1. Introduction
Flexibility is the ability to move freely through a full range of motion, without pain or discomfort, necessary to achieve an appropriate level of physical fitness [
1]. It is considered to be one of the basic components of Health-Related Fitness, and many studies emphasize the need for stretching exercises in physical education lessons as well as a supplement to training regimens in different sports. Flexibility testing is part of any fitness assessment. However, there are no publications on the quality of flexibility tests, which consist in performing the full possible forward bend. However, it seems that the strategy for doing this exercise may be different and depends on many factors. Limitation of flexibility is believed to be a predisposing factor for musculoskeletal disorders, e.g., lumbar spine pain, injuries of the hamstrings, and even excessive muscle tension in the neck [
2,
3,
4,
5]. On the other hand, some publications disprove the relationship between the range of motion of the lumbar spine and hip joint and injuries of the hamstrings [
6]. Flexibility, which is the subject of numerous scientific reports, is paradoxically a poorly understood trait of motor skills.
In assessing flexibility, the most frequently used tests are the sit and reach and the stand and reach tests (also known as the toe touch test). They are used in physical education lessons, in physiotherapy, in sports and as one of the elements of the evaluation of physical fitness of people of different ages. These tests are commonly available as they are easy and cheap to use [
3,
7,
8]. Research shows that these tests are accurate tools, and that their scores correlate with the range of motion of the lumbar spine, hip joint and the flexibility of the hamstrings [
9]. The comparison between the sit and reach and the stand and reach tests shows no significant differences, since both tests produce similar results in the assessment of flexibility. However, surface EMG reveals that the activity of the lumbar spine extensor is higher in the stand and reach test [
10]. In our research, we used the stand and reach test because it seems to be more functional. The forward bend motion while standing is made multiple times each day, as opposed to the forward bending motion while sitting.
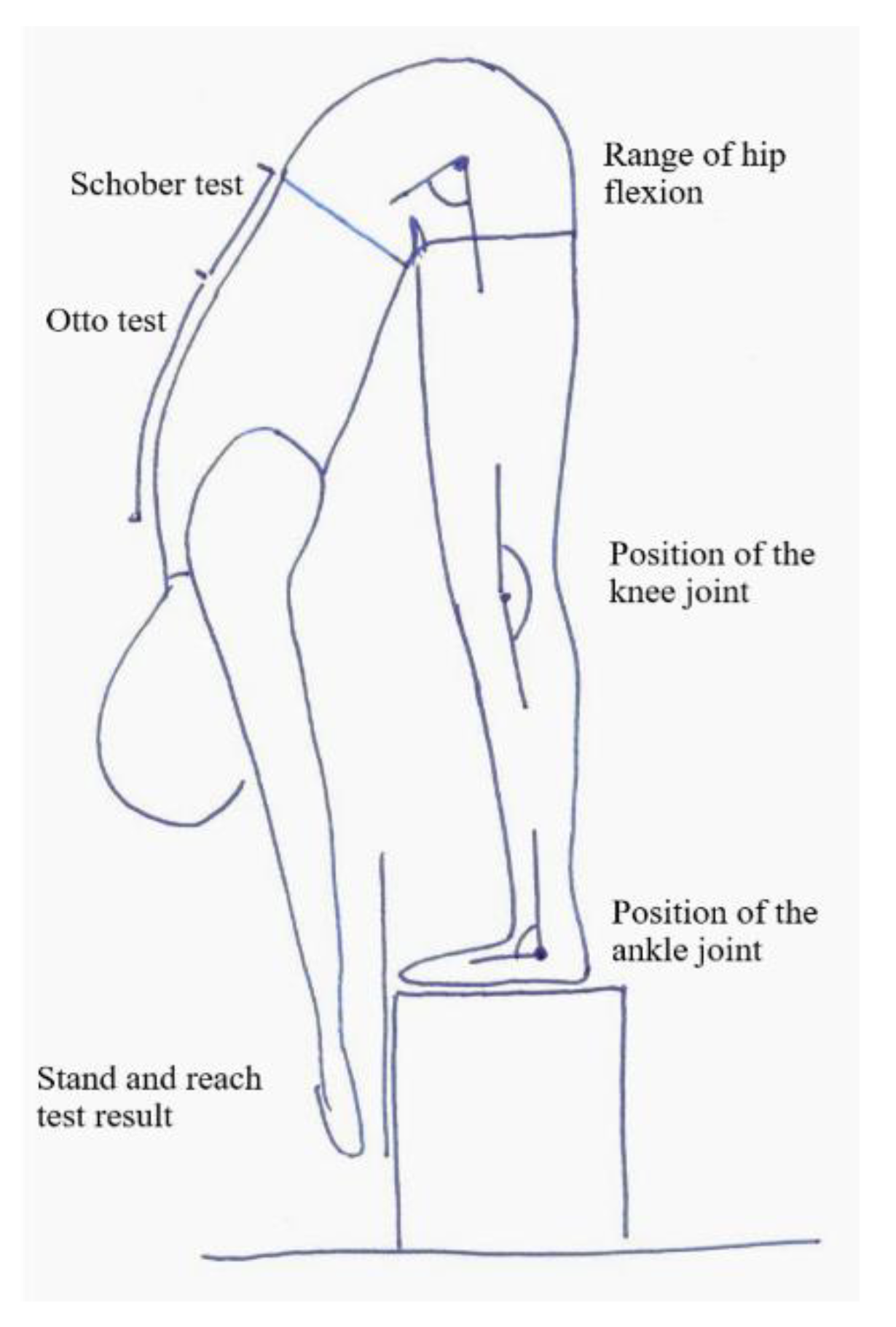
The aim of the study has been to compare the results and the quality of the stand and reach test between the girls and boys with normal body weight and those who are overweight. The objective of the research has been to discover whether gender and body weight has an influence on the amount and quality of movement. We have tried to determine whether the forward bend motion in the examined children is symmetrically distributed over the hip joints and the lumbar and thoracic spine, and how it influences the position of the knee and ankle joints. We have checked whether any body segments are hypermobile and require stabilization exercises and hypomobile and require flexibility.
3. Results
The examined girls and boys did not differ significantly in terms of body weight, height and BMI (
Table 2). Correct body weight was diagnosed in 158 (79%) of 200 children, including 78 boys and 80 girls. Twenty-two boys and twenty girls were overweight. Obesity was not found in any of the studied children.
The overweight and normal-weight children did not differ either in the stand and reach test scores (which were slightly better in overweight children), or in the range of flexion of the thoracic (Otto test) and lumbar (Schober test) spine. The position of the hip and ankle joints in the forward bend also did not differentiate between the groups. The only examined variable that significantly distinguished overweight children and children with normal body weight was the position of the knee joint in the bend. Overweight children’s knee joint was closer to the fully extended position (180°), while children with normal body weight had greater flexion in the knee joint. The difference was 2.72° (
Table 3).
The girls had slightly better stand and reach test results (the difference was 1.52 cm). During the forward bend, girls tended to use the flexion of the thoracic spine to a lesser extent (the difference of 0.12 cm), and the flexion of the lumbar spine to a greater extent (the difference of 0.32 cm). In the girls’ full bend, the hip and knee joints were less flexed (difference 1.14° and 0.19°), and the ankle joint had greater plantar flexion (difference 1.65 °) but the differences were not statistically significant (
Table 3).
In the examined children, the quality of flexibility was determined on the basis of the stand and reach test scores. It was assumed that reaching the surface of the step on which the child was standing with the tip of their longest finger (value ‘0′ on the measuring bar) means good flexibility, while poor flexibility was diagnosed when the child was unable to reach this point.
One in four children was diagnosed with good flexibility, of whom girls were found to have good flexibility slightly more frequently. Among 158 children with normal body weight, a good stand and reach test result was recorded in 24% of the participants, while among 42 overweight children, a good stand and reach test result was found in 31% of the participants (
Table 4).
Children with normal and poor flexibility did not differ in height, weight, or BMI. In children with normal flexibility, a greater range of flexion of the thoracic and lumbar spine, less flexion of the hip and knee joints and less plantar flexion of the ankle joint were observed in the position of a full forward bend (
Table 5).
Significant, though weak, correlations were found between the stand and reach test results and the mobility of the thoracic and lumbar spine as well as the position of the hip, knee and ankle joint in the bend. The analysis of the same correlations across gender groups and body weight status confirmed these observations: a better stand and reach test score was associated with a greater range of movement of the thoracic and lumbar spine (positive correlations) and less flexion of the hip joint in the bend position (negative correlation) (
Table 6).
4. Discussion
Girls and boys aged between 10 and 14 had poor flexibility. It was found that the assessment of the stand and reach helped identify children with limited flexibility, but additional tests were necessary to assess the quality of the bend. Our research showed significant differences in the method of performing the bend by children with good and poor flexibility. Girls and boys with a good flexibility test score used more thoracic and lumbar spine flexion and held the knee and ankle joints closer to the neutral position. In children with limited flexibility, reduced flexion within the spine joints, greater flexion of the hip and knee joints and greater plantar flexion of the ankle joint were noted. Moreover, it was found that gender and also the body weight status had not an influence on the result of the stand and reach test and the quality of the performance of the bend.
There was no evidence of an influence of being overweight on the result and quality of the stand and reach test. Nikoladis’s research also indicates the lack of a relationship between BMI and body fat and flexibility in adolescents and adults [
16]. On the other hand, Hands et al. [
17], different to our study, diagnosed better results of flexibility in teenage girls compared to boys of the same age.
The average result of the Schober test indicated limited mobility of the lumbar spine in the examined children. This finding was true for both genders, with the range of lumbar spine motion being slightly smaller in boys.
According to Kendall et al. [
18], the correct range of hip motion in the forward bend (sit and reach) is around 80° (the angle between the sacrum and the horizontal line). Comerford and Mottram [
19] determined the correct range of hip flexion during a forward bend while standing at 70°. Comparing our findings with the conclusions of the above-mentioned authors, we observed that the examined children used the hip joint excessively. At the same time, the participants found it difficult to extend the knee joint. The question is: does this tendency indicate a weakening of the hamstring muscles in the upper segments and the shortening of these muscles in the lower segments? Perhaps this hypothesis can be explained by the sedentary lifestyle that is very common today. Of course, our research does not answer this question, but only motivates the search for the answer. Rakholiya et al. [
20] indicated in their research that a sedentary lifestyle leads to an imbalance of hip extensor. On the other hand, the influence of the sedentary life on the flexibility of hamstrings is unclear. One study shows that long-lasting sitting can lead to hamstring tightness [
21], others contradict this thesis [
22]. However, the above-mentioned studies investigated the elasticity of hamstrings as a whole, without taking into account that their proximal and distal segments, acting on a different joint (as hip extensors or knee flexors), may have different flexibility.
The stand and reach and sit and reach tests are often used to evaluate the flexibility of the hamstrings. According to Magnusson et al. [
23], the range of the forward bend is a good measure of the flexibility of these muscles. As Chillon et al. [
24] state, the hip angle explains 42% of the sit and reach test result, the lumbar angle-30% and the thoracic angle-just 4%. The research carried out by Muyor et al. [
8] shows, however, that the sit and reach test correlates poorly or at most moderately with the flexibility of the hamstrings as assessed by the passive strait leg raise test. It must be remembered that both the sit and reach test and the stand and reach test are indirect measures and the limitation of flexibility diagnosed by one of these tests cannot be a direct indication for stretching the hamstrings [
8]. Stretching the structures that are not shortened leads to hypermobility which, like hypomobility, can cause injury and reduced sport performance [
25].
4.1. Limitations
It seems that in further studies on flexibility, the flexibility of the hamstrings and the flexibility of the calf muscles should be additionally assessed in an isolated study.
4.2. Clinical Implications
It was our intention that our findings should stimulate further research to seek answers to the following questions: What is correct flexibility? Is the range or the quality of the movement more important? How to find a compromise between these features? Should the approach to stretching exercises change: first the analysis of the quantity and quality of the forward bend, then individually selected exercises for segmental increase in flexibility and stabilization of hypermobile segments?


 ,
, 

{kind=link}