

Virtual Scoliosis Surgery Using a 3D-Printed Model Based on Biplanar Radiographs

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Surgical Technique
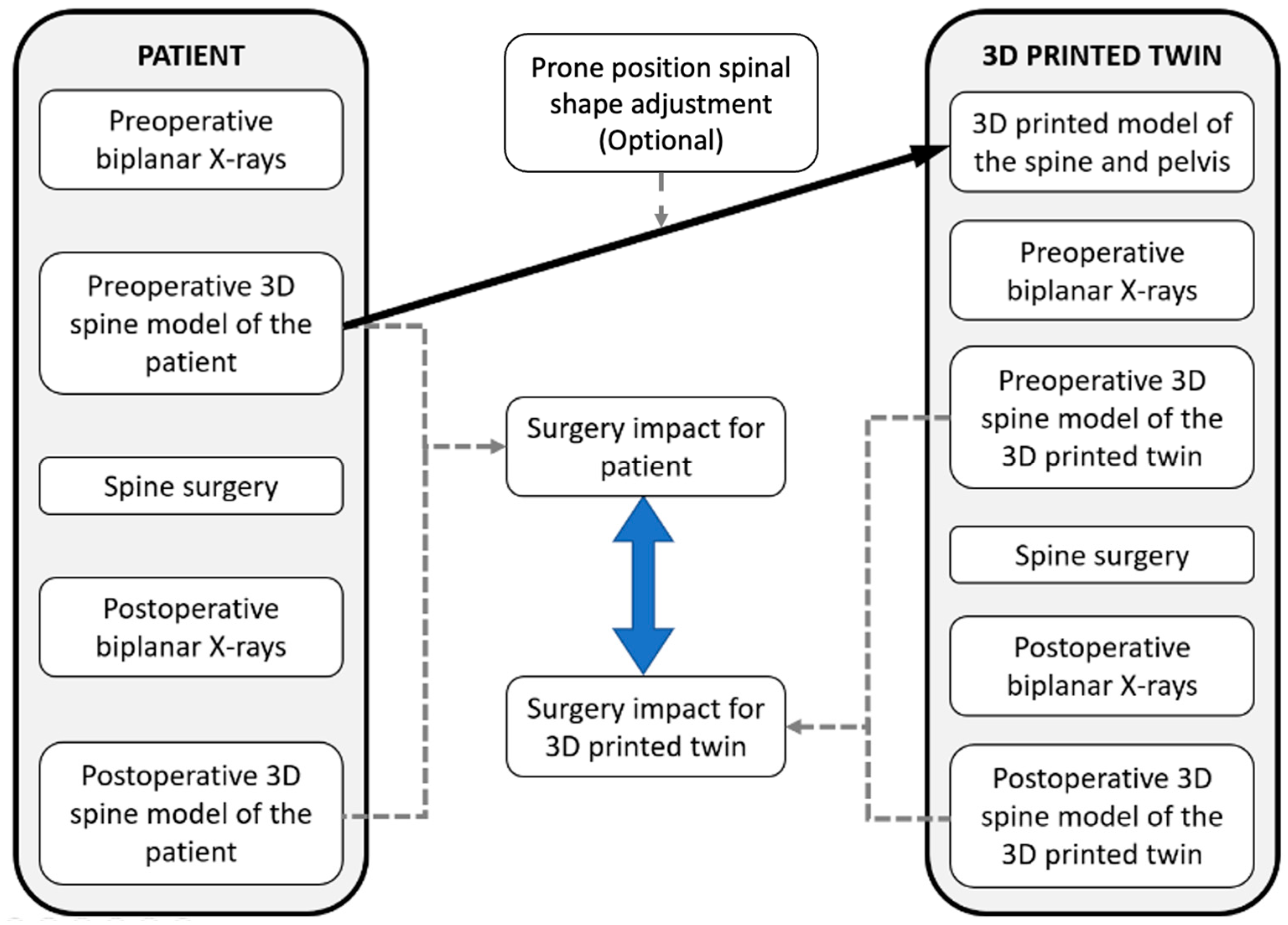
2.2. Conceptual Model
2.3. Imaging for Subject-Specific 3D Modeling
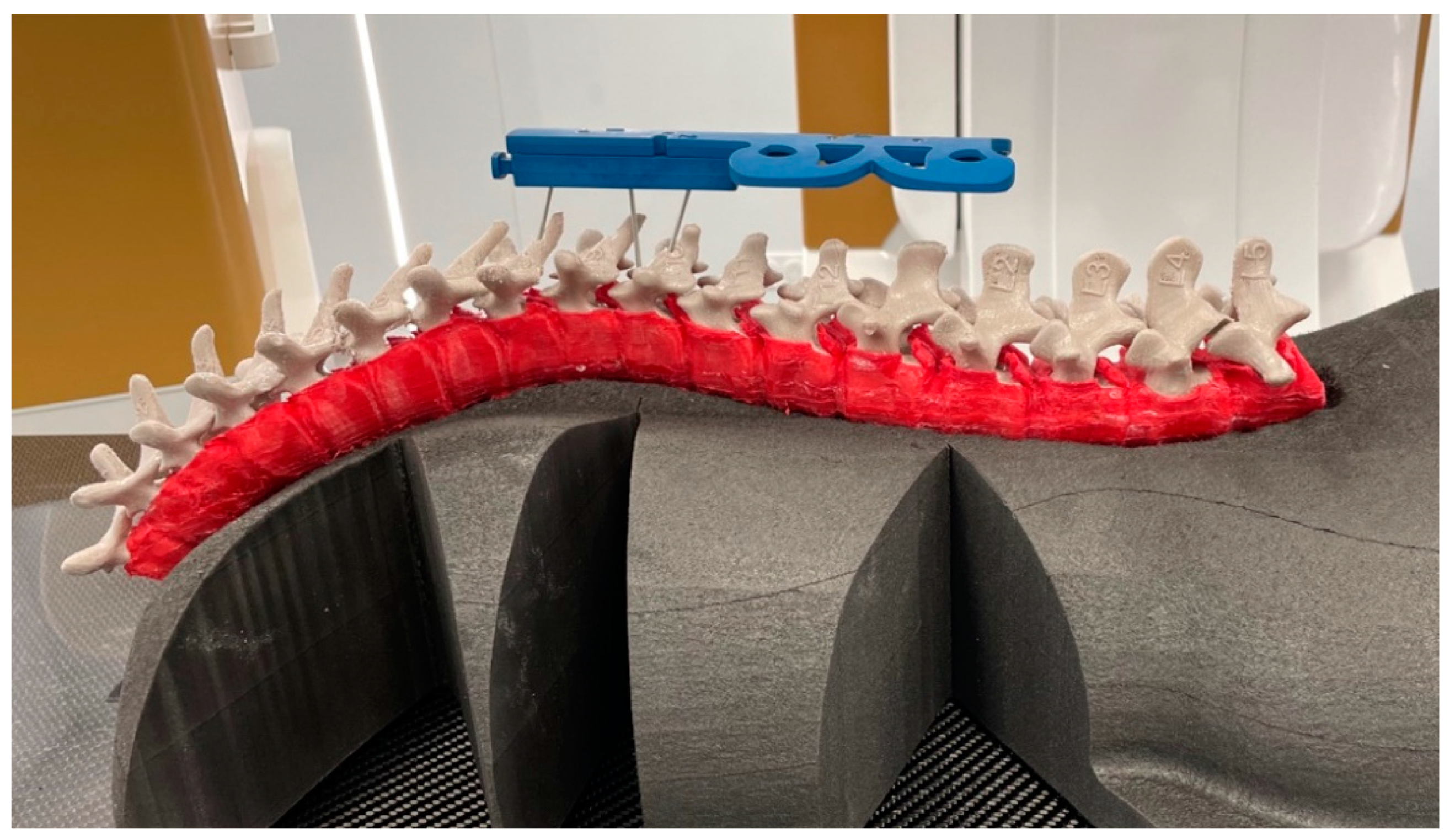
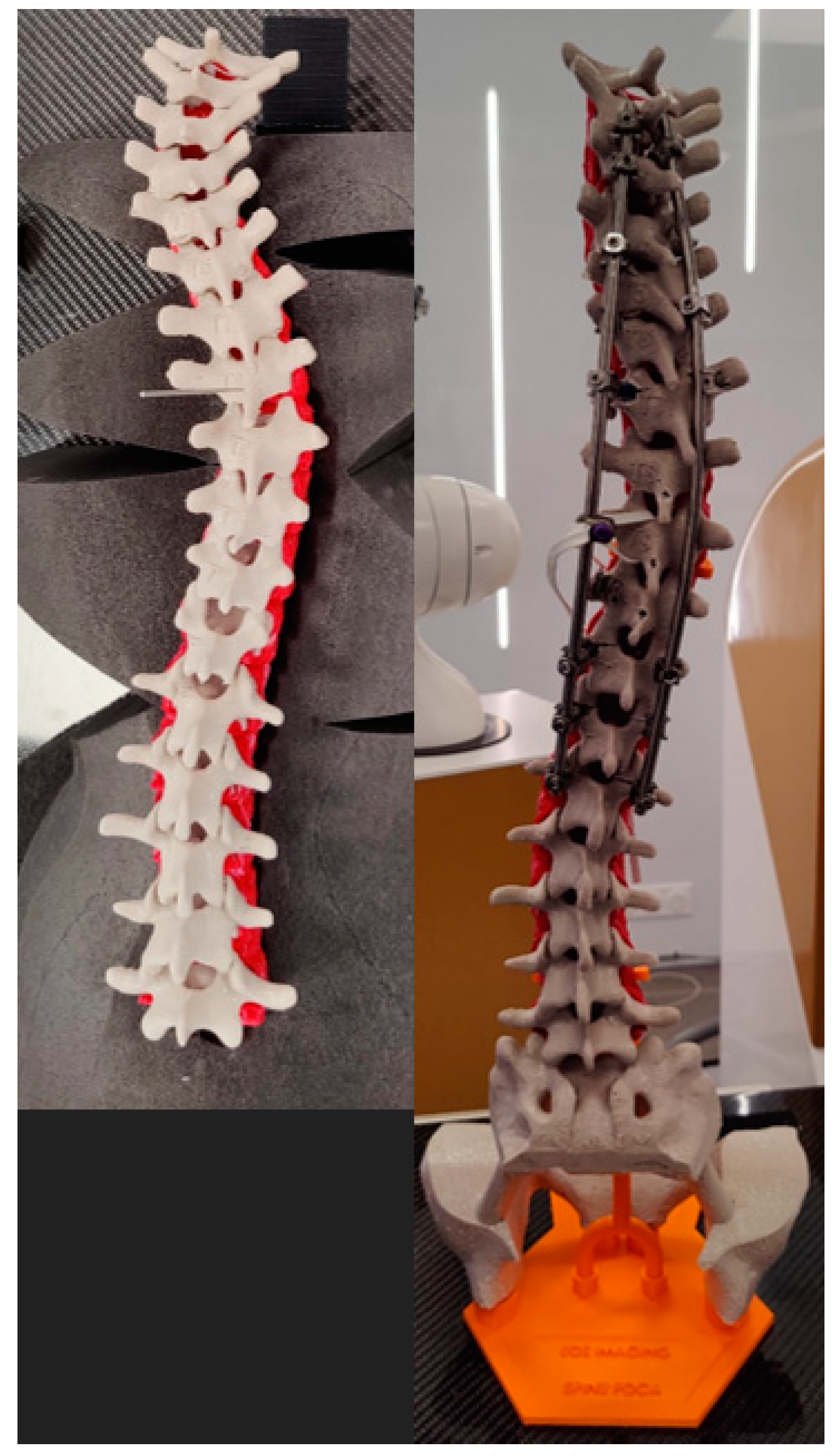
2.4. 3D Printing of the Spine
- To enable standing and prone positions of the 3D-printed spine
- To reproduce the mechanical behavior of the actual patient spine
- To be compatible with X-ray-based imaging techniques
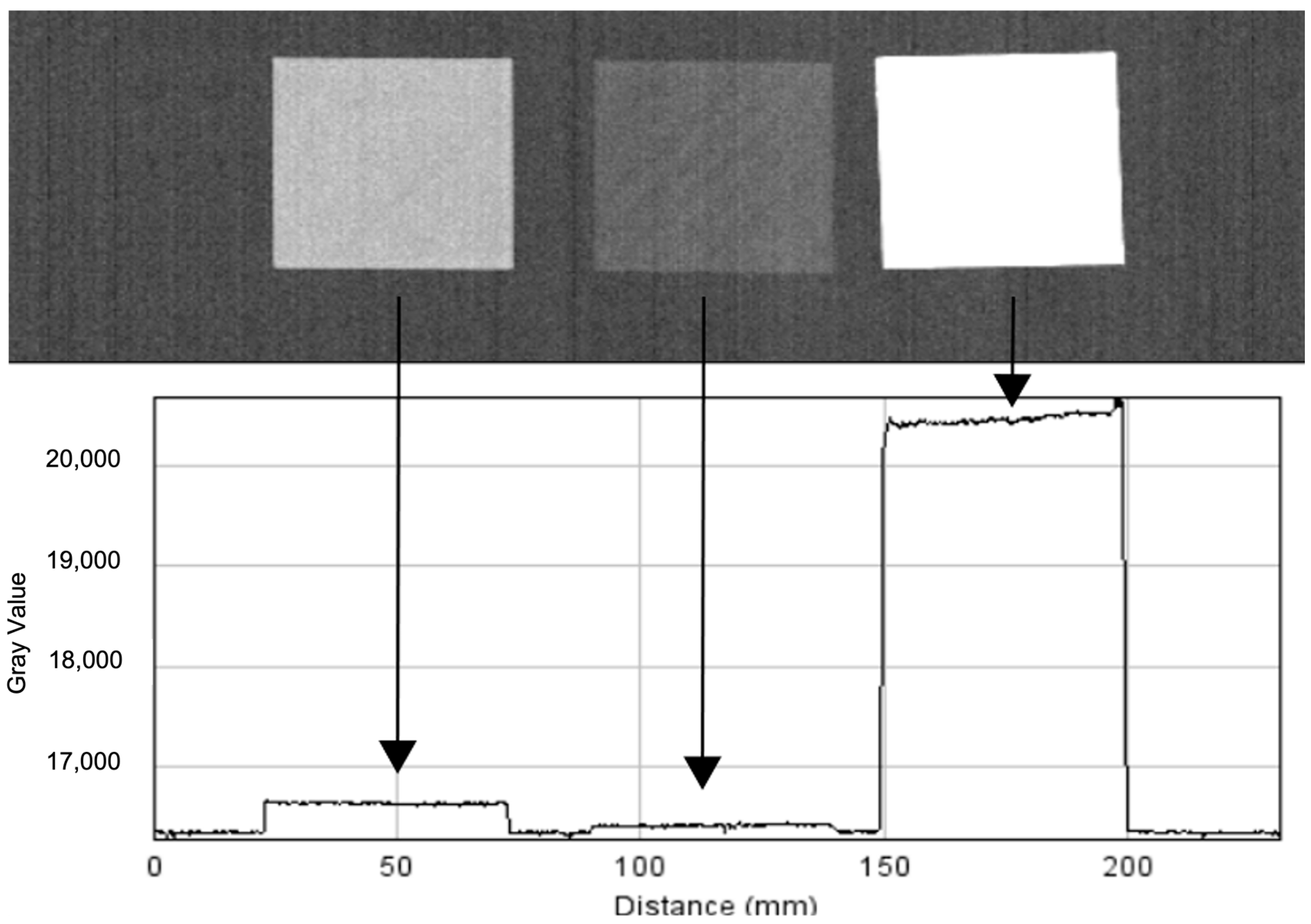
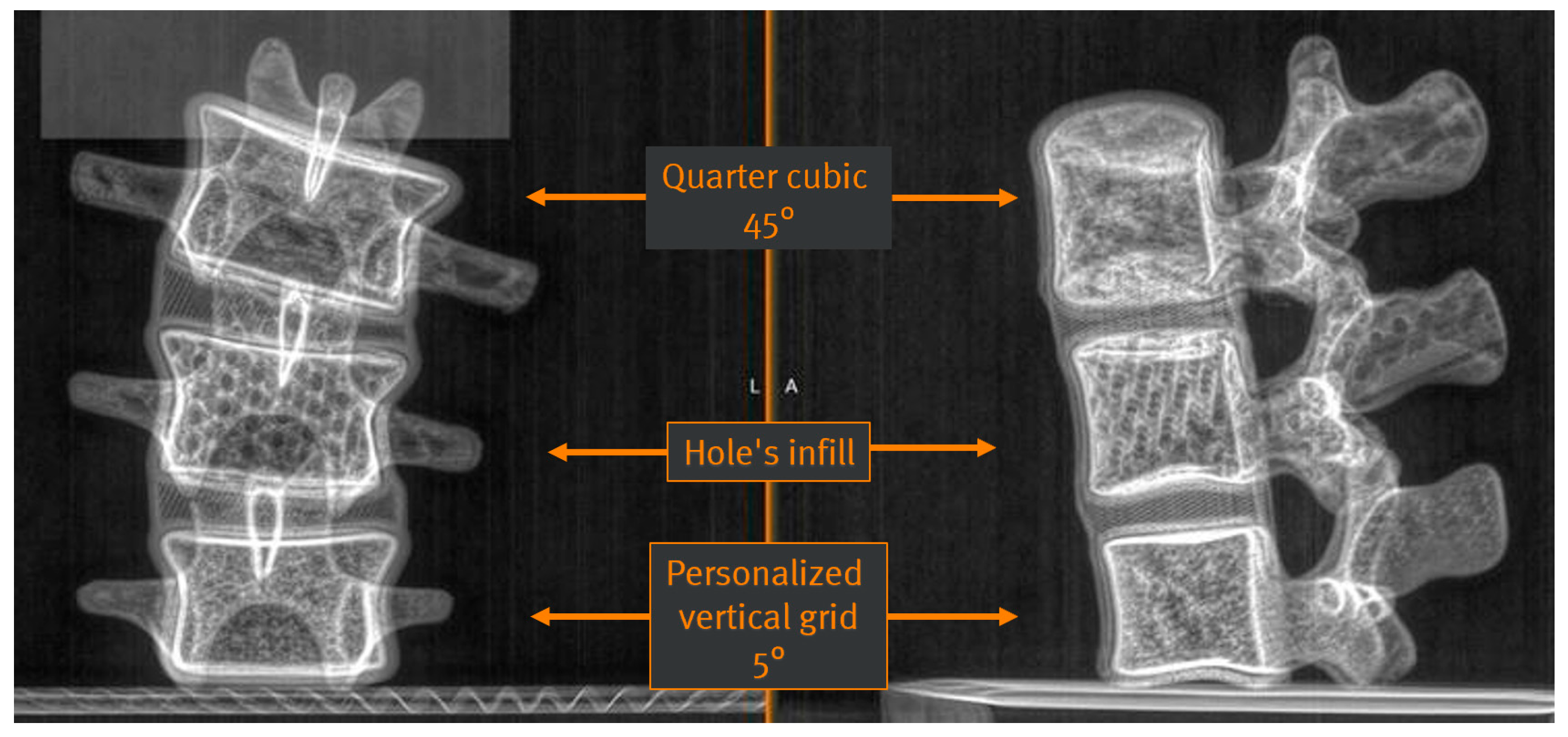
2.4.1. Vertebrae
- Polylactic acid was too too opaque.
- Polylactic acid filled with 80% copper was transparent.
- Polylactic acid with 50% ceramic was identified to reproduce the radio-opacity of bone most closely.
- Filling “quarter cubic 45°” (pre-set in the 3D printer);
- Filling “hole’s infill” (pre-set in the 3D printer);
- Filling “personalized vertical grid 5°” (customized).
2.4.2. Shell
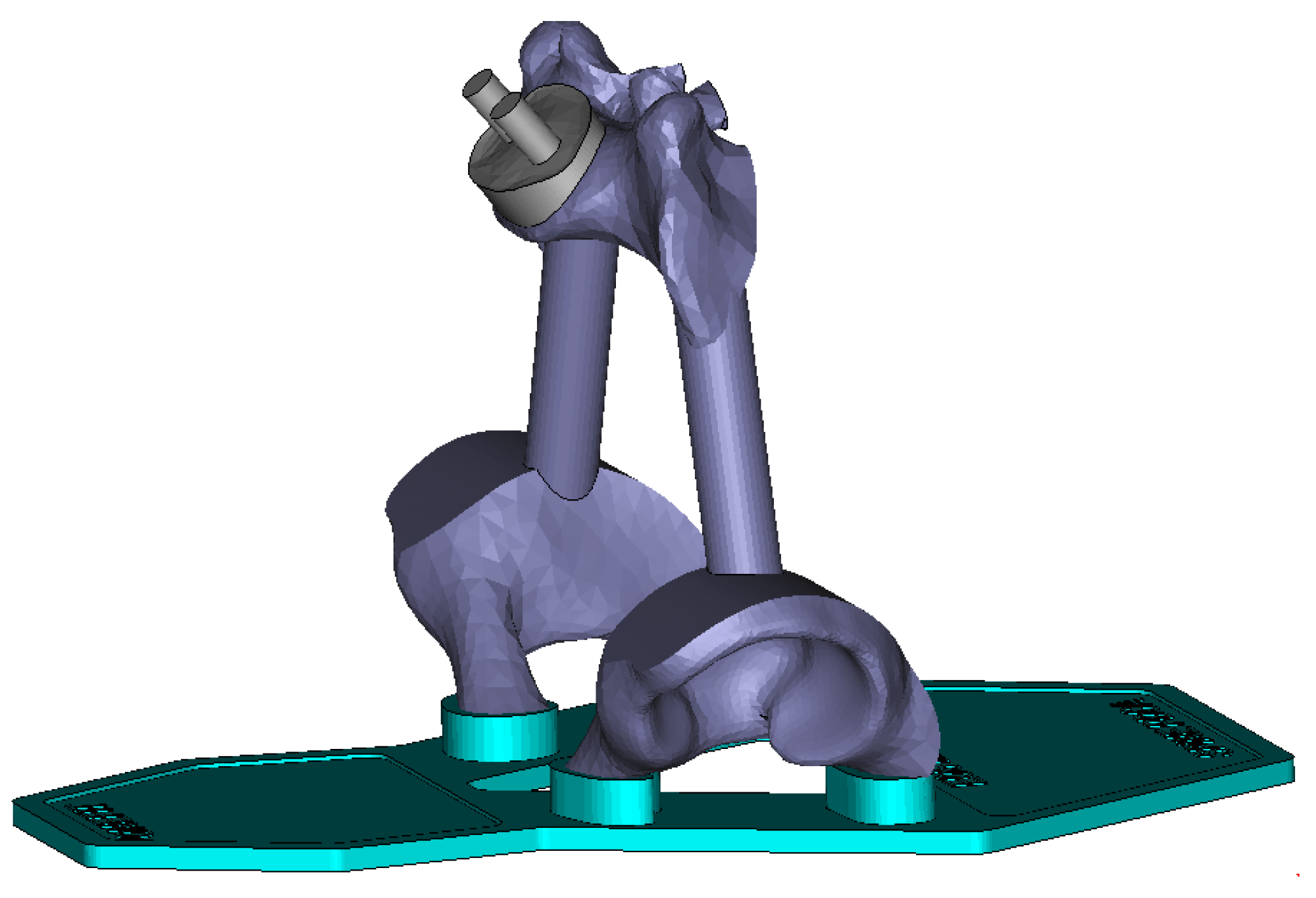
2.4.3. Pelvis and Support Structure
2.5. 3D-Printed Models’ Assessment
2.6. Virtual Surgical Procedure on 3D-Printed Models
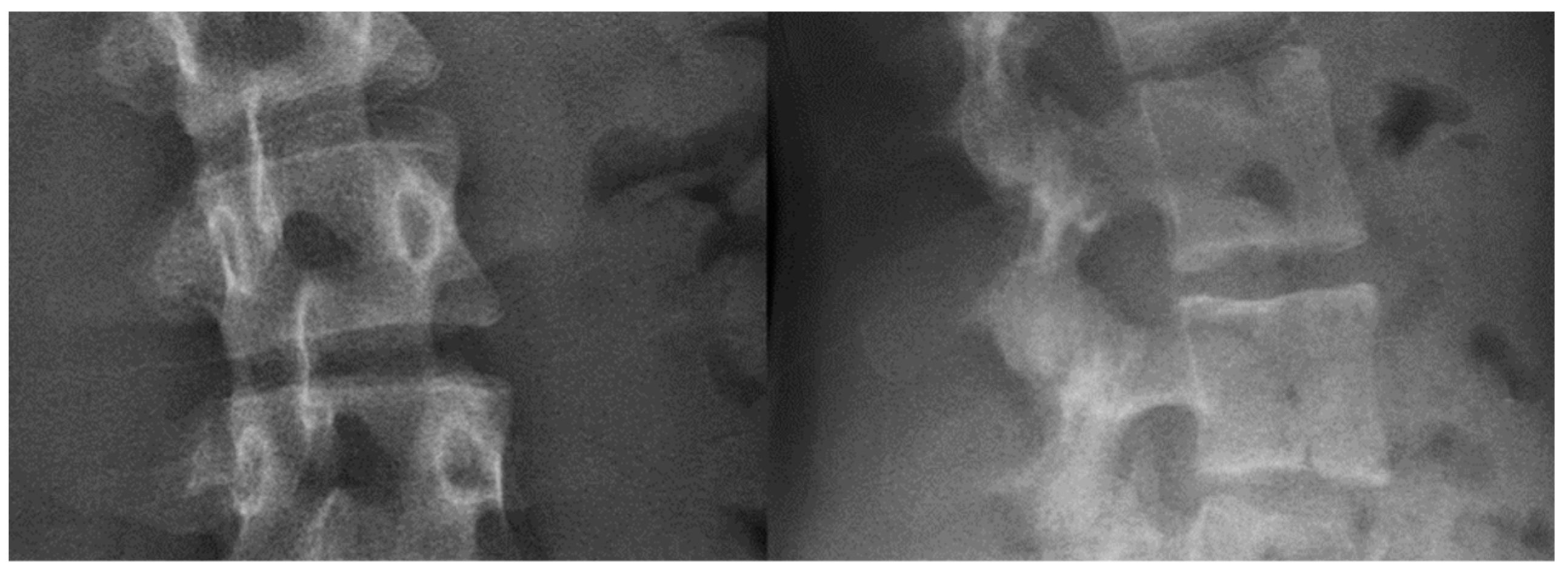
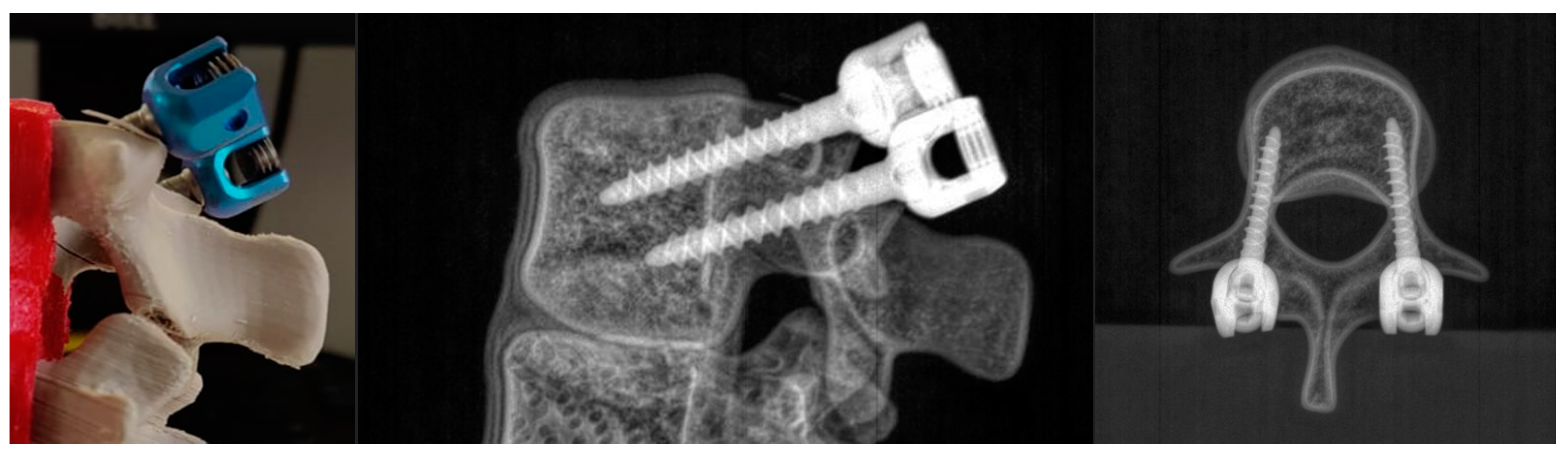
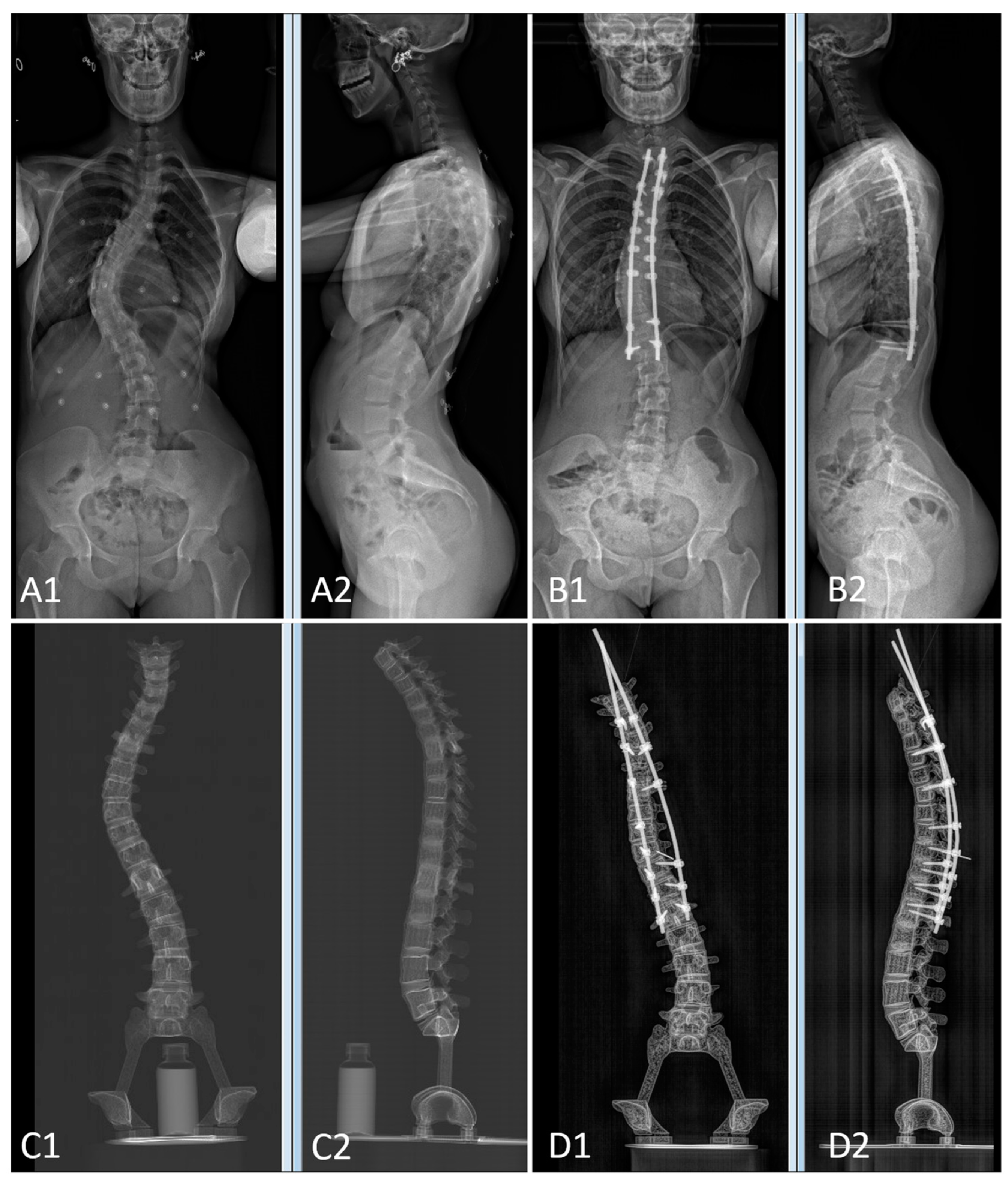
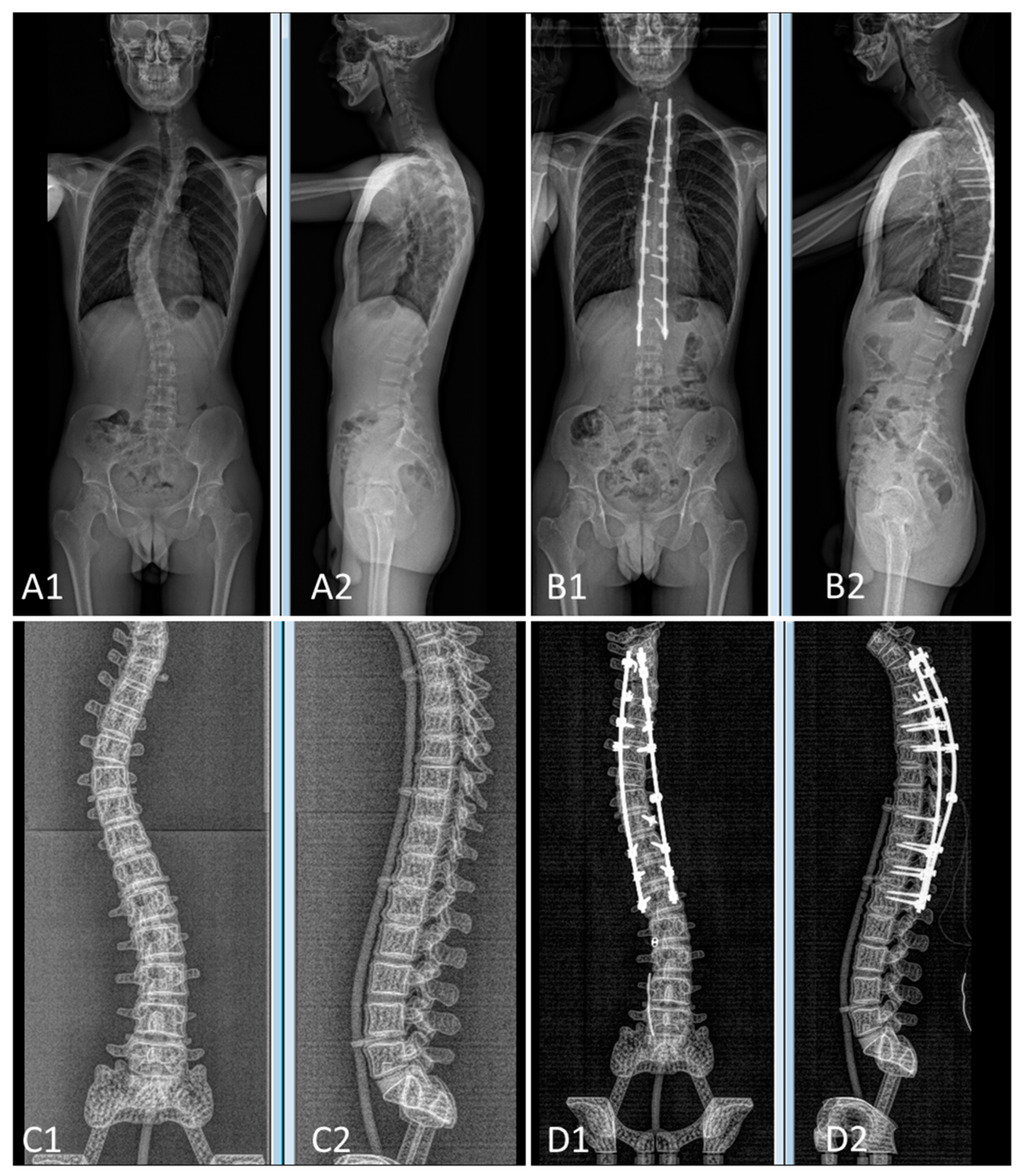
2.6.1. Preoperative and Postoperative Imaging
2.6.2. Virtual Surgery
3. Results
3.1. 3D Printing
3.2. Spinopelvic Parameters of Both Pairs of Patients and 3D-Printed Twins
3.3. Surgeon Feedback from Virtual Surgery
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Habib, A.; Jovanovich, N.; Muthiah, N.; Alattar, A.; Alan, N.; Agarwal, N.; Ozpinar, A.; Hamilton, D.K. 3D printing applications in spine surgery: An evidence-based assessment toward personalized patient care. Eur. Spine J. 2022, 31, 1682–1690. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.M.; Lin, J.L.; Kwan, K.Y.H.; Wang, X.Y.; Zhao, J. 3D-printing techniques in spine surgery: The future prospects and current challenges. Expert Rev. Med. Devices 2018, 15, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.M.Y.; Wong, P.Y.; Liu, C.; Chung, Y.L.; Wong, K.C.; Tso, C.Y.; Chow, S.K.; Cheung, W.H.; Yung, P.S.; Chui, C.S.; et al. 3D printing in orthopaedic surgery: A scoping review of randomized controlled trials. Bone Jt. Res. 2021, 10, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Kang, J.; Kim, N.; Heo, S. Accuracy of a patient-specific 3D-printed drill guide for placement of bicortical screws in atlantoaxial ventral stabilization in dogs. PLoS ONE 2022, 17, e0272336. [Google Scholar] [CrossRef]
- Xin, X.; Wang, F.; Liu, X. A 3D-printed Personalized, Combined, Modular Pedicle Subtraction Osteotomy Guide Plate System: An Experimental Study. Spine 2022, 47, 931–937. [Google Scholar] [CrossRef]
- Liao, J.Y.; Huang, C.Y.; Liao, W.C.; Kang, B.H.; Chang, K.P. Application of 3D-Printed Model in the Cervical Spine Osteochondroma Surgery: A Case Report. Ear Nose Throat J. 2021, 1455613211040577. [Google Scholar] [CrossRef]
- Thayaparan, G.K.; Owbridge, M.G.; Thompson, R.G.; D’Urso, P.S. Designing patient-specific solutions using biomodelling and 3D-printing for revision lumbar spine surgery. Eur. Spine J. 2019, 28, 18–24. [Google Scholar] [CrossRef]
- Sheha, E.D.; Gandhi, S.D.; Colman, M.W. 3D printing in spine surgery. Ann. Transl. Med. 2019, 7, S164. [Google Scholar] [CrossRef]
- Ozturk, A.M.; Suer, O.; Govsa, F.; Ozer, M.A.; Akcali, O. Patient-specific three-dimensional printing spine model for surgical planning in AO spine type-C fracture posterior long-segment fixation. Acta Orthop. Traumatol. Turc. 2022, 56, 138–146. [Google Scholar] [CrossRef]
- Shah, K.; Gadiya, A.; Shah, M.; Vyas, D.; Patel, P.; Bhojraj, S.; Nene, A. Does Three-Dimensional Printed Patient-Specific Templates Add Benefit in Revision Surgeries for Complex Pediatric Kyphoscoliosis Deformity with Sublaminar Wires in Situ? A Clinical Study. Asian Spine J. 2021, 15, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Leary, O.P.; Crozier, J.; Liu, D.D.; Niu, T.; Pertsch, N.J.; Camara-Quintana, J.Q.; Svokos, K.A.; Syed, S.; Telfeian, A.E.; Oyelese, A.A.; et al. Three-Dimensional Printed Anatomic Modeling for Surgical Planning and Real-Time Operative Guidance in Complex Primary Spinal Column Tumors: Single-Center Experience and Case Series. World Neurosurg. 2021, 145, e116–e126. [Google Scholar] [CrossRef]
- Tong, Y.; Kaplan, D.J.; Spivak, J.M.; Bendo, J.A. Three-dimensional printing in spine surgery: A review of current applications. Spine J. 2020, 20, 833–846. [Google Scholar] [CrossRef]
- Garg, B.; Mehta, N. Current status of 3D printing in spine surgery. J. Clin. Orthop. Trauma 2018, 9, 218–225. [Google Scholar] [CrossRef]
- Cai, H.; Liu, Z.; Wei, F.; Yu, M.; Xu, N.; Li, Z. 3D Printing in Spine Surgery. Adv. Exp. Med. Biol. 2018, 1093, 345–359. [Google Scholar] [CrossRef]
- Pacione, D.; Tanweer, O.; Berman, P.; Harter, D.H. The utility of a multimaterial 3D printed model for surgical planning of complex deformity of the skull base and craniovertebral junction. J. Neurosurg. 2016, 125, 1194–1197. [Google Scholar] [CrossRef]
- Wu, A.M.; Shao, Z.X.; Wang, J.S.; Yang, X.D.; Weng, W.Q.; Wang, X.Y.; Xu, H.Z.; Chi, Y.L.; Lin, Z.K. The accuracy of a method for printing three-dimensional spinal models. PLoS ONE 2015, 10, e0124291. [Google Scholar] [CrossRef]
- Markovitz, M.A.; Lu, S.; Viswanadhan, N.A. Role of 3D Printing and Modeling to Aid in Neuroradiology Education for Medical Trainees. Fed. Pract. 2021, 38, 256–260. [Google Scholar] [CrossRef]
- Koh, J.C.; Jang, Y.K.; Seong, H.; Lee, K.H.; Jun, S.; Choi, J.B. Creation of a three-dimensional printed spine model for training in pain procedures. J. Int. Med. Res. 2021, 49, 3000605211053281. [Google Scholar] [CrossRef]
- Clifton, W.; Damon, A.; Soares, C.; Nottmeier, E.; Pichelmann, M. Investigation of a three-dimensional printed dynamic cervical spine model for anatomy and physiology education. Clin. Anat. 2021, 34, 30–39. [Google Scholar] [CrossRef]
- Clifton, W.; Damon, A.; Valero-Moreno, F.; Nottmeier, E.; Pichelmann, M. The SpineBox: A Freely Available, Open-access, 3D-printed Simulator Design for Lumbar Pedicle Screw Placement. Cureus 2020, 12, e7738. [Google Scholar] [CrossRef] [Green Version]
- Senkoylu, A.; Daldal, I.; Cetinkaya, M. 3D printing and spine surgery. J. Orthop. Surg. 2020, 28, 2309499020927081. [Google Scholar] [CrossRef]
- Park, H.J.; Wang, C.; Choi, K.H.; Kim, H.N. Use of a life-size three-dimensional-printed spine model for pedicle screw instrumentation training. J. Orthop. Surg. Res. 2018, 13, 86. [Google Scholar] [CrossRef]
- Shi, J.; Fu, S.; Cavagnaro, M.J.; Xu, S.; Zhao, M. 3D Printing Improve the Effectiveness of Fracture Teaching and Medical Learning: A Comprehensive Scientometric Assessment and Future Perspectives. Front. Physiol. 2021, 12, 726591. [Google Scholar] [CrossRef] [PubMed]
- Bohl, M.A.; McBryan, S.; Pais, D.; Chang, S.W.; Turner, J.D.; Nakaji, P.; Kakarla, U.K. The Living Spine Model: A Biomimetic Surgical Training and Education Tool. Oper. Neurosurg. 2020, 19, 98–106. [Google Scholar] [CrossRef]
- Zhuang, Y.D.; Zhou, M.C.; Liu, S.C.; Wu, J.F.; Wang, R.; Chen, C.M. Effectiveness of personalized 3D printed models for patient education in degenerative lumbar disease. Patient Educ. Couns. 2019, 102, 1875–1881. [Google Scholar] [CrossRef]
- Wu, A.M.; Wang, K.; Wang, J.S.; Chen, C.H.; Yang, X.D.; Ni, W.F.; Hu, Y.Z. The addition of 3D printed models to enhance the teaching and learning of bone spatial anatomy and fractures for undergraduate students: A randomized controlled study. Ann. Transl. Med. 2018, 6, 403. [Google Scholar] [CrossRef] [PubMed]
- Burkhard, M.; Furnstahl, P.; Farshad, M. Three-dimensionally printed vertebrae with different bone densities for surgical training. Eur. Spine J. 2019, 28, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Halanski, M.A.; Elfman, C.M.; Cassidy, J.A.; Hassan, N.E.; Sund, S.A.; Noonan, K.J. Comparing results of posterior spine fusion in patients with AIS: Are two surgeons better than one? J. Orthop. 2013, 10, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Lonner, B.S.; Auerbach, J.D.; Estreicher, M.B.; Kean, K.E. Thoracic pedicle screw instrumentation: The learning curve and evolution in technique in the treatment of adolescent idiopathic scoliosis. Spine 2009, 34, 2158–2164. [Google Scholar] [CrossRef]
- Clifton, W.; Nottmeier, E.; Edwards, S.; Damon, A.; Dove, C.; Refaey, K.; Pichelmann, M. Development of a Novel 3D Printed Phantom for Teaching Neurosurgical Trainees the Freehand Technique of C2 Laminar Screw Placement. World Neurosurg. 2019, 129, e812–e820. [Google Scholar] [CrossRef]
- Humbert, L.; De Guise, J.A.; Aubert, B.; Godbout, B.; Skalli, W. 3D reconstruction of the spine from biplanar X-rays using parametric models based on transversal and longitudinal inferences. Med. Eng. Phys. 2009, 31, 681–687. [Google Scholar] [CrossRef]
- Deschenes, S.; Charron, G.; Beaudoin, G.; Labelle, H.; Dubois, J.; Miron, M.C.; Parent, S. Diagnostic imaging of spinal deformities: Reducing patients radiation dose with a new slot-scanning X-ray imager. Spine 2010, 35, 989–994. [Google Scholar] [CrossRef]
- Boudissa, M.; Prod’homme, M.; Kerschbaumer, G.; Ruatti, S.; Tonetti, J. 3D-imaging in percutaneous spine surgery using the Surgivisio system. Orthop. Traumatol. Surg. Res. 2020, 106, 1183–1186. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Rousseau, J.; Dreuil, S.; Bassinet, C.; Cao, S.; Elleaume, H. Surgivisio(R) and O-arm(R)O2 cone beam CT mobile systems for guidance of lumbar spine surgery: Comparison of patient radiation dose. Phys. Med. 2021, 85, 192–199. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Patient 1 | Patient 2 | |||||
|---|---|---|---|---|---|---|---|
| Age (years) | 14 | 18 | |||||
| BMI (kg/m2) | 26 | 24 | |||||
| Levels instrumented | T4L1 | T2L1 | |||||
| Exam | Preop | Postop | Change | Preop | Postop | Change | |
| Pelvic parameters | PI (°) | 39 | 40 | 1 | 53 | 52 | −1 |
| PT (°) | −9 | −8 | 2 | 14 | 16 | 2 | |
| SS (°) | 49 | 48 | −1 | 39 | 36 | −3 | |
| Sagittal curvatures | TK T1T12 (°) | 41 | 40 | 0 | 40 | 55 | 16 |
| LL L1S1 (°) | 73 | 55 | −19 | 55 | 53 | −2 | |
| Coronal curve 1 | Levels | L1-L3-L4 | L1-L3-L4 | NA | T12-L3-L5 | T12-L3-L5 | NA |
| Cobb (°) | 32 | 27 | −5 | 22 | 5 | −17 | |
| Coronal curve 2 | Levels | T7-T10-L1 | T7-T10-L1 | NA | T6-T9-T12 | T6-T9-T12 | NA |
| Cobb (°) | 61 | 32 | −29 | 53 | 16 | −37 | |
| Coronal curve 3 | Levels | T1-T3-T7 | T1-T3-T7 | NA | T1-T3-T6 | T1-T3-T6 | NA |
| Cobb (°) | 40 | 29 | −11 | 44 | 27 | −17 | |
| Radiological Parameters | 3D-Printed Twin 1 | 3D-Printed Twin 2 | |||||
|---|---|---|---|---|---|---|---|
| Preop | Postop | Change | Preop | Postop | Change | ||
| Pelvic parameters | PI (°) | 40 (39) | 40 (40) | 0 (1) | 54 (53) | 57 (52) | 3 (−1) |
| PT (°) | −6 (−9) | −8 (−8) | −2 (2) | 13 (14) | 15 (16) | 2 (2) | |
| SS (°) | 46 (49) | 48 (48) | 2 (−1) | 41 (39) | 42 (36) | 1 (−3) | |
| Sagittal curvatures | TK T1-T12 (°) | 46 (41) | 40 (40) | −6 (0) | 51 (40) | 59 (55) | 8 (16) |
| LL L1S1 (°) | 53 (73) | 61 (55) | 8 (−19) | 45 (55) | 53 (53) | 8 (−2) | |
| Coronal curve 1 | Levels | L1-L3-L4 | L1-L3-L4 | Na | T12-L3-L5 | T12-L3-L5 | Na |
| Cobb (°) | 29 (32) | 29 (27) | 0 (−5) | 23 (22) | 22 (5) | −1 (−17) | |
| Coronal curve 2 | Levels | T7-T10-L1 | T7-T10-L1 | Na | T6-T9-T12 | T6-T9-T12 | Na |
| Cobb (°) | 47 (61) | 27 (32) | −20 (−29) | 37 (53) | 27 (16) | −10 (−37) | |
| Coronal curve 3 | Levels | T1-T3-T7 | T1-T3-T7 | Na | T1-T3-T6 | T1-T3-T6 | Na |
| Cobb (°) | 19 (40) | 28 (29) | 9 (−11) | 37 (44) | 23 (27) | −14 (−17) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courvoisier, A.; Cebrian, A.; Simon, J.; Désauté, P.; Aubert, B.; Amabile, C.; Thiébaut, L. Virtual Scoliosis Surgery Using a 3D-Printed Model Based on Biplanar Radiographs. Bioengineering 2022, 9, 469. https://doi.org/10.3390/bioengineering9090469
Courvoisier A, Cebrian A, Simon J, Désauté P, Aubert B, Amabile C, Thiébaut L. Virtual Scoliosis Surgery Using a 3D-Printed Model Based on Biplanar Radiographs. Bioengineering. 2022; 9(9):469. https://doi.org/10.3390/bioengineering9090469
Chicago/Turabian StyleCourvoisier, Aurélien, Antonio Cebrian, Julien Simon, Pascal Désauté, Benjamin Aubert, Célia Amabile, and Lucie Thiébaut. 2022. "Virtual Scoliosis Surgery Using a 3D-Printed Model Based on Biplanar Radiographs" Bioengineering 9, no. 9: 469. https://doi.org/10.3390/bioengineering9090469