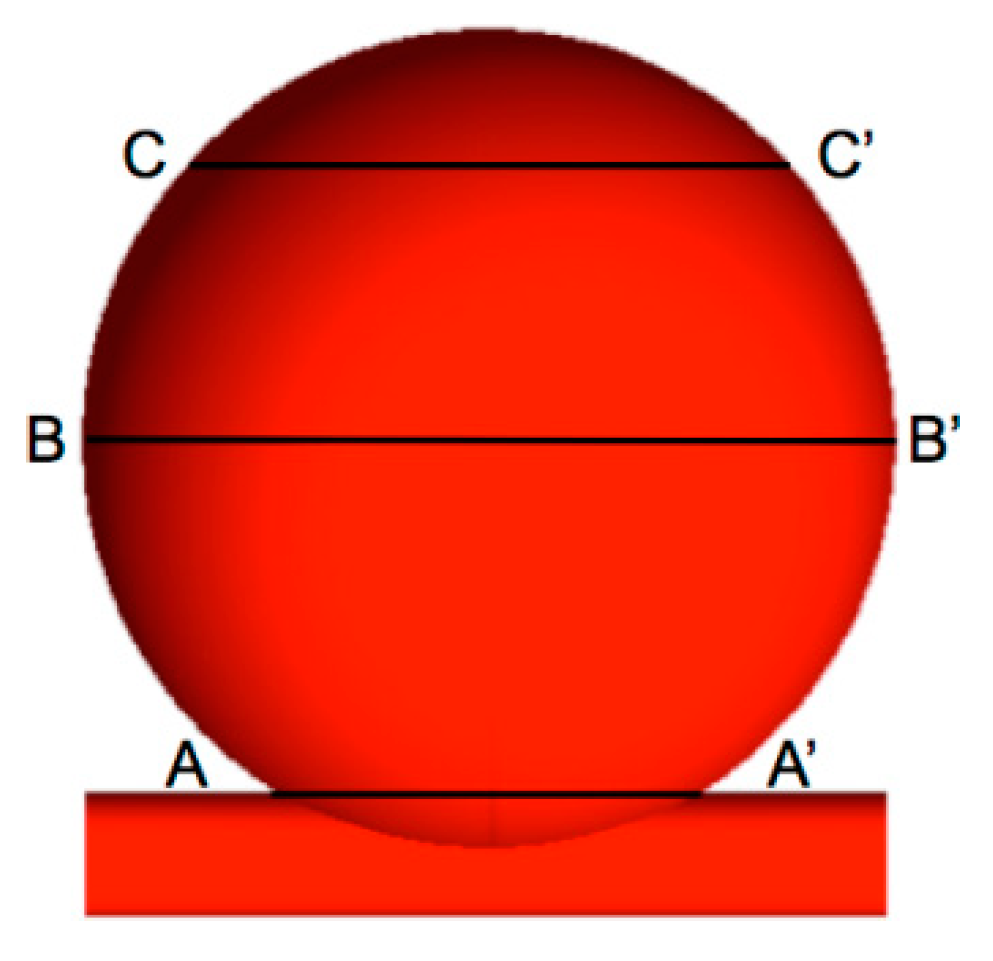
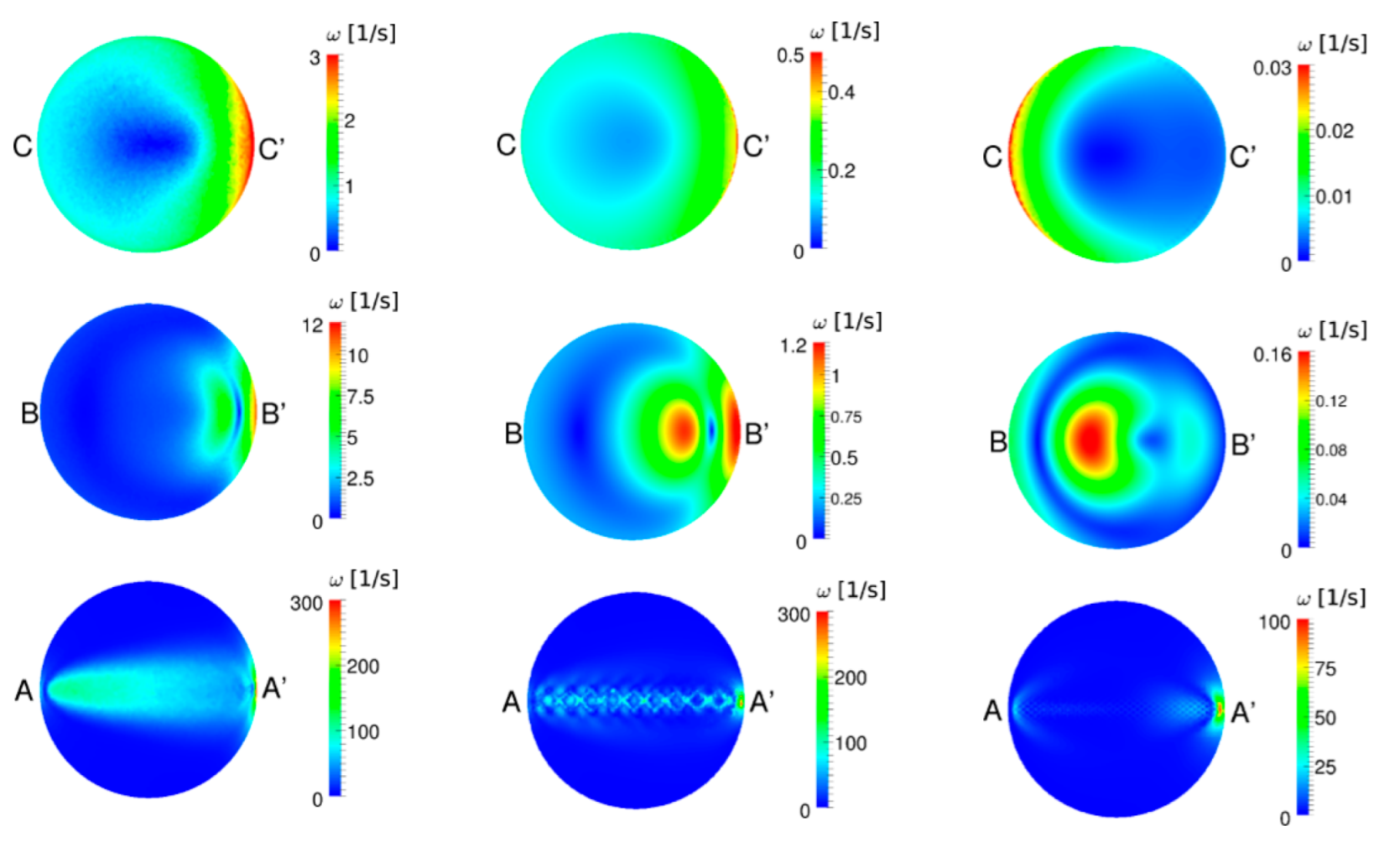
| UA | RS | FD | |
|---|---|---|---|
| A-A’ | 13.2000 Pa | 2.6000 Pa (−80.3%) | 1.3000 Pa (−90.1%) |
| B-B’ | 0.4500 Pa | 0.0660 Pa (−85.3%) | 0.0400 Pa (−91.1%) |
| C-C’ | 0.1800 Pa | 0.0310 Pa (−82.7%) | 0.0015 Pa (−99.2%) |
| UA | RS | FD | |
|---|---|---|---|
| A-A’ | 1.620 Pa | 0.8800 Pa (−45%) | 0.2400 Pa (−85%) |
| B-B’ | 0.0380 Pa | 0.0043 Pa (−88.7%) | 0.0043 Pa (−88.7%) |
| C-C’ | 0.0130 Pa | 0.0018 Pa (−86.1%) | 0.0001 Pa (−99.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanches, A.F.; Shit, S.; Özpeynirci, Y.; Liebig, T. CFD to Quantify Idealized Intra-Aneurysmal Blood Flow in Response to Regular and Flow Diverter Stent Treatment. Fluids 2022, 7, 254. https://doi.org/10.3390/fluids7080254
Sanches AF, Shit S, Özpeynirci Y, Liebig T. CFD to Quantify Idealized Intra-Aneurysmal Blood Flow in Response to Regular and Flow Diverter Stent Treatment. Fluids. 2022; 7(8):254. https://doi.org/10.3390/fluids7080254
Chicago/Turabian StyleSanches, Augusto Fava, Suprosanna Shit, Yigit Özpeynirci, and Thomas Liebig. 2022. "CFD to Quantify Idealized Intra-Aneurysmal Blood Flow in Response to Regular and Flow Diverter Stent Treatment" Fluids 7, no. 8: 254. https://doi.org/10.3390/fluids7080254