
Early Mortality in Infants Born with Neonatally Operated Congenital Heart Defects and Low or Very-Low Birthweight: A Systematic Review and Meta-Analysis
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Literature Search Strategy and Study Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis and Statistical Analysis
3. Results
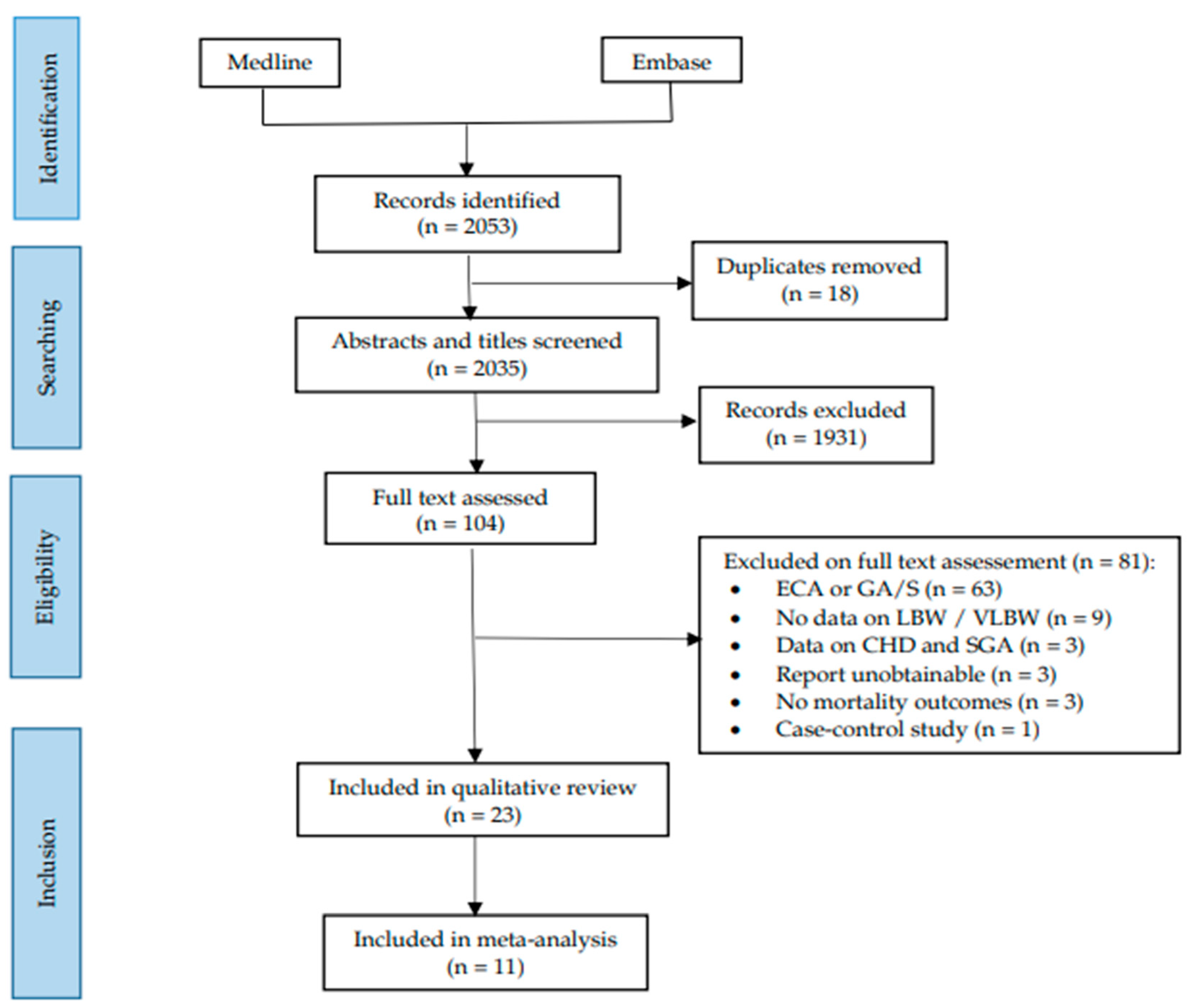
3.1. Literature Searches
3.2. Characteristics of Included Studies

{kind=link}
{kind=link}
{kind=link}
| Study | Year | Duration | Location | N CHD | All iCHD | Other Specific CHD | Population | Outcome(s) |
|---|---|---|---|---|---|---|---|---|
| Anderson [27] § + | 2014 | 1997–2012 | USA | 299 | No | HLHS, AS, Ebs, TAPVR and CoA | VLBW | Discharge mortality |
| Archer [21] § + | 2011 | 2006–2007 | USA | 893 | No | HLHS, AS, TAPVR, TGA and CoA | VLBW | Mortality at discharge or 1 year |
| Bacha [28] + | 2001 | 1990–1999 | USA | 189 | No | CoA | VLBW | Hospital and 5-year survival |
| Bain [29] § + | 2014 | 1997–2010 | USA | 98,523 | No | SD | VLBW | NEC |
| Best [26] § | 2017 | 1985–2003 | UK | 5093 | Yes | AS, TGA and CoA | LBW | Overall survival and 5-year survival for cohort born in 2003 |
| Curzon [3] § | 2008 | 2002–2004 | USA | 3022 | No | HLHS, TAPVR, TGA and CoA | LBW | 90-day post-op |
| El Hassan [30] § | 2018 | 2004–2013 | USA | 5720 | No | HLHS | SGA and LBW | Hospitalization mortality and NEC |
| Fisher [31] § + | 2015 | 2006–2011 | USA | 1931 | No | HLHS, AS, TAPVR, TGA and CoA | VLBW | NEC |
| Gelehrter [32] + | 2011 | 1998–2007 | USA | 47 | No | HLHS | SGA and LBW | Transplant-free survival through Fontan palliation |
| Hirsch [33] § | 2011 | 1992–2005 | USA | 406 | No | HLHS | LBW | Survival and mortality at 1 year after surgical intervention |
| Kalfa [34] | 2014 | 2006–2012 | USA | 146 | No | HLHS, Ebs, TAPVR, TGA and CoA | LBW | Mortality before discharge or within 30-days post-op and immediate post-operative outcomes (ECMO, NEC, length of mechanical ventilation, delayed chest closure, prolonged inotropic support, renal failure, and cardiac arrest) |
| Kalfa [9] | 2015 | 2006–2014 | USA | 28 | No | HLHS | LBW | Death before discharge or 30-days post-op, delayed chest closure, cardiac arrest, length of mechanical ventilation, arrhythmia, pulmonary complications, renal failure, and NEC |
| Karamlou [35] | 2009 | 1993–2004 | USA | 36 | No | CoA | LBW | 1-year survival |
| Manchego [36] | 2018 | 2003–2016 | Australia | 171 | No | HLHS, TGA and CoA | LBW | Survival and post-operative complications (unplanned re-intervention, ECMO, sepsis, stroke, NEC, etc., for all CHDs only) at 6 months, |
| Miller [37] § | 2019 | 2005–2008 | USA | 509 | No | HLHS | SGA and LBW | 6-year mortality, neurodevelopment, hospital length of stay, unplanned re-intervention and quality of life |
| Murphy [38] | 2015 | 2005–2013 | UK | 41 | No | HLHS | LBW | Midterm survival after initial hybrid procedure |
| Oh [39] § | 2017 | 1992–2014 | New Zealand | 133 | No | HLHS | LBW | Mortality before discharge or within 30-days post-op |
| Oppido [40] | 2004 | 1993–2002 | Italy | 60 | No | HLHS, TGA and CoA | LBW | Inpatient mortality (within 30 days after operation) |
| Oster [22] § | 2013 | 1979–2005 | USA | 415 | No | CCHD | LBW | 1-year survival |
| Pappas [25] § + | 2012 | 1998–2005 | USA | 110 | Yes | HLHS, TAPVR, TGA and CoA | VLBW | Discharge mortality and in hospital morbidity (seizures, NEC, ICH, PVL, BPD, neurological impairment, premature retinopathy, Apgar score, late-onset sepsis) |
| Roussin [24] + | 2007 | 1990–2003 | France | 25 | No | TGA | LBW, SGA and VLBW | Discharge mortality and early morbidity (prolonged inotropic support, cardiac ischemia, pulmonary hypertension, prolonged ventilation, neurologic disease) |
| Shepard [41] § | 2010 | 1982–2006 | USA | 450 | No | HLHS, TAPVR and CoA | MLBW and VLBW | 30-day survival |
| Siffle [23] § | 2015 | 1979–2005 | USA | 212 | No | HLHS | LBW and VLBW | Overall survival between 1979–2005 |
3.3. Risk of Bias
| Study | CASP Criteria | Total Score/9 ǂ | Overall Risk of Bias ** | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Focused Issue | Selection Bias § | Measurement Bias | Confounding | Follow-Up | Results § | External Validity | |||
| Anderson * [27] | + | + | - | - | + | - | + | 4 | High |
| Archer * [21] | + | + | - | - | + | ++ | + | 6 | Low |
| Bacha * [28] | + | - | - | + | + | - | - | 3 | High |
| Bain [29] | + | + | - | + | + | + | + | 6 | Low |
| Best [26] | + | + | + | + | + | + | + | 7 | Low |
| Curzon [3] | + | - | - | - | + | + | + | 4 | High |
| ElHassan * [30] | + | - | - | - | + | + | + | 4 | High |
| Fisher [31] | + | + | - | + | + | ++ | + | 7 | Low |
| Gelehrter [32] | + | - | - | + | + | + | - | 4 | High |
| Hirsch [33] | + | - | - | + | + | ++ | + | 6 | Low |
| Kalfa (2015) * [9] | + | + | - | - | + | - | - | 3 | High |
| Kalfa (2014) * [34] | + | + | + | + | + | + | - | 6 | Low |
| Karamlou [35] | + | ++ | - | - | + | - | - | 4 | High |
| Manchego [36] | + | + | + | - | + | - | - | 4 | High |
| Miller [37] | + | - | - | + | + | ++ | + | 6 | Low |
| Murphy [38] | + | ++ | + | - | + | - | - | 5 | High |
| Oh * [39] | + | - | + | + | + | + | + | 6 | Low |
| Oppido * [40] | + | - | + | - | + | - | - | 3 | High |
| Oster [22] | + | - | - | + | + | ++ | + | 6 | Low |
| Pappas * [25] | + | - | + | + | + | - | + | 5 | High |
| Roussin * [24] | + | - | + | - | + | - | - | 3 | High |
| Shepard * [41] | + | ++ | + | - | + | - | + | 6 | Low |
| Siffle [23] | + | - | - | + | + | ++ | + | 6 | Low |
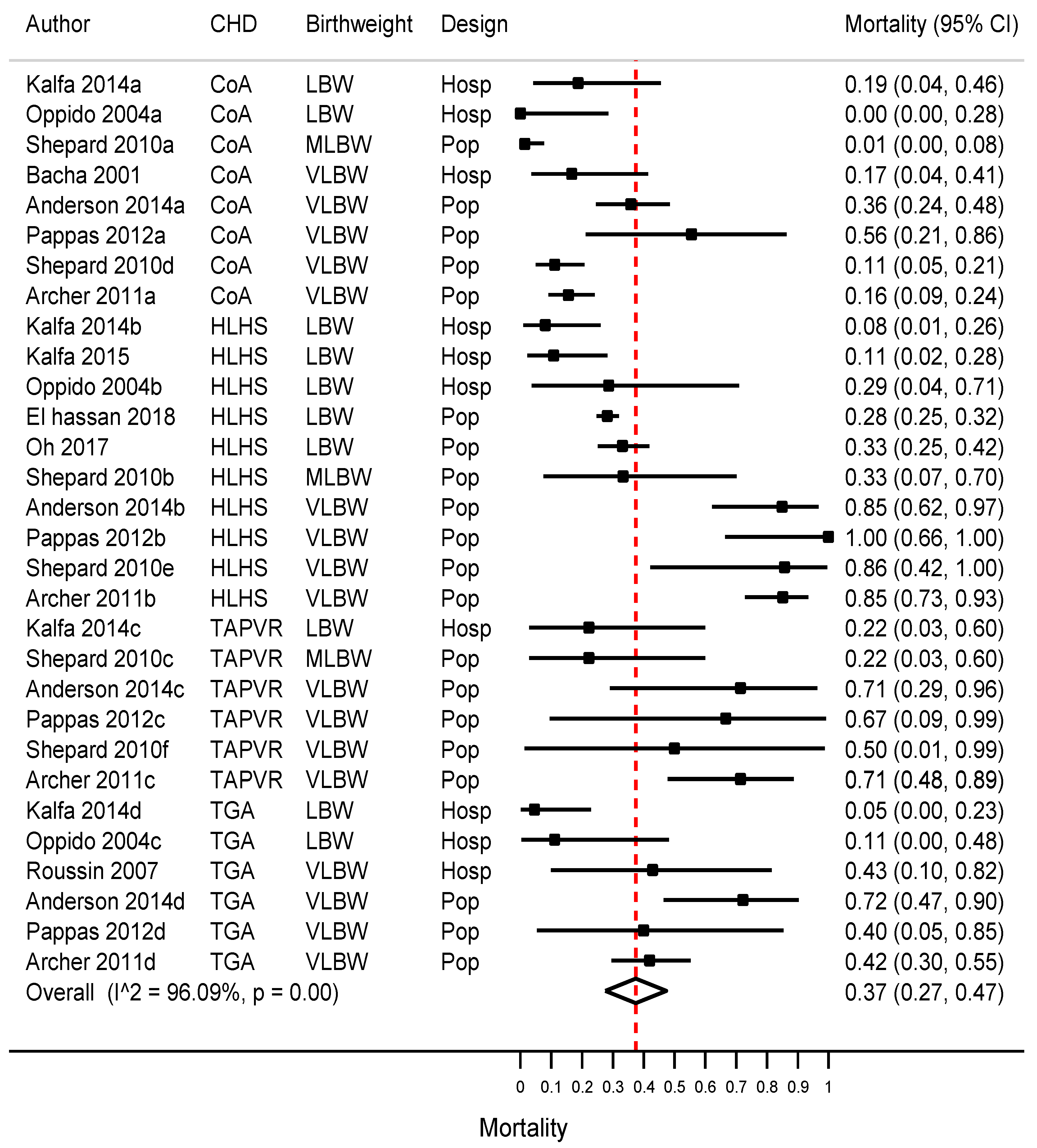
3.4. Early Mortality in Infants Born with OCHD
3.5. Morbidity in Infants Born with an LBW or VLBW with a CHD
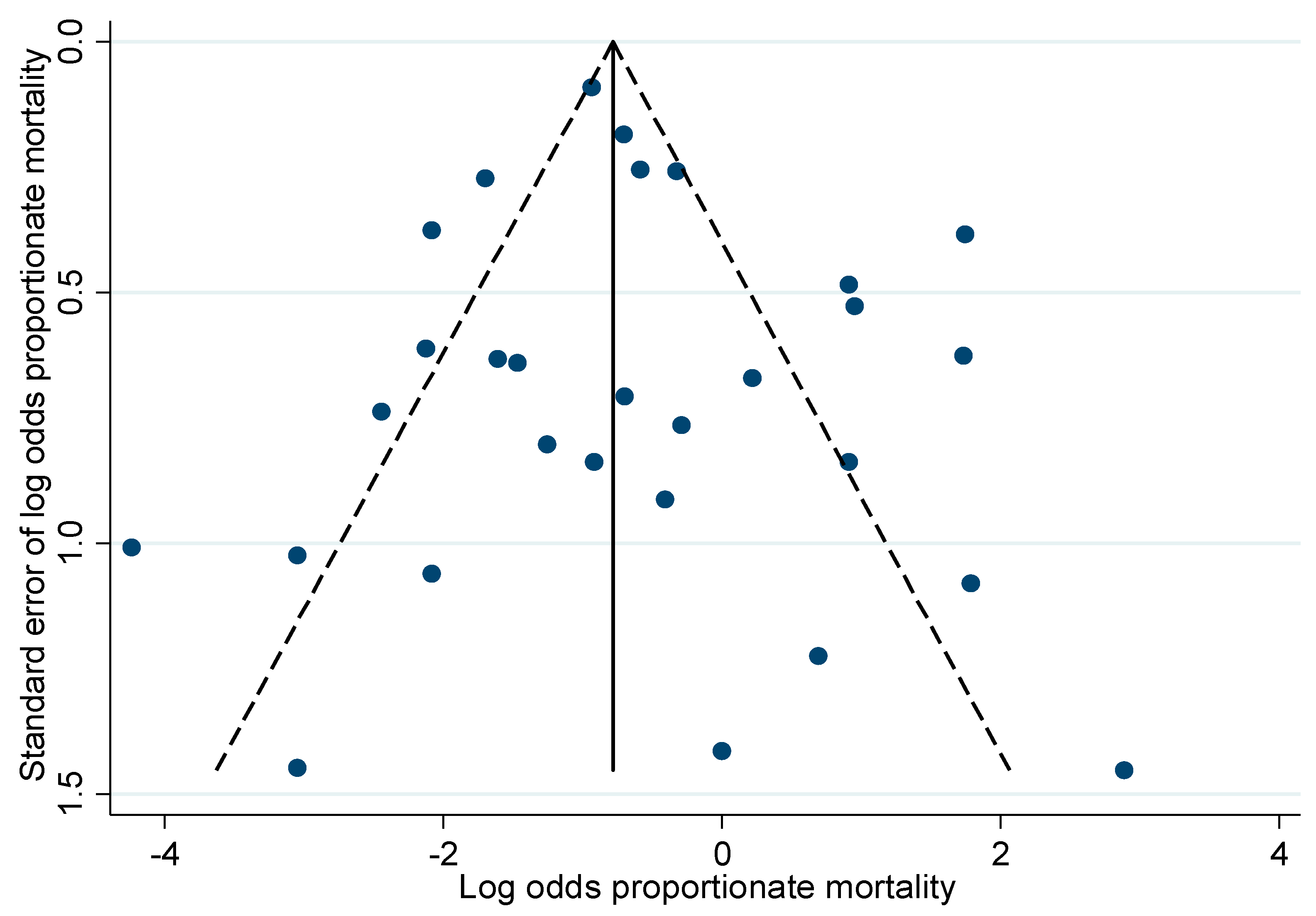
3.6. Additional Analyses
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AS | Aortic stenosis |
| BPD | Bronchopulmonary Dysplasia |
| CASP | Critical Appraisal Skills Program |
| CHD | Congenital heart defects |
| CoA | Coarctation of the aorta |
| CI | Confidence interval |
| HLHS | Hypoplastic left heart syndrome |
| IVH | Intraventricular hemorrhage |
| LBW | Low birth weight |
| MLBW | Moderately low birth weight |
| NEC | Necrotizing enterocolitis |
| OCHD | Neonatally operated congenital heart defects |
| SGA | Small for gestational age |
| TGA | Transposition of the great arteries |
| TAPVR | Total anomalous pulmonary venous return |
| VLBW | Very-low birth weight |
References
- Liu, Y.; Chen, S.; Zühlke, L.; Black, G.C.; Choy, M.K.; Li, N.; Keavney, B.D. Global birth prevalence of congenital heart defects 1970–2017: Updated systematic review and meta-analysis of 260 studies. Int. J. Epidemiol. 2019, 48, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Kramer, H.H.; Trampisch, H.J.; Rammos, S.; Giese, A. Birth weight of children with congenital heart disease. Eur. J. Pediatr. 1990, 149, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Curzon, C.L.; Milford-Beland, S.; Li, J.S.; O’Brien, S.M.; Jacobs, J.P.; Jacobs, M.L.; Welke, K.F.; Lodge, A.J.; Peterson, E.D.; Jaggers, J. Cardiac surgery in infants with low birth weight is associated with increased mortality: Analysis of the Society of Thoracic Surgeons Congenital Heart Database. J. Thorac. Cardiovasc. Surg. 2008, 135, 546–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindinger, A.; Schwedler, G.; Hense, H.W. Prevalence of congenital heart defects in newborns in Germany: Results of the first registration year of the PAN Study (July 2006 to June 2007). Klin. Padiatr. 2010, 222, 321–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). Data and Statistics on Congenital Heart Defects|CDC [Website]; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/ncbddd/heartdefects/data.html (accessed on 11 December 2022).
- Levin, D.L.; Stanger, P.; Kitterman, J.A.; Heymann, M. Congenital heart disease in low birth weight infants. Circulation 1975, 52, 500–503. [Google Scholar] [CrossRef] [Green Version]
- Godfrey, M.; Schimmel, M.; Hammerman, C.; Farber, B.; Glaser, J.; Nir, A. The incidence of congenital heart defects in very low birth weight and extremely low birth weight infants. Sat 2010, 27, 21. [Google Scholar]
- Ghanchi, A.; Derridj, N.; Bonnet, D.; Bertille, N.; Salomon, L.J.; Khoshnood, B. Children born with congenital heart defects and growth restriction at birth: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 3056. [Google Scholar] [CrossRef]
- Kalfa, D.; Krishnamurthy, G.; Levasseur, S.; Najjar, M.; Chai, P.; Chen, J.; Quaegebeur, J.; Bacha, E. Norwood Stage I Palliation in Patients Less Than or Equal to 2.5 kg: Outcomes and Risk Analysis. Ann. Thorac. Surg. 2015, 100, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Ghanchi, A.; Derridj, N.; Bertille, N.; Salomon, L.J.; Khoshnood, B. Adverse Outcomes in Infants Born with Isolated Congenital Heart Defects and Growth Restriction in the Newborn (GRN): A Systematic Review and Meta-Analysis. PROSPERO 2020 CRD42020170289 [Website]. 2020. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=170289 (accessed on 11 December 2022).
- Nees, S.N.; Chung, W.K. The Genetics of Isolated Congenital Heart Disease; Wiley Online Library: Hoboken, NJ, USA, 2020; pp. 97–106. [Google Scholar]
- Miller, A.; Riehle-Colarusso, T.; Alverson, C.J.; Frías, J.L.; Correa, A. Congenital heart defects and major structural noncardiac anomalies, Atlanta, Georgia, 1968 to 2005. J. Pediatr. 2011, 159, 70–78.e2. [Google Scholar] [CrossRef]
- Cutland, C.; Lackritz, E.; Mallett-Moore, T.; Bardají, A.; Chandrasekaran, R.; Lahariya, C.; Nisar, M.I.; Tapia, M.D.; Pathirana, J.; Kochhar, S.; et al. Brighton Collaboration Low Birth Weight Working Group Low birth weight: Case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine 2017, 35, 6492–6500. [Google Scholar] [PubMed]
- Hernandez, J.B.; Kim, P. Epidemiology Morbidity and Mortality; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Osswald, B.R.; Blackstone, E.H.; Tochtermann, U.; Thomas, G.; Vahl, C.F.; Hagl, S. The meaning of early mortality after CABG. Eur. J. Cardiothorac. Surg. 1999, 15, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Critical Skills Appraisal Programme. CASP Cohort Study Checklist [Website]. 2018. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 11 December 2022).
- Barendregt, J.J.; Doi, S.A.; Lee, Y.Y.; Norman, R.E.; Vos, T. Meta-analysis of prevalence. J. Epidemiol. Community Health 2013, 67, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [Green Version]
- Archer, J.M.; Yeager, S.B.; Kenny, M.J.; Soll, R.F.; Horbar, J.D. Distribution of and mortality from serious congenital heart disease in very low birth weight infants. Pediatrics 2011, 127, 293–299. [Google Scholar] [CrossRef]
- Oster, M.E.; Lee, K.A.; Honein, M.A.; Riehle-Colarusso, T.; Shin, M.; Correa, A. Temporal trends in survival among infants with critical congenital heart defects. Pediatrics 2013, 131, e1502–e1508. [Google Scholar] [CrossRef] [Green Version]
- Siffel, C.; Riehle-Colarusso, T.; Oster, M.E.; Correa, A. Survival of children with hypoplastic left heart syndrome. Pediatrics 2015, 136, e864–e870. [Google Scholar] [CrossRef] [Green Version]
- Roussin, R.; Belli, E.; Bruniaux, J.; Demontoux, S.; Touchot, A.; Planché, C.; Serraf, A. Surgery for transposition of the great arteries in neonates weighing less than 2000 grams: A consecutive series of 25 patients. Ann. Thorac. Surg. 2007, 83, 173–178. [Google Scholar] [CrossRef]
- Pappas, A.; Shankaran, S.; Hansen, N.I.; Bell, E.F.; Stoll, B.J.; Laptook, A.R.; Walsh, M.C.; Das, A.; Bara, R.; Hale, E.C.; et al. Outcome of extremely preterm infants (<1000 g) with congenital heart defects from the National Institute of Child Health and Human Development Neonatal Research Network. Pediatr. Cardiol. 2012, 33, 1415–1426. [Google Scholar]
- Best, K.E.; Tennant, P.W.; Rankin, J. Survival, by birth weight and gestational age, in individuals with congenital heart disease: A population-based study. J. Am. Heart. Assoc. 2017, 6, e005213. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.W.; Smith, P.B.; Corey, K.M.; Hill, K.D.; Zimmerman, K.O.; Clark, R.H.; Hornik, C.P. Clinical outcomes in very low birth weight infants with major congenital heart defects. Early Hum. Dev. 2014, 90, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Bacha, E.A.; Scheule, A.M.; Zurakowski, D.; Erickson, L.C.; Hung, J.; Lang, P.; Mayer, J.E., Jr.; Pedro, J.; Jonas, R.A. Long-term results after early primary repair of tetralogy of Fallot. J. Thorac. Cardiovasc. Surg. 2001, 122, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Bain, J.; Benjamin, D.; Hornik, C.P.; Clark, R.; Smith, P. Risk of necrotizing enterocolitis in very-low-birth-weight infants with isolated atrial and ventricular septal defects. J. Perinatol. 2014, 34, 319–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ElHassan, N.O.; Tang, X.; Gossett, J.; Zakaria, D.; Ross, A.; Kona, S.K.; Prodhan, P. Necrotizing enterocolitis in infants with hypoplastic left heart syndrome following stage 1 palliation or heart transplant. Pediatr. Cardiol. 2018, 39, 774–785. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.G.; Bairdain, S.; Sparks, E.A.; Khan, F.A.; Archer, J.M.; Kenny, M.; Edwards, E.M.; Soll, R.F.; Modi, B.P.; Yeager, S.; et al. Serious congenital heart disease and necrotizing enterocolitis in very low birth weight neonates. J. Am. Coll. Surg. 2015, 220, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Gelehrter, S.; Fifer, C.G.; Armstrong, A.; Hirsch, J.; Gajarski, R. Outcomes of hypoplastic left heart syndrome in low-birth-weight patients. Pediatr. Cardiol. 2011, 32, 1175–1181. [Google Scholar] [CrossRef]
- Hirsch, J.C.; Copeland, G.; Donohue, J.E.; Kirby, R.S.; Grigorescu, V.; Gurney, J.G. Population-based analysis of survival for hypoplastic left heart syndrome. J. Pediatr. 2011, 159, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Kalfa, D.; Krishnamurthy, G.; Duchon, J.; Najjar, M.; Levasseur, S.; Chai, P.; Chen, J.; Quaegebeur, J.; Bacha, E. Outcomes of cardiac surgery in patients weighing <2.5 kg: Affect of patient-dependent and-independent variables. J. Thorac. Cardiovasc. Surg. 2014, 148, 2499–2506. [Google Scholar]
- Karamlou, T.; Bernasconi, A.; Jaeggi, E.; Alhabshan, F.; Williams, W.G.; Van Arsdell, G.S.; Coles, J.G.; Caldarone, C.A. Factors associated with arch reintervention and growth of the aortic arch after coarctation repair in neonates weighing less than 2.5 kg. J. Thorac. Cardiovasc. Surg. 2009, 137, 1163–1167. [Google Scholar] [CrossRef] [Green Version]
- Manchego, P.A.; Cheung, M.; Zannino, D.; Nunn, R.; D’Udekem, Y.; Brizard, C. Audit of Cardiac Surgery Outcomes for Low Birth Weight and Premature Infants; Elsevier: Amsterdam, The Netherlands, 2018; pp. 71–78. [Google Scholar]
- Miller, T.A.; Ghanayem, N.S.; Newburger, J.W.; McCrindle, B.W.; Hu, C.; DeWitt, A.G.; Cnota, J.F.; Tractenberg, F.L.; Pemberton, V.L.; Wolf, M.J. Gestational age, birth weight, and outcomes six years after the Norwood procedure. Pediatrics 2019, 143, e20182577. [Google Scholar]
- Murphy, M.O.; Bellsham-Revell, H.; Morgan, G.J.; Krasemann, T.; Rosenthal, E.; Qureshi, S.A.; Salih, C.; Austin, C.B.; Anderson, D.R. Hybrid procedure for neonates with hypoplastic left heart syndrome at high-risk for Norwood: Midterm outcomes. Ann. Thorac. Surg. 2015, 100, 2286–2292. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.H.; Artrip, J.H.; Graddon, C.; Minogue, C.; Marcondes, L.; Finucane, K.; Gentles, T. The New Zealand Norwood procedure experience: 22-year cumulative review. Heart Lung Circ. 2017, 26, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Oppido, G.; Napoleone, C.P.; Formigari, R.; Gabbieri, D.; Pacini, D.; Frascaroli, G.; Gargiulo, G. Outcome of cardiac surgery in low birth weight and premature infants. Eur. J. Cardiothorac. Surg. 2004, 26, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Shepard, C.W.; Kochilas, L.K.; Rosengart, R.M.; Brearley, A.M.; Bryant, R., III; Moller, J.H.; Louis, J.D.S. Repair of major congenital cardiac defects in low-birth-weight infants: Is delay warranted? J. Thorac. Cardiovasc. Surg. 2010, 140, 1104–1109. [Google Scholar] [CrossRef] [Green Version]
- Raissadati, A.; Nieminen, H.; Jokinen, E.; Sairanen, H. Progress in late results among pediatric cardiac surgery patients: A population-based 6-decade study with 98% follow-up. Circulation 2015, 131, 347–353, discussion 353. [Google Scholar] [CrossRef] [Green Version]
- Lacour-Gayet, F.; Clarke, D.; Jacobs, J.; Comas, J.; Daebritz, S.; Daenen, W.; Gaynor, W.; Hamilton, L.; Jacobs, M.; Maruszsewski, B.; et al. The Aristotle score: A complexity-adjusted method to evaluate surgical results. Eur. J. Cardio. Thorac. Surg. Off. J. Eur. Assoc. Cardio. Thorac. Surg. 2004, 25, 911–924. [Google Scholar] [CrossRef] [Green Version]
- Laussen, P.C. Neonates with congenital heart disease. Curr. Opin. Pediatr. 2001, 13, 220–226. [Google Scholar] [CrossRef]
- Woodson, K.E.; Sable, C.A.; Berger, J.T.; Slack, M.C.; Wernovsky, G.; Spray, T.L. A Case of Congenitally Protected d-Transposition of the Great Arteries in a Very Low-Birth-Weight Infant. Pediatr. Cardiol. 2003, 24, 175–178. [Google Scholar] [CrossRef]
- Bhombal, S.; Chock, V.Y.; Shashidharan, S. The impact of prematurity and associated comorbidities on clinical outcomes in neonates with congenital heart disease. Semin. Perinatol. 2022, 46, 151586. [Google Scholar] [CrossRef]
- Harrison, A.M.; Davis, S.; Reid, J.R.; Morrison, S.C.; Arrigain, S.; Connor, J.T.; Temple, M.E. Neonates with hypoplastic left heart syndrome have ultrasound evidence of abnormal superior mesenteric artery perfusion before and after modified Norwood procedure. Pediatr. Crit. Care Med. J. Soc. Crit. Care Med. World Fed. Pediatr. Intensive. Crit. Care Soc. 2005, 6, 445–447. [Google Scholar] [CrossRef] [PubMed]
- McElhinney, D.B.; Hedrick, H.L.; Bush, D.M.; Pereira, G.R.; Stafford, P.W.; Gaynor, J.W.; Spray, T.L.; Wernovsky, G. Necrotizing enterocolitis in neonates with congenital heart disease: Risk factors and outcomes. Pediatrics 2000, 106, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Motta, C.; Scott, W.; Mahony, L.; Koch, J.; Wyckoff, M.; Reisch, J.; Burchfield, P.J.; Brion, L.P. The association of congenital heart disease with necrotizing enterocolitis in preterm infants: A birth cohort study. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2015, 35, 949–953. [Google Scholar] [CrossRef] [Green Version]
- Natarajan, G.; Anne, S.R.; Aggarwal, S. Outcomes of congenital heart disease in late preterm infants: Double jeopardy? Acta Paediatr. Int. J. Paediatr. 2011, 100, 1104–1107. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.J.; Zappitelli, M.; Robertson, C.M.T.; Alton, G.Y.; Sauve, R.S.; Joffe, A.R.; Ross, D.B.; Rebeyka, I.M.; Western Canadian Complex Pediatric Therapies Follow-Up Group. Risk Factors for and Outcomes of Acute Kidney Injury in Neonates Undergoing Complex Cardiac Surgery. J. Pediatr. 2013, 162, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Krawczeski, C.D.; Zappitelli, M.; Devarajan, P.; Thiessen-Philbrook, H.; Coca, S.G.; Kim, R.W.; Parikh, C.R. Incidence, risk factors, and outcomes of acute kidney injury after pediatric cardiac surgery—A prospective multicenter study. Crit. Care Med. 2011, 39, 1493–1499. [Google Scholar] [CrossRef] [Green Version]
- Beken, S.; Akbulut, B.B.; Albayrak, E.; Güner, B.; Ünlü, Y.; Temur, B.; Aydin, S.; Ödemiş, E.; Erek, E.; Korkmaz, A. Evaluation of neonatal acute kidney injury after critical congenital heart disease surgery. Pediatr. Nephrol. 2021, 36, 1923–1929. [Google Scholar] [CrossRef]
- Stojanović, V.; Barišić, N.; Milanović, B.; Doronjski, A. Acute kidney injury in preterm infants admitted to a neonatal intensive care unit. Pediatr. Nephrol. 2014, 29, 2213–2220. [Google Scholar] [CrossRef]
- McMahon, C.J.; Penny, D.J.; Nelson, D.P.; Ades, A.M.; Al Maskary, S.; Speer, M.; Katkin, J.; McKenzie, E.D.; Fraser, C.D., Jr.; Chang, A.C. Preterm infants with congenital heart disease and bronchopulmonary dysplasia: Postoperative course and outcome after cardiac surgery. Pediatrics 2005, 116, 423–430. [Google Scholar] [CrossRef]
- Khoshnood, B.; De Vigan, C.; Vodovar, V.; Goujard, J.; Lhomme, A.; Bonnet, D.; Goffinet, F. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983–2000: A population-based evaluation. Pediatrics 2005, 115, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Khoshnood, B.; Lelong, N.; Houyel, L.; Bonnet, D.; Ballon, M.; Jouannic, J.M.; Goffinet, F. Impact of prenatal diagnosis on survival of newborns with four congenital heart defects: A prospective, population-based cohort study in France (the EPICARD Study). BMJ Open 2017, 7, e018285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckersley, L.; Sadler, L.; Parry, E.; Finucane, K.; Gentles, T.L. Timing of diagnosis affects mortality in critical congenital heart disease. Arch. Dis. Child 2016, 101, 516–520. [Google Scholar] [CrossRef]
- Chakraborty, A.; Gorla, S.R.; Swaminathan, S. Impact of prenatal diagnosis of complex congenital heart disease on neonatal and infant morbidity and mortality. Prenat. Diagn. 2018, 38, 958–963. [Google Scholar] [CrossRef]
- Cloete, E.; Bloomfield, F.H.; Sadler, L.; de Laat, M.W.M.; Finucane, A.K.; Gentles, T.L. Antenatal Detection of Treatable Critical Congenital Heart Disease Is Associated with Lower Morbidity and Mortality. J. Pediatr. 2019, 204, 66–70. [Google Scholar] [CrossRef]
- Levey, A.; Glickstein, J.S.; Kleinman, C.S.; Levasseur, S.M.; Chen, J.; Gersony, W.M.; Williams, I.A. The impact of prenatal diagnosis of complex congenital heart disease on neonatal outcomes. Pediatr. Cardiol. 2010, 31, 587–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Velzen, C.; Clur, S.; Rijlaarsdam, M.; Bax, C.; Pajkrt, E.; Heymans, M.; Bekker, M.N.; Hruda, J.; De Groot, C.J.M.; Blom, N.A.; et al. Prenatal detection of congenital heart disease—Results of a national screening programme. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 400–407. [Google Scholar] [CrossRef] [PubMed]



| Stratified Analysis | No. of Study Cohorts | Summary Mortality, % (95%CI) | I2, % | Meta-Regression | |
|---|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | ||||
| Specific CHD | 0.13 | ||||
| Coarctation of the aorta | 8 | 16 (6–25) | 88 | Reference | |
| Transposition of the great arteries | 6 | 34 (11–58) | 90 | 2.6 (0.5–12.8) | |
| Hypoplastic left heart syndrome | 10 | 50 (30–69) | 97 | 4.4 (1.1–17.7) | |
| Total anomalous pulmonary venous return | 6 | 47 (26–72) | 66 | 5.1 (0.9–12.8) | |
| Birthweight | 0.003 | ||||
| Low birthweight | 10 | 16 (6–25) | 93 | Reference | |
| Moderately low birthweight | 3 | 15 (0–36) | 68 | 0.77 (0.1–4.7) | |
| Very-low birthweight | 17 | 56 (38–73) | 95 | 6.0 (2.3–15.6) | |
| Study design | 0.006 | ||||
| Hospital-based | 10 | 10 (4–15) | 17 | Reference | |
| Population-based | 20 | 49 (36–63) | 97 | 4.9 (1.6–14.5) | |
| Overall meta-analysis | 30 | 37 (27–47) | 96 | N/A | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derridj, N.; Ghanchi, A.; Bonnet, D.; Adnot, P.; Rahshenas, M.; Salomon, L.J.; Cohen, J.F.; Khoshnood, B. Early Mortality in Infants Born with Neonatally Operated Congenital Heart Defects and Low or Very-Low Birthweight: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2023, 10, 47. https://doi.org/10.3390/jcdd10020047
Derridj N, Ghanchi A, Bonnet D, Adnot P, Rahshenas M, Salomon LJ, Cohen JF, Khoshnood B. Early Mortality in Infants Born with Neonatally Operated Congenital Heart Defects and Low or Very-Low Birthweight: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2023; 10(2):47. https://doi.org/10.3390/jcdd10020047
Chicago/Turabian StyleDerridj, Neil, Ali Ghanchi, Damien Bonnet, Pauline Adnot, Makan Rahshenas, Laurent J. Salomon, Jérémie F. Cohen, and Babak Khoshnood. 2023. "Early Mortality in Infants Born with Neonatally Operated Congenital Heart Defects and Low or Very-Low Birthweight: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 10, no. 2: 47. https://doi.org/10.3390/jcdd10020047