
Negative Pressure Wound Therapy in Spinal Surgery

 , and
, and
Abstract
:
1. Introduction
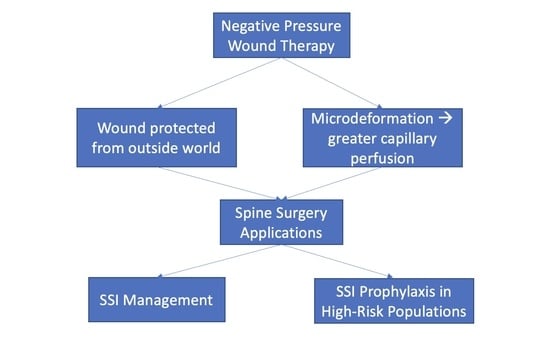
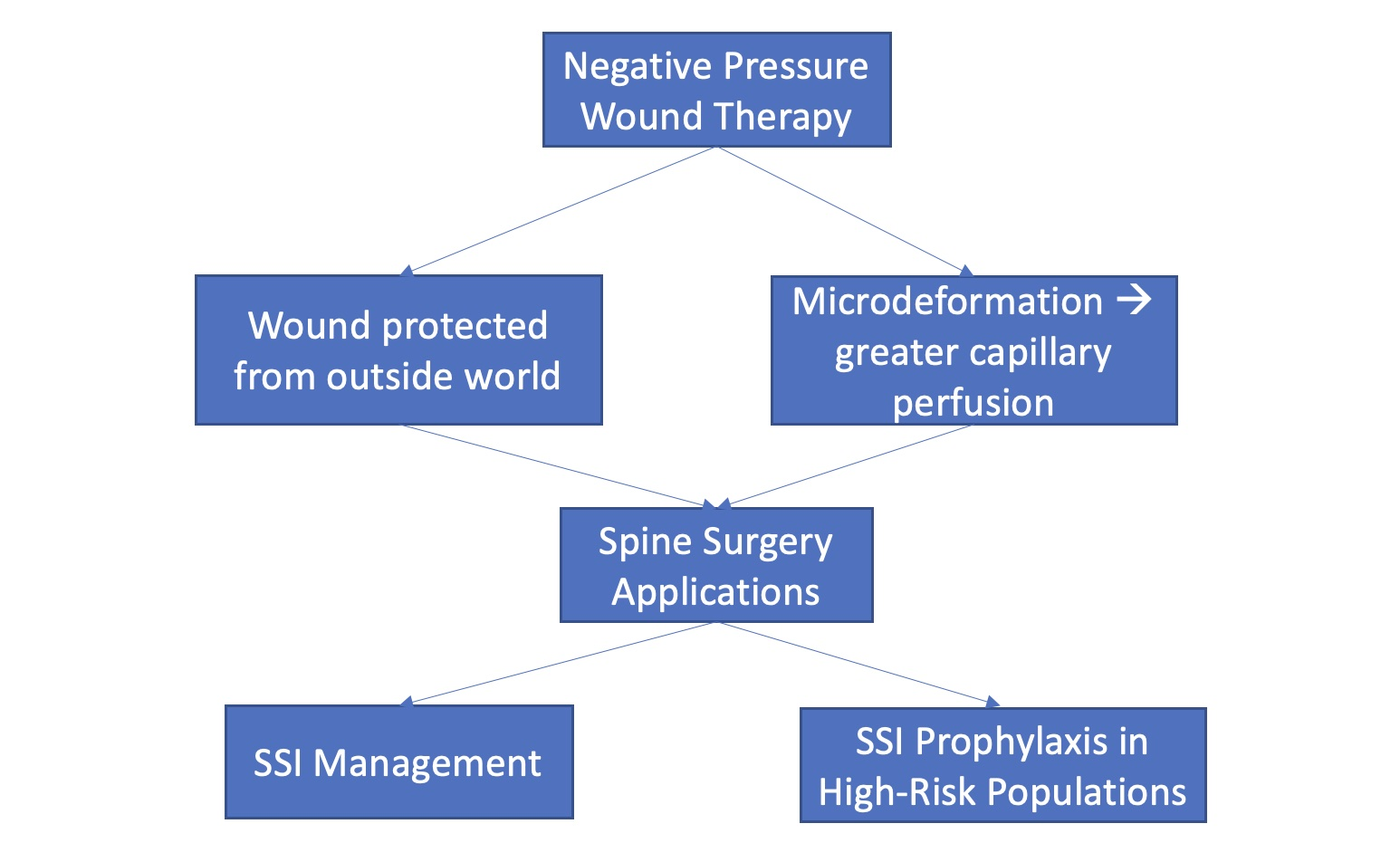
2. Mechanisms and Evidence for NPWT
3. NPWT in Spine
3.1. NPWT for Infection Management
Safety of NPWT over Exposed Spinal Dura
3.2. NPWT for Infection Prophylaxis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Webster, J.; Liu, Z.; Norman, G.; Dumville, J.C.; Chiverton, L.; Scuffham, P.; Stankiewicz, M.; Chaboyer, W.P. Negative Pressure Wound Therapy for Surgical Wounds Healing by Primary Closure. Cochrane Database Syst. Rev. 2019, 3, CD009261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalise, A.; Calamita, R.; Tartaglione, C.; Pierangeli, M.; Bolletta, E.; Gioacchini, M.; Gesuita, R.; Benedetto, G. Di Improving Wound Healing and Preventing Surgical Site Complications of Closed Surgical Incisions: A Possible Role of Incisional Negative Pressure Wound Therapy. A Systematic Review of the Literature. Int. Wound J. 2016, 13, 1260–1281. [Google Scholar] [CrossRef] [PubMed]
- Horch, R.E.; Ludolph, I.; Müller-Seubert, W.; Zetzmann, K.; Hauck, T.; Arkudas, A.; Geierlehner, A. Topical Negative-Pressure Wound Therapy: Emerging Devices and Techniques. Expert Rev. Med. Devices 2020, 17, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.; Scuffham, P.; Sherriff, K.L.; Stankiewicz, M.; Chaboyer, W.P. Negative Pressure Wound Therapy for Skin Grafts and Surgical Wounds Healing by Primary Intention. Cochrane Database Syst. Rev. 2012, 4, CD009261. [Google Scholar]
- Agarwal, P.; Kukrele, R.; Sharma, D. Vacuum Assisted Closure (VAC)/Negative Pressure Wound Therapy (NPWT) for Difficult Wounds: A Review. J. Clin. Orthop. Trauma 2019, 10, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Normandin, S.; Safran, T.; Winocour, S.; Chu, C.K.; Vorstenbosch, J.; Murphy, A.M.; Davison, P.G. Negative Pressure Wound Therapy: Mechanism of Action and Clinical Applications. Semin. Plast. Surg. 2021, 35, 164–170. [Google Scholar] [CrossRef]
- Morykwas, M.J.; Argenta, L.C.; Shelton-Brown, E.I.; McGuirt, W. Vacuum-Assisted Closure: A New Method for Wound Control and Treatment: Animal Studies and Basic Foundation. Ann. Plast. Surg. 1997, 38, 837–840. [Google Scholar] [CrossRef]
- Willy, C.; Agarwal, A.; Andersen, C.A.; De Santis, G.; Gabriel, A.; Grauhan, O.; Guerra, O.M.; Lipsky, B.A.; Malas, M.B.; Mathiesen, L.L.; et al. Closed Incision Negative Pressure Therapy: International Multidisciplinary Consensus Recommendations. Int. Wound J. 2017, 14, 385–398. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Leavitt, T.; Bayer, L.R.; Orgill, D.P. Effect of Negative Pressure Wound Therapy on Wound Healing. Curr. Probl. Surg. 2014, 51, 301–331. [Google Scholar] [CrossRef] [Green Version]
- Lalezari, S.; Lee, C.J.; Borovikova, A.A.; Banyard, D.A.; Paydar, K.Z.; Wirth, G.A.; Widgerow, A.D. Deconstructing Negative Pressure Wound Therapy. Int. Wound J. 2017, 14, 649–657. [Google Scholar] [CrossRef]
- Kim, D.C.; Carlson, B.C.; Shafa, E.; Mehbod, A.A. Vacuum-Assisted Wound Closure Management for Posterior Lumbar Spine Infections. J. Am. Acad. Orthop. Surg. 2022, 30, 395–399. [Google Scholar] [CrossRef]
- Janssen, A.H.J.; Mommers, E.H.H.; Notter, J.; De Vries Reilingh, T.S.; Wegdam, J.A. Negative Pressure Wound Therapy versus Standard Wound Care on Quality of Life: A Systematic Review. J. Wound Care 2016, 25, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Gabriel, A.; Lantis, J.; Téot, L. Clinical Recommendations and Practical Guide for Negative Pressure Wound Therapy with Instillation. Int. Wound J. 2016, 13, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Z.; Xu, X.H.; Wang, D.W.; Lin, Y.M.; Lin, N.; Lu, H.D. Negative Pressure Wound Therapy for Surgical Site Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Microbiol. Infect. 2019, 25, 1328–1338. [Google Scholar] [CrossRef] [PubMed]
- Suh, H.; Lee, A.Y.; Park, E.J.; Hong, J.P. Negative Pressure Wound Therapy on Closed Surgical Wounds with Dead Space Animal Study Using a Swine Model. Ann. Plast. Surg. 2016, 76, 717–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilpadi, D.V.; Lessing, C.; Derrick, K. Healed Porcine Incisions Previously Treated with a Surgical Incision Management System: Mechanical, Histomorphometric, and Gene Expression Properties. Aesthetic Plast. Surg. 2014, 38, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Atkins, B.Z.; Tetterton, J.K.; Petersen, R.P.; Hurley, K.; Wolfe, W.G. Laser Doppler Flowmetry Assessment of Peristernal Perfusion after Cardiac Surgery: Beneficial Effect of Negative Pressure Therapy. Int. Wound J. 2011, 8, 56–62. [Google Scholar] [CrossRef]
- Semsarzadeh, N.N.; Tadisina, K.K.; Maddox, J.; Chopra, K.; Singh, D.P. Closed Incision Negative-Pressure Therapy Is Associated with Decreased Surgical-Site Infections: A Meta-Analysis. Plast. Reconstr. Surg. 2015, 136, 592–602. [Google Scholar] [CrossRef]
- Hyldig, N.; Birke-Sorensen, H.; Kruse, M.; Vinter, C.; Joergensen, J.S.; Sorensen, J.A.; Mogensen, O.; Lamont, R.F.; Bille, C. Meta-Analysis of Negative-Pressure Wound Therapy for Closed Surgical Incisions. Br. J. Surg. 2016, 103, 477–486. [Google Scholar] [CrossRef] [Green Version]
- Andrew Glennie, R.; Dea, N.; Street, J.T. Dressings and Drains in Posterior Spine Surgery and Their Effect on Wound Complications. J. Clin. Neurosci. 2015, 22, 1081–1087. [Google Scholar] [CrossRef]
- Biancari, F.; Santoro, G.; Provenzano, F.; Savarese, L.; Iorio, F.; Giordano, S.; Zebele, C.; Speziale, G. Negative-Pressure Wound Therapy for Prevention of Sternal Wound Infection after Adult Cardiac Surgery: Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4268. [Google Scholar] [CrossRef] [PubMed]
- Grauhan, O.; Navasardyan, A.; Hofmann, M.; Müller, P.; Stein, J.; Hetzer, R. Prevention of Poststernotomy Wound Infections in Obese Patients by Negative Pressure Wound Therapy. J. Thorac. Cardiovasc. Surg. 2013, 145, 1387–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickl, S.; Steindl, J.; Langthaler, D.; Nierlich-Hold, A.; Pona, I.; Hitzl, W.; Kocher, A.; Happak, W.; Radtke, C.; Tzou, C.H. First Experiences with Incisional Negative Pressure Wound Therapy in a High-Risk Poststernotomy Patient Population Treated with Pectoralis Major Muscle Flap for Deep Sternal Wound Infection. J. Reconstr. Microsurg. 2018, 34, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nam, D.; Sershon, R.A.; Levine, B.R.; Della Valle, C.J. The Use of Closed Incision Negative-Pressure Wound Therapy in Orthopaedic Surgery. J. Am. Acad. Orthop. Surg. 2018, 26, 295–302. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, H.; Cen, S.; Huang, F. Negative Pressure Wound Therapy versus Conventional Wound Dressings in Treatment of Open Fractures: A Systematic Review and Meta-Analysis. Int. J. Surg. 2018, 53, 72–79. [Google Scholar] [CrossRef]
- Svensson-Björk, R.; Saha, S.; Acosta, S.; Gerdtham, U.G.; Hasselmann, J.; Asciutto, G.; Zarrouk, M. Cost-Effectiveness Analysis of Negative Pressure Wound Therapy Dressings after Open Inguinal Vascular Surgery—The Randomised INVIPS-Trial. J. Tissue Viability 2021, 30, 95–101. [Google Scholar] [CrossRef]
- Petrou, S.; Parker, B.; Masters, J.; Achten, J.; Bruce, J.; Lamb, S.E.; Parsons, N.; Costa, M.L.; Willett, K.; Griffin, D.; et al. Cost-Effectiveness of Negative-Pressure Wound Therapy in Adults with Severe Open Fractures of the Lower Limb: Evidence from the WOLLF Randomized Controlled Trial. Bone Joint J. 2019, 101-B, 1392–1401. [Google Scholar] [CrossRef]
- Hyldig, N.; Joergensen, J.S.; Wu, C.; Bille, C.; Vinter, C.A.; Sorensen, J.A.; Mogensen, O.; Lamont, R.F.; Möller, S.; Kruse, M. Cost-Effectiveness of Incisional Negative Pressure Wound Therapy Compared with Standard Care after Caesarean Section in Obese Women: A Trial-Based Economic Evaluation. BJOG 2019, 126, 619–627. [Google Scholar] [CrossRef]
- Ousey, K.J.; Atkinson, R.A.; Williamson, J.B.; Lui, S. Negative Pressure Wound Therapy (NPWT) for Spinal Wounds: A Systematic Review. Spine J. 2013, 13, 1393–1405. [Google Scholar] [CrossRef] [Green Version]
- White, A.J.; Fiani, B.; Jarrah, R.; Momin, A.A.; Rasouli, J. Surgical Site Infection Prophylaxis and Wound Management in Spine Surgery. Asian Spine J. 2022, 16, 451–461. [Google Scholar] [CrossRef]
- Mehbod, A.A.; Ogilvie, J.W.; Pinto, M.R.; Schwender, J.D.; Transfeldt, E.E.; Wood, K.B.; Le Huec, J.C.; Dressel, T. Postoperative Deep Wound Infections in Adults after Spinal Fusion: Management with Vacuum-Assisted Wound Closure. J. Spinal Disord. Tech. 2005, 18, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Labler, L.; Keel, M.; Trentz, O.; Heinzelmann, M. Wound Conditioning by Vacuum Assisted Closure (V.A.C.) in Postoperative Infections after Dorsal Spine Surgery. Eur. Spine J. 2006, 15, 1388–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.; Zhu, L.; Jiang, Z.L.; Huang, Z.H.; Wu, X.T. The Use of Incisional Vacuum-Assisted Closure System Following One-Stage Incision Suture Combined with Continuous Irrigation to Treat Early Deep Surgical Site Infection after Posterior Lumbar Fusion with Instrumentation. J. Orthop. Surg. Res. 2021, 16, 445. [Google Scholar] [CrossRef] [PubMed]
- Canavese, F.; Gupta, S.; Krajbich, J.I.; Emara, K.M. Vacuum-Assisted Closure for Deep Infection after Spinal Instrumentation for Scoliosis. J. Bone Jt. Surg. Ser. B 2008, 90, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Canavese, F.; Marengo, L.; Corradin, M.; Mansour, M.; Samba, A.; Andreacchio, A.; Rousset, M.; Dimeglio, A. Deep Postoperative Spine Infection Treated by Negative Pressure Therapy in Patients with Progressive Spinal Deformities. Arch. Orthop. Trauma Surg. 2018, 138, 463–469. [Google Scholar] [CrossRef]
- van Rhee, M.A.; de Klerk, L.W.L.; Verhaar, J.A.N. Vacuum-Assisted Wound Closure of Deep Infections after Instrumented Spinal Fusion in Six Children with Neuromuscular Scoliosis. Spine J. 2007, 7, 596–600. [Google Scholar] [CrossRef]
- Horn, P.L.; Ruth, B.; Kean, J.R. Use of Wound V.A.C. Therapy in Pediatric Patients with Infected Spinal Wounds: A Retrospective Review. Orthop. Nurs. 2007, 26, 317–324. [Google Scholar] [CrossRef]
- Jones, G.A.; Butler, J.; Lieberman, I.; Schlenk, R. Negative-Pressure Wound Therapy in the Treatment of Complex Postoperative Spinal Wound Infections: Complications and Lessons Learned Using Vacuum-Assisted Closure. J. Neurosurg. Spine 2007, 6, 407–411. [Google Scholar] [CrossRef]
- Foxx, K.C.; Mesfin, A.; Molinari, R. Negative-Pressure Dressing Management of Recurrent Postoperative Epidural Hematoma and Uncontrollable Intraoperative Hemorrhage in Posterior Spine Surgery: Report of 4 Cases. J. Neurosurg. Spine 2018, 28, 220–225. [Google Scholar] [CrossRef] [Green Version]
- Novelli, G.; Daleffe, F.; Birra, G.; Canzi, G.; Mazzoleni, F.; Boni, P.; Maino, C.; Giussani, C.; Sozzi, D.; Bozzetti, A. Negative Pressure Wound Therapy in Complex Cranio-Maxillofacial and Cervical Wounds. Int. Wound J. 2018, 15, 16–23. [Google Scholar] [CrossRef]
- Watt, J.P.; Dunn, R.N. The Use of Vacuum Dressings for Dead Space Management in Deep Surgical Site Infections Allows Implant and Bone Graft Retention. Glob. Spine J. 2017, 7, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.; Beder, D.; Street, J.; Boyd, M.; Fisher, C.; Dvorak, M.; Paquette, S.; Kwon, B. The Use of Vacuum-Assisted Closure in Spinal Wound Infections with or without Exposed Dura. Eur. Spine J. 2018, 27, 2536–2542. [Google Scholar] [CrossRef] [PubMed]
- Ploumis, A.; Mehbod, A.A.; Dressel, T.D.; Dykes, D.C.; Transfeldt, E.E.; Lonstein, J.E. Therapy of Spinal Wound Infections Using Vacuum-Assisted Wound Closure: Risk Factors Leading to Resistance to Treatment. J. Spinal Disord. Tech. 2008, 21, 320–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rickert, M.; Rauschmann, M.; Latif-Richter, N.; Arabmotlagh, M.; Rahim, T.; Schmidt, S.; Fleege, C. Management of Deep Spinal Wound Infections Following Instrumentation Surgery with Subfascial Negative Pressure Wound Therapy. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kale, M.; Padalkar, P.; Mehta, V. Vacuum-Assisted Closure in Patients with Post-Operative Infections after Instrumented Spine Surgery: A Series of 12 Cases. J. Orthop. Case Rep. 2017, 7, 95–100. [Google Scholar] [CrossRef]
- Yuan, W.; Liu, X.; Zhou, X.; Pei, L.; Zhu, Y. Management of Early Deep Wound Infection after Thoracolumbar Instrumentation. Spine 2018, 43, E1089–E1095. [Google Scholar] [CrossRef]
- Chen, K.; Lin, J.-t.; Sun, S.-b.; Lin, J.; Kong, J.-z.; Tian, N.-f. Vacuum-Assisted Closure Combined with a Closed Suction Irrigation System for Treating Postoperative Wound Infections Following Posterior Spinal Internal Fixation. J. Orthop. Surg. Res. 2018, 13, 321. [Google Scholar] [CrossRef]
- Shi, H.; Zhu, L.; Chen, L.; Jiang, Z.L.; Xu, Z.Y.; Wu, X.T. A Novel Technique for Treating Early Deep Surgical Site Infection After Posterior Lumbar Fusion with Instrumentation. World Neurosurg. 2021, 156, e167–e174. [Google Scholar] [CrossRef]
- Hrašovec, S.; Rečnik, G. Initial Experience Using Negative Pressure Wound Therapy with Instillation and Dwell Time for Postoperative Wound Treatment After Spinal Fusion Surgery: A Case Report. Wounds 2020, 32, E71–E75. [Google Scholar]
- Khan, S.A.; Choudry, U.K.; Salim, A.; Nathani, K.R.; Enam, S.A.; Shehzad, N. Current Management Trends for Surgical Site Infection After Posterior Lumbar Spinal Instrumentation: A Systematic Review. World Neurosurg. 2022, 164, 374–380. [Google Scholar] [CrossRef]
- Kurra, S.; Rashid, A.; Yirenkyi, H.; Castle, P.; Lavelle, W.F. Outcomes of Negative Pressure Wound Therapies in the Management of Spine Surgical Site Wound Infections. Int. J. Spine Surg. 2020, 14, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Alcala-Marquez, C.; Torrealba, R.; Mehbod, A.A.; Dawson, J.M.; Dressel, T.D.; Transfeldt, E.E. Recurrent Surgical Site Infections in the Spine after Treatment with the Vacuum-Assisted Closure (VAC) System. Clin. Spine Surg. 2018, 31, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Ridwan, S.; Grote, A.; Simon, M. Safety and Efficacy of Negative Pressure Wound Therapy for Deep Spinal Wound Infections After Dural Exposure, Durotomy, or Intradural Surgery. World Neurosurg. 2020, 134, e624–e630. [Google Scholar] [CrossRef] [PubMed]
- Pujji, O.; Farrar, E.; Jeffery, S. Negative Pressure Wound Therapy to the Dura. J. Burn. Care Res. 2018, 39, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Adogwa, O.; Fatemi, P.; Perez, E.; Moreno, J.; Gazcon, G.C.; Gokaslan, Z.L.; Cheng, J.; Gottfried, O.; Bagley, C.A. Negative Pressure Wound Therapy Reduces Incidence of Postoperative Wound Infection and Dehiscence after Long-Segment Thoracolumbar Spinal Fusion: A Single Institutional Experience. Spine J. 2014, 14, 2911–2917. [Google Scholar] [CrossRef] [PubMed]
- Nordmeyer, M.; Pauser, J.; Biber, R.; Jantsch, J.; Lehrl, S.; Kopschina, C.; Rapke, C.; Bail, H.J.; Forst, R.; Brem, M.H. Negative Pressure Wound Therapy for Seroma Prevention and Surgical Incision Treatment in Spinal Fracture Care. Int. Wound J. 2016, 13, 1176–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyck, B.A.; Bailey, C.S.; Steyn, C.; Petrakis, J.; Urquhart, J.C.; Raj, R.; Rasoulinejad, P. Use of Incisional Vacuum-Assisted Closure in the Prevention of Postoperative Infection in High-Risk Patients Who Underwent Spine Surgery: A Proof-of-Concept Study. J. Neurosurg. Spine 2019, 31, 430–439. [Google Scholar] [CrossRef]
- Akhter, A.S.; McGahan, B.G.; Close, L.; Dornbos, D.; Toop, N.; Thomas, N.R.; Christ, E.; Dahdaleh, N.S.; Grossbach, A.J. Negative Pressure Wound Therapy in Spinal Fusion Patients. Int. Wound J. 2021, 18, 158–163. [Google Scholar] [CrossRef]
- Vidalis, B.M.; Ngwudike, S.I.; McCandless, M.G.; Chohan, M.O. Negative Pressure Wound Therapy in Facilitating Wound Healing After Surgical Decompression for Metastatic Spine Disease. World Neurosurg. 2021, 159, e407–e415. [Google Scholar] [CrossRef]
- Naylor, R.M.; Gilder, H.E.; Gupta, N.; Hydrick, T.C.; Labott, J.R.; Mauler, D.J.; Trentadue, T.P.; Ghislain, B.; Elder, B.D.; Fogelson, J.L. Effects of Negative Pressure Wound Therapy on Wound Dehiscence and Surgical Site Infection Following Instrumented Spinal Fusion Surgery—A Single Surgeon’s Experience. World Neurosurg. 2020, 137, e257–e262. [Google Scholar] [CrossRef]
- Mueller, K.B.; D’Antuono, M.; Patel, N.; Pivazyan, G.; Aulisi, E.F.; Evans, K.K.; Nair, M.N. Effect of Incisional Negative Pressure Wound Therapy vs Standard Wound Dressing on the Development of Surgical Site Infection after Spinal Surgery: A Prospective Observational Study. Neurosurgery 2021, 88, E445–E451. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Sun, J.; Yao, Z.; Song, C.; Liu, W. Can Prophylactic Negative Pressure Wound Therapy Improve Clinical Outcomes in Spinal Fusion Surgery? A Meta-Analysis. Eur. Spine J. 2022, 31, 1546–1552. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Name | Manufacturer | Uses | Portable? |
|---|---|---|---|
| V.A.C.® Ulta | 3MTM | NPWT, instillation | No |
| V.A.C.® Simplicity | 3MTM | NPWT, ciNPWT | Yes |
| V.A.C.® Rx4 | 3MTM | NPWT in up to 4 wounds | No |
| ActiV.A.C.® | 3MTM | NPWT, home care | Yes |
| ActiV.A.C.® with iOn ProgressTM | 3MTM | NPWT with monitoring of home use | Yes |
| V.A.C.® Via | 3MTM | NPWT for 7 days | Yes |
| Pico System | Smith + Nephew | ciNPWT | Yes |
| PrevenaTM | 3MTM | NPWT, ciNPWT | Yes |
| Proposed Use | Recommendation | Level of Evidence |
|---|---|---|
| Treatment of deep and superficial SSI | Wound VACs are effective in managing SSI | 2A |
| ciNPWT for infection prophylaxis | Supported by literature in orthopedic and cardiac surgery | 2A |
| Routine use of ciNPWT | Likely not beneficial | 3B |
| Routine use of ciNPWT in “high-risk” patient populations | Potentially beneficial; more studies are needed | 2B |
| Cost-effectiveness | Unknown | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
White, A.J.; Gilad, R.; Motivala, S.; Fiani, B.; Rasouli, J. Negative Pressure Wound Therapy in Spinal Surgery. Bioengineering 2022, 9, 614. https://doi.org/10.3390/bioengineering9110614
White AJ, Gilad R, Motivala S, Fiani B, Rasouli J. Negative Pressure Wound Therapy in Spinal Surgery. Bioengineering. 2022; 9(11):614. https://doi.org/10.3390/bioengineering9110614
Chicago/Turabian StyleWhite, Alexandra Jeanne, Ronit Gilad, Soriaya Motivala, Brian Fiani, and Jonathan Rasouli. 2022. "Negative Pressure Wound Therapy in Spinal Surgery" Bioengineering 9, no. 11: 614. https://doi.org/10.3390/bioengineering9110614