
Risk of Mortality from Respiratory Malignant and Non-Malignant Diseases among Talc Miners and Millers: A Systematic Review and Meta-Analysis
 , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
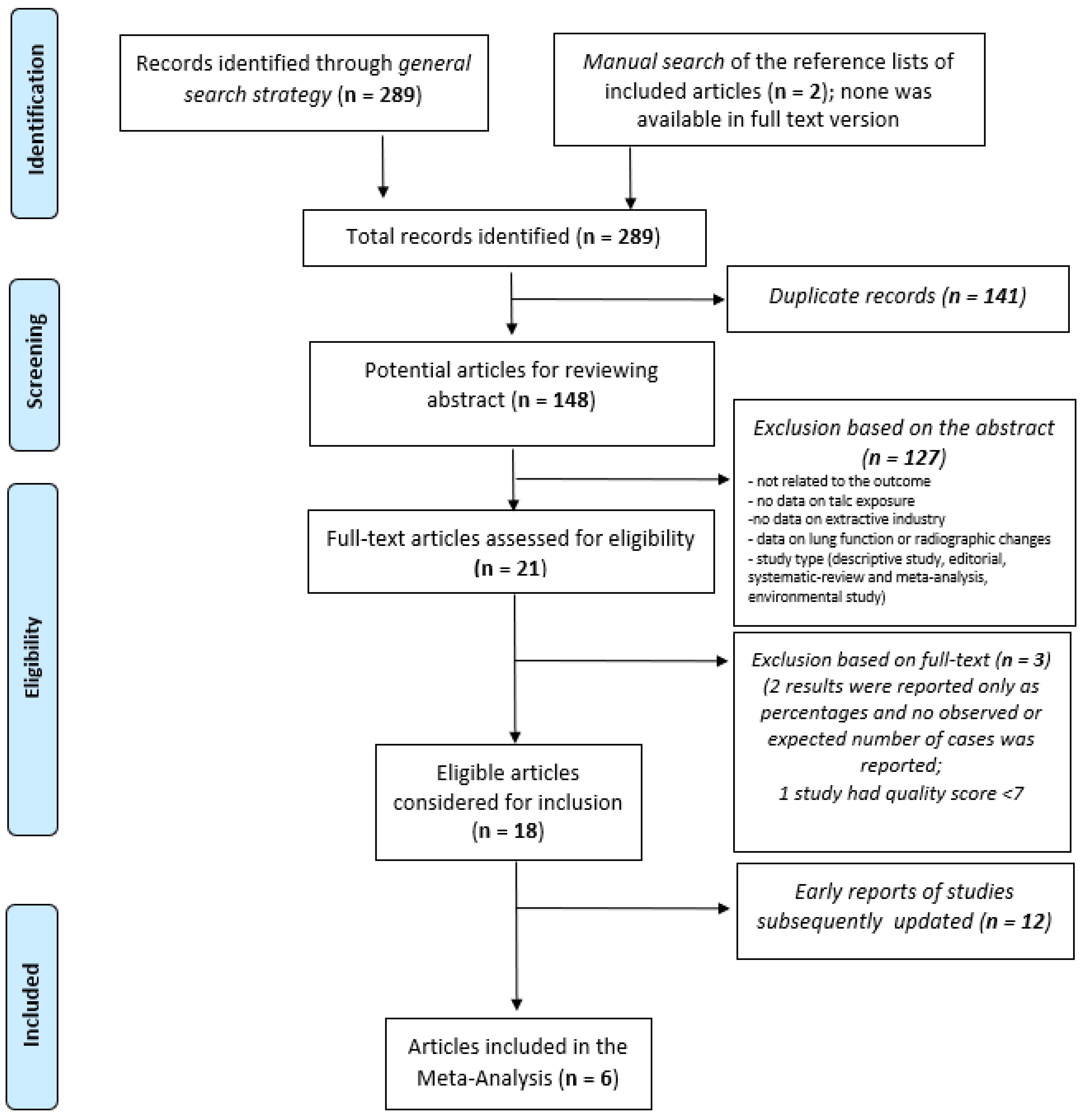
2.1. Search Strategy
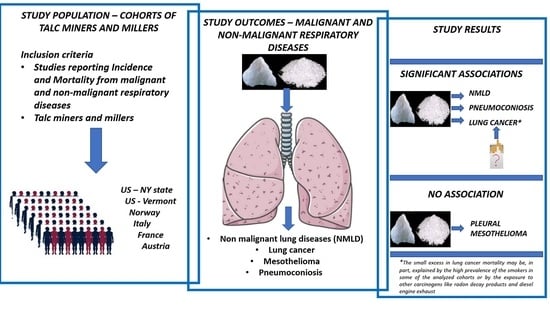
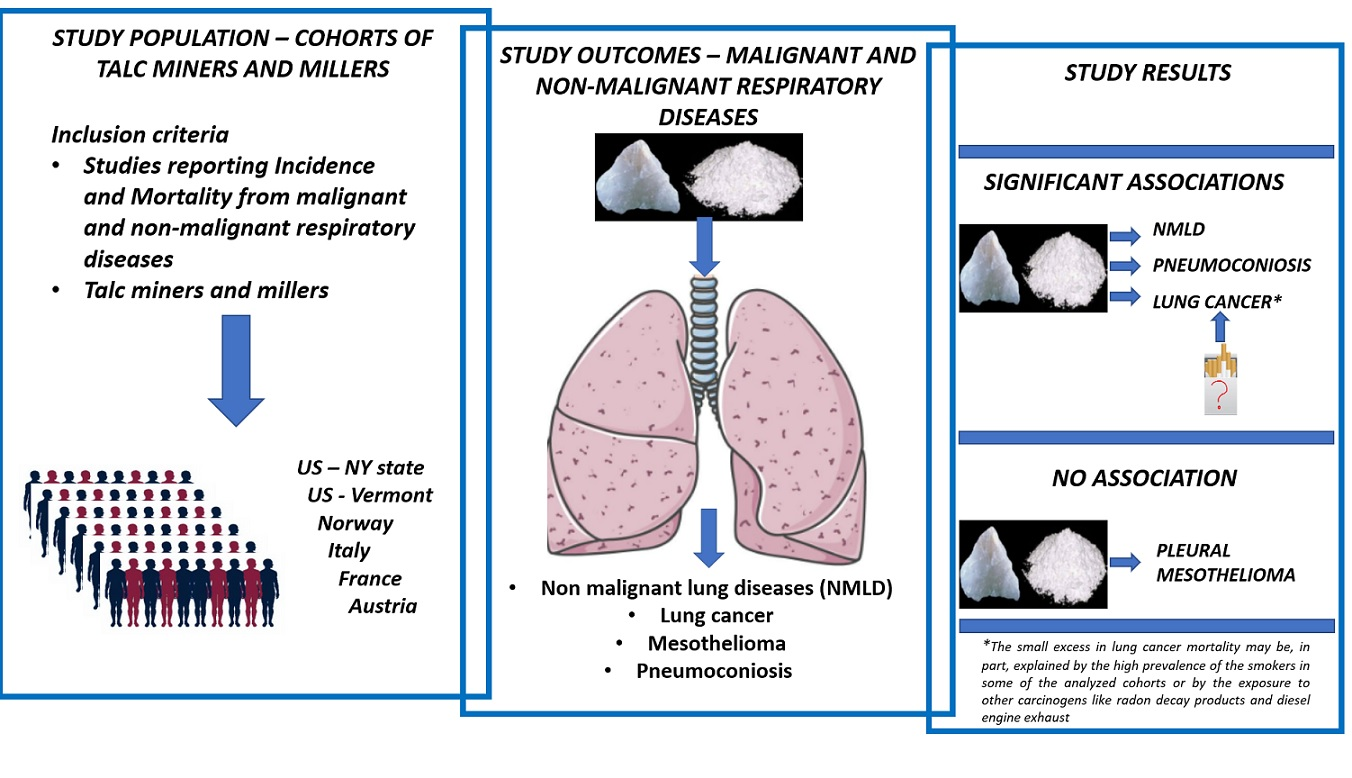
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Meta-Analysis Statistical Method
3. Results
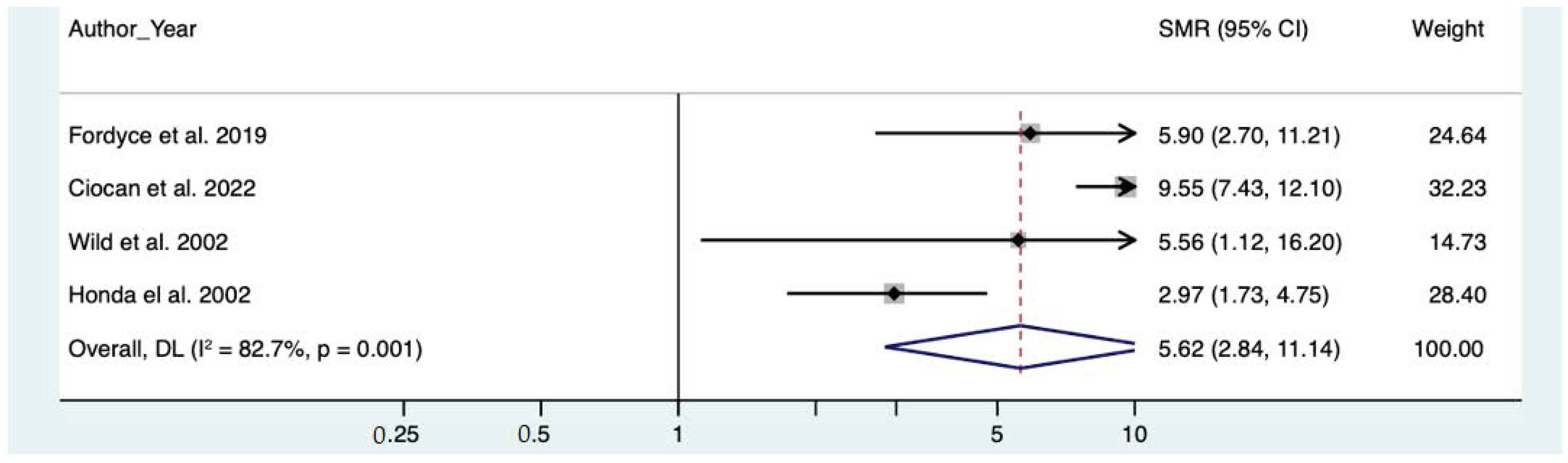
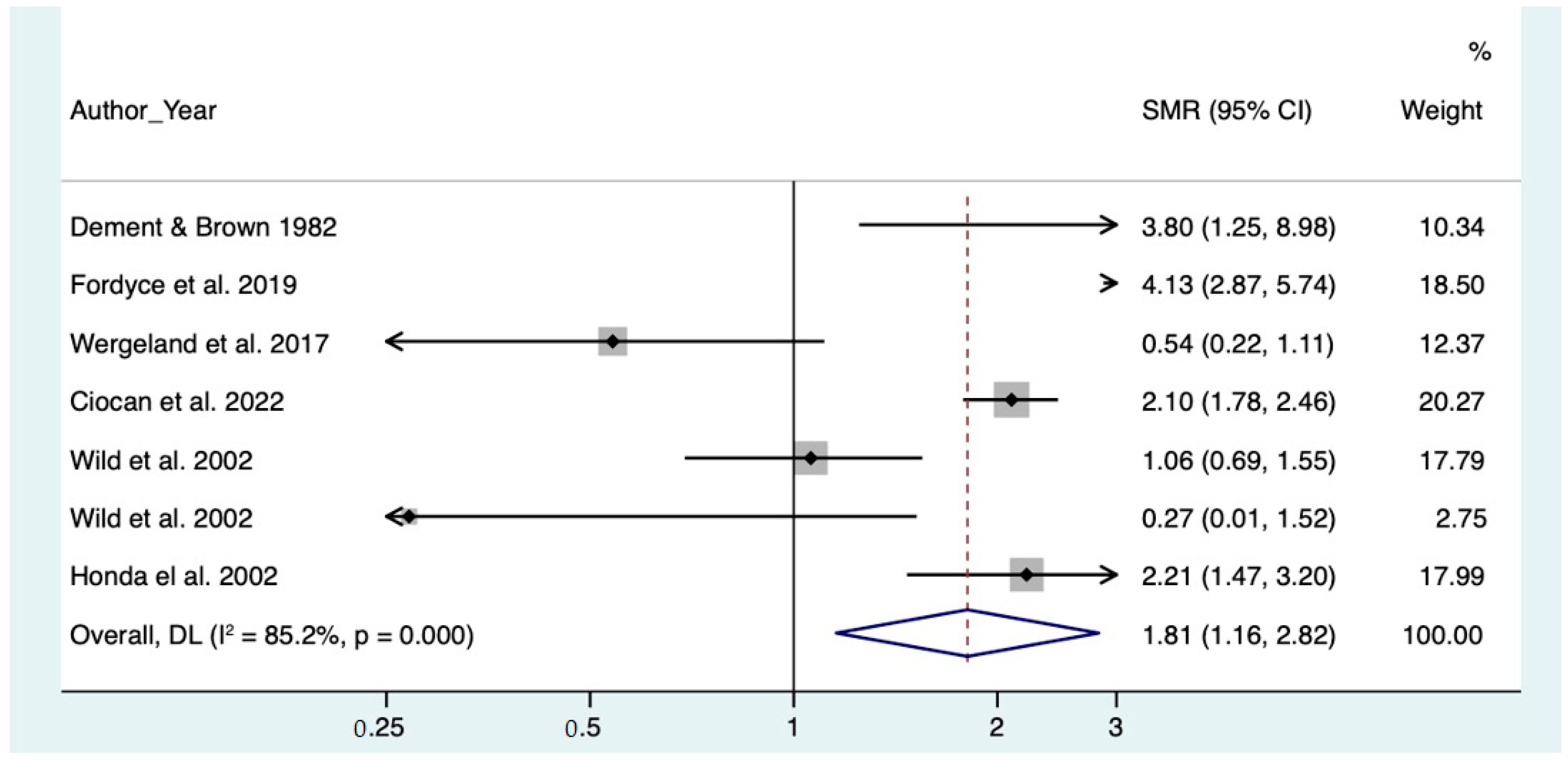
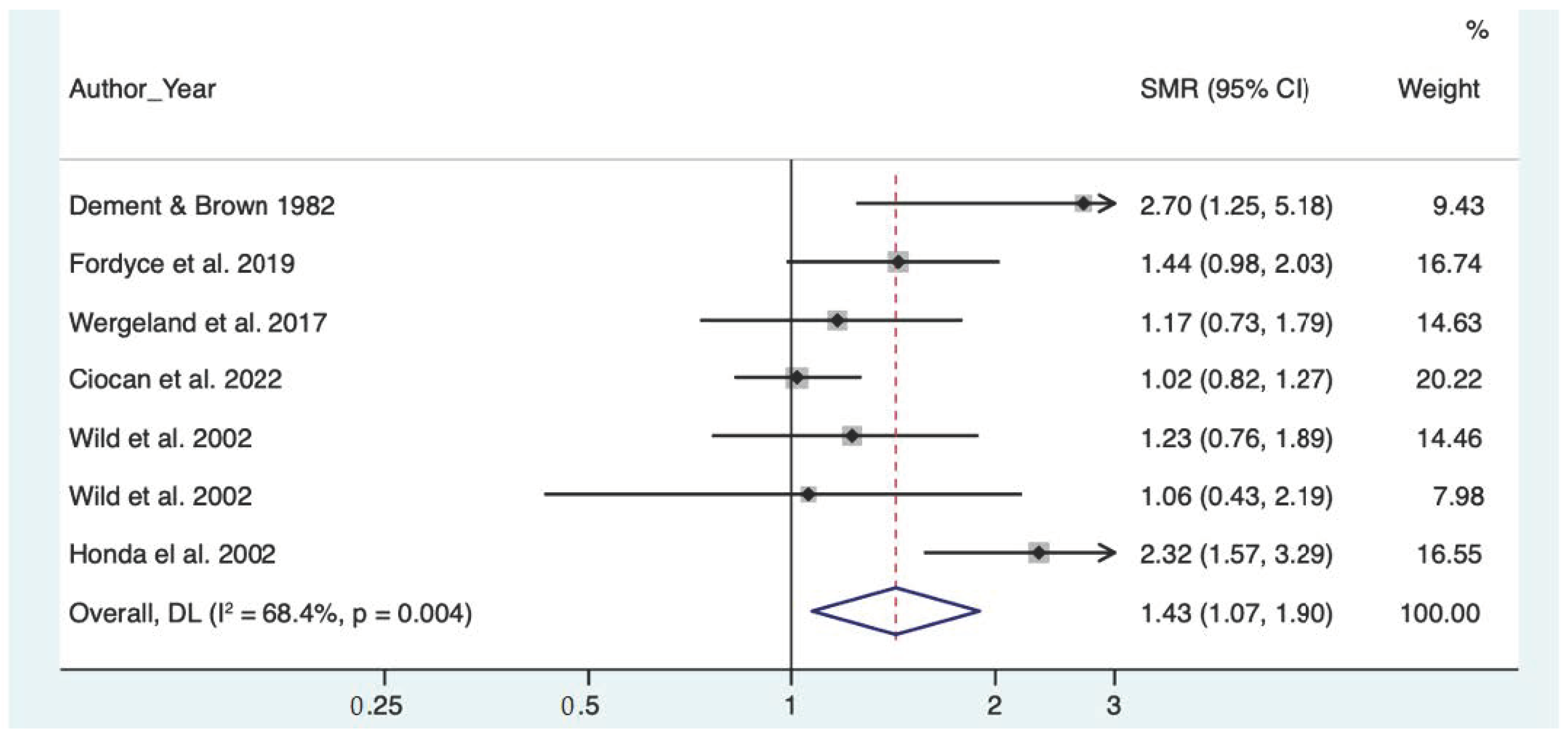
Meta-Analysis
4. Discussion
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. Silica. In Silica, Some Silicates, Coal, Dust, and Para-Aramid Fibrils. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 1997; Volume 68, pp. 42–242. [Google Scholar]
- International Agency for Research on Cancer. Talc. In Carbon Black, Titanium Dioxide and Talc. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2010; Volume 93, pp. 277–413. [Google Scholar]
- Thorel, C. Talcosis of the lung: A contribution to the pathological anatomy of pneumoconiosis. Beitr. Pathol. Anat. Allgem. Pathol. 1896, 20, 85–101. [Google Scholar]
- Porro, F.W.; Patton, J.R.; Hobbs, A.A. Pneumoconiosis in the talc industry. Amer. J. Roentgen. 1942, 47, 507. [Google Scholar]
- Siegal, W.; Smith, A.R.; Greenburg, L. The dust hazard in tremolite talc mining, including roentgenological findings in talc workers. Amer. J. Roentgen. 1943, 49, 11. [Google Scholar]
- Kleinfeld, M.; Messite, J.; Tabershaw, I.R. Talc pneumoconiosis. Arch. Ind. Health 1955, 12, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Wild, P. Lung cancer risk and talc not containing asbestiform fibers: A review of the epidemiological evidence. Occup. Environ. Med. 2006, 63, 4–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubino, G.F.; Scansetti, G.; Piolatto, P.G.; Romano, C. Mortality study of talc miners and millers. J. Occup. Med. 1976, 18, 186–193. [Google Scholar] [CrossRef]
- Coggiola, M.; Bosio, D.; Pira, E.; Piolatto, P.G.; Vecchia, C.L.; Negri, E.; Michelazzi, M.; Bacaloni, A. An update of a mortality study of talc miners and millers in Italy. Am. J. Ind. Med. 2003, 44, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Pira, E.; Coggiola, M.; Ciocan, C.; Romano, C.; La Vecchia, C.; Pelucchi, C.; Boffetta, P. Mortality of talc miners and millers from Val Chisone, northern Italy: An updated cohort study. J. Occup. Environ. Med. 2017, 59, 659–664. [Google Scholar] [CrossRef]
- Ciocan, C.; Pira, E.; Coggiola, M.; Franco, N.; Godono, A.; La Vecchia, C.; Negri, E.; Boffetta, P. Mortality in the cohort of talc miners and millers from Val Chisone, Northern Italy: 74 years of follow-up. Environ. Res. 2022, 203, 11865. [Google Scholar] [CrossRef]
- Fordyce, T.A.; Leonhard, M.J.; Mowat, F.S.; Moolgavkar, S.H. A 37-year Update on Mortality Patterns in an Expanded Cohort of Vermont Talc Miners and Millers. J. Occup. Environ. Med. Nov. 2019, 61, 916–923. [Google Scholar] [CrossRef]
- Wild, P.; Leodolter, K.; Refregier, M.; Schmidt, H.; Zidek, T.; Haidinger, G. A cohort mortality and nested case-control study of French and Austrian talc workers. Occup. Environ. Med. 2002, 59, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selevan, S.G.; Dement, J.M.; Wagoner, J.K.; Froines, J.R. Mortality patterns among miners and millers of non-asbestiform talc: Preliminary report. J. Environ Pathol. Toxicol. 1979, 2, 273–284. [Google Scholar] [PubMed]
- Wergeland, E.; Andersen, A.; Barheim, A. Morbidity and mortality in talc-exposed workers. Am. J. Ind. Med. 1990, 17, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.J.; Tu, Y.K.; Chen, P.C.; Yang, H.Y. Occupational exposure to talc increases the risk of lung cancer: A meta-analysis of occupational cohort studies. Can. Res. J. 2017, 1270608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, T.L.; Stewart, P.A. Mortality from lung cancer and respiratory disease among pottery workers exposed to silica and talc. Am. J. Epidemiol. 1987, 125, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Whitlock, E. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- NIH National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 20 July 2022).
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials Revisited. Contemp. Clin. Trials 2015, 122, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Brit. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Leophonte, P.; Basset, M.P.; Pincemin, J.; Louis, A.; Pernet, P.; Delaude, A. Mortalite´des travailleurs du talc en France. Rev. Fr. Mal. Resp. 1983, 11, 489–490. [Google Scholar]
- Fu, J.; Zhang, Y.F. Epidemiological studies of lung cancer in talc workers. Ind. Health Occup. Dis. 1992, 18, 160–163. [Google Scholar]
- Dement, J.M.; Zumwalde, R.D.; Gamble, J.F. Occupational Exposure to Talc Containing Asbestos: Morbidity, Mortality, and Environmental Studies of Miners and Millers; National Institute for Occupational Safety and Health (NIOSH) Publication No. 80-115; Public Health Service, Center for Disease Control; U.S. Department of Health and Welfare (DHEW); National Institute for Occupational Safety and Health (NIOSH): Cincinnati, OH, USA, 1980.
- Honda, Y.; Beall, C.; Delzell, E.; Oestenstad, K.; Brill, I.; Matthews, R. Mortality among workers at a talc mining and milling facility. Ann. Occup. Hyg. 2002, 46, 575–585. [Google Scholar] [PubMed] [Green Version]
- Lamm, S.H.; Levine, M.S.; Starr, J.A.; Tirey, S.L. Analysis of excess lung cancer risk in short-term employees. Am. J. Epidemiol. 1988, 127, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- Alashkar Alhamwe, B.; Alhamdan, F.; Ruhl, A.; Potaczek, D.P.; Renz, H. The role of epigenetics in allergy and asthma development. Curr. Opin. Allergy Clin. Immunol. 2020, 20, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Emi, T.; Rivera, L.M.; Tripathi, V.C.; Yano, N.; Ragavendran, A.; Wallace, J.; Fedulov, A.V. Transcriptomic and epigenomic effects of insoluble particles on J774 macrophages. Epigenetics 2021, 16, 1053–1070. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Marsh, G.M. Absence of mesothelioma risk maintained in an expanded international cohort of cosmetic talc miners and millers. Inhal. Toxicol. 2020, 32, 257–264. [Google Scholar] [CrossRef]
- Pira, E.; Coggiola, M.; Ciocan, C.; Romano, C.; La Vecchia, C.; Pelucchi, C.; Boffetta, P. Response to Letter to the Editor on the Mortality of Talc Miners and Millers from Val Chisone, Northern Italy. J. Occup. Environ. Med. 2017, 59, e195. [Google Scholar] [CrossRef]
- Wild, P.; Réfrégier, M.; Auburtin, G.; Carton, B.; Moulin, J.J. Survey of the respiratory health of the workers of a talc producing factory. Occup. Environ. Med. 1995, 52, 470–477. [Google Scholar] [CrossRef]
- Katsnelson, B.A.; Mokronosova, K.A. Non-Fibrous Mineral Dust and Malignant Tumors: An Epidemiological Study of Mortality. J. Occup. Med. 1979, 21, 15–20. [Google Scholar]
- Oestenstad, K.; Honda, Y.; Delzell, E.; Brill, I. Assessment of historical exposures to talc at a mining and milling facility. Ann. Occup. Hyg. 2002, 46, 587–596. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s), Year | Total Dust (mppcf or mg/m3) and Time Period | Free Silica Exposure Level | Presence of Asbestos |
|---|---|---|---|
| Dement J.M. et al., 1980 [25] | 0.25–2.96 mg/m3 (time period not stated) | 0.04 mg/m3 | fibrous tremolite and anthophyllite |
| Fordyce T.A. et al., 2019 [12] | not available | <1 | no |
| Wergeland E. et al., 1990 [15] | 0.94–318.9 mg/m3 (1980–1982) | 3–6% during drilling operations (after 1981) | only trace amounts of tremolite and anthophyllite |
| Ciocan C. et al., 2022 [11] | 0.8–790 mppcf (before 1965) <10 mppcf (1965–2003) 0.5–2.5 mg/m3 (after 2003) | 10% of total dust (before 1974) 2% of total dust (1978) <1% (after 2003) | No |
| Honda et al., 2002 [26] | 0.01–2.67 mg/m3 | not stated | no |
| Wild P. et al., 2002 (France) [13] | 0.5 mg/m3–15 mg/m3 (1986–1991) | <3% of total dust | no |
| Wild P. et al., 2002 (Austria) [13] | 6.14 mg/m3 | 0.5–4% of total dust | 0.25 fibers/cm3 (in the PM < 10 µm sample) 0.12 fibers/cm3 (in the PM < 2 µm sample) Analyses by polarized light microscopy indicated the presence of asbestiform tremolite, chrysotile, and anthophyllite in these samples. |
| Author(s), Year | Smokers’ Prevalence (%) | Sample Size and Smokers Prevalence |
| Dement J.M. et al., 1980 [25] | 48–79% | 121 subjects, 48% smokers and 31% ex smokers (data from Dement, 1982) |
| Fordyce T.A. et al., 2019 [12] | 64–99% | 22 cases of lung cancer, 91% smokers and 9% ex smokers 66 controls, 64% smokers and 9% ex smokers (data from Gamble 1993) |
| Wergeland E. et al., 1990 [15] | 70–76% | 94 miners, 76% smokers 296 millers, 70% smokers |
| Ciocan C. et al., 2022 [11] | 45–51% | in 1993, 200 workers, 45% smokers in 2010, 52 workers, 51% smokers (data from Pira, 2017) |
| Honda et al., 2002 [26] | 73% | 818 workers, 73% smokers |
| Wild P. et al., 2002 [13] | 42–59% | Austrian cohort: 542 workers, in 1988, 42% smokers French cohort: 1070 workers, in 1989, 59% smokers |
| Author(s), Year | Country | Study Design | Follow-Up Period | The First Year of Employment | Presence of Asbestos | No. of Subjects | Diagnostic Evidence | Outcome Studied | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|
| Dement J.M. et al., 1980 [25] | US | cohort | 28 | 1947 | Yes | 398 | Death certificate | Mortality | 11 |
| Fordyce T.A. et al., 2019 [12] | US | cohort | 72 | 1930 | No | 200 | Death certificate | Mortality | 10 |
| Wergeland E. et al., 1990 [15] | Norway | cohort | 58 | 1953 | only in traces | 390 | Cancer register | Mortality | 11 |
| Ciocan C. et al., 2022 [11] | Italy | cohort | 74 | 1946 | No | 1749 | Death certificate | Mortality | 12 |
| Honda et al., 2002 [26] | US | cohort | 39 | 1948 | No | 809 | Death certificate | Mortality | 12 |
| Wild P. et al., 2002 [13] | Austria | cohort-nested case-control | 50 | 1972 | No | 542 | Death certificate | Mortality | 11 |
| Subgroup Items | SMR Pooled Results (95% CI) Non-Malignant Lung Diseases | SMR Pooled Results (95% CI) Malignant Lung Diseases | SMR Pooled Results (95% CI) Malignant Pleural Diseases | SMR Pooled Results (95% CI) Pneumoconiosis |
|---|---|---|---|---|
| all cohort | 1.80 (1.15–2.82) | 1.42 (1.07–1.89) | insufficient data to perform analysis | 5.62 (2.83–11.14) |
| silica > 1% | 2.29 (1.51–3.47) | 1.56 (0.60–4.02) | - | 9.55 (7.48–12.18) |
| silica < 1% | 1.13 (0.37–3.42) | 1.27 (1.01–1.60) | - | 5.82 (3.10–10.91) |
| Subgroup Items | SMR Pooled Results (95% CI) Non-Malignant Lung Diseases | SMR Pooled Results (95% CI) Malignant Lung Diseases | SMR Pooled Results (95% CI) Malignant Pleural Diseases | SMR Pooled Results (95% CI) Pneumoconiosis |
|---|---|---|---|---|
| Miners | 2.82 (2.02–3.95) | 1.55 (0.75–3.19) | 1.00 (0.18–5.51) | 7.90 (2.76–22.58) |
| Millers | 1.52 (0.69–3.35) | 1.18 (0.91–1.52) | - | 2.64 (1.40–4.96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciocan, C.; Godono, A.; Stefanin, S.; Boffetta, P.; Pira, E.; Clari, M. Risk of Mortality from Respiratory Malignant and Non-Malignant Diseases among Talc Miners and Millers: A Systematic Review and Meta-Analysis. Toxics 2022, 10, 589. https://doi.org/10.3390/toxics10100589
Ciocan C, Godono A, Stefanin S, Boffetta P, Pira E, Clari M. Risk of Mortality from Respiratory Malignant and Non-Malignant Diseases among Talc Miners and Millers: A Systematic Review and Meta-Analysis. Toxics. 2022; 10(10):589. https://doi.org/10.3390/toxics10100589
Chicago/Turabian StyleCiocan, Catalina, Alessandro Godono, Sandro Stefanin, Paolo Boffetta, Enrico Pira, and Marco Clari. 2022. "Risk of Mortality from Respiratory Malignant and Non-Malignant Diseases among Talc Miners and Millers: A Systematic Review and Meta-Analysis" Toxics 10, no. 10: 589. https://doi.org/10.3390/toxics10100589