
Role of Antiplatelet Therapy in Patients with Severe Coronary Artery Disease Undergoing Coronary Artery Endarterectomy within Coronary Artery Bypass Surgery ψ
 , ,
, , 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Population
2.2. Surgery
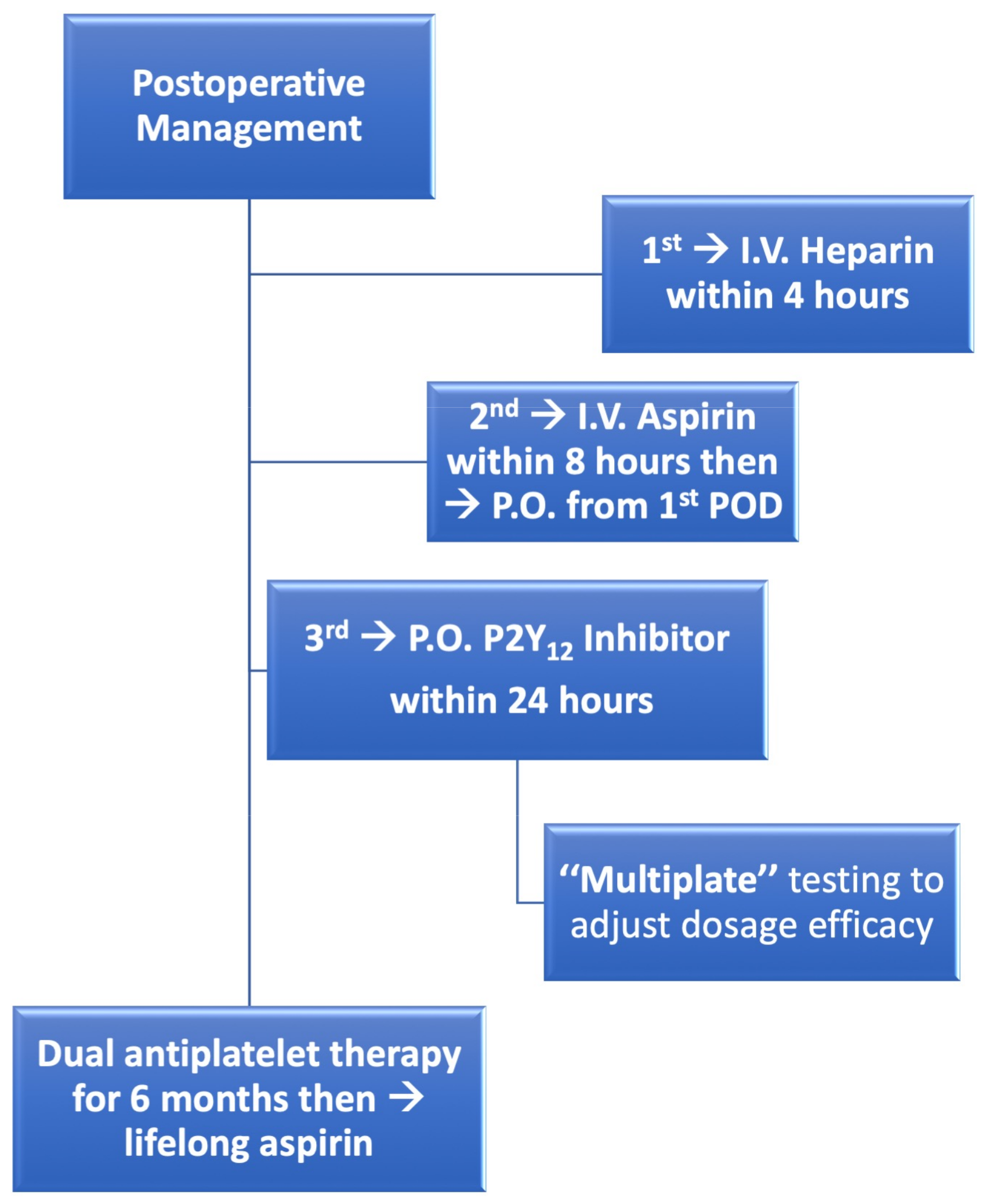
2.3. Postoperative Management
2.4. Endpoints
2.5. Statistical Analysis
3. Results
3.1. Patients’ Demographics
3.2. Early Outcomes
3.3. Late Outcomes
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Longmire, W.P., Jr.; Cannon, J.A.; Kattus, A.A. Direct-vision coronary endarterectomy for angina pectoris. N. Engl. J. Med. 1958, 259, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.P.; May, A.; Lemmon, W.M. Survival after coronary endarterectomy in man. J. Am. Med. Assoc. 1957, 164, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Shehada, S.-E.; Mourad, F.; Balaj, I.; El Gabry, M.; Wendt, D.; Thielmann, M.; Schlosser, T.; Jakob, H. Long-Term Outcomes of Coronary Endarterectomy in Patients With Complete Imaging Follow-Up. Semin. Thorac. Cardiovasc. Surg. 2020, 32, 730–737. [Google Scholar] [CrossRef] [Green Version]
- Nishigawa, K.; Fukui, T.; Yamazaki, M.; Takanashi, S. Ten-Year Experience of Coronary Endarterectomy for the Diffusely Diseased Left Anterior Descending Artery. Ann. Thorac. Surg. 2017, 103, 710–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Gu, C.; Yu, W.; Gao, M.; Yu, Y. Short- and Long-Term Patient Outcomes From Combined Coronary Endarterectomy and Coronary Artery Bypass Grafting: A Meta-Analysis of 63,730 Patients (PRISMA). Medicine 2015, 94, e1781. [Google Scholar] [CrossRef]
- Soylu, E.; Harling, L.; Ashrafian, H.; Casula, R.; Kokotsakis, J.; Athanasiou, T. Adjunct coronary endarterectomy increases myocardial infarction and early mortality after coronary artery bypass grafting: A meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2014, 19, 462–473. [Google Scholar] [CrossRef] [Green Version]
- Lemma, M.; Beretta, L.; Vanelli, P.; Santoli, C. Open coronary endarterectomy, saphenous vein patch reconstruction, and internal mammary artery grafting. Ann. Thorac. Surg. 1992, 53, 1151–1152. [Google Scholar] [CrossRef]
- Beretta, L.; Lemma, M.; Vanelli, P.; DiMattia, D.; Bozzi, G.; Broso, P.; Salvaggio, A.; Santoli, C. Coronary “open” endarterectomy and reconstruction: Short- and long-term results of the revascularization with saphenous vein versus IMA-graft. Eur. J. Cardiothorac. Surg. 1992, 6, 382–387. [Google Scholar] [CrossRef]
- Erdil, N.; Cetin, L.; Kucuker, S.; Demirkilic, U.; Sener, E.; Tatar, H. Closed Endarterectomy for Diffuse Right Coronary Artery Disease: Early Results with Angiographic Controls. J. Card. Surg. 2010, 17, 261–266. [Google Scholar] [CrossRef]
- Shehada, S.E.; Mourad, F.; Haddad, A.; Darwish, B.; Ryadi, N.; Balaj, I.; Jakob, H.; Ruhparwar, A. Outcomes of Patients Undergoing Closed Traction CoronaryEndarterectomy: A Long-Term Single Center Study. J. Clin. Med. 2022, 11, 7026. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation 2016, 134, e123–e155. [Google Scholar] [PubMed] [Green Version]
- Valgimigli, M.; Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar]
- Sousa-Uva, M.; Head, S.J.; Milojevic, M.; Collet, J.-P.; Landoni, G.; Castella, M.; Dunning, J.; Gudbjartsson, T.; Linker, N.J.; Sandoval, E.; et al. 2017 EACTS Guidelines on perioperative medication in adult cardiac surgery. Eur. J. Cardiothorac. Surg. 2018, 53, 5–33. [Google Scholar] [CrossRef] [Green Version]
- Loffler, A.I.; Kramer, C.M. Myocardial Viability Testing to Guide Coronary Revascularization. Interv. Cardiol. Clin. 2018, 7, 355–365. [Google Scholar] [CrossRef]
- Previtali, M.; Lanzarini, L.; Poli, A.; Fetiveau, R.; Barberis, P. Dobutamine stress echocardiography early after myocardial infarction treated with thrombolysis. Identification of myocardial viability and ischemia and relation to spontaneous functional recovery. Int. J. Card. Imaging 1996, 12, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Jakob, H.; Mourad, F.; Lubarski, J.; Schlosser, T.; Shehada, S.-E. A Case of Diffuse Three-Vessel Coronary Artery Disease With Triple Coronary Endarterectomy in a Patient Undergoing Coronary Artery Bypass Grafting. CTSNet 2019. [Google Scholar] [CrossRef]
- Wendt, D.; Sharaf-Eldin Shehada, S.E.; Mourad, F.; Machulla, R.; Demircioglu, E.; Marx, P.; Demircioglu, A.; Tsagakis, K.; Thielmann, M.; Jakob, H.; et al. Transit time flow measurement and high frequency ultrasound epi-cardiac imaging to guide coronary artery bypass surgery. J. Cardiovasc. Surg. 2018, 60, 245–250. [Google Scholar]
- The Task Force on myocardial revascularization of the European Society of Cardiology. Guidelines on myocardial revascularization. Eur. J. Cardiothorac. Surg. 2010, 38 (Suppl. S1), S1–S52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, G.; Zhe, Z.; Pi, Y.; Lu, B.; Lu, J.; Hu, S. Aspirin plus clopidogrel therapy increases early venous graft patency after coronary artery bypass surgery a single-center, randomized, controlled trial. J. Am. Coll. Cardiol. 2010, 56, 1639–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tóth, O.; Calatzis, A.; Penz, S.; Losonczy, H.; Siess, W. Multiple electrode aggregometry: A new device to measure platelet aggregation in whole blood. Thromb. Haemost. 2006, 96, 781–788. [Google Scholar]
- Effler, D.B.; Groves, L.K.; Sones, F.M.; Shirey, E.K. Endarterectomy in the Treatment of Coronary Artery Disease. J. Thorac. Cardiovasc. Surg. 1964, 47, 98–108. [Google Scholar] [CrossRef]
- Kragel, A.H.; McIntosh, C.M.; Roberts, W.C. Morphologic changes in coronary artery seen late after endarterectomy. Am. J. Cardiol. 1989, 63, 757–759. [Google Scholar] [CrossRef] [PubMed]
- Walley, V.M.; Byard, R.W.; Keon, W.J. A study of the sequential morphologic changes after manual coronary endarterectomy. J. Thorac. Cardiovasc. Surg. 1991, 102, 890–894. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Kim, D.H.; Daskalakis, C.; Silvestry, S.C.; Sheth, M.P.; Lee, A.N.; Adams, S.; Hohmann, S.; Medvedev, S.; Whellan, D.J. Aspirin and clopidogrel use in the early postoperative period following on-pump and off-pump coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2009, 138, 1377–1384. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.; Goodman, S.G.; Mehta, S.R.; Latter, D.A.; Ruel, M.; Gupta, M.; Yanagawa, B.; Al-Omran, M.; Gupta, N.; Teoh, H.; et al. Should dual antiplatelet therapy be used in patients following coronary artery bypass surgery? A meta-analysis of randomized controlled trials. BMC Surg. 2015, 15, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, P.O.; Tabata, M.; Shekar, P.S.; Couper, G.S.; Khalpey, Z.I.; Aranki, S.F. Extensive endarterectomy and reconstruction of the left anterior descending artery: Early and late outcomes. J. Thorac. Cardiovasc. Surg. 2012, 143, 1336–1340. [Google Scholar] [CrossRef] [Green Version]
- Livesay, J.J.; Cooley, D.A.; Hallman, G.L.; Reul, G.J.; Ott, D.A.; Duncan, J.M.; Frazier, O.H. Early and late results of coronary endarterectomy. Analysis of 3369 patients. J. Thorac. Cardiovasc. Surg. 1986, 92, 649–660. [Google Scholar] [CrossRef]
- Goldman, S.; Zadina, K.; Moritz, T.; Ovitt, T.; Sethi, G.; Copeland, J.G.; Thottapurathu, L.; Krasnicka, B.; Ellis, N.; Anderson, R.J.; et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: Results from a Department of Veterans Affairs Cooperative Study. J. Am. Coll. Cardiol. 2004, 44, 2149–2156. [Google Scholar] [CrossRef]
- Benedetto, U.; Caputo, M.; Gaudino, M.; Mariscalco, G.; Bryan, A.; Angelini, G.D. Is the right internal thoracic artery superior to saphenous vein for grafting the right coronary artery? A propensity score-based analysis. J. Thorac. Cardiovasc. Surg. 2017, 154, 1269–1275.e5. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.J.; Han, J.J.; Desai, N.D.; Iyengar, A.; Acker, A.M.; Grau-Sepulveda, M.; Zwischenberger, B.A.; Jawitz, O.K.; Hargrove, W.C.; Szeto, W.Y.; et al. Coronary Endarterectomy: Analysis of The Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann. Thorac. Surg. 2022, 114, 667–674. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 353) | Single-APT (n = 153) | Dual-APT (n = 200) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 67 ± 9.3 | 65.7 ± 8.6 | 68.7 ± 9.5 | 0.017 |
| Gender, males | 311 (88.1) | 125 (81.7) | 186 (93) | 0.004 |
| Body mass index, kg/m2 | 27.4 ± 4.0 | 27.7 ± 4.3 | 27.1 ± 3.8 | 0.196 |
| Risk factors and comorbidities | ||||
| Diabetes mellitus | 133 (37.7) | 55 (35.9) | 78 (39) | 0.38 |
| Systemic hypertension | 310 (87.8) | 134 (87.6) | 175 (87.5) | 1.0 |
| Active smoker | 67 (19) | 26 (17) | 41 (20.5) | 0.306 |
| Hypercholesterinaemia | 225 (63.7) | 96 (62.7) | 129 (64.5) | 0.824 |
| COPD | 39 (11.0) | 20 (13.1) | 19 (9.5) | 0.307 |
| Peripheral vascular disease | 59 (16.7) | 29 (18.9) | 30 (15) | 0.388 |
| Central vascular disease | 62 (17.6) | 23 (15) | 39 (19.5) | 0.578 |
| Preoperative dialysis | 6 (1.7) | 2 (1.3) | 4 (2) | 0.702 |
| Previous cerebrovascular event | 27 (7.6) | 10 (6.5) | 17 (8.5) | 0.547 |
| Previous myocardial infarction | 140 (39.7) | 60 (39.2) | 80 (40) | 0.913 |
| Previous CABG | 20 (5.7) | 11 (7.2) | 9 (4.5) | 0.245 |
| Non-elective surgery | 104 (29.5) | 54 (35.3) | 50 (25) | 0.035 |
| CCS III-IV | 136 (38.5) | 65 (42.5) | 71 (35.5) | <0.0001 |
| NYHA III-IV | 109 (30.9) | 78 (51) | 31 (15.5) | <0.0001 |
| Extent of coronary artery disease | 0.126 | |||
| Three-vessel disease | 330 (93.5) | 142 (92.8) | 188 (94) | |
| Two-vessel disease | 20 (5.7) | 8 (5.2) | 12 (6) | |
| One-vessel disease | 3 (0.8) | 3 (2) | 0 | |
| SYNTAX-scores | ||||
| SYNTAX-SCORE I | 27.4 ± 9.3 | 28.2 ± 9.6 | 26.8 ± 9.0 | 0.174 |
| SYNTAX-SCORE II | 34.2 ± 19.4 | 34.4 ± 27.17 | 34.1 ± 11.6 | 0.91 |
| Left ventricular function | 0.81 | |||
| EF > 50% | 219 (62) | 98 (64.0) | 121 (60.5) | |
| EF = 30–50% | 111 (31.4) | 46 (30.1) | 65 (32.5) | |
| EF < 30% | 23 (6.5) | 9 (5.9) | 14 (7) | |
| Risk scores | ||||
| Logistic EuroSCORE I | 2.8 (1.5–4.5) | 3.7 (1.8–8.2) | 2.9 (1.5–4.6) | 0.863 |
| EuroSCORE II | 1.3 (1–2.1) | 1.6 (0.94–1.8) | 1.3 (0.88–2.3) | 0.722 |
| All Patients (n = 353) | Single-APT (n = 153) | Dual-APT (n = 200) | p-Value | |
|---|---|---|---|---|
| Aortic cross-clamp time, minutes | 85 ± 19.4 | 85.4 ± 18.4 | 84.9 ± 20.2 | 0.81 |
| CBP-time = bypass time, minutes | 121.6 ± 31.5 | 121.9 ± 30.3 | 121.4 ± 32.5 | 0.872 |
| Total number of grafts | 1534 | 641 | 893 | -- |
| Mean number of grafts/patient | 4.3 ± 1.0 | 4.2 ± 1.1 | 4.5 ± 1.0 | 0.17 |
| Total number of CEA-grafts | 435 | 171 | 264 | -- |
| Mean number of CEA-graft/patient | 1.23 ± 0.51 | 1.1 ± 0.4 | 1.3 ± 0.6 | 0.1 |
| Number of CEA-grafts in each patient | 0.001 | |||
| One-CEA | 285 (80.7) | 137 (89.5) | 148 (74) | |
| Two-CEAs | 56 (15.9) | 14 (9.2) | 42 (21) | |
| Three-CEAs | 10 (2.8) | 2 (1.3) | 8 (4) | |
| Four-CEAs | 2 (0.6) | 0 | 2 (1) | |
| Indication of CEA | 0.006 | |||
| Totally occluded vessels | 96 (27.2) | 53 (34.6) | 43 (21.5) | |
| Sub-totally occluded vessels | 249 (70.5) | 99 (64.7) | 150 (75) | |
| both | 8(2.3) | 1(0.7) | 7(3.5) | |
| Graft used after CEA | 0.23 | |||
| Arterial graft | 116 (32.9) | 49 (32) | 67 (33.5) | |
| Venous graft | 202 (57.2) | 96 (62.7) | 106 (53) | |
| Arterial and Venous graft | 35 (9.9) | 8 (5.2) | 27 (13.5) | |
| TTFM of CEA graft after CPB | ||||
| TTFM | 64 (43–94) | 57 (35–80) | 65 (45–90) | 0.028 |
| Pulsatility index | 2.1 (1.6–2.9) | 2 (2–3.5) | 2.1 (1.5–2.8) | 0.849 |
| CEA was done at | n = 435 | n = 171 | n = 264 | |
| LAD-Territory | 191 (43.9) | 72 (42.1) | 119 (45.1) | 0.133 |
| RCA-Territory | 175 (40.2) | 61 (35.7) | 114 (43.2) | 0.013 |
| LCX-Territory | 69 (15.9) | 38 (22.2) | 31 (11.7) | 0.029 |
| All Patients (n = 353) | Single-APT (n = 153) | Dual-APT (n = 200) | p-Value | |
|---|---|---|---|---|
| Low cardiac output syndrome | 25 (7.1) | 15 (9.8) | 10 (5) | 0.16 |
| Need for IABP | 18 (5.1) | 10 (6.5) | 8 (4) | |
| Need for ECMO | 7 (2) | 5 (3.3) | 2 (1) | |
| Myocardial infarction | 9 (2.5) | 6 (3.9) | 3 (1.5) | 0.183 |
| Stroke | 8 (2.3) | 5 (3.3) | 3 (1.5) | 0.3 |
| Revision for bleeding | 20 (5.7) | 10 (6.5) | 10 (5) | 0.64 |
| Packed red cell transfusion | 660 (600–800) | 750 (75–502.5) | 600 (0–1200) | 0.827 |
| Temporary dialysis | 33 (9.3) | 16 (10.5) | 17 (8.5) | 0.58 |
| Respiratory complications | 42 (11.9) | 17(11.1) | 25 (12.5) | 0.94 |
| Need for re-intubation | 18 (5.1) | 7 (4.6) | 11 (5.5) | |
| Need for tracheostomy | 24 (6.8) | 10 (6.5) | 14 (7) | |
| Deep wound infection | 13 (3.7) | 3 (2) | 10 (5) | 0.162 |
| ICU-stay, days | 1.6 (1–3.5) | 1.5 (1–3) | 2 (1–3) | 0.806 |
| Hospital stay, days | 12.1 ± 10.1 | 11.8 ± 10.7 | 12.4 ± 9.6 | 0.59 |
| Operative mortality | ||||
| 30-day mortality | 17 (4.8) | 8 (5.2) | 9 (4.5) | 0.8 |
| Cardiac-related mortality | 11 (3.1) | 6 (3.9) | 5 (2.5) | |
| Operative MACCE | 33 (9.3) | 18 (11.8) | 15 (7.5) | 0.19 |
| All Patients (n = 353) | Single-APT (n = 153) | Dual-APT (n = 200) | p-Value | |
|---|---|---|---|---|
| Lost during follow-up | 5 (1.4) | 3 (2) | 2 (1) | |
| Mortality at one year | 31 (8.8) | 16 (10.6) | 15 (7.5) | 0.347 |
| Mortality at five years | 94 (26.6) | 58 (37.9) | 36 (18) | <0.0001 |
| Overall mortality at last follow-up | 116 (32.9) | 78 (51) | 38 (19) | <0.0001 |
| Survivors at last follow-up | 232 (65.7) | 72 (47) | 160 (80) | <0.0001 |
| Patients did not fill out the questionnaire | 36 (10.2) | 19 (12.4) | 17 (9) | |
| Overall MACCE at last follow-up | 138 (39.1) | 89 (58.2) | 49 (24.5) | <0.0001 |
| Questionnaire Validation | Total Number (n = 196) | Single-APT (n = 53) | Dual-APT (n = 143) | p-Value |
|---|---|---|---|---|
| Clinical follow-up | ||||
| Completely independent | 175 (89.3) | 42 (79.2) | 133 (93) | 0.012 |
| Depends on help for daily routine | 21 (10.7) | 11 (20.8) | 10 (7) | 0.012 |
| NYHA-class I-II | 178 (90.8) | 43 (81.1) | 135 (94.4) | 0.018 |
| NYHA-class III-IV | 18 (9.2) | 10 (18.9) | 8 (5.6) | 0.018 |
| Stroke | 11 (5.6) | 5 (9.4) | 6 (4.2) | 0.172 |
| Angina pectoris | 17 (8.7) | 9 (17) | 8 (5.6) | 0.02 |
| Myocardial infarction | 10 (5.1) | 7 (13.2) | 3 (2.1) | 0.004 |
| PCI/Stenting | 15 (7.7) | 9 (17) | 6 (4.2) | 0.011 |
| Re-CABG | 0 | |||
| Other cardiac surgery | 5 (2.6) | 4 (7.5) | 1 (0.7) | 0.027 |
| Pacemaker implantation | 13 (6.6) | 6 (11.3) | 7 (4.9) | 0.037 |
| Imaging follow-up | ||||
| Imaging | 95 (48.5) | 39 (73.6) | 56 (39) | <0.0001 |
| Coronary catheter | 53 | 29 | 24 | |
| Computed tomography | 42 | 10 | 32 | |
| Indication for Imaging | 95 (48.5) | 39 (73.6) | 56 (39) | <0.0001 |
| Symptoms | 56 | 24 | 32 | |
| Research | 39 | 15 | 24 | |
| Graft patency | ||||
| CEA-graft patency | 107/124 (86.3) | 44/54 (81.5) | 63/70 (90) | 0.017 |
| Total graft patency | 378/423 (89.4) | 136/168 (81) | 242/255 (95) | 0.017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balaj, I.; Jakob, H.; Haddad, A.; Mourad, F.; Haneya, A.; Ali, E.; Ryadi, N.; Thielmann, M.; Ruhparwar, A.; Shehada, S.-E. Role of Antiplatelet Therapy in Patients with Severe Coronary Artery Disease Undergoing Coronary Artery Endarterectomy within Coronary Artery Bypass Surgery. J. Cardiovasc. Dev. Dis. 2023, 10, 112. https://doi.org/10.3390/jcdd10030112
Balaj I, Jakob H, Haddad A, Mourad F, Haneya A, Ali E, Ryadi N, Thielmann M, Ruhparwar A, Shehada S-E. Role of Antiplatelet Therapy in Patients with Severe Coronary Artery Disease Undergoing Coronary Artery Endarterectomy within Coronary Artery Bypass Surgery. Journal of Cardiovascular Development and Disease. 2023; 10(3):112. https://doi.org/10.3390/jcdd10030112
Chicago/Turabian StyleBalaj, Ilir, Heinz Jakob, Ali Haddad, Fanar Mourad, Assad Haneya, Ebrahim Ali, Noura Ryadi, Matthias Thielmann, Arjang Ruhparwar, and Sharaf-Eldin Shehada. 2023. "Role of Antiplatelet Therapy in Patients with Severe Coronary Artery Disease Undergoing Coronary Artery Endarterectomy within Coronary Artery Bypass Surgery" Journal of Cardiovascular Development and Disease 10, no. 3: 112. https://doi.org/10.3390/jcdd10030112