

Tricuspid Valve Regurgitation in Hypoplastic Left Heart Syndrome: Current Insights and Future Perspectives
 ,
,
Abstract
:1. Introduction
2. Tricuspid Regurgitation as a Predictor of Mortality
Failure of TV Repair and Recurrence of TR
3. Identified Indicators of TR in HLHS
3.1. Geometric Differences in TR and Non-TR Cases
3.2. Structural Anomalies as Mechanisms of TR
3.2.1. Discrepancy in Findings with a Longitudinal Cohort
3.2.2. Summary of Primary Structural Findings
3.2.3. Discrepancies in Echocardiographic Findings
3.3. Ventricular Mechanics and Its Relation to TR
3.4. Surgical Decisions and Potential Impacts on TR
3.4.1. Fetal Diagnoses and Pre-Surgical Planning
3.4.2. Norwood: Shunt Selection
3.4.3. Alternatives to the Norwood Procedure
3.4.4. Stage II (Glenn) Operation
3.5. Mechanisms of Post-Repair Recurrent TR
4. Lacking Knowledge and Future Perspectives
4.1. Engineering Insights for an Improved Understanding of TR
4.1.1. Non-Invasive Analysis of Tissue Biomechanics
4.1.2. Computational Modeling
4.2. Statistical Analysis Designs in TR-Related HLHS Research
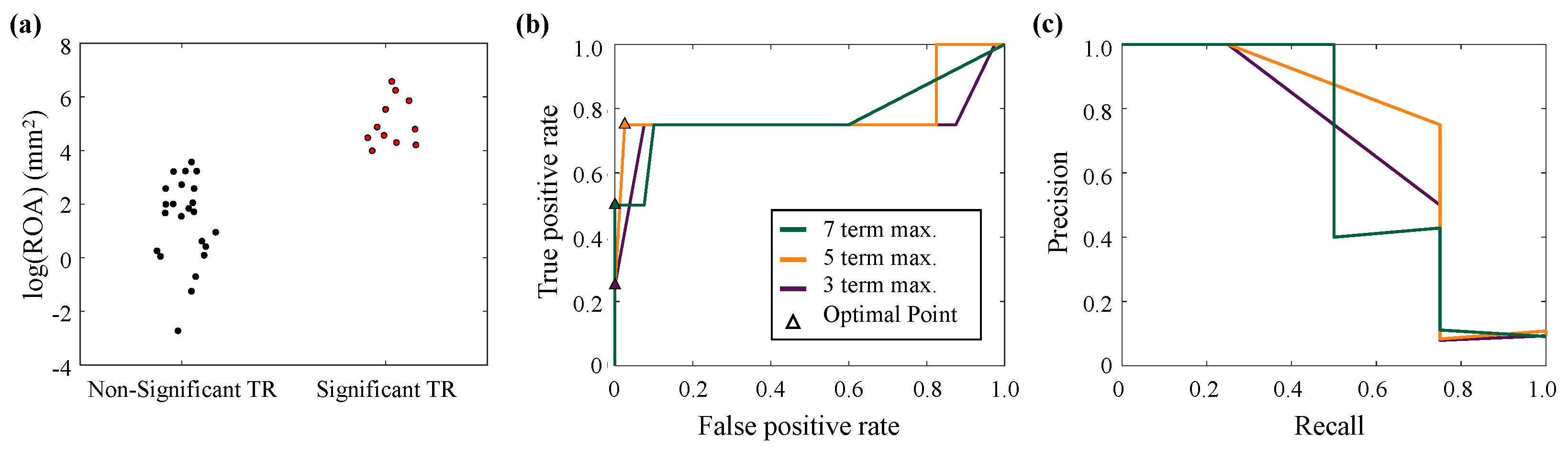
4.2.1. Demonstration of Multivariate Logistic Modeling
4.2.2. Longitudinal Cohorts and Mixed-Effect Models
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tchervenkov, C.I.; Jacobs, J.P.; Weinberg, P.M.; Aiello, V.D.; Béland, M.J.; Colan, S.D.; Elliott, M.J.; Franklin, R.C.; Gaynor, J.W.; Krogmann, O.N.; et al. The nomenclature, definition and classification of hypoplastic left heart syndrome. Cardiol. Young 2006, 16, 339–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabrodi, M.; Mastropietro, C.W. Hypoplastic left heart syndrome: From comfort care to long-term survival. Pediatr. Res. 2017, 81, 142–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraf, A.; Book, W.M.; Nelson, T.J.; Xu, C. Hypoplastic left heart syndrome: From bedside to bench and back. J. Mol. Cell. Cardiol. 2019, 135, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Norwood, W.I.; Kirklin, J.K.; Sanders, S.P. Hypoplastic left heart syndrome: Experience with palliative surgery. Am. J. Cardiol. 1980, 45, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, J.; Pigott, J.D.; Murphy, J.D.; Barber, G.; Norwood, W.I. Palliative reconstructive surgery for hypoplastic left heart syndrome. Ann. Thorac. Surg. 1988, 45, 122–128. [Google Scholar] [CrossRef]
- Sano, S.; Ishino, K.; Kawada, M.; Arai, S.; Kasahara, S.; Asai, T.; Masuda, Z.; Takeuchi, M.; Ohtsuki, S. Right ventricle–pulmonary artery shunt in first-stage palliation of hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2003, 126, 504–509. [Google Scholar] [CrossRef] [Green Version]
- Pridjian, A.K.; Mendelsohn, A.M.; Lupinetti, F.M.; Beekman III, R.H.; Dick II, M.; Serwer, G.; Bove, E.L. Usefulness of the bidirectional Glenn procedure as staged reconstruction for the functional single ventricle. Am. J. Cardiol. 1993, 71, 959–962. [Google Scholar] [CrossRef] [Green Version]
- Scheurer, M.A.; Hill, E.G.; Vasuki, N.; Maurer, S.; Graham, E.M.; Bandisode, V.; Shirali, G.S.; Atz, A.M.; Bradley, S.M. Survival after bidirectional cavopulmonary anastomosis: Analysis of preoperative risk factors. J. Thorac. Cardiovasc. Surg. 2007, 134, 82–89.e2. [Google Scholar] [CrossRef] [Green Version]
- Fontan, F.; Baudet, E. Surgical repair of tricuspid atresia. Thorax 1971, 26, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Salazar, J.D.; Zafar, F.; Siddiqui, K.; Coleman, R.D.; Morales, D.L.; Heinle, J.S.; Rossano, J.W.; Mossad, E.B.; Fraser, C.D., Jr. Fenestration during Fontan palliation: Now the exception instead of the rule. J. Thorac. Cardiovasc. Surg. 2010, 140, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Ono, M.; Boethig, D.; Goerler, H.; Lange, M.; Westhoff-Bleck, M.; Breymann, T. Clinical outcome of patients 20 years after Fontan operation–Effect of fenestration on late morbidity. Eur. J. Cardio-Thorac. Surg. 2006, 30, 923–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pundi, K.N.; Johnson, J.N.; Dearani, J.A.; Pundi, K.N.; Li, Z.; Hinck, C.A.; Dahl, S.H.; Cannon, B.C.; O’Leary, P.W.; Driscoll, D.J.; et al. 40-year follow-up after the Fontan operation: Long-term outcomes of 1052 patients. J. Am. Coll. Cardiol. 2015, 66, 1700–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poh, C.; d’Udekem, Y. Life after surviving Fontan surgery: A meta-analysis of the incidence and predictors of late death. Heart Lung Circ. 2018, 27, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Barber, G.; Helton, J.G.; Aglira, B.A.; Chin, A.J.; Murphy, J.D.; Pigott, J.D.; Norwood, W.I. The significance of tricuspid regurgitation in hypoplastic left-heart syndrome. Am. Heart J. 1988, 116, 1563–1567. [Google Scholar] [CrossRef] [PubMed]
- Reyes 2nd, A.; Bove, E.L.; Mosca, R.S.; Kulik, T.J.; Ludomirsky, A. Tricuspid valve repair in children with hypoplastic left heart syndrome during staged surgical reconstruction. Circulation 1997, 96, II-341-345. [Google Scholar]
- Sano, S.; Huang, S.C.; Kasahara, S.; Yoshizumi, K.; Kotani, Y.; Ishino, K. Risk factors for mortality after the Norwood procedure using right ventricle to pulmonary artery shunt. Ann. Thorac. Surg. 2009, 87, 178–186. [Google Scholar] [CrossRef]
- Elmi, M.; Hickey, E.J.; Williams, W.G.; Van Arsdell, G.; Caldarone, C.A.; McCrindle, B.W. Long-term tricuspid valve function after Norwood operation. J. Thorac. Cardiovasc. Surg. 2011, 142, 1341–1347. [Google Scholar] [CrossRef] [Green Version]
- Sugiura, J.; Nakano, T.; Oda, S.; Usui, A.; Ueda, Y.; Kado, H. Effects of tricuspid valve surgery on tricuspid regurgitation in patients with hypoplastic left heart syndrome: A non-randomized series comparing surgical and non-surgical cases. Eur. J. Cardio-Thorac. Surg. 2014, 46, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Alsoufi, B.; Sinha, R.; McCracken, C.; Figueroa, J.; Altin, F.; Kanter, K. Outcomes and risk factors associated with tricuspid valve repair in children with hypoplastic left heart syndrome. Eur. J. Cardio-Thorac. Surg. 2018, 54, 993–1000. [Google Scholar] [CrossRef]
- Ono, M.; Mayr, B.; Burri, M.; Piber, N.; Röhlig, C.; Strbad, M.; Cleuziou, J.; Hager, A.; Hörer, J.; Lange, R. Tricuspid valve repair in children with hypoplastic left heart syndrome: Impact of timing and mechanism on outcome. Eur. J. Cardio-Thorac. Surg. 2020, 57, 1083–1090. [Google Scholar] [CrossRef]
- Starnes, V.A.; Griffin, M.L.; Pitlick, P.T.; Bernstein, D.; Baum, D.; Ivens, K.; Shumway, N.E. Current approach to hypoplastic left heart syndrome:Palliation, transplantation, or both? J. Thorac. Cardiovasc. Surg. 1992, 104, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, K.; Ogawa, K.; Hishitani, T.; Kitazawa, R.; Uehara, R. Hypoplastic left heart syndrome: Duration of survival without surgical intervention. Am. Heart J. 1999, 137, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.; Gaynor, J.W.; Bridges, N.D.; Wernovsky, G.; Montenegro, L.M.; Godinez, R.I.; Spray, T.L. Early survival of infants weighing 2.5 kilograms or less undergoing first-stage reconstruction for hypoplastic left heart syndrome. Circulation 1999, 100, II167–II170. [Google Scholar] [CrossRef]
- Lang, P.; Norwood, W.I. Hemodynamic assessment after palliative surgery for hypoplastic left heart syndrome. Circulation 1983, 68, 104–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helton, J.; Aglira, B.; Chin, A.; Murphy, J.; Pigott, J.; Norwood, W. Analysis of potential anatomic or physiologic determinants of outcome of palliative surgery for hypoplastic left heart syndrome. Circulation 1986, 74, 170–176. [Google Scholar]
- Hraška, V.; Nosál, M.; Sỳkora, P.; Soják, V.; Šagát, M.; Kunovskỳ, P. Results of modified Norwood’s operation for hypoplastic left heart syndrome. Eur. J. Cardio-Thorac. Surg. 2000, 18, 214–219. [Google Scholar] [CrossRef] [Green Version]
- Jonas, R.A.; Hansen, D.D.; Cook, N.; Wessel, D. Anatomic subtype and survival after reconstructive operation for hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 1994, 107, 1121–1128. [Google Scholar] [CrossRef]
- Forbess, J.M.; Cook, N.; Roth, S.J.; Serraf, A.; Mayer, J.E., Jr.; Jonas, R.A. Ten-year institutional experience with palliative surgery for hypoplastic left heart syndrome: Risk factors related to stage I mortality. Circulation 1995, 92, 262–266. [Google Scholar] [CrossRef]
- Hirsch, J.; Ohye, R.; Devaney, E.; Goldberg, C.; Bove, E. The lateral tunnel Fontan procedure for hypoplastic left heart syndrome: Results of 100 consecutive patients. Pediatr. Cardiol. 2007, 28, 426–432. [Google Scholar] [CrossRef]
- Hehir, D.A.; Dominguez, T.E.; Ballweg, J.A.; Ravishankar, C.; Marino, B.S.; Bird, G.L.; Nicolson, S.C.; Spray, T.L.; Gaynor, J.W.; Tabbutt, S. Risk factors for interstage death after stage 1 reconstruction of hypoplastic left heart syndrome and variants. J. Thorac. Cardiovasc. Surg. 2008, 136, 94–99.e3. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.C.; Farrell, P.E., Jr.; Murdison, K.A.; Baffa, J.M.; Barber, G.; Norwood, W.I.; Murphy, J.D. Hypoplastic left heart syndrome: Hemodynamic and angiographic assessment after initial reconstructive surgery and relevance to modified Fontan procedure. J. Am. Coll. Cardiol. 1991, 17, 1143–1149. [Google Scholar] [CrossRef] [Green Version]
- Mosca, R.S.; Kulik, T.J.; Goldberg, C.S.; Vermilion, R.P.; Charpie, J.R.; Crowley, D.C.; Bove, E.L. Early results of the Fontan procedure in one hundred consecutive patients with hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2000, 119, 1110–1118. [Google Scholar] [CrossRef] [Green Version]
- Gaynor, J.W.; Bridges, N.D.; Cohen, M.I.; Mahle, W.T.; DeCampli, W.M.; Steven, J.M.; Nicolson, S.C.; Spray, T.L. Predictors of outcome after the Fontan operation: Is hypoplastic left heart syndrome still a risk factor? J. Thorac. Cardiovasc. Surg. 2002, 123, 237–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamszad, P.; Gospin, T.A.; Hong, B.J.; McKenzie, E.D.; Petit, C.J. Impact of preoperative risk factors on outcomes after Norwood palliation for hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2014, 147, 897–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlo, W.F.; Carberry, K.E.; Heinle, J.S.; Morales, D.L.; McKenzie, E.D.; Fraser, C.D., Jr.; Nelson, D.P. Interstage attrition between bidirectional Glenn and Fontan palliation in children with hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2011, 142, 511–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wamala, I.; Friedman, K.G.; Saeed, M.Y.; Gauvreau, K.; Gellis, L.; Borisuk, M.; Kaza, A.; Emani, S.; Del Nido, P.J.; Baird, C.W. Tricuspid valve repair concomitant with the Norwood operation among babies with hypoplastic left heart syndrome. Eur. J. Cardio-Thorac. Surg. 2022, 62, ezac033. [Google Scholar] [CrossRef]
- Son, J.S.; James, A.; Fan, C.P.S.; Mertens, L.; McCrindle, B.W.; Manlhiot, C.; Friedberg, M.K. Prognostic value of serial echocardiography in hypoplastic left heart syndrome. Circ. Cardiovasc. Imaging 2018, 11, e006983. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, A.V.; Lasso, A.; Nam, H.H.; Faerber, J.; Aly, A.H.; Pouch, A.M.; Scanlan, A.B.; McGowan, F.X.; Mercer-Rosa, L.; Cohen, M.S.; et al. Dynamic three-dimensional geometry of the tricuspid valve annulus in hypoplastic left heart syndrome with a Fontan circulation. J. Am. Soc. Echocardiogr. 2019, 32, 655–666. [Google Scholar] [CrossRef]
- Nii, M.; Guerra, V.; Roman, K.S.; Macgowan, C.K.; Smallhorn, J.F. Three-dimensional tricuspid annular function provides insight into the mechanisms of tricuspid valve regurgitation in classic hypoplastic left heart syndrome. J. Am. Soc. Echocardiogr. 2006, 19, 391–402. [Google Scholar] [CrossRef]
- Takahashi, K.; Inage, A.; Rebeyka, I.; Ross, D.; Thompson, R.; Mackie, A.; Smallhorn, J. Real-time 3-dimensional echocardiography provides new insight into mechanisms of tricuspid valve regurgitation in patients with hypoplastic left heart syndrome. Circulation 2009, 120, 1091–1098. [Google Scholar] [CrossRef] [Green Version]
- Kutty, S.; Colen, T.; Thompson, R.B.; Tham, E.; Li, L.; Vijarnsorn, C.; Polak, A.; Truong, D.T.; Danford, D.A.; Smallhorn, J.F.; et al. Tricuspid regurgitation in hypoplastic left heart syndrome: Mechanistic insights from 3 to dimensional echocardiography and relationship with outcomes. Circ. Cardiovasc. Imaging 2014, 7, 765–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shigemitsu, S.; Mah, K.; Thompson, R.B.; Grenier, J.; Lin, L.Q.; Silmi, A.; Beigh, M.V.R.; Khoo, N.S.; Colen, T. Tricuspid valve tethering is associated with residual regurgitation after valve repair in hypoplastic left heart syndrome: A three-dimensional echocardiographic study. J. Am. Soc. Echocardiogr. 2021, 34, 1199–1210. [Google Scholar] [CrossRef] [PubMed]
- Mah, K.; Khoo, N.S.; Martin, B.J.; Maruyama, M.; Alvarez, S.; Rebeyka, I.M.; Smallhorn, J.; Colen, T. Insights from 3D echocardiography in hypoplastic left heart syndrome patients undergoing TV repair. Pediatr. Cardiol. 2022, 43, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Bautista-Hernandez, V.; Brown, D.W.; Loyola, H.; Myers, P.O.; Borisuk, M.; Pedro, J.; Baird, C.W. Mechanisms of tricuspid regurgitation in patients with hypoplastic left heart syndrome undergoing tricuspid valvuloplasty. J. Thorac. Cardiovasc. Surg. 2014, 148, 832–840. [Google Scholar] [CrossRef] [Green Version]
- Bharucha, T.; Honjo, O.; Seller, N.; Atlin, C.; Redington, A.; Caldarone, C.A.; Van Arsdell, G.; Mertens, L. Mechanisms of tricuspid valve regurgitation in hypoplastic left heart syndrome: A case-matched echocardiographic–surgical comparison study. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 135–141. [Google Scholar] [CrossRef]
- Colen, T.; Kutty, S.; Thompson, R.B.; Tham, E.; Mackie, A.S.; Li, L.; Truong, D.T.; Maruyama, M.; Smallhorn, J.F.; Khoo, N.S. Tricuspid valve adaptation during the first interstage period in hypoplastic left heart syndrome. J. Am. Soc. Echocardiogr. 2018, 31, 624–633. [Google Scholar] [CrossRef]
- Lin, L.Q.; Hatami, S.; Coe, J.Y.; Colen, T.M.; Sergi, C.; Thompson, R.; Di Martino, E.S.; Herzog, W.; Sara, Z.A.; Freed, D.H.; et al. A novel right ventricular volume and pressure loaded piglet heart model for the study of tricuspid valve function. J. Vis. Exp. 2020, 161, e61251. [Google Scholar] [CrossRef]
- Mah, K.; Khoo, N.S.; Tham, E.; Yaskina, M.; Maruyama, M.; Martin, B.J.; Alvarez, S.; Alami, N.; Rebeyka, I.M.; Smallhorn, J.; et al. Tricuspid regurgitation in hypoplastic left heart syndrome: Three-dimensional echocardiography provides additional information in describing jet location. J. Am. Soc. Echocardiogr. 2021, 34, 529–536. [Google Scholar] [CrossRef]
- Ohye, R.G.; Gomez, C.A.; Goldberg, C.S.; Graves, H.L.; Devaney, E.J.; Bove, E.L. Repair of the tricuspid valve in hypoplastic left heart syndrome. Cardiol. Young 2006, 16, 21–26. [Google Scholar] [CrossRef]
- Ohye, R.G.; Gomez, C.A.; Goldberg, C.S.; Graves, H.L.; Devaney, E.J.; Bove, E.L. Tricuspid valve repair in hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2004, 127, 465–472. [Google Scholar] [CrossRef] [Green Version]
- Bellsham-Revell, H.R.; Tibby, S.M.; Bell, A.J.; Witter, T.; Simpson, J.; Beerbaum, P.; Anderson, D.; Austin, C.B.; Greil, G.F.; Razavi, R. Serial magnetic resonance imaging in hypoplastic left heart syndrome gives valuable insight into ventricular and vascular adaptation. J. Am. Coll. Cardiol. 2013, 61, 561–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsha, D.; Li, L.; Joseph, N.; Kutty, S.; Friedberg, M.K. Association of left ventricular size with regional right ventricular mechanics in hypoplastic left heart syndrome. Int. J. Cardiol. 2020, 298, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laohachai, K.; Winlaw, D.; Sholler, G.; Veerappan, S.; Cole, A.; Ayer, J. The degree of left ventricular hypoplasia is associated with tricuspid regurgitation severity in infants with hypoplastic left heart syndrome. Pediatr. Cardiol. 2019, 40, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Muthurangu, V.; Taylor, A.M.; Hegde, S.R.; Johnson, R.; Tulloh, R.; Simpson, J.M.; Qureshi, S.; Rosenthal, E.; Baker, E.; Anderson, D.; et al. Cardiac magnetic resonance imaging after stage I Norwood operation for hypoplastic left heart syndrome. Circulation 2005, 112, 3256–3263. [Google Scholar] [CrossRef] [Green Version]
- Tongsong, T.; Sittiwangkul, R.; Khunamornpong, S.; Wanapirak, C. Prenatal sonographic features of isolated hypoplastic left heart syndrome. J. Clin. Ultrasound 2005, 33, 367–371. [Google Scholar] [CrossRef]
- Mart, C.R.; Eckhauser, A.W.; Murri, M.; Su, J.T. A systematic method for using 3D echocardiography to evaluate tricuspid valve insufficiency in hypoplastic left heart syndrome. Ann. Pediatr. Cardiol. 2014, 7, 193–200. [Google Scholar] [CrossRef]
- Tworetzky, W.; McElhinney, D.B.; Reddy, V.M.; Brook, M.M.; Hanley, F.L.; Silverman, N.H. Improved surgical outcome after fetal diagnosis of hypoplastic left heart syndrome. Circulation 2001, 103, 1269–1273. [Google Scholar] [CrossRef] [Green Version]
- Kipps, A.K.; Feuille, C.; Azakie, A.; Hoffman, J.I.; Tabbutt, S.; Brook, M.M.; Moon-Grady, A.J. Prenatal diagnosis of hypoplastic left heart syndrome in current era. Am. J. Cardiol. 2011, 108, 421–427. [Google Scholar] [CrossRef]
- Stoica, S.C.; Philips, A.B.; Egan, M.; Rodeman, R.; Chisolm, J.; Hill, S.; Cheatham, J.P.; Galantowicz, M.E. The retrograde aortic arch in the hybrid approach to hypoplastic left heart syndrome. Ann. Thorac. Surg. 2009, 88, 1939–1947. [Google Scholar] [CrossRef]
- Tworetzky, W.; Wilkins-Haug, L.; Jennings, R.W.; van der Velde, M.E.; Marshall, A.C.; Marx, G.R.; Colan, S.D.; Benson, C.B.; Lock, J.E.; Perry, S.B. Balloon dilation of severe aortic stenosis in the fetus: Potential for prevention of hypoplastic left heart syndrome: Candidate selection, technique, and results of successful intervention. Circulation 2004, 110, 2125–2131. [Google Scholar] [CrossRef] [Green Version]
- Szwast, A.; Tian, Z.; McCann, M.; Donaghue, D.; Rychik, J. Vasoreactive response to maternal hyperoxygenation in the fetus with hypoplastic left heart syndrome. Circ. Cardiovasc. Imaging 2010, 3, 172–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freud, L.R.; McElhinney, D.B.; Marshall, A.C.; Marx, G.R.; Friedman, K.G.; del Nido, P.J.; Emani, S.M.; Lafranchi, T.; Silva, V.; Wilkins-Haug, L.E.; et al. Fetal aortic valvuloplasty for evolving hypoplastic left heart syndrome: Postnatal outcomes of the first 100 patients. Circulation 2014, 130, 638–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sano, S.; Ishino, K.; Kado, H.; Shiokawa, Y.; Sakamoto, K.; Yokota, M.; Kawada, M. Outcome of right ventricle–to–pulmonary artery shunt in first-stage palliation of hypoplastic left heart syndrome: A multi-institutional study. Ann. Thorac. Surg. 2004, 78, 1951–1958. [Google Scholar] [CrossRef] [PubMed]
- Asakai, H.; Galati, J.C.; Weskamp, S.; Jones, B.; Millar, J.; Konstantinov, I.E.; d’Udekem, Y.; Brizard, C.P.; Cheung, M.M. Impact of Blalock-Taussig shunt size on tricuspid regurgitation in hypoplastic left heart syndrome. Ann. Thorac. Surg. 2014, 97, 2123–2128. [Google Scholar] [CrossRef] [PubMed]
- Pizarro, C.; Mroczek, T.; Malec, E.; Norwood, W.I. Right ventricle to pulmonary artery conduit reduces interim mortality after stage 1 Norwood for hypoplastic left heart syndrome. Ann. Thorac. Surg. 2004, 78, 1959–1964. [Google Scholar] [CrossRef] [PubMed]
- Cua, C.L.; Thiagarajan, R.R.; Gauvreau, K.; Lai, L.; Costello, J.M.; Wessel, D.L.; Pedro, J.; Mayer, J.E., Jr.; Newburger, J.W.; Laussen, P.C. Early postoperative outcomes in a series of infants with hypoplastic left heart syndrome undergoing stage I palliation operation with either modified Blalock-Taussig shunt or right ventricle to pulmonary artery conduit. Pediatr. Crit. Care Med. 2006, 7, 238–244. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.Y.; Phan, K.; Ayer, J.; Celermajer, D.S.; Winlaw, D.S. Long term survival of hypoplastic left heart syndrome infants: Meta-analysis comparing outcomes from the modified Blalock–Taussig shunt and the right ventricle to pulmonary artery shunt. Int. J. Cardiol. 2018, 254, 107–116. [Google Scholar] [CrossRef]
- Bautista-Hernandez, V.; Scheurer, M.; Thiagarajan, R.; Salvin, J.; Pigula, F.A.; Emani, S.; Fynn-Thompson, F.; Loyola, H.; Schiff, J.; del Nido, P.J.; et al. Right ventricle and tricuspid valve function at midterm after the Fontan operation for hypoplastic left heart syndrome: Impact of shunt type. Pediatr. Cardiol. 2011, 32, 160–166. [Google Scholar] [CrossRef]
- Galantowicz, M.; Cheatham, J.P. Lessons learned from the development of a new hybrid strategy for the management of hypoplastic left heart syndrome. Pediatr. Cardiol. 2005, 26, 190–199. [Google Scholar] [CrossRef]
- Lim, D.; Peeler, B.; Matherne, G.; Kron, I.; Gutgesell, H. Risk-stratified approach to hybrid transcatheter–surgical palliation of hypoplastic left heart syndrome. Pediatr. Cardiol. 2006, 27, 91–95. [Google Scholar] [CrossRef]
- Philip, J.; Reyes, K.; Ebraheem, M.; Gupta, D.; Fudge, J.C.; Bleiweis, M.S. Hybrid procedure with pulsatile ventricular assist device for hypoplastic left heart syndrome awaiting transplantation. J. Thorac. Cardiovasc. Surg. 2019, 158, e59–e61. [Google Scholar] [CrossRef]
- Chetan, D.; Kotani, Y.; Jacques, F.; Poynter, J.A.; Benson, L.N.; Lee, K.J.; Chaturvedi, R.R.; Friedberg, M.K.; Van Arsdell, G.S.; Caldarone, C.A.; et al. Surgical palliation strategy does not affect interstage ventricular dysfunction or atrioventricular valve regurgitation in children with hypoplastic left heart syndrome and variants. Circulation 2013, 128, S205–S212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grotenhuis, H.B.; Ruijsink, B.; Chetan, D.; Dragulescu, A.; Friedberg, M.K.; Kotani, Y.; Caldarone, C.A.; Honjo, O.; Mertens, L.L. Impact of Norwood versus hybrid palliation on cardiac size and function in hypoplastic left heart syndrome. Heart 2016, 102, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Fraser, C.D., Jr.; Mee, R.B. Modified Norwood procedure for hypoplastic left heart syndrome. Ann. Thorac. Surg. 1995, 60, S546–S549. [Google Scholar] [CrossRef] [PubMed]
- Ashburn, D.A.; McCrindle, B.W.; Tchervenkov, C.I.; Jacobs, M.L.; Lofland, G.K.; Bove, E.L.; Spray, T.L.; Williams, W.G.; Blackstone, E.H.; Society, C.H.S. Outcomes after the Norwood operation in neonates with critical aortic stenosis or aortic valve atresia. J. Thorac. Cardiovasc. Surg. 2003, 125, 1070–1082. [Google Scholar] [CrossRef] [Green Version]
- Kasnar-Samprec, J.; Kühn, A.; Hörer, J.; Vogt, M.; Cleuziou, J.; Lange, R.; Schreiber, C. Unloading of right ventricle by bidirectional superior cavopulmonary anastomosis in hypoplastic left heart syndrome patients promotes remodeling of systemic right ventricle but does not improve tricuspid regurgitation. J. Thorac. Cardiovasc. Surg. 2012, 144, 1102–1109. [Google Scholar] [CrossRef] [Green Version]
- Hansen, J.H.; Uebing, A.; Furck, A.K.; Scheewe, J.; Jung, O.; Fischer, G.; Kramer, H.H. Risk factors for adverse outcome after superior cavopulmonary anastomosis for hypoplastic left heart syndrome. Eur. J. Cardio-Thorac. Surg. 2011, 40, e43–e49. [Google Scholar] [CrossRef]
- Salik, I.; Mehta, B.; Ambati, S. Bidirectional Glenn Procedure or Hemi-Fontan; StatPearls Publishing: Tampa, FL, USA, 2020. [Google Scholar]
- Douglas, W.I.; Goldberg, C.S.; Mosca, R.S.; Law, I.H.; Bove, E.L. Hemi-Fontan procedure for hypoplastic left heart syndrome: Outcome and suitability for Fontan. Ann. Thorac. Surg. 1999, 68, 1361–1367. [Google Scholar] [CrossRef]
- Edelson, J.B.; Ravishankar, C.; Griffis, H.; Zhang, X.; Faerber, J.; Gardner, M.M.; Naim, M.Y.; Macsio, C.E.; Glatz, A.C.; Goldberg, D.J. A comparison of bidirectional Glenn vs. Hemi-Fontan procedure: An analysis of the single ventricle reconstruction trial public use dataset. Pediatr. Cardiol. 2020, 41, 1166–1172. [Google Scholar] [CrossRef]
- Alsoufi, B.; Manlhiot, C.; Awan, A.; Alfadley, F.; Al-Ahmadi, M.; Al-Wadei, A.; McCrindle, B.W.; Al-Halees, Z. Current outcomes of the Glenn bidirectional cavopulmonary connection for single ventricle palliation. Eur. J. Cardio-Thorac. Surg. 2012, 42, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Ugaki, S.; Khoo, N.S.; Ross, D.B.; Rebeyka, I.M.; Adatia, I. Tricuspid valve repair improves early right ventricular and tricuspid valve remodeling in patients with hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2013, 145, 446–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bove, E.L.; Ohye, R.G.; Devaney, E.J.; Hirsch, J. Tricuspid valve repair for hypoplastic left heart syndrome and the failing right ventricle. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2007, 10, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Honjo, O.; Atlin, C.R.; Mertens, L.; Al-Radi, O.O.; Redington, A.N.; Caldarone, C.A.; Van Arsdell, G.S. Atrioventricular valve repair in patients with functional single-ventricle physiology: Impact of ventricular and valve function and morphology on survival and reintervention. J. Thorac. Cardiovasc. Surg. 2011, 142, 326–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, C.J.; Trimble, E.J.; Johnson, E.L.; Baumwart, R.; Jolley, M.A.; Mir, A.; Burkhart, H.M.; Lee, C.H. A pilot investigation of the tricuspid valve annulus in newborns with hypoplastic left heart syndrome. JTCVS Open 2022, 10, 324–339. [Google Scholar] [CrossRef]
- Vicory, J.; Herz, C.; Allemang, D.; Nam, H.H.; Cianciulli, A.; Vigil, C.; Han, Y.; Lasso, A.; Jolley, M.A.; Paniagua, B. Statistical shape analysis of the tricuspid valve in hypoplastic left heart syndrome. In Proceedings of the International Workshop on Statistical Atlases and Computational Models of the Heart, Singapore, 18 September 2021; pp. 132–140. [Google Scholar] [CrossRef]
- Herz, C.; Pace, D.F.; Nam, H.H.; Lasso, A.; Dinh, P.; Flynn, M.; Cianciulli, A.; Golland, P.; Jolley, M.A. Segmentation of tricuspid valve leaflets from transthoracic 3D echocardiograms of children with hypoplastic left heart syndrome using deep learning. Front. Cardiovasc. Med. 2021, 8, 1839. [Google Scholar] [CrossRef]
- Chen, J.; Li, H.; He, G.; Yao, F.; Lai, L.; Yao, J.; Xie, L. Automatic 3D mitral valve leaflet segmentation and validation of quantitative measurement. Biomed. Signal Process. Control 2023, 79, 104166. [Google Scholar] [CrossRef]
- Bove, E.L.; Migliavacca, F.; de Leval, M.R.; Balossino, R.; Pennati, G.; Lloyd, T.R.; Khambadkone, S.; Hsia, T.Y.; Dubini, G. Use of mathematic modeling to compare and predict hemodynamic effects of the modified Blalock–Taussig and right ventricle–pulmonary artery shunts for hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2008, 136, 312–320. [Google Scholar] [CrossRef] [Green Version]
- Laurence, D.W.; Johnson, E.L.; Hsu, M.C.; Baumwart, R.; Mir, A.; Burkhart, H.M.; Holzapfel, G.A.; Wu, Y.; Lee, C.H. A pilot in silico modeling-based study of the pathological effects on the biomechanical function of tricuspid valves. Int. J. Numer. Methods Biomed. Eng. 2020, 36, e3346. [Google Scholar] [CrossRef]
- Lasso, A.; Nam, H.H.; Cianciulli, A.; Pieper, S.; Drouin, S.; Pinter, C.; St-Onge, S.; Vigil, C.; Ching, S.; Sutherland, K.; et al. SlicerHeart: An open-source computing platform for cardiac image analysis and modeling. Front. Cardiovasc. Med. 2022, 9, 2384. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Ching, S.; Maas, S.A.; Lasso, A.; Sabin, P.; Weiss, J.A.; Jolley, M.A. A computational framework for atrioventricular valve modeling using open-source software. J. Biomech. Eng. 2022, 144, 101012. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Sacks, M.S. An inverse modeling approach for semilunar heart valve leaflet mechanics: Exploitation of tissue structure. Biomech. Model. Mechanobiol. 2016, 15, 909–932. [Google Scholar] [CrossRef] [PubMed]
- Kusiak, A.; Caldarone, C.A.; Kelleher, M.D.; Lamb, F.S.; Persoon, T.J.; Burns, A. Hypoplastic left heart syndrome: Knowledge discovery with a data mining approach. Comput. Biol. Med. 2006, 36, 21–40. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.L.; Laurence, D.W.; Xu, F.; Crisp, C.E.; Mir, A.; Burkhart, H.M.; Lee, C.H.; Hsu, M.C. Parameterization, geometric modeling, and isogeometric analysis of tricuspid valves. Comput. Methods Appl. Mech. Eng. 2021, 384, 113960. [Google Scholar] [CrossRef]
- Fonti, V.; Belitser, E. Feature selection using LASSO. VU Amst. Res. Pap. Bus. Anal. 2017, 30, 1–25. [Google Scholar]
- Waljee, A.K.; Higgins, P.D.; Singal, A.G. A primer on predictive models. Clin. Transl. Gastroenterol. 2014, 5, e44. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Faraway, J.J. Extending the Linear Model with R: Generalized Linear, Mixed Effects and Nonparametric Regression Models; Chapman and Hall/CRC: Boca Raton, FL, USA, 2016. [Google Scholar]
- Vande Geest, J.P.; Wang, D.H.; Wisniewski, S.R.; Makaroun, M.S.; Vorp, D.A. Towards a noninvasive method for determination of patient-specific wall strength distribution in abdominal aortic aneurysms. Ann. Biomed. Eng. 2006, 34, 1098–1106. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Geometry Parameter | Parameter Range | Description |
|---|---|---|
| Anterior–Posterior Diameter (mm) | 100–200% of the average value for emulating annular dilation | |
| Septal–Lateral Diameter (mm) | 100–200% of the average value for emulating annular dilation | |
| Bending Angle (deg) | % of the average value | |
| Area Change (%) | [5, 20] | Covering the range described in Section 3.1 |
| Septal Leaflet Height (mm) | % of the average value | |
| Anterior Leaflet Height (mm) | % of the average value | |
| Posterior Leaflet Height (mm) | % of the average value |
| Maximum Number of Parameters | 3 | 5 | 7 |
|---|---|---|---|
| Intercept Term | |||
| Anterior–Posterior Diameter (mm) | 0 | ||
| Septal–Lateral Diameter (mm) | |||
| Bending Angle (deg) | 0 | 0 | |
| Septal Leaflet Height (mm) | 0 | 0 | 0 |
| Anterior Leaflet Height (mm) | 0 | ||
| Posterior Leaflet Height(mm) | |||
| Area Change (%) | |||
| Area Under the Curve (-) | |||
| Sensitivity (-) | |||
| Specificity (-) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ross, C.J.; Mir, A.; Burkhart, H.M.; Holzapfel, G.A.; Lee, C.-H. Tricuspid Valve Regurgitation in Hypoplastic Left Heart Syndrome: Current Insights and Future Perspectives. J. Cardiovasc. Dev. Dis. 2023, 10, 111. https://doi.org/10.3390/jcdd10030111
Ross CJ, Mir A, Burkhart HM, Holzapfel GA, Lee C-H. Tricuspid Valve Regurgitation in Hypoplastic Left Heart Syndrome: Current Insights and Future Perspectives. Journal of Cardiovascular Development and Disease. 2023; 10(3):111. https://doi.org/10.3390/jcdd10030111
Chicago/Turabian StyleRoss, Colton J., Arshid Mir, Harold M. Burkhart, Gerhard A. Holzapfel, and Chung-Hao Lee. 2023. "Tricuspid Valve Regurgitation in Hypoplastic Left Heart Syndrome: Current Insights and Future Perspectives" Journal of Cardiovascular Development and Disease 10, no. 3: 111. https://doi.org/10.3390/jcdd10030111