

Patient-Specific 3D Printed Soft Models for Liver Surgical Planning and Hands-On Training
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Results and Discussion
2.1. Results
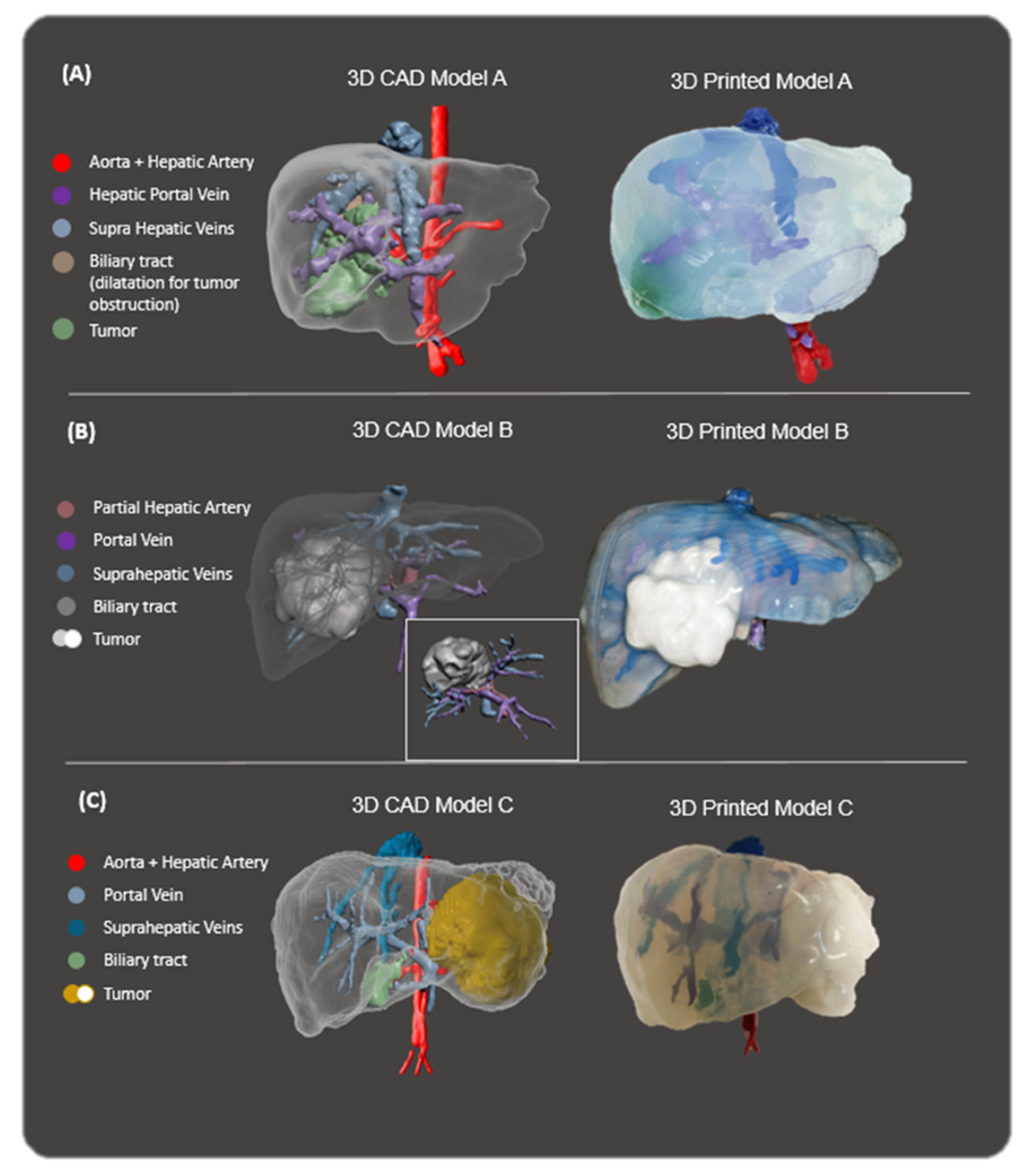
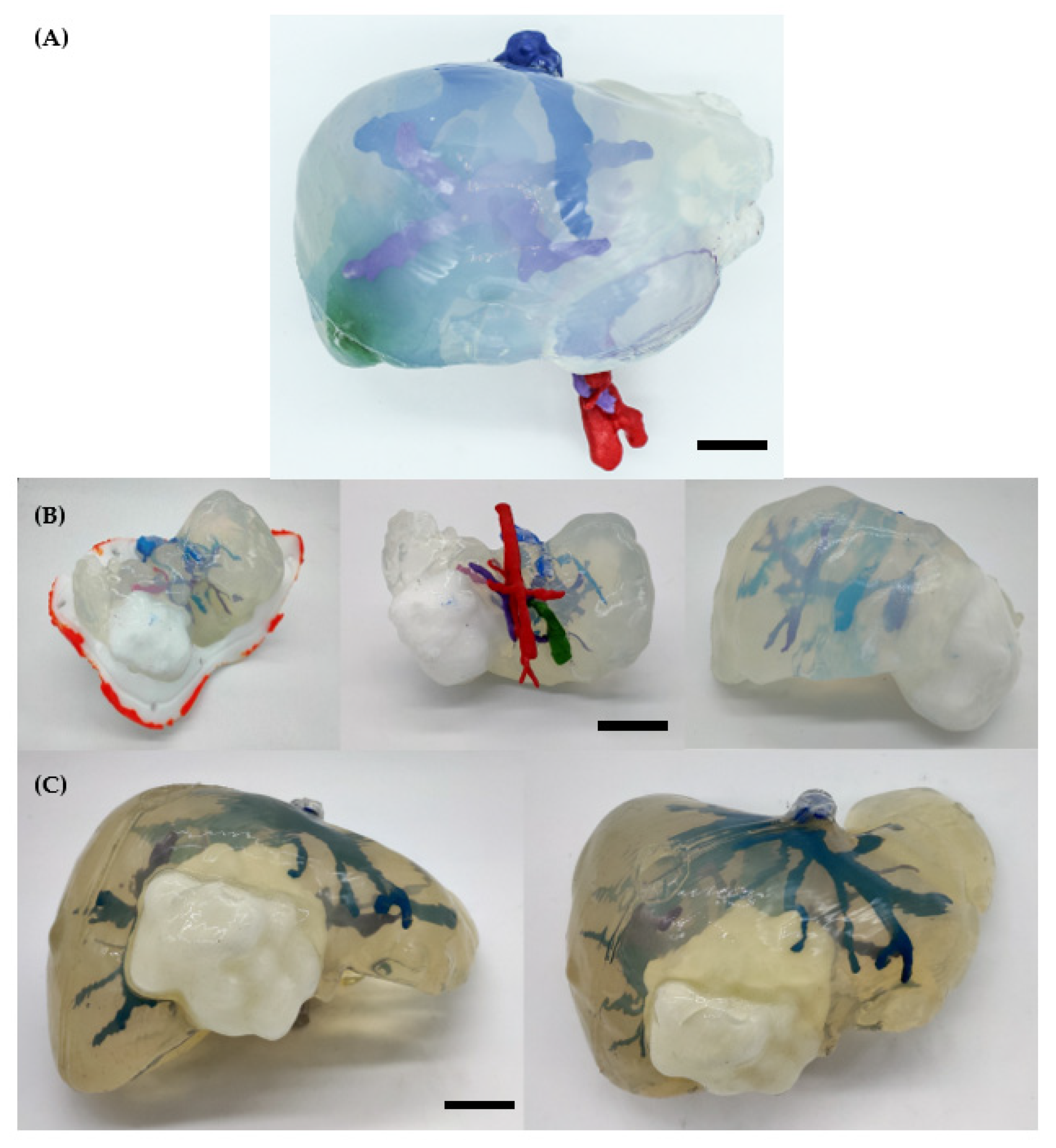
2.1.1. 3D Models
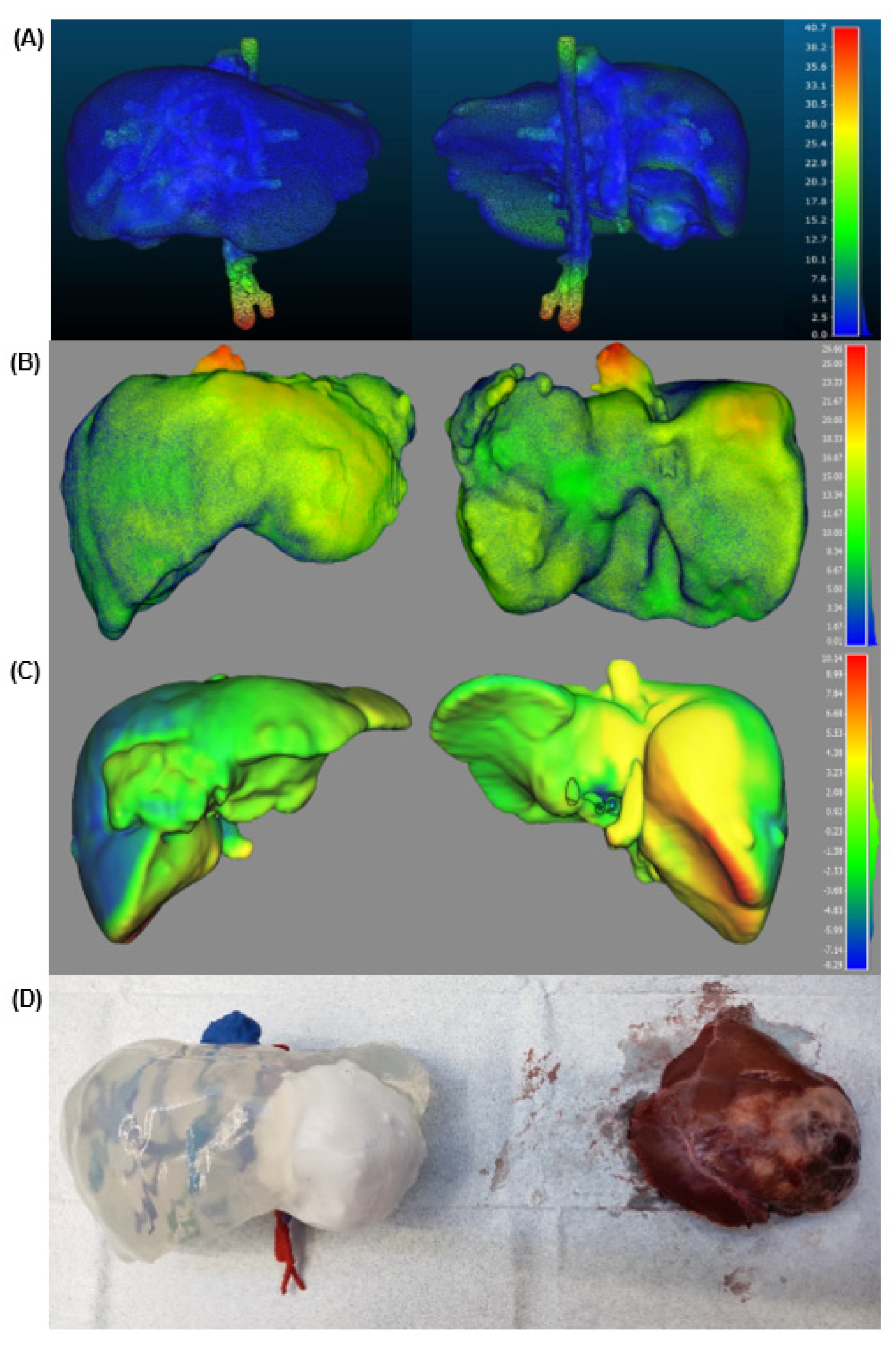
2.1.2. Validation
2.1.3. Cost
2.1.4. Time
2.2. Discussion
2.2.1. Clinical Relevance
2.2.2. Limitations
3. Conclusions
4. Materials and Methods
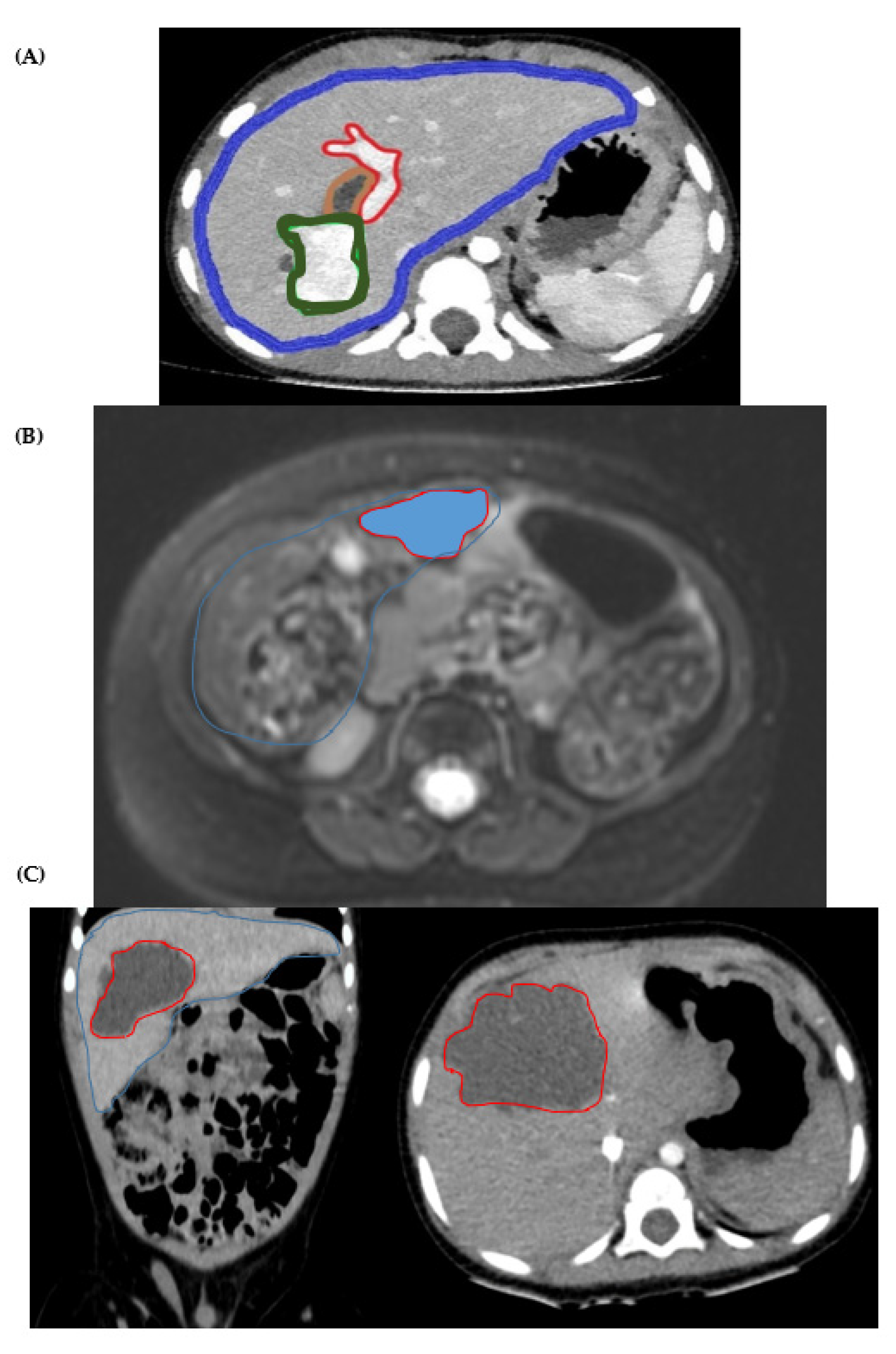
4.1. Cases Presentation
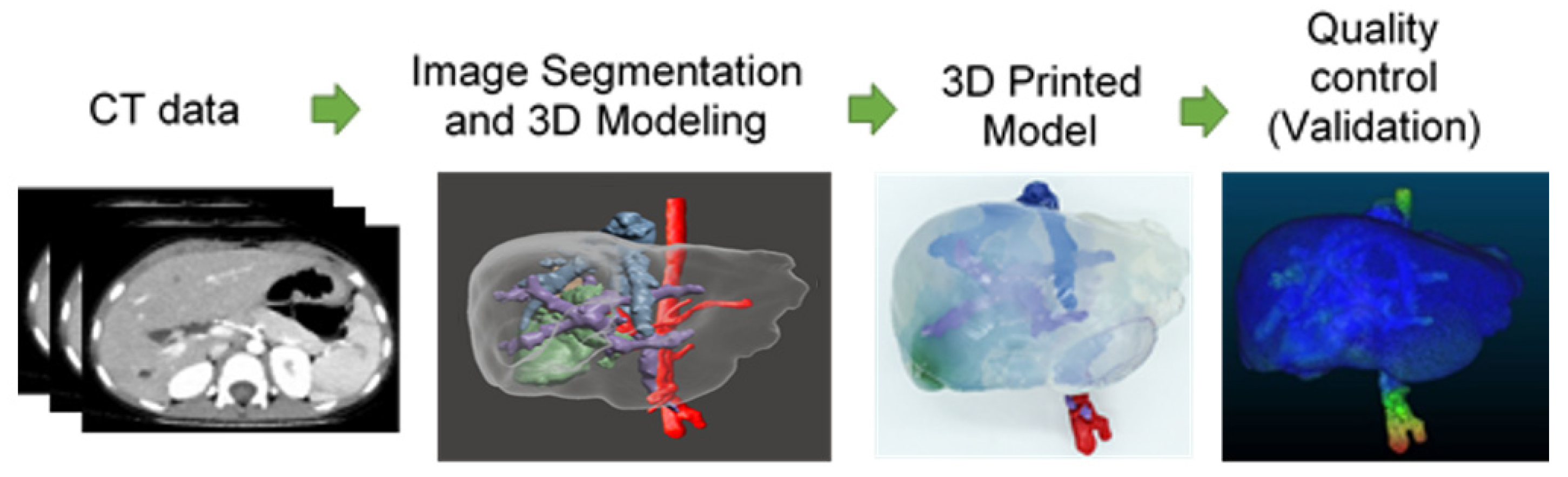
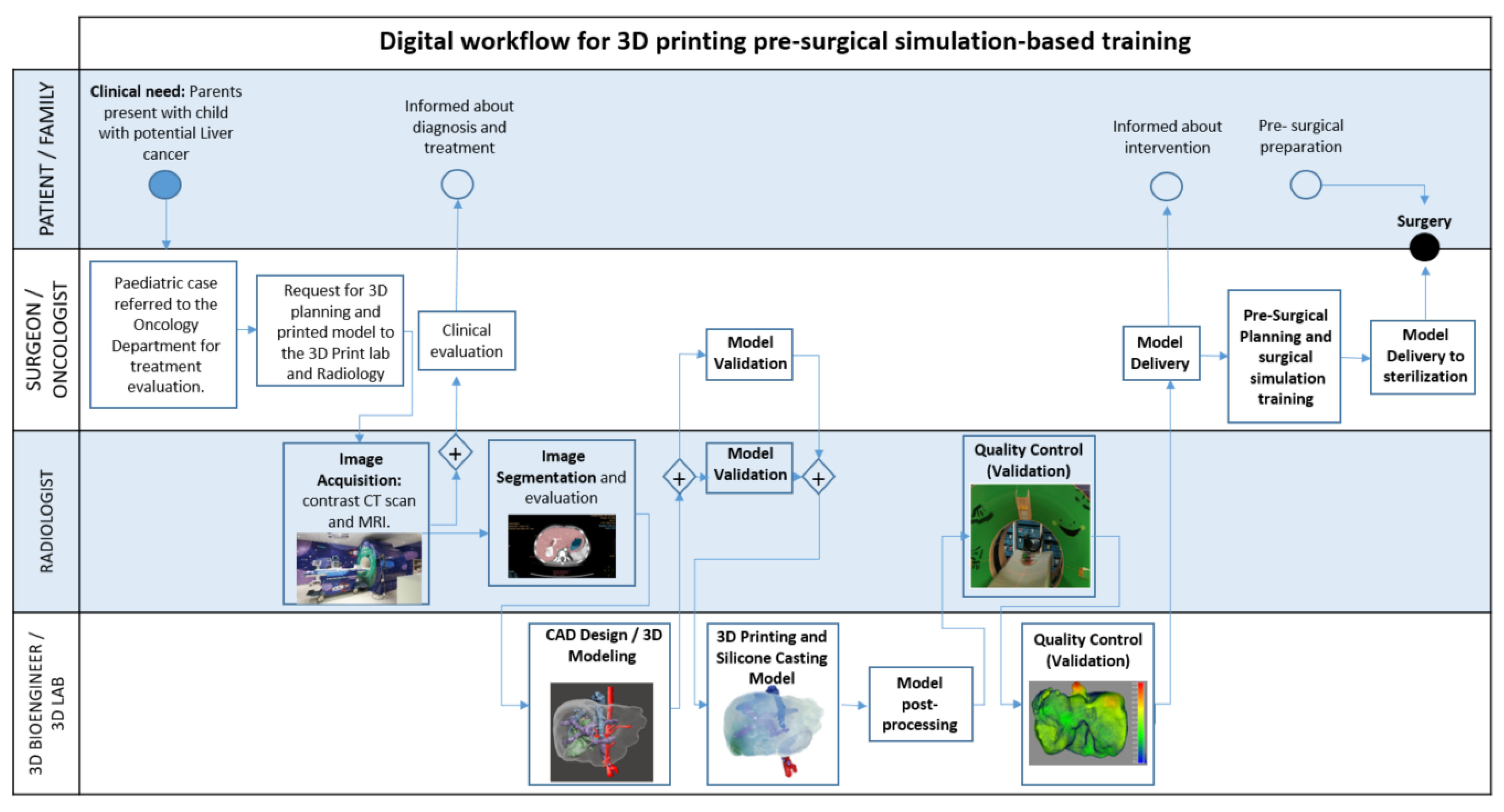
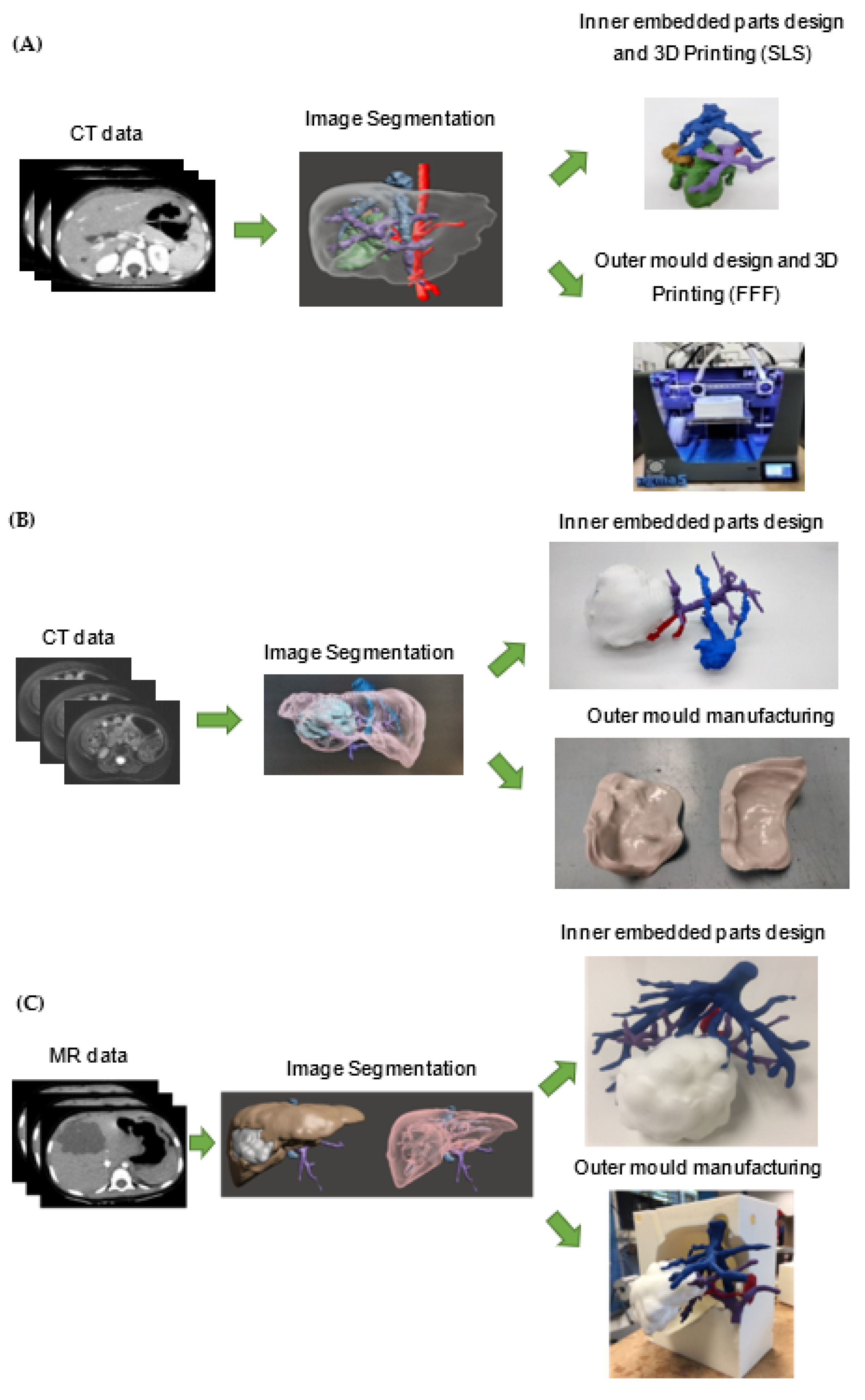
4.2. Digital Workflow for 3D Printing Pre-Surgical Simulation-Based Training
4.3. Image Acquisition
4.4. Image Segmentation and Surface Reconstruction
4.5. CAD Design and 3D Moulding
4.6. 3D Printing and Silicone Casting of the Phantom
4.7. Validation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthc. Eng. 2019, 2019, 5340616. [Google Scholar] [CrossRef] [PubMed]
- Perica, E.R.; Sun, Z. A Systematic Review of Three-Dimensional Printing in Liver Disease. J. Digit. Imaging 2018, 31, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Pereira, H.R.; Barzegar, M.; Hamadelseed, O.; Esteve, A.V.; Munuera, J. 3D surgical planning of pediatric tumors: A review. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Li, D.; Jeong, M.; Yu, T.; Ma, Z.; Afat, S.; Grund, K.-E.; Qiu, T. Soft Liver Phantom with a Hollow Biliary System. Ann. Biomed. Eng. 2021, 49, 2139–2149. [Google Scholar] [CrossRef] [PubMed]
- Wake, N.; Nussbaum, J.E.; Elias, M.I.; Nikas, C.V.; Bjurlin, M.A. 3D printing, augmented reality, and virtual reality for the assessment and management of kidney and prostate cancer: A systematic review. Urology 2020, 143, 20–32. [Google Scholar] [CrossRef]
- Boedecker, C.; Huettl, F.; Saalfeld, P.; Paschold, M.; Kneist, W.; Baumgart, J.; Preim, B.; Hansen, C.; Lang, H.; Huber, T. Using virtual 3D-models in surgical planning: Workflow of an immersive virtual reality application in liver surgery. Langenbeck’s Arch. Surg. 2021, 406, 911–915. [Google Scholar] [CrossRef]
- Tejo-Otero, A.; Fenollosa-Artés, F.; Achaerandio, I.; Rey-Vinolas, S.; Buj-Corral, I.; Mateos-Timoneda, M.; Engel, E. Soft-tissue-mimicking using hydrogels for the development of phantoms. Gels 2022, 8, 40. [Google Scholar] [CrossRef]
- Singh, G.; Chanda, A. Mechanical properties of whole-body soft human tissues: A review. Biomed. Mater. 2021, 16, 062004. [Google Scholar] [CrossRef]
- Mattei, G.; Ahluwalia, A. Sample, testing and analysis variables affecting liver mechanical properties: A review. Acta Biomater. 2016, 45, 60–71. [Google Scholar] [CrossRef]
- Yoon, Y.C.; Lee, J.S.; Park, S.U.; Kwon, J.H.; Hong, T.H.; Kim, D.G. Quantitative assessment of liver fibrosis using shore durometer. Ann. Surg. Treat. Res. 2017, 93, 300–304. [Google Scholar] [CrossRef]
- Estermann, S.-J.; Pahr, D.H.; Reisinger, A. Quantifying tactile properties of liver tissue, silicone elastomers, and a 3D printed polymer for manufacturing realistic organ models. J. Mech. Behav. Biomed. Mater. 2020, 104, 103630. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Hanna, G.B.; Cuschieri, A. Analysis of errors enacted by surgical trainees during skills training courses. Surgery 2005, 138, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Lama, S.; Gan, L.S.; Maddahi, Y.; Zareinia, K.; Sutherland, G.R. Forces of tool-tissue interaction to assess surgical skill level. JAMA Surg. 2018, 153, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Wohlers, T. Rapid Prototyping & Tooling State of the Industry: 1998 Worldwide Progress Report. Mater. Technol. 2016, 13, 174–176. [Google Scholar] [CrossRef]
- ASTM52900-15; Standard Terminology for Additive Manufacturing—General Principles—Terminology. ASTM International: West Conshohocken, PA, USA, 2015.
- Forte, A.E.; Galvan, S.; Manieri, F.; Rodriguez y Baena, F.; Dini, D. A composite hydrogel for brain tissue phantoms. Mater. Des. 2016, 112, 227–238. [Google Scholar] [CrossRef]
- Noor, N.; Shapira, A.; Edri, R.; Gal, I.; Wertheim, L.; Dvir, T. 3D Printing of Personalized Thick and Perfusable Cardiac Patches and Hearts. Adv. Sci. 2019, 6, 1900344. [Google Scholar] [CrossRef] [PubMed]
- Bezek, L.B.; Cauchi, M.P.; De Vita, R.; Foerst, J.R.; Williams, C.B. 3D printing tissue-mimicking materials for realistic transseptal puncture models. J. Mech. Behav. Biomed. Mater. 2020, 110, 103971. [Google Scholar] [CrossRef]
- Krauel, L.; Fenollosa, F.; Riaza, L.; Pérez, M.; Tarrado, X.; Morales, A.; Gomà, J.; Mora, J. Use of 3D Prototypes for Complex Surgical Oncologic Cases. World J. Surg. 2016, 40, 889–894. [Google Scholar] [CrossRef]
- Muguruza Blanco, A.; Krauel, L.; Fenollosa Artés, F. Development of a patients-specific 3D-printed preoperative planning and training tool, with functionalized internal surfaces, for complex oncologic cases. Rapid Prototyp. J. 2019, 25, 363–377. [Google Scholar] [CrossRef]
- Tejo-Otero, A.; Lustig-Gainza, P.; Fenollosa-Artés, F.; Valls-Esteve, A.; Krauel, L.; Buj-Corral, I. 3D printed soft surgical planning prototype for a biliary tract rhabdomyosarcoma. J. Mech. Behav. Biomed. Mater. 2020, 109, 103844. [Google Scholar] [CrossRef]
- Souzaki, R.; Kinoshita, Y.; Ieiri, S.; Hayashida, M.; Koga, Y.; Shirabe, K.; Hara, T.; Maehara, Y.; Hashizume, M.; Taguchi, T. Three-dimensional liver model based on preoperative CT images as a tool to assist in surgical planning for hepatoblastoma in a child. Pediatr. Surg. Int. 2015, 31, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Zein, N.N.; Hanouneh, I.A.; Bishop, P.D.; Samaan, M.; Eghtesad, B.; Quintini, C.; Miller, C.; Yerian, L.; Klatte, R. Techniques to ensure adequate portal flow in the presence of splenorenal shunts. Liver Transpl. 2007, 13, 767–768. [Google Scholar] [CrossRef]
- Witowski, J.S.; Pędziwiatr, M.; Major, P.; Budzyński, A. Cost-effective, personalized, 3D-printed liver model for preoperative planning before laparoscopic liver hemihepatectomy for colorectal cancer metastases. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 2047–2054. [Google Scholar] [CrossRef] [PubMed]
- Tejo-Otero, A.; Buj-Corral, I.; Fenollosa-Artés, F. 3D Printing in Medicine for Preoperative Surgical Planning: A Review. Ann. Biomed. Eng. 2020, 48, 536–555. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Si, Y.; Han, Y.; Wu, T.; Iqbal, M.I.; Fei, B.; Li, R.K.Y.; Hu, J.; Qu, J. Recent progress in protective membranes fabricated via electrospinning: Advanced materials, biomimetic structures, and functional applications. Adv. Mater. 2022, 34, 2107938. [Google Scholar] [CrossRef] [PubMed]
- Su, C.; Chen, Y.; Tian, S.; Lu, C.; Lv, Q. Natural Materials for 3D Printing and Their Applications. Gels 2022, 8, 748. [Google Scholar] [CrossRef]
- Zare, M.; Ghomi, E.R.; Venkatraman, P.D.; Ramakrishna, S. Silicone-based biomaterials for biomedical applications: Antimicrobial strategies and 3D printing technologies. J. Appl. Polym. Sci. 2021, 138, 50969. [Google Scholar] [CrossRef]
- Zingaretti, N.; Galvano, F.; Vittorini, P.; De Francesco, F.; Almesberger, D.; Riccio, M.; Vaienti, L.; Parodi, P.C. Smooth prosthesis: Our experience and current state of art in the use of smooth sub-muscular silicone gel breast implants. Aesthetic Plast. Surg. 2019, 43, 1454–1466. [Google Scholar] [CrossRef]
- Sastri, V.R. Plastics in Medical Devices: Properties, Requirements, and Applications; William Andrew: Norwich, NY, USA, 2021. [Google Scholar]
- Momeni, M.; Hafezi, F.; Rahbar, H.; Karimi, H. Effects of silicone gel on burn scars. Burns 2009, 35, 70–74. [Google Scholar] [CrossRef]
- In, E.; Walker, E.; Naguib, H. Novel development of 3D printable UV-curable silicone for multimodal imaging phantom. Bioprinting 2017, 7, 19–26. [Google Scholar] [CrossRef]
- Tejo-Otero, A.; Valls-Esteve, A.; Fenollosa-Artés, F.; Siles-Hinojosa, A.; Nafria, B.; Ayats, M.; Buj-Corral, I.; Otero, M.; Rubio-Palau, J.; Munuera, J.; et al. Patient comprehension of oncologic surgical procedures using 3D printed surgical planning prototypes. Ann. 3D Print. Med. 2022, 7, 100068. [Google Scholar] [CrossRef]
- Bücking, T.M.; Hill, E.R.; Robertson, J.L.; Maneas, E.; Plumb, A.A.; Nikitichev, D.I. From medical imaging data to 3D printed anatomical models. PLoS ONE 2017, 12, e0178540. [Google Scholar] [CrossRef] [PubMed]
- Witowski, J.; Wake, N.; Grochowska, A.; Sun, Z.; Budzyński, A.; Major, P.; Popiela, T.J.; Pędziwiatr, M. Investigating accuracy of 3D printed liver models with computed tomography. Quant. Imaging Med. Surg. 2019, 9, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Filippou, V.; Tsoumpas, C. Recent advances on the development of phantoms using 3D printing for imaging with CT, MRI, PET, SPECT, and ultrasound. Med. Phys. 2018, 45, e740–e760. [Google Scholar] [CrossRef] [PubMed]
- Mitsouras, D.; Liacouras, P.; Imanzadeh, A.; Giannopoulos, A.A.; Cai, T.; Kumamaru, K.K.; George, E.; Wake, N.; Caterson, E.J.; Pomahac, B.; et al. Medical 3D printing for the radiologist. Radiographic 2015, 35, 1965–1988. [Google Scholar] [CrossRef]
- Mitsouras, D.; Lee, T.C.; Liacouras, P.; Ionita, C.N.; Pietilla, T.; Maier, S.E.; Mulkern, R.V. Three-dimensional printing of MRI-visible phantoms and MR image-guided therapy simulation. Magn. Reson. Med. 2017, 77, 613–622. [Google Scholar] [CrossRef]
- Madurska, M.J.; Poyade, M.; Eason, D.; Rea, P.; Watson, A.J.M. Development of a Patient-Specific 3D-Printed Liver Model for Preoperative Planning. Surg. Innov. 2017, 24, 145–150. [Google Scholar] [CrossRef]
- Igami, T.; Nakamura, Y.; Hirose, T.; Ebata, T.; Yokoyama, Y.; Sugawara, G.; Mizuno, T.; Mori, K.; Nagino, M. Application of a three-dimensional print of a liver in hepatectomy for small tumors invisible by Intraoperative ultrasonography: Preliminary experience. World J. Surg. 2014, 38, 3163–3166. [Google Scholar] [CrossRef]
- Ravi, P.; Burch, M.B.; Farahani, S.; Chepelev, L.L.; Yang, D.; Ali, A.; Joyce, J.R.; Lawera, N.; Stringer, J.; Morris, J.M.; et al. Utility and Costs During the Initial Year of 3-D Printing in an Academic Hospital. J. Am. Coll. Radiol. 2022, 20, 193–204. [Google Scholar] [CrossRef]
- Curtis, J.; Steichen, S.D. Silicones. In Biomaterials Science; Academic Press: Cambridge, MA, USA, 2020; pp. 109–123. [Google Scholar]
- Zarrintaj, P.; Manouchehri, S.; Ahmadi, Z.; Saeb, M.R.; Urbanska, A.M.; Kaplan, D.L.; Mozafari, M. Agarose-based biomaterials for tissue engineering. Carbohydr. Polym. 2018, 187, 66–84. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Parameters | Values [mm] |
|---|---|---|
| #1 | Average Distance | 3.35 |
| Standard deviation | 2.2 | |
| Maximum Distance | 40.7 | |
| #2 | Average Distance | 4.74 |
| Standard deviation | 4.16 | |
| Maximum Distance | 26.37 | |
| #3 | Average Distance | 2.1 |
| Standard deviation | 1.98 | |
| Maximum Distance | 10.03 |
| Case | Process | Material | Material Cost [€] | Labour Cost [€] | Total [€] |
|---|---|---|---|---|---|
| #1 | SLS | PA 12 SLS (Inner Parts) | 112 | 138 | 250 |
| FFF | PLA FFF (Outer Mould) | 16 | 133 | 149 | |
| Moulding | Essil 291 Resin | 12 | 113 | 125 | |
| Total [€] | 140 | 384 | 524 | ||
| #2 | SLS | PA 12 SLS (Outer Mould) | 206 | 140 | 458 |
| PA 12 SLS (Inner Parts) | 112 | ||||
| Moulding | Essil 291 Resin | 12 | 113 | 125 | |
| Total [€] | 330 | 253 | 583 | ||
| #3 | SLS | PA 12 SLS (Inner Parts) | 130 | 138 | 268 |
| FFF | PLA FFF (Outer Mould) | 14 | 133 | 147 | |
| Moulding | Essil 291 Resin | 12 | 113 | 125 | |
| Total [€] | 156 | 384 | 540 | ||
| Case | Segmentation | CAD Modeling | 3D Printing | Silicone Casting | Total [Hours] | |
|---|---|---|---|---|---|---|
| #1 | 45 min | 20 min | SLS (Inner Parts) | 240 | 10 min | 16/24 (One full day) |
| FFF (Outer Mould) | 720 (Overnight) | |||||
| #2 | 38 min | 25 min | SLS (Inner Parts) | 240 | 10 min | 8 (One working day) |
| SLS (Outer Mould) | 240 | |||||
| #3 | 42 min | 20 min | SLS (Inner Parts) | 240 | 10 min | 16/24 (One full day) |
| FFF (Outer Mould) | 720 (Overnight) | |||||
| Age (Years) | Sex | Diagnosis | Surgical Approach | |
|---|---|---|---|---|
| Case #1 | 2 | M | Biliary tract Rhabdomyosarcoma | Extended Right Hepatectomy andRoux-en-Y Hepaticojejunostomy |
| Case #2 | 1 | F | PreText II Hepatoblastoma | Left Hepatectomy |
| Case #3 | 1 | M | Mesenchymal Hamartoma | Tumorectomy (segment IV) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valls-Esteve, A.; Tejo-Otero, A.; Lustig-Gainza, P.; Buj-Corral, I.; Fenollosa-Artés, F.; Rubio-Palau, J.; Barber-Martinez de la Torre, I.; Munuera, J.; Fondevila, C.; Krauel, L. Patient-Specific 3D Printed Soft Models for Liver Surgical Planning and Hands-On Training. Gels 2023, 9, 339. https://doi.org/10.3390/gels9040339
Valls-Esteve A, Tejo-Otero A, Lustig-Gainza P, Buj-Corral I, Fenollosa-Artés F, Rubio-Palau J, Barber-Martinez de la Torre I, Munuera J, Fondevila C, Krauel L. Patient-Specific 3D Printed Soft Models for Liver Surgical Planning and Hands-On Training. Gels. 2023; 9(4):339. https://doi.org/10.3390/gels9040339
Chicago/Turabian StyleValls-Esteve, Arnau, Aitor Tejo-Otero, Pamela Lustig-Gainza, Irene Buj-Corral, Felip Fenollosa-Artés, Josep Rubio-Palau, Ignasi Barber-Martinez de la Torre, Josep Munuera, Constantino Fondevila, and Lucas Krauel. 2023. "Patient-Specific 3D Printed Soft Models for Liver Surgical Planning and Hands-On Training" Gels 9, no. 4: 339. https://doi.org/10.3390/gels9040339