
Associations with Blood Lead and Urinary Cadmium Concentrations in Relation to Mortality in the US Population: A Causal Survival Analysis with G-Computation

Abstract
:1. Introduction
2. Methods
2.1. Design and Participants
2.2. Mortality Data
2.3. Measurements of Blood Lead and Urinary Cadmium
2.4. Covariates
2.5. Statistical Analysis
2.6. Sensitivity Analyses
3. Results
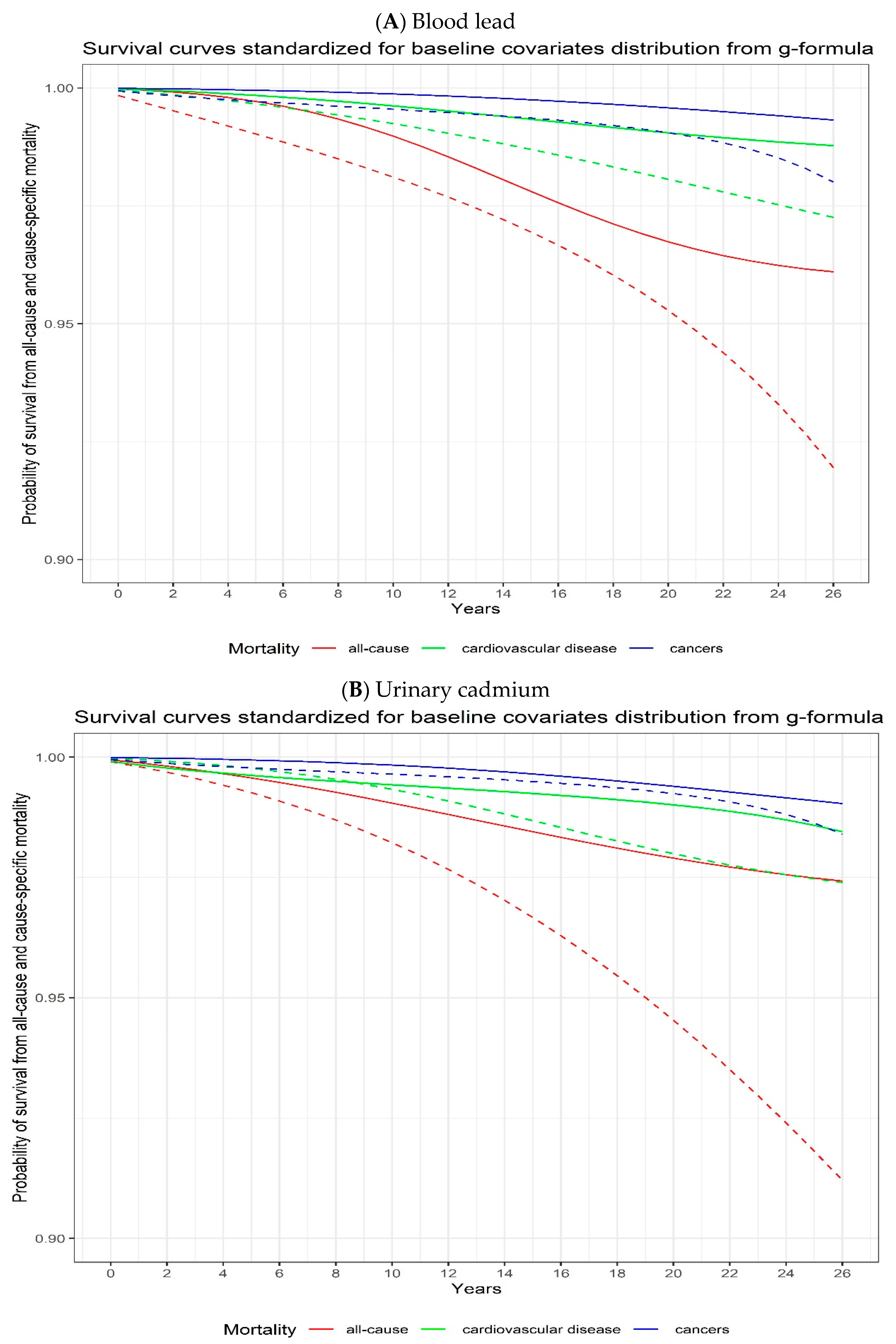
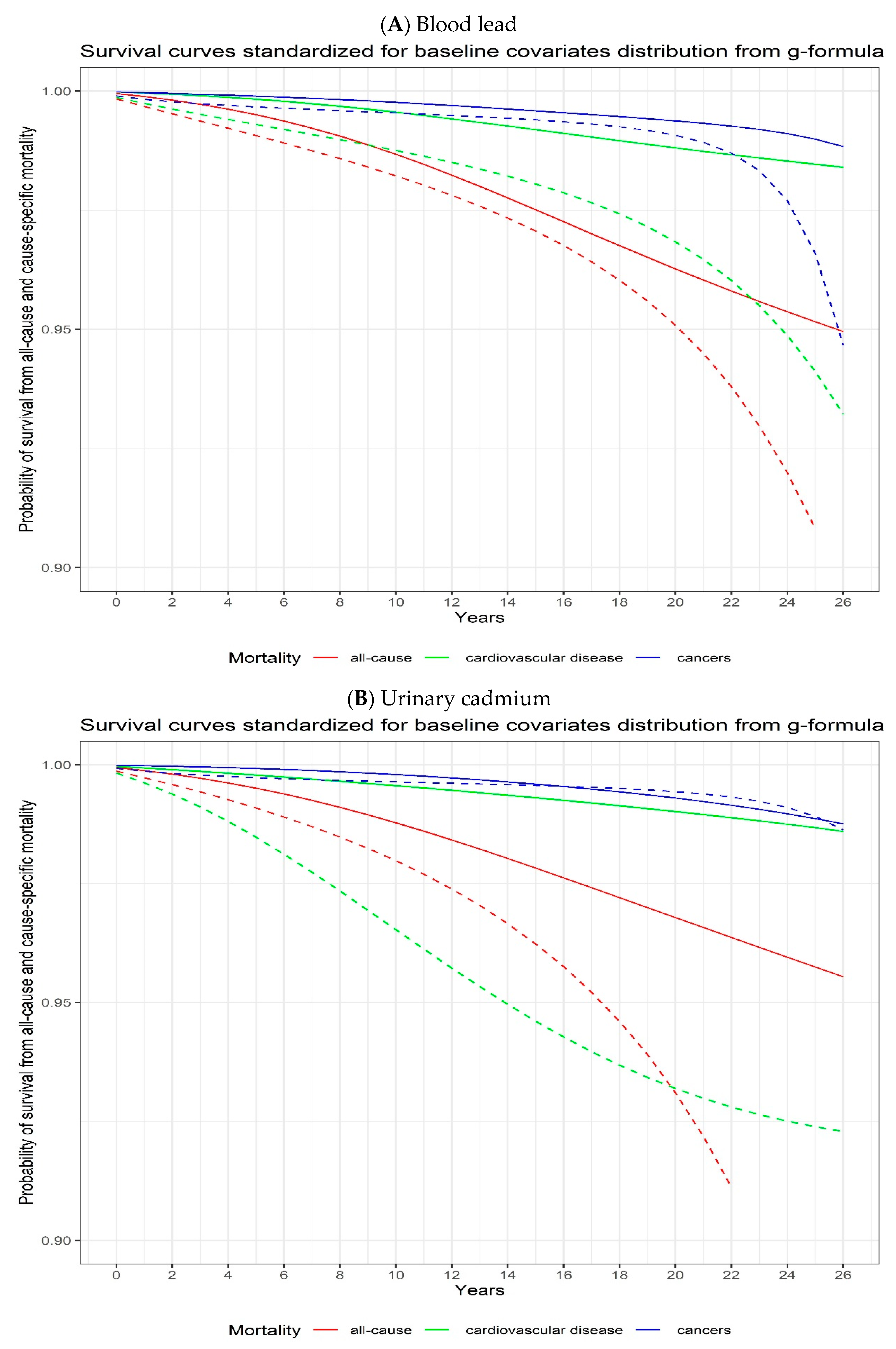
3.1. Blood Lead and Urinary Cadmium Concentrations and All-Cause and Cause-Specific Mortality
3.2. Analyses Stratified by Sex and Age
3.3. Sensitivity Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. NCD Mortality and Morbidity. Available online: https://www.who.int/teams/surveillance-of-noncommunicable-diseases/about/ncds (accessed on 6 November 2021).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Parra-Soto, S.; Cowley, E.S.; Rezende, L.F.M.; Ferreccio, C.; Mathers, J.C.; Pell, J.P.; Ho, F.K.; Celis-Morales, C. Associations of six adiposity-related markers with incidence and mortality from 24 cancers-findings from the UK Biobank prospective cohort study. BMC Med. 2021, 19, 7. [Google Scholar] [CrossRef]
- Zhang, Y.B.; Pan, X.F.; Chen, J.; Cao, A.; Xia, L.; Zhang, Y.; Wang, J.; Li, H.; Liu, G.; Pan, A. Combined lifestyle factors, all-cause mortality and cardiovascular disease: A systematic review and meta-analysis of prospective cohort studies. J. Epidemiol. Community Health 2021, 75, 92–99. [Google Scholar] [CrossRef]
- Ekblom-Bak, E.; Halldin, M.; Vikstrom, M.; Stenling, A.; Gigante, B.; de Faire, U.; Leander, K.; Hellenius, M.L. Physical activity attenuates cardiovascular risk and mortality in men and women with and without the metabolic syndrome—A 20-year follow-up of a population-based cohort of 60-year-olds. Eur. J. Prev. Cardiol. 2020, 28, 1376–1385. [Google Scholar] [CrossRef] [Green Version]
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Andrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K.; et al. American Cancer Society guideline for diet and physical activity for cancer prevention. CA Cancer J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef]
- Naghshi, S.; Sadeghi, O.; Willett, W.C.; Esmaillzadeh, A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2020, 370, m2412. [Google Scholar] [CrossRef]
- Duan, W.; Xu, C.; Liu, Q.; Xu, J.; Weng, Z.; Zhang, X.; Basnet, T.B.; Dahal, M.; Gu, A. Levels of a mixture of heavy metals in blood and urine and all-cause, cardiovascular disease and cancer mortality: A population-based cohort study. Environ. Pollut. 2020, 263, 114630. [Google Scholar] [CrossRef]
- Dignam, T.; Kaufmann, R.B.; LeStourgeon, L.; Brown, M.J. Control of Lead Sources in the United States, 1970–2017: Public Health Progress and Current Challenges to Eliminating Lead Exposure. J. Public Health Manag. Pract. 2019, 25 (Suppl. 1), S13–S22. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry: Substance Priority List. Available online: https://hero.epa.gov/hero/index.cfm/reference/details/reference_id/3378161 (accessed on 5 January 2021).
- Menke, A.; Muntner, P.; Silbergeld, E.K.; Platz, E.A.; Guallar, E. Cadmium levels in urine and mortality among U.S. adults. Environ. Health Perspect. 2009, 117, 190–196. [Google Scholar] [CrossRef]
- Schober, S.E.; Mirel, L.B.; Graubard, B.I.; Brody, D.J.; Flegal, K.M. Blood lead levels and death from all causes, cardiovascular disease, and cancer: Results from the NHANES III mortality study. Environ. Health Perspect. 2006, 114, 1538–1541. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Rauch, S.; Auinger, P.; Allen, R.W.; Hornung, R.W. Low-level lead exposure and mortality in US adults: A population-based cohort study. Lancet Public Health 2018, 3, e177–e184. [Google Scholar] [CrossRef]
- Menke, A.; Muntner, P.; Batuman, V.; Silbergeld, E.K.; Guallar, E. Blood lead below 0.48 micromol/L (10 microg/dL) and mortality among US adults. Circulation 2006, 114, 1388–1394. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Wolk, A. Urinary cadmium and mortality from all causes, cancer and cardiovascular disease in the general population: Systematic review and meta-analysis of cohort studies. Int. J. Epidemiol. 2016, 45, 782–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.S.; Skaar, D.A.; Jirtle, R.L.; Hoyo, C. Epigenetics, obesity and early-life cadmium or lead exposure. Epigenomics 2017, 9, 57–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernan, M.A. The hazards of hazard ratios. Epidemiology 2010, 21, 13–15. [Google Scholar] [CrossRef] [Green Version]
- Coory, M.; Lamb, K.E.; Sorich, M. Risk-difference curves can be used to communicate time-dependent effects of adjuvant therapies for early stage cancer. J. Clin. Epidemiol. 2014, 67, 966–972. [Google Scholar] [CrossRef]
- (NCHS)—National Center for Health Statistics. NCHS Data Linked to NDI Mortality Files; NCHS: Hyattsville, MD, USA, 2016.
- National Center for Health Statistics. NHANES I Epidemiologic Follow-Up Survey (NHEFS): Calibration Sample for NDI Matching Methodology; NCHS: Washington, DC, USA, 2009.
- Gunter, E.W.; Lewis, B.G.; Koncikowski, S.M. Laboratory Procedures Used for the Third National Health and Nutrition Examination Survey (NHANES III), 1988–1994; Centers for Disease Control and Prevention: Atlanta, GA, USA, 1996.
- Pruszkowska, E.; Carnrick, G.R.; Slavin, W. Direct determination of cadmium in urine with use of a stabilized temperature platform furnace and Zeeman background correction. Clin. Chem. 1983, 29, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laouali, N.; Mancini, F.R.; Hajji-Louati, M.; El Fatouhi, D.; Balkau, B.; Boutron-Ruault, M.C.; Bonnet, F.; Fagherazzi, G. Dietary inflammatory index and type 2 diabetes risk in a prospective cohort of 70,991 women followed for 20 years: The mediating role of BMI. Diabetologia 2019, 62, 2222–2232. [Google Scholar] [CrossRef]
- Robins, J. A new approach to causal inference in mortality studies with a sustained exposure period—Application to control of the healthy worker survivor effect. Math. Model. 1986, 17, 1393–1512. [Google Scholar] [CrossRef] [Green Version]
- Hernan, M.A.; Robins, J.M. Estimating causal effects from epidemiological data. J. Epidemiol. Community Health 2006, 60, 578–586. [Google Scholar] [CrossRef] [Green Version]
- Oulhote, Y.; Le Bot, B.; Poupon, J.; Lucas, J.P.; Mandin, C.; Etchevers, A.; Zmirou-Navier, D.; Glorennec, P. Identification of sources of lead exposure in French children by lead isotope analysis: A cross-sectional study. Environ. Health 2011, 10, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breskin, A.; Edmonds, A.; Cole, S.R.; Westreich, D.; Cocohoba, J.; Cohen, M.H.; Kassaye, S.G.; Metsch, L.R.; Sharma, A.; Williams, M.S.; et al. G-computation for policy-relevant effects of interventions on time-to-event outcomes. Int. J. Epidemiol. 2021, 49, 2021–2029. [Google Scholar] [CrossRef] [PubMed]
- Keil, A.P.; Edwards, J.K.; Richardson, D.B.; Naimi, A.I.; Cole, S.R. The parametric g-formula for time-to-event data: Intuition and a worked example. Epidemiology 2014, 25, 889–897. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Hubbard, A.; Galea, S. Estimating the effects of potential public health interventions on population disease burden: A step-by-step illustration of causal inference methods. Am. J. Epidemiol. 2009, 169, 1140–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herndon, J.E., 2nd; Harrell, F.E., Jr. The restricted cubic spline as baseline hazard in the proportional hazards model with step function time-dependent covariables. Stat. Med. 1995, 14, 2119–2129. [Google Scholar] [CrossRef]
- Kaufman, J.S.; MacLehose, R.F. Which of these things is not like the others? Cancer 2013, 119, 4216–4222. [Google Scholar] [CrossRef]
- Korn, E.L.; Graubard, B.I. Epidemiologic studies utilizing surveys: Accounting for the sampling design. Am. J. Public Health 1991, 81, 1166–1173. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Hernandez, A.; Navas-Acien, A.; Pastor-Barriuso, R.; Crainiceanu, C.M.; Redon, J.; Guallar, E.; Tellez-Plaza, M. Declining exposures to lead and cadmium contribute to explaining the reduction of cardiovascular mortality in the US population, 1988–2004. Int. J. Epidemiol. 2017, 46, 1903–1912. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Nishijo, M.; Morikawa, Y.; Miura, K.; Tawara, K.; Kuriwaki, J.; Kido, T.; Ikawa, A.; Kobayashi, E.; Nogawa, K. Urinary cadmium and mortality among inhabitants of a cadmium-polluted area in Japan. Environ. Res. 2006, 100, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Nawrot, T.S.; Van Hecke, E.; Thijs, L.; Richart, T.; Kuznetsova, T.; Jin, Y.; Vangronsveld, J.; Roels, H.A.; Staessen, J.A. Cadmium-related mortality and long-term secular trends in the cadmium body burden of an environmentally exposed population. Environ. Health Perspect. 2008, 116, 1620–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tellez-Plaza, M.; Navas-Acien, A.; Menke, A.; Crainiceanu, C.M.; Pastor-Barriuso, R.; Guallar, E. Cadmium exposure and all-cause and cardiovascular mortality in the U.S. general population. Environ. Health Perspect. 2012, 120, 1017–1022. [Google Scholar] [CrossRef]
- Tellez-Plaza, M.; Guallar, E.; Howard, B.V.; Umans, J.G.; Francesconi, K.A.; Goessler, W.; Silbergeld, E.K.; Devereux, R.B.; Navas-Acien, A. Cadmium exposure and incident cardiovascular disease. Epidemiology 2013, 24, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Suwazono, Y.; Nogawa, K.; Morikawa, Y.; Nishijo, M.; Kobayashi, E.; Kido, T.; Nakagawa, H.; Nogawa, K. Impact of urinary cadmium on mortality in the Japanese general population in cadmium non-polluted areas. Int. J. Hyg. Environ. Health 2014, 217, 807–812. [Google Scholar] [CrossRef]
- Suwazono, Y.; Nogawa, K.; Morikawa, Y.; Nishijo, M.; Kobayashi, E.; Kido, T.; Nakagawa, H.; Nogawa, K. All-cause mortality increased by environmental cadmium exposure in the Japanese general population in cadmium non-polluted areas. J. Appl. Toxicol. 2015, 35, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Nishijo, M.; Nakagawa, H.; Morikawa, Y.; Sakurai, M.; Nakamura, K.; Kido, T.; Nogawa, K.; Dai, M. Relationship between urinary cadmium and mortality in habitants of a cadmium-polluted area: A 22-year follow-up study in Japan. Chin. Med. J. 2011, 124, 3504–3509. [Google Scholar] [PubMed]
- Lin, Y.S.; Caffrey, J.L.; Lin, J.W.; Bayliss, D.; Faramawi, M.F.; Bateson, T.F.; Sonawane, B. Increased risk of cancer mortality associated with cadmium exposures in older Americans with low zinc intake. J. Toxicol. Environ. Health A 2013, 76, 1–15. [Google Scholar] [CrossRef]
- Garcia-Esquinas, E.; Pollan, M.; Tellez-Plaza, M.; Francesconi, K.A.; Goessler, W.; Guallar, E.; Umans, J.G.; Yeh, J.; Best, L.G.; Navas-Acien, A. Cadmium exposure and cancer mortality in a prospective cohort: The strong heart study. Environ. Health Perspect. 2014, 122, 363–370. [Google Scholar] [CrossRef] [Green Version]
- (ATSDR)—Agency for Toxic Substances and Disease Registry. Toxicological Profile for Lead. Available online: https://wwwn.cdc.gov/TSP/ToxProfiles/ToxProfiles.aspx?id=96&tid=22 (accessed on 16 May 2022).
- Vaziri, N.D. Mechanisms of lead-induced hypertension and cardiovascular disease. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H454–H465. [Google Scholar] [CrossRef]
- Navas-Acien, A.; Guallar, E.; Silbergeld, E.K.; Rothenberg, S.J. Lead exposure and cardiovascular disease—A systematic review. Environ. Health Perspect. 2007, 115, 472–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Inorganic and organic lead compounds. IARC Monogr. Eval. Carcinog. Risks Hum. 2006, 87, 1–471. [Google Scholar]
- Caffo, M.; Caruso, G.; Fata, G.L.; Barresi, V.; Visalli, M.; Venza, M.; Venza, I. Heavy metals and epigenetic alterations in brain tumors. Curr. Genom. 2014, 15, 457–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silbergeld, E.K. Facilitative mechanisms of lead as a carcinogen. Mutat. Res. 2003, 533, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Knoflach, M.; Messner, B.; Shen, Y.H.; Frotschnig, S.; Liu, G.; Pfaller, K.; Wang, X.; Matosevic, B.; Willeit, J.; Kiechl, S.; et al. Non-toxic cadmium concentrations induce vascular inflammation and promote atherosclerosis. Circ. J. 2011, 75, 2491–2495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almenara, C.C.; Broseghini-Filho, G.B.; Vescovi, M.V.; Angeli, J.K.; Faria Tde, O.; Stefanon, I.; Vassallo, D.V.; Padilha, A.S. Chronic cadmium treatment promotes oxidative stress and endothelial damage in isolated rat aorta. PLoS ONE 2013, 8, e68418. [Google Scholar] [CrossRef]
- Angeli, J.K.; Cruz Pereira, C.A.; de Oliveira Faria, T.; Stefanon, I.; Padilha, A.S.; Vassallo, D.V. Cadmium exposure induces vascular injury due to endothelial oxidative stress: The role of local angiotensin II and COX-2. Free. Radic. Biol. Med. 2013, 65, 838–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caciari, T.; Sancini, A.; Fioravanti, M.; Capozzella, A.; Casale, T.; Montuori, L.; Fiaschetti, M.; Schifano, M.P.; Andreozzi, G.; Nardone, N.; et al. Cadmium and hypertension in exposed workers: A meta-analysis. Int. J. Occup. Med. Environ. Health 2013, 26, 440–456. [Google Scholar] [CrossRef]
- Fagerberg, B.; Barregard, L.; Sallsten, G.; Forsgard, N.; Ostling, G.; Persson, M.; Borne, Y.; Engstrom, G.; Hedblad, B. Cadmium exposure and atherosclerotic carotid plaques--results from the Malmo diet and Cancer study. Environ. Res. 2015, 136, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Fagerberg, B.; Bergstrom, G.; Boren, J.; Barregard, L. Cadmium exposure is accompanied by increased prevalence and future growth of atherosclerotic plaques in 64-year-old women. J. Intern. Med. 2012, 272, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Julin, B.; Wolk, A.; Thomas, L.D.; Akesson, A. Exposure to cadmium from food and risk of cardiovascular disease in men: A population-based prospective cohort study. Eur. J. Epidemiol. 2013, 28, 837–840. [Google Scholar] [CrossRef] [PubMed]
- Obeng-Gyasi, E. Chronic cadmium exposure and cardiovascular disease in adults. J. Environ. Sci. Health A 2020, 55, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Tellez-Plaza, M.; Jones, M.R.; Dominguez-Lucas, A.; Guallar, E.; Navas-Acien, A. Cadmium exposure and clinical cardiovascular disease: A systematic review. Curr. Atheroscler. Rep. 2013, 15, 356. [Google Scholar] [CrossRef] [PubMed]
- Lamas, G.A.; Ujueta, F.; Navas-Acien, A. Lead and Cadmium as Cardiovascular Risk Factors: The Burden of Proof Has Been Met. J. Am. Heart Assoc. 2021, 10, e018692. [Google Scholar] [CrossRef] [PubMed]
- Hart, B.A.; Lee, C.H.; Shukla, G.S.; Shukla, A.; Osier, M.; Eneman, J.D.; Chiu, J.F. Characterization of cadmium-induced apoptosis in rat lung epithelial cells: Evidence for the participation of oxidant stress. Toxicology 1999, 133, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Rani, A.; Kumar, A.; Lal, A.; Pant, M. Cellular mechanisms of cadmium-induced toxicity: A review. Int. J. Environ. Health Res. 2014, 24, 378–399. [Google Scholar] [CrossRef] [PubMed]
- Asara, Y.; Marchal, J.A.; Carrasco, E.; Boulaiz, H.; Solinas, G.; Bandiera, P.; Garcia, M.A.; Farace, C.; Montella, A.; Madeddu, R. Cadmium modifies the cell cycle and apoptotic profiles of human breast cancer cells treated with 5-fluorouracil. Int. J. Mol. Sci. 2013, 14, 16600–16616. [Google Scholar] [CrossRef] [PubMed]
- Pierron, F.; Baillon, L.; Sow, M.; Gotreau, S.; Gonzalez, P. Effect of low-dose cadmium exposure on DNA methylation in the endangered European eel. Environ. Sci. Technol. 2014, 48, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Stoica, A.; Katzenellenbogen, B.S.; Martin, M.B. Activation of estrogen receptor-alpha by the heavy metal cadmium. Mol. Endocrinol. 2000, 14, 545–553. [Google Scholar] [CrossRef]
- McGivern, L.; Shulman, L.; Carney, J.K.; Shapiro, S.; Bundock, E. Death Certification Errors and the Effect on Mortality Statistics. Public Health Rep. 2017, 132, 669–675. [Google Scholar] [CrossRef]
- van Woudenbergh, G.J.; Theofylaktopoulou, D.; Kuijsten, A.; Ferreira, I.; van Greevenbroek, M.M.; van der Kallen, C.J. Adapted dietary inflammatory index and its association with a summary score for low-grade inflammation and markers of glucose metabolism: The Cohort study on Diabetes and Atherosclerosis Maastricht (CODAM) and the Hoorn study. Am. J. Clin. Nutr. 2013, 98, 1533–1542. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavicchia, P.P.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Hébert, J.R. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J. Nutr. 2009, 139, 2365–2372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S; discussion 9S–31S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panizza, C.E.; Shvetsov, Y.B.; Harmon, B.E.; Wilkens, L.R.; Le Marchand, L.; Haiman, C.; Reedy, J.; Boushey, C.J. Testing the Predictive Validity of the Healthy Eating Index-2015 in the Multiethnic Cohort: Is the Score Associated with a Reduced Risk of All-Cause and Cause-Specific Mortality? Nutrients 2018, 10, 452. [Google Scholar] [CrossRef] [Green Version]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Blood Lead (μg/dL) | Urinary Cadmium (μg/g) | ||
|---|---|---|---|
| N (%) | GM (GSE) | GM (GSE) | |
| Age classes (years) | |||
| <50 | 8170 (57.09) | 2.59 (1.01) | 0.26 (1.01) |
| ≥50 | 6141 (42.91) | 3.56 (1.01) | 0.56 (1.01) |
| Sex | |||
| Women | 7570 (52.90) | 2.26 (1.01) | 0.42 (1.01) |
| Men | 6741 (47.10) | 4.03 (1.01) | 0.31 (1.01) |
| Ethnicity | |||
| Mexican-American | 3891 (27.19) | 2.99 (1.01) | 0.31 (1.02) |
| Other Hispanic | 369 (2.58) | 2.88 (1.04) | 0.32 (1.07) |
| Non-Hispanic | 10,051 (70.23) | 2.96 (1.01) | 0.39 (1.01) |
| Smoking status | |||
| Never smoker | 6807 (47.7) | 2.37 (1.01) | 0.27 (1.01) |
| Current smoker | 4477 (31.28) | 3.86 (1.01) | 0.48 (1.02) |
| Former smoker | 3027 (21.15) | 3.32 (1.01) | 0.46 (1.02) |
| Body-mass index | |||
| Normal weight (<25·0 kg/m2) | 5707 (39.88) | 2.91 (1.01) | 0.34 (1.02) |
| Overweight (25·0–29·9 kg/m2) | 4855 (33.92) | 3.18 (1.01) | 0.38 (1.02) |
| Obese (≥30·0 kg/m2) | 3749 (26.20) | 2.80 (1.01) | 0.38 (1.02) |
| Physical activity (per month) | |||
| None | 2939 (20.54) | 3.14 (1.01) | 0.44 (1.02) |
| One to 14 times | 5099 (35.63) | 2.89 (1.01) | 0.37 (1.02) |
| 15 or more times | 6273 (43.83) | 2.95 (1.01) | 0.32 (1.02) |
| Poverty to income ratio tertile | |||
| First | 4776 (33.37) | 3.21 (1.01) | 0.38 (1.02) |
| Second | 4765 (33.30) | 2.85 (1.01) | 0.36 (1.02) |
| Third | 4770 (33.33) | 2.85 (1.01) | 0.35 (1.02) |
| Alcohol intake (drinks per month) | |||
| Four or fewer | 9940 (69.46) | 2.72 (1.01) | 0.38 (1.01) |
| More than four | 4371 (30.54) | 3.63 (1.01) | 0.33 (1.02) |
| Healthy eating index tertile | |||
| First | 4765 (33.30) | 3.23 (1.01) | 0.36 (1.02) |
| Second | 4774 (33.36) | 2.91 (1.01) | 0.35 (1.02) |
| Third | 4772 (33.34) | 2.78 (1.01) | 0.38 (1.02) |
| Adapted dietary inflammatory index tertile | |||
| First | 4770 (0.33) | 2.79 (1.01) | 0.34 (1.02) |
| Second | 4771 (0.33) | 2.95 (1.01) | 0.35 (1.02) |
| Third | 4770 (0.33) | 3.17 (1.01) | 0.40 (1.02) |
| Outcomes | Blood Lead | Urinary Cadmium |
|---|---|---|
| All-cause Mortality | ||
| Number of events (%) among low level before the intervention | 177/1217 (14.5%) | 122/682 (17.9%) |
| Number of events (%) among high level before the intervention | 4767/13,603 (35.0%) | 4645/13,598 (34.2%) |
| Adjusted risk ratio (95% CI) | 2.38 (1.14 to 2.96) | 2.26 (1.77 to 4.83) |
| Adjusted risk difference (95% CI) | +4.17% (1.54 to 8.77) | +6.22% (4.51 to 12.00) |
| Cardiovascular disease mortality | ||
| Number of events (%) among low level before the intervention | 35/1217 (2.9%) | 30/682 (4.4%) |
| Number of events (%) among high level before the intervention | 1423/13,603 (10.5%) | 1405/13,598 (10.3%) |
| Adjusted risk ratio (95% CI) | 2.09 (1.04 to 3.68) | 1.37 (0.80 to 3.39) |
| Adjusted risk difference (95% CI) | +1.52% (0.09 to 3.74) | +1.06% (−0.57 to 3.50) |
| Cancer mortality | ||
| Number of events (%) among low level before the intervention | 49/1217 (4.0%) | 22/682 (3.2%) |
| Number of events (%) among high level before the intervention | 1027/13,603 (7.6%) | 1007/13,598 (7.4%) |
| Adjusted risk ratio (95% CI) | 3.87 (1.12 to 7.91) | 2.44 (0.66 to 3.81) |
| Adjusted risk difference (95% CI) | +1.32% (−0.09 to 3.67) | +0.64% (−0.98 to 2.80) |
| Outcomes | Blood Lead | Urinary Cadmium |
|---|---|---|
| All-cause mortality | ||
| Number of events (%) among quartile 1 before the intervention | 695/3640 (19.1%) | 504/3578 (14.1%) |
| Number of events (%) among quartile 4 before the intervention | 1877/3564 (52.7%) | 2157/3578 (60.3%) |
| Adjusted risk ratio (95% CI) | 1.61 (1.12 to 3.34) | 2.09 (1.75 to 5.42) |
| Adjusted risk difference (95% CI) | +5.52% (1.25 to 18.25) | +10.48% (5.15 to 27.99) |
| Cardiovascular disease mortality | ||
| Number of events (%) among quartile 1 before the intervention | 168/3640 (4.6%) | 123/3578 (3.4%) |
| Number of events (%) among quartile 4 before the intervention | 589/3564 (16.5%) | 631/3578 (17.6%) |
| Adjusted risk ratio (95% CI) | 3.38 (1.29 to 25.66) | 7.18 (3.12 to 78.03) |
| Adjusted risk difference (95% CI) | +5.18% (0.47 to 48.61) | +6.31% (3.76 to 50.38) |
| Cancer mortality | ||
| Number of events (%) among quartile 1 before the intervention | 172/3640 (4.7%) | 98/3578 (2.7%) |
| Number of events (%) among quartile 4 before the intervention | 431/3564 (12.1%) | 544/3578 (15.2%) |
| Adjusted risk ratio (95% CI) | 2.44 (1.01 to 13.48) | 2.08 (0.42 to 40.73) |
| Adjusted risk difference (95% CI) | +4.17% (−0.28 to 26.00) | +0.13% (−1.57 to 48.35) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laouali, N.; Benmarhnia, T.; Lanphear, B.P.; Oulhote, Y. Associations with Blood Lead and Urinary Cadmium Concentrations in Relation to Mortality in the US Population: A Causal Survival Analysis with G-Computation. Toxics 2023, 11, 133. https://doi.org/10.3390/toxics11020133
Laouali N, Benmarhnia T, Lanphear BP, Oulhote Y. Associations with Blood Lead and Urinary Cadmium Concentrations in Relation to Mortality in the US Population: A Causal Survival Analysis with G-Computation. Toxics. 2023; 11(2):133. https://doi.org/10.3390/toxics11020133
Chicago/Turabian StyleLaouali, Nasser, Tarik Benmarhnia, Bruce P. Lanphear, and Youssef Oulhote. 2023. "Associations with Blood Lead and Urinary Cadmium Concentrations in Relation to Mortality in the US Population: A Causal Survival Analysis with G-Computation" Toxics 11, no. 2: 133. https://doi.org/10.3390/toxics11020133