

A Tumour and Liver Automatic Segmentation (ATLAS) Dataset on Contrast-Enhanced Magnetic Resonance Imaging for Hepatocellular Carcinoma
 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethics Approval
2.2. Data Description
2.3. CE-MRI Acquisition
- A normalisation filter that corrected the signal inhomogeneities in depth;
- An outlier removal filter applied in the frequency domain;
- 2D and 3D distortion corrections;
- Bias field correction.
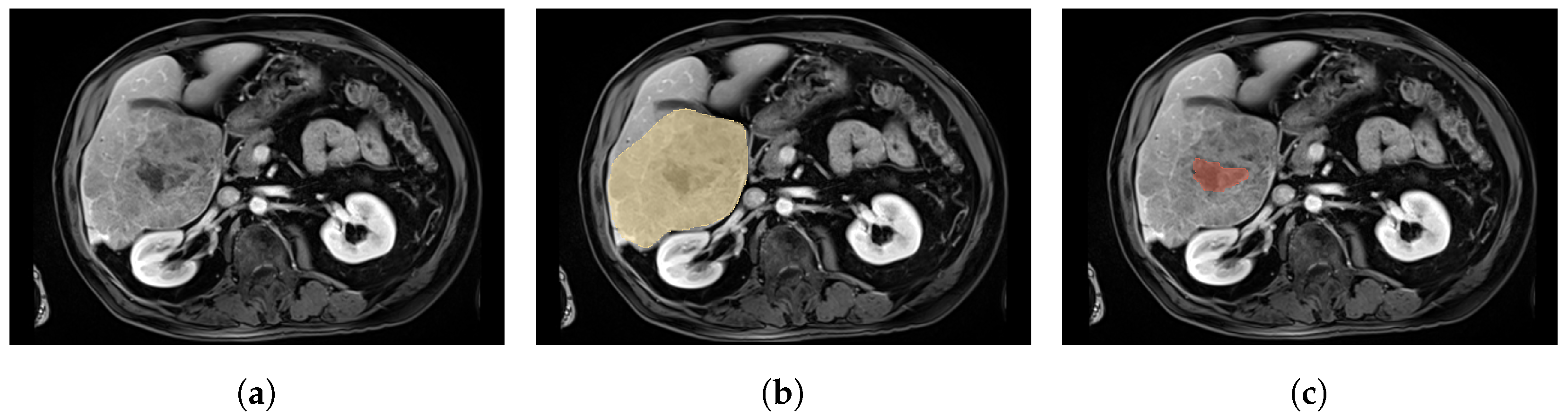
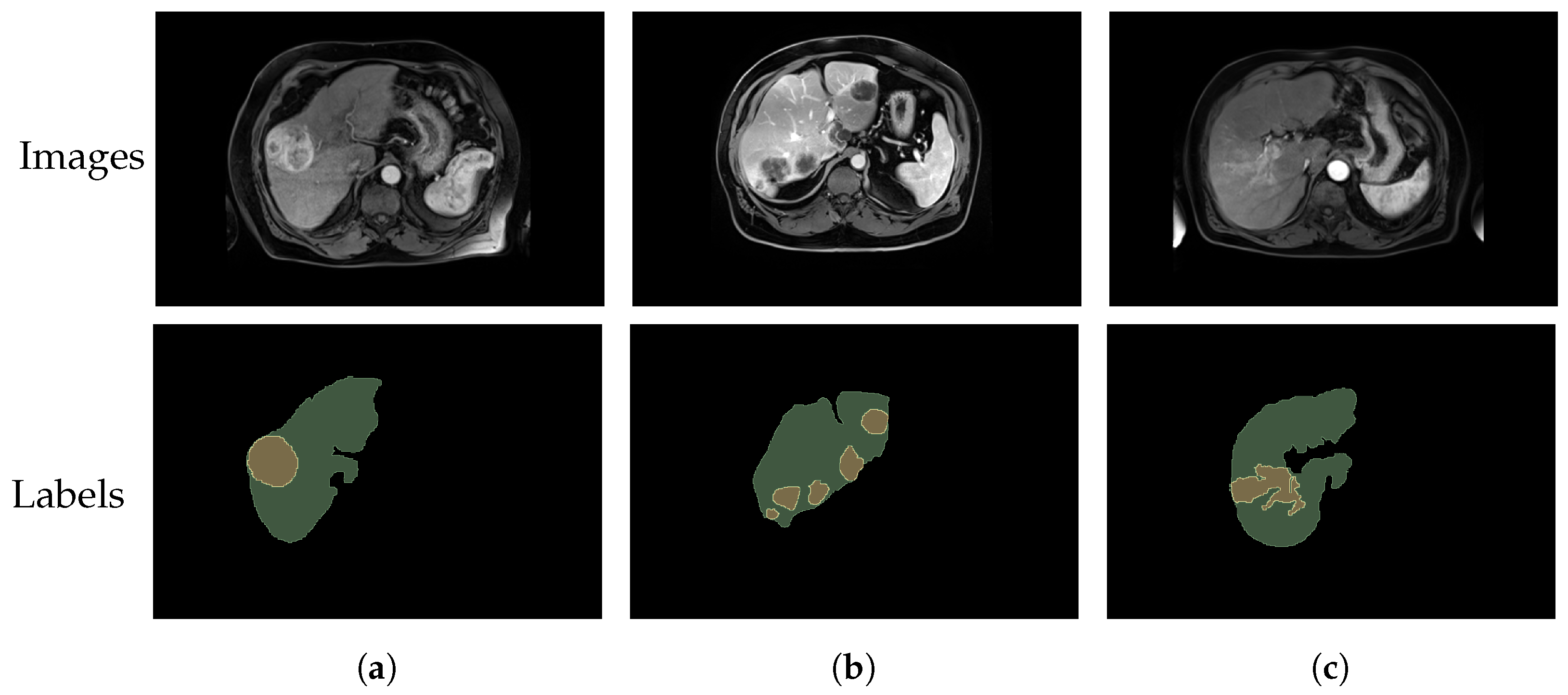
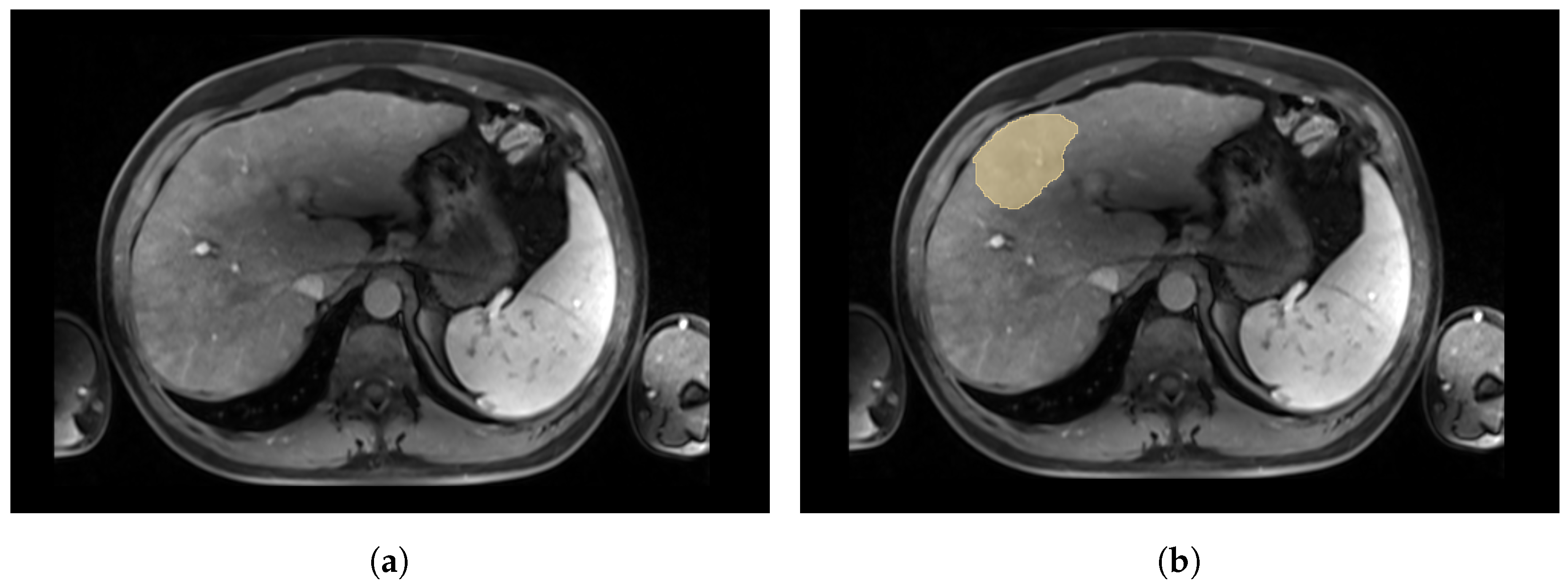
2.4. Annotation of the CE-MR Images
3. Discussion
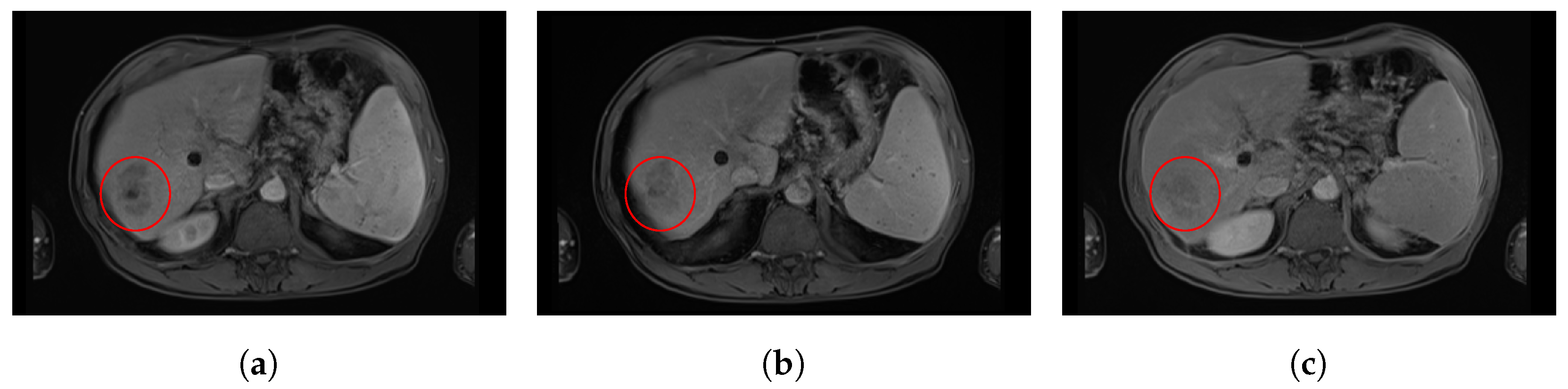
3.1. Intensity Distribution and Tumour Specifications
3.2. Training and Testing Sets’ Distribution
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/online-analysis-map (accessed on 14 February 2023).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Crocetti, L.; Bargellini, I.; Cioni, R. Loco-regional treatment of HCC: Current status. Clin. Radiol. 2017, 72, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Gates, V.L.; Atassi, B.; Lewandowski, R.J.; Ryu, R.K.; Sato, K.T.; Nemcek, A.A.; Omary, R.; Salem, R. Radioembolization with Yttrium-90 microspheres: Review of an emerging treatment for liver tumors. Futur. Oncol. 2007, 3, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Smits, M.L.; Elschot, M.; Sze, D.Y.; Kao, Y.H.; Nijsen, J.F.; Iagaru, A.H.; de Jong, H.W.; van den Bosch, M.A.; Lam, M.G. Radioembolization dosimetry: The road ahead. Cardiovasc. Interv. Radiol. 2015, 38, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Tcga-Lihc-The Cancer Imaging Archive (TCIA) Public Access. Available online: https://wiki.cancerimagingarchive.net/pages/viewpage.action?pageId=6885436 (accessed on 14 February 2023).
- Xiao, X.; Zhao, J.; Qiang, Y.; Chong, J.; Yang, X.; Kazihise, N.G.F.; Chen, B.; Li, S. Radiomics-guided GAN for segmentation of liver tumor without contrast agents. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2019: 22nd International Conference, Shenzhen, China, 13–17 October 2019; Part II 22. Springer: Berlin/Heidelberg, Germany, 2019; pp. 237–245. [Google Scholar]
- Zhao, J.; Li, D.; Kassam, Z.; Howey, J.; Chong, J.; Chen, B.; Li, S. Tripartite-GAN: Synthesizing liver contrast-enhanced MRI to improve tumor detection. Med. Image Anal. 2020, 63, 101667. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Min, J.H.; Kim, S.K.; Shin, S.Y.; Lee, M.W. Detection of hepatocellular carcinoma in contrast-enhanced magnetic resonance imaging using deep learning classifier: A multi-center retrospective study. Sci. Rep. 2020, 10, 9458. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, D.; Xiao, X.; Accorsi, F.; Marshall, H.; Cossetto, T.; Kim, D.; McCarthy, D.; Dawson, C.; Knezevic, S.; et al. United adversarial learning for liver tumor segmentation and detection of multi-modality non-contrast MRI. Med. Image Anal. 2021, 73, 102154. [Google Scholar] [CrossRef] [PubMed]
- Zheng, R.; Wang, Q.; Lv, S.; Li, C.; Wang, C.; Chen, W.; Wang, H. Automatic liver tumor segmentation on dynamic contrast enhanced mri using 4D information: Deep learning model based on 3D convolution and convolutional lstm. IEEE Trans. Med. Imaging 2022, 41, 2965–2976. [Google Scholar] [CrossRef] [PubMed]
- Bilic, P.; Christ, P.; Li, H.B.; Vorontsov, E.; Ben-Cohen, A.; Kaissis, G.; Szeskin, A.; Jacobs, C.; Mamani, G.E.H.; Chartrand, G.; et al. The liver tumor segmentation benchmark (lits). Med. Image Anal. 2023, 84, 102680. [Google Scholar] [CrossRef] [PubMed]
- Ircad France. Available online: https://www.ircad.fr/research/data-sets/liver-segmentation-3d-ircadb-01/ (accessed on 14 February 2023).
- Antonelli, M.; Reinke, A.; Bakas, S.; Farahani, K.; Kopp-Schneider, A.; Landman, B.A.; Litjens, G.; Menze, B.; Ronneberger, O.; Summers, R.M.; et al. The medical segmentation decathlon. Nat. Commun. 2022, 13, 4128. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Shi, T.; Bai, Z.; Huang, L. Ahcnet: An application of attention mechanism and hybrid connection for liver tumor segmentation in ct volumes. IEEE Access 2019, 7, 24898–24909. [Google Scholar] [CrossRef]
- Rister, B.; Yi, D.; Shivakumar, K.; Nobashi, T.; Rubin, D.L. CT-ORG, a new dataset for multiple organ segmentation in computed tomography. Sci. Data 2020, 7, 381. [Google Scholar] [CrossRef] [PubMed]
- Ouhmich, F.; Agnus, V.; Noblet, V.; Heitz, F.; Pessaux, P. Liver tissue segmentation in multiphase CT scans using cascaded convolutional neural networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Wang, B.; Gong, D.; Zhang, D.; Yang, Y.; You, Z.; Zhang, Y.; Shi, J.Q. A Comprehensive CT Dataset for Liver Computer Assisted Diagnosis. In Proceedings of the British Machine Vision Conference, Online, 22–25 November 2021. [Google Scholar]
- Remia2. 2023. Available online: https://miccai-remia.github.io/ (accessed on 14 February 2023).
- MICCAI Registered Challenges in 2023. Available online: http://www.miccai.org/special-interest-groups/challenges/ (accessed on 14 February 2023).
- Nodari, G.; Popoff, R.; Riedinger, J.M.; Lopez, O.; Pellegrinelli, J.; Dygai-Cochet, I.; Tabouret-Viaud, C.; Presles, B.; Chevallier, O.; Gehin, S.; et al. Impact of contouring methods on pre-treatment and post-treatment dosimetry for the prediction of tumor control and survival in HCC patients treated with selective internal radiation therapy. EJNMMI Res. 2021, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Mim Software. Available online: https://www.mimsoftware.com/ (accessed on 14 February 2023).
- Command Line ITK. Available online: https://github.com/benpresles/vv (accessed on 14 February 2023).
- Schlageter, M.; Terracciano, L.M.; D’Angelo, S.; Sorrentino, P. Histopathology of hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 15955. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specification Type | |
|---|---|
| Subject Area | Biomedical Imaging, Oncology |
| More specific subject area | CE-MRI segmentation of liver and HCC |
| Type of data | 3D T1 CE-MRI and associated annotations |
| How data were acquired | MR acquisitions, Siemens and GE Healthcare |
| Data format | NIfTI |
| Experimental factors | Gadolinium-based contrast agent injection |
| Experiment features | Clinical thorax/abdomen CE-MRI of HCC patients |
| Main data source location | University Hospital, Dijon 21000, France |
| Data accessibility | https://atlas-challenge.u-bourgogne.fr |
| MR Equipment | Number of Train Acquisitions | Number of Test Acquisitions |
|---|---|---|
| SIEMENS MAGNETOM SKYRA 3T | 13 | 27 |
| SIEMENS MAGNETOM AERA T | 27 | 1 |
| SIEMENS TRIOTIM 3T | 9 | 0 |
| SIEMENS MAGNETOM SOLA T | 4 | 1 |
| SIEMENS MAGNETOM AMIRA T | 0 | 1 |
| GE SIGNA HDXT T | 2 | 0 |
| GE SIGNA EXPLORER T | 2 | 0 |
| GE OPTIMA MR450W T | 1 | 0 |
| GE OPTIMA MR360 T | 1 | 0 |
| GE SIGNA VOYAGER T | 1 | 0 |
| Sequence | Number of Train Acquisitions | Number of Test Acquisitions |
|---|---|---|
| VIBE | 24 | 15 |
| VIBE CAIPIRINHA | 22 | 2 |
| VIBE TWIST | 7 | 13 |
| LAVA | 5 | 0 |
| LAVA FLEX | 2 | 0 |
| Delay after Contrast Agent Injection | Number of Train Acquisitions | Number of Test Acquisitions |
|---|---|---|
| Arterial phase | 33 | 14 |
| Portal venous phase | 10 | 15 |
| Delayed phase | 8 | 1 |
| No contrast agent | 2 | 0 |
| Unknown | 7 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinton, F.; Popoff, R.; Presles, B.; Leclerc, S.; Meriaudeau, F.; Nodari, G.; Lopez, O.; Pellegrinelli, J.; Chevallier, O.; Ginhac, D.; et al. A Tumour and Liver Automatic Segmentation (ATLAS) Dataset on Contrast-Enhanced Magnetic Resonance Imaging for Hepatocellular Carcinoma. Data 2023, 8, 79. https://doi.org/10.3390/data8050079
Quinton F, Popoff R, Presles B, Leclerc S, Meriaudeau F, Nodari G, Lopez O, Pellegrinelli J, Chevallier O, Ginhac D, et al. A Tumour and Liver Automatic Segmentation (ATLAS) Dataset on Contrast-Enhanced Magnetic Resonance Imaging for Hepatocellular Carcinoma. Data. 2023; 8(5):79. https://doi.org/10.3390/data8050079
Chicago/Turabian StyleQuinton, Félix, Romain Popoff, Benoît Presles, Sarah Leclerc, Fabrice Meriaudeau, Guillaume Nodari, Olivier Lopez, Julie Pellegrinelli, Olivier Chevallier, Dominique Ginhac, and et al. 2023. "A Tumour and Liver Automatic Segmentation (ATLAS) Dataset on Contrast-Enhanced Magnetic Resonance Imaging for Hepatocellular Carcinoma" Data 8, no. 5: 79. https://doi.org/10.3390/data8050079