
Evidence Linking Cadmium Exposure and β2-Microglobulin to Increased Risk of Hypertension in Diabetes Type 2
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment of Study Subjects
2.2. Blood and Urine Sampling and Analysis
2.3. Determinarion of Blood and Urinary Concentration of Cadmium
2.4. Normalization of the Excretion of Cadmium and β2Microglobulin
2.5. Computation of the Estimated Glomerular Filtration Rate
2.6. Statistical Analysis
3. Results
3.1. Study Subjects
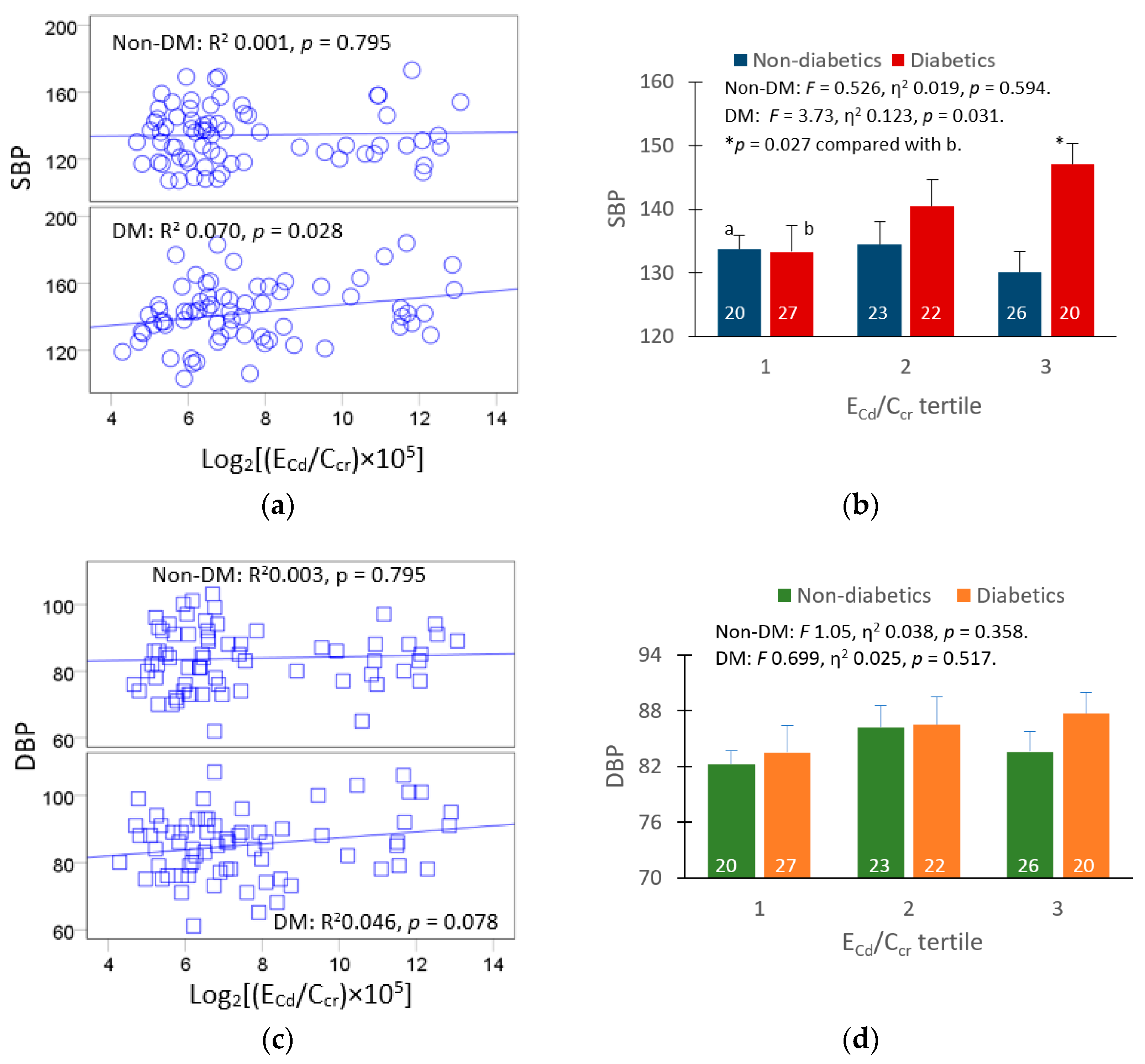
3.2. Urinary Cd and Serum β2M as the Predictors of Blood Pressure Measures
3.3. Age and Serum β2M as Predictors of eGFR Decline
3.4. An Association of Blood Cadmium and Increased Risk of Hypertension
3.5. Determinants of Blood Cadmium in Men and Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horowitz, B.; Miskulin, D.; Zager, P. Epidemiology of Hypertension in CKD. Adv. Chronic Kidney Dis. 2015, 22, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Fryar, C.D.; Ostchega, Y.; Hales, C.; Zhang, G.; Kruszon-Moran, D. Hypertension Prevalence and Control Among Adults: United States, 2015–2016. NCHS Data Brief 2017, 289, 1–8. [Google Scholar]
- Bloch, M.J.; Basile, J.N. Review of Recent Literature in Hypertension: Updated Clinical Practice Guidelines for Chronic Kidney Disease Now Include Albuminuria in the Classification System. J. Clin. Hypertens. 2013, 15, 865–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scinicariello, F.; Abadin, H.G.; Murray, H.E. Association of low-level blood lead and blood pressure in NHANES 1999–2006. Environ. Res. 2011, 111, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, N.; Fry, R.C.; Balakrishnan, P.; Navas-Acien, A.; Oliver-Williams, C.; Howard, A.G.; Cole, S.A.; Haack, K.; Lange, E.M.; Howard, B.V.; et al. Cadmium body burden and increased blood pressure in middle-aged American Indians: The Strong Heart Study. J. Hum. Hypertens. 2017, 31, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Kwon, J.A.; Park, E.; Kim, S.; Kim, B. Influence of serum ferritin combined with blood cadmium concentrations on blood pressure and hypertension: From the Korean National Health and Nutrition Examination Survey. Chemosphere 2022, 288, 132469. [Google Scholar] [CrossRef]
- Wu, S.; Li, L.; Ji, G.; Xing, X.; Li, J.; Ma, A.; Wei, Y.; Zhao, D.; Huang, H.; Ma, W.; et al. Association of multi-metals with the risk of hypertension and the interaction with obesity: A cross-sectional study in China. Front. Public Health 2023, 11, 1090935. [Google Scholar] [CrossRef]
- Zhong, Q.; Wu, H.-B.; Niu, Q.-S.; Jia, P.-P.; Qin, Q.-R.; Wang, X.-D.; He, J.-L.; Yang, W.-J.; Huang, F. Exposure to multiple metals and the risk of hypertension in adults: A prospective cohort study in a local area on the Yangtze River, China. Environ. Int. 2021, 153, 106538. [Google Scholar] [CrossRef]
- Garner, R.E.; Levallois, P. Associations between cadmium levels in blood and urine, blood pressure and hypertension among Canadian adults. Environ. Res. 2017, 155, 64–72. [Google Scholar] [CrossRef]
- Kaneda, M.; Wai, K.M.; Kanda, A.; Ando, M.; Murashita, K.; Nakaji, S.; Ihara, K. Low Level of Serum Cadmium in Relation to Blood Pressures Among Japanese General Population. Biol. Trace Element Res. 2021, 200, 67–75. [Google Scholar] [CrossRef]
- Boonprasert, K.; Vesey, D.A.; Gobe, G.C.; Ruenweerayut, R.; Johnson, D.W.; Na-Bangchang, K.; Satarug, S. Is renal tubular cadmium toxicity clinically relevant? Clin. Kidney J. 2018, 11, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver-Williams, C.; Howard, A.G.; Navas-Acien, A.; Howard, B.V.; Tellez-Plaza, M.; Franceschini, N. Cadmium body burden, hypertension, and changes in blood pressure over time: Results from a prospective cohort study in American Indians. J. Am. Soc. Hypertens. 2018, 12, 426–437.e9. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Baker, J.R.; Reilly, P.E.B.; Moore, M.R.; Williams, D.J. Cadmium Levels in the Lung, Liver, Kidney Cortex, and Urine Samples from Australians without Occupational Exposure to Metals. Arch. Environ. Health Int. J. 2002, 57, 69–77. [Google Scholar] [CrossRef]
- Elinder, C.G.; Lind, B.; Kjellström, T.; Linnman, L.; Friberg, L. Cadmium in kidney cortex, liver, and pancreas from Swedish autopsies. Estimation of biological half time in kidney cortex, considering calorie intake and smoking habits. Arch. Environ. Health 1976, 31, 292–302. [Google Scholar] [CrossRef]
- Barregard, L.; Sallsten, G.; Lundh, T.; Mölne, J. Low-level exposure to lead, cadmium and mercury, and histopathological findings in kidney biopsies. Environ. Res. 2022, 211, 113119. [Google Scholar] [CrossRef]
- Argyropoulos, C.P.; Chen, S.S.; Ng, Y.-H.; Roumelioti, M.-E.; Shaffi, K.; Singh, P.P.; Tzamaloukas, A.H. Rediscovering Beta-2 Microglobulin As a Biomarker across the Spectrum of Kidney Diseases. Front. Med. 2017, 4, 73. [Google Scholar] [CrossRef] [Green Version]
- Huan, T.; Meng, Q.; A Saleh, M.; E Norlander, A.; Joehanes, R.; Zhu, J.; Chen, B.H.; Zhang, B.; Johnson, A.D.; Ying, S.; et al. Integrative network analysis reveals molecular mechanisms of blood pressure regulation. Mol. Syst. Biol. 2015, 11, 799. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.R.; Hank, S.; Dale, B.L.; Himmel, L.; Zhong, X.; Smart, C.D.; Fehrenbach, D.J.; Chen, Y.; Prabakaran, N.; Tirado, B.; et al. A single nucleotide polymorphism in SH2B3/LNK promotes hypertension development and renal damage. Circ. Res. 2022, 131, 731–747. [Google Scholar] [CrossRef]
- Keefe, J.A.; Hwang, S.J.; Huan, T.; Mendelson, M.; Yao, C.; Courchesne, P.; Saleh, M.A.; Madhur, M.S.; Levy, D. Evidence for a causal role of the SH2B3-β2M axis in blood pressure regulation. Hypertension 2019, 73, 497–503. [Google Scholar] [CrossRef]
- Kudo, K.; Konta, T.; Mashima, Y.; Ichikawa, K.; Takasaki, S.; Ikeda, A.; Hoshikawa, M.; Suzuki, K.; Shibata, Y.; Watanabe, T.; et al. The association between renal tubular damage and rapid renal deterioration in the Japanese population: The Takahata study. Clin. Exp. Nephrol. 2011, 15, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Mashima, Y.; Konta, T.; Kudo, K.; Takasaki, S.; Ichikawa, K.; Suzuki, K.; Shibata, Y.; Watanabe, T.; Kato, T.; Kawata, S.; et al. Increases in urinary albumin and beta2-microglobulin are independently associated with blood pressure in the Japanese general population: The Takahata Study. Hypertens. Res. 2011, 34, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Ruangyuttikarn, W.; Nishijo, M.; Gobe, G.C.; Phelps, K.R. The Source and Pathophysiologic Significance of Excreted Cadmium. Toxics 2019, 7, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satarug, S.; Vesey, D.A.; Nishijo, M.; Ruangyuttikarn, W.; Gobe, G.C.; Phelps, K.R. The Effect of Cadmium on GFR Is Clarified by Normalization of Excretion Rates to Creatinine Clearance. Int. J. Mol. Sci. 2021, 22, 1762. [Google Scholar] [CrossRef]
- Phelps, K.R.; Gosmanova, E.O. A generic method for analysis of plasma concentrations. Clin. Nephrol. 2020, 94, 43–49. [Google Scholar] [CrossRef]
- Nishijo, M.; Satarug, S.; Honda, R.; Tsuritani, I.; Aoshima, K. The gender differences in health effects of environmental cadmium exposure and potential mechanisms. Mol. Cell. Biochem. 2004, 255, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Trzcinka-Ochocka, M.; Jakubowski, M.; Szymczak, W.; Janasik, B.; Brodzka, R. The effects of low environmental cadmium exposure on bone density. Environ. Res. 2010, 110, 286–293. [Google Scholar] [CrossRef]
- Hornung, R.W.; Reed, L.D. Estimation of Average Concentration in the Presence of Nondetectable Values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Denic, A.; Elsherbiny, H.; Rule, A.D. In-vivo techniques for determining nephron number. Curr. Opin. Nephrol. Hypertens. 2019, 28, 545–551. [Google Scholar] [CrossRef]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef] [Green Version]
- Soveri, I.; Berg, U.B.; Björk, J.; Elinder, C.-G.; Grubb, A.; Mejare, I.; Sterner, G.; Bäck, S.-E.; SBU GFR Review Group. Measuring GFR: A Systematic Review. Am. J. Kidney Dis. 2014, 64, 411–424. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- White, C.A.; Allen, C.M.; Akbari, A.; Collier, C.P.; Holland, D.C.; Day, A.G.; Knoll, G.A. Comparison of the new and traditional CKD-EPI GFR estimation equations with urinary inulin clearance: A study of equation performance. Clin. Chim. Acta 2019, 488, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Crowley, S.D.; Coffman, T.M. The inextricable role of the kidney in hypertension. J. Clin. Investig. 2014, 124, 2341–2347. [Google Scholar]
- Ohashi, N.; Isobe, S.; Ishigaki, S.; Yasuda, H. Circadian rhythm of blood pressure and the renin–angiotensin system in the kidney. Hypertens. Res. 2016, 40, 413–422. [Google Scholar] [CrossRef]
- Satarug, S.; Phelps, K.R. Cadmium Exposure and Toxicity. In Metal Toxicology Handbook; Bagchi, D., Bagchi, M., Eds.; CRC Press: Boca Raton, FL, USA, 2021; pp. 219–274. [Google Scholar]
- Colombo, M.; on behalf of the SUMMIT Investigators; Looker, H.C.; Farran, B.; Hess, S.; Groop, L.; Palmer, C.N.A.; Brosnan, M.J.; Dalton, R.N.; Wong, M.; et al. Serum kidney injury molecule 1 and β2-microglobulin perform as well as larger biomarker panels for prediction of rapid decline in renal function in type 2 diabetes. Diabetologia 2019, 62, 156–168. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Yun, K.-J.; Chun, H.; Jang, E.-H.; Han, K.-D.; Park, Y.-M.; Baek, K.-H.; Song, K.-H.; Cha, B.-Y.; Park, C.; et al. Clinical utility of serum beta-2-microglobulin as a predictor of diabetic complications in patients with type 2 diabetes without renal impairment. Diabetes Metab. 2014, 40, 459–465. [Google Scholar] [CrossRef]
- Cheung, C.-L.; Lam, K.S.L.; Cheung, B.M.Y. Serum β-2 microglobulin predicts mortality in people with diabetes. Eur. J. Endocrinol. 2013, 169, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Sears, C.G.; Eliot, M.; Raaschou-Nielsen, O.; Poulsen, A.H.; Harrington, J.M.; Howe, C.J.; James, K.A.; Roswall, N.; Overvad, K.; Tjønneland, A.; et al. Urinary cadmium and incident heart failure: A case-cohort analysis among never-smokers in Denmark. Epidemiology 2022, 33, 185–192. [Google Scholar] [CrossRef]
- Hagedoorn, I.J.M.; Gant, C.M.; Huizen, S.V.; Maatman, R.G.H.J.; Navis, G.; Bakker, S.J.L.; Laverman, G.D. Lifestyle-Related Exposure to Cadmium and Lead is Associated with Diabetic Kidney Disease. J. Clin. Med. 2020, 9, 2432. [Google Scholar] [CrossRef]
- Oosterwijk, M.M.; Hagedoorn, I.J.M.; Maatman, R.G.H.J.; Bakker, S.J.L.; Navis, G.; Laverman, G.D. Cadmium, active smoking and renal function deterioration in patients with type 2 diabetes. Nephrol. Dial. Transplant. 2023, 38, 876–883. [Google Scholar] [CrossRef]
- Islam, T.M.; Fox, C.S.; Mann, D.; Muntner, P. Age-related associations of hypertension and diabetes mellitus with chronic kidney disease. BMC Nephrol. 2009, 10, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. Kidney Cadmium Toxicity, Diabetes and High Blood Pressure: The Perfect Storm. Tohoku J. Exp. Med. 2017, 241, 65–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Parameters | All Subjects, n = 176 | Non-Diabetics, n = 88 | Diabetics, n = 88 | p |
|---|---|---|---|---|
| Age, years | 59.9 ± 9.7 | 60.4 ± 9.2 | 59.3 ± 10.2 | 0.389 |
| Duration of diabetes, years | n/a | 0 | 9.3 ± 7.6 | − |
| Fasting plasma glucose, mg/dL | 132 ± 61 | 94 ± 12 | 169 ± 68 | <0.001 |
| BMI, kg/m2 | 25.4 ± 4.7 | 24.7 ± 4.4 | 26.1 ± 5.0 | 0.024 |
| Obese a, % | 10.8 | 5.7 | 15.9 | 0.029 |
| Female, % | 80.7 | 80.7 | 80.7 | 1.0 |
| Smoker, % | 9.7 | 11.4 | 8.0 | 0.444 |
| Systolic blood pressure | 138 ± 17 | 135 ± 17 | 141 ± 17 | 0.015 |
| Diastolic blood pressure | 84 ± 9 | 84 ± 9 | 83 ± 10 | 0.515 |
| Hypertension, % | 52.0 | 44.7 | 59.1 | 0.058 |
| eGFR b, mL/min/1.73 m2 | 79.4 ± 18.0 | 79.4 ± 14.4 | 79.5 ± 21.2 | 0.519 |
| Reduced eGFR c, % | 16.5 | 11.4 | 21.6 | 0.067 |
| Plasma creatinine, mg/dL | 0.87 ± 0.24 | 0.85 ± 0.16 | 0.89 ± 0.30 | 0.834 |
| Urine creatinine, mg/dL | 89.2 ± 54.1 | 97.4 ± 52.6 | 81.0 ± 54.6 | 0.012 |
| Serum β2M, mg/L | 5.98 ± 3.41 | 4.93 ± 2.22 | 7.03 ± 4.03 | 0.002 |
| Urine β2M, µg/L | 740 ± 696 | 414 ± 362 | 1071 ± 793 | <0.001 |
| Blood Cd, µg/L | 0.59 ± 0.74 | 0.64 ± 0.85 | 0.53 ± 0.60 | 0.986 |
| Urine Cd, µg/L | 0.68 ± 1.18 | 0.66 ± 1.07 | 0.70 ± 1.29 | 0.862 |
| Normalized to Ccr (Ex/Ccr) d | ||||
| (ECd/Ccr) × 100, µg/L filtrate | 0.84 ± 1.66 | 0.86 ± 1.69 | 0.82 ± 1.64 | 0.389 |
| (Eβ2M/Ccr) × 100, µg/L filtrate | 1313 ± 2397 | 543 ± 625 | 2104 ± 3175 | <0.001 |
| Normalized to Ecr (Ex/Ecr) e | ||||
| ECd/Ecr, µg/g creatinine | 0.96 ± 1.83 | 0.99 ± 1.94 | 0.92 ± 1.73 | 0.482 |
| Eβ2M/Ecr, µg/g creatinine | 1284 ± 1747 | 633 ± 762 | 1954 ± 2178 | <0.001 |
| Independent Variables/Factors | SBP, mmHg | |||||
|---|---|---|---|---|---|---|
| All Subjects | Non-Diabetics | Diabetics | ||||
| β | p | β | p | β | p | |
| Age, years | 0.247 | 0.006 | 0.348 | 0.005 | 0.238 | 0.081 |
| BMI, kg/m2 | 0.124 | 0.149 | 0.140 | 0.257 | −0.016 | 0.901 |
| Log10 ([β2M]s) × 103), mg/L | 0.230 | 0.006 | 0.209 | 0.082 | 0.153 | 0.235 |
| Log2[(ECd/Ccr) × 105], µg/L | 0.167 | 0.042 | −0.009 | 0.939 | 0.303 | 0.012 |
| Gender | −0.119 | 0.251 | −0.080 | 0.598 | −0.094 | 0.526 |
| Smoking | −0.218 | 0.033 | −0.263 | 0.072 | −0.114 | 0.446 |
| Adjusted R2 | 0.123 | 0.001 | 0.152 | 0.011 | 0.089 | 0.065 |
| Independent Variables/Factors | DBP, mmHg | |||||
|---|---|---|---|---|---|---|
| All Subjects | Non-Diabetics | Diabetics | ||||
| β | p | β | p | β | p | |
| Age, years | −0.110 | 0.233 | −0.086 | 0.520 | −0.137 | 0.323 |
| BMI, kg/m2 | 0.041 | 0.645 | 0.112 | 0.406 | −0.072 | 0.581 |
| Log10 ([β2M]s) × 103), mg/L | 0.132 | 0.130 | 0.072 | 0.580 | 0.155 | 0.240 |
| Log2[(ECd/Ccr) × 105], µg/L | 0.172 | 0.045 | 0.117 | 0.378 | 0.223 | 0.067 |
| Gender | −0.213 | 0.052 | −0.142 | 0.391 | −0.255 | 0.096 |
| Smoking | −0.207 | 0.053 | −0.276 | 0.085 | −0.110 | 0.475 |
| Adjusted R2 | 0.042 | 0.069 | −0.022 | 0.451 | 0.044 | 0.186 |
| Independent Variables/Factors | SBP | DBP | ||||||
|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | |||||
| β | p | β | p | β | p | β | p | |
| Age, years | 0.247 | 0.006 | 0.348 | 0.005 | 0.238 | 0.081 | −0.110 | 0.233 |
| BMI, kg/m2 | 0.124 | 0.149 | 0.140 | 0.257 | −0.016 | 0.901 | 0.041 | 0.645 |
| Log10 ([β2M]s) × 103), mg/L | 0.230 | 0.006 | 0.209 | 0.082 | 0.153 | 0.235 | 0.132 | 0.130 |
| Log2[(ECd/Ccr) × 105], µg/L | 0.167 | 0.042 | −0.009 | 0.939 | 0.303 | 0.012 | 0.172 | 0.045 |
| Smoking | −0.218 | 0.033 | −0.263 | 0.072 | −0.114 | 0.446 | −0.207 | 0.053 |
| Adjusted R2 | 0.123 | 0.001 | 0.152 | 0.011 | 0.089 | 0.065 | 0.042 | 0.069 |
| Independent Variables/Factors | eGFR, mL/min/1.73 m2 | |||||
|---|---|---|---|---|---|---|
| All Subjects | Men | Women | ||||
| β | p | β | p | β | p | |
| Age, years | −0.307 | <0.001 | −0.269 | 0.265 | −0.299 | 0.002 |
| BMI, kg/m2 | 0.038 | 0.651 | −0.101 | 0.639 | 0.072 | 0.461 |
| Log10 ([β2M]s) × 103), mg/L | −0.235 | 0.004 | −0.397 | 0.093 | −0.176 | 0.059 |
| Log2[(ECd/Ccr) × 105], µg/L | −0.142 | 0.074 | 0.112 | 0.569 | −0.173 | 0.061 |
| Smoking | 0.028 | 0.777 | 0.012 | 0.956 | −0.034 | 0.712 |
| Gender | 0.083 | 0.408 | − | − | − | − |
| Hypertension | 0.035 | 0.662 | 0.00001 | 1.000 | 0.021 | 0.821 |
| Adjusted R2 | 0.191 | <0.001 | 0.150 | 0.132 | 0.158 | 0.001 |
| Independent Variables/ Factors | Hypertension | ||||
|---|---|---|---|---|---|
| β Coefficients | POR | 95% CI | p | ||
| (SE) | Lower | Upper | |||
| Age, years | 0.019 (0.019) | 1.019 | 0.982 | 1.058 | 0.318 |
| BMI, kg/m2 | 0.081 (0.040) | 1.084 | 1.003 | 1.172 | 0.042 |
| Log10 ([Cd]b) × 103), mg/L | 0.544 (0.237) | 1.723 | 1.083 | 2.741 | 0.022 |
| Log10 ([β2M]s) × 103), µg/L | 0.374 (0.700) | 1.454 | 0.369 | 5.732 | 0.593 |
| Gender | 0.653 (0.556) | 1.922 | 0.646 | 5.719 | 0.240 |
| Smoking | 1.331 (0.738) | 3.785 | 0.890 | 16.09 | 0.071 |
| Non-DM | Referent | ||||
| <10-y DM | 0.413 (0.047) | 1.512 | 0.601 | 3.802 | 0.380 |
| ≥10-y DM | 0.682 (0.0426) | 1.977 | 0.857 | 4.560 | 0.110 |
| Independent Variables/Factors | Log10([Cd]b × 103), µg/L | |||||
|---|---|---|---|---|---|---|
| All Subjects | Men | Women | ||||
| β | p | β | p | β | p | |
| Age, years | −0.066 | 0.467 | 0.129 | 0.589 | −0.101 | 0.314 |
| BMI, kg/m2 | 0.105 | 0.217 | 0.246 | 0.266 | 0.115 | 0.241 |
| eGFR, ml/min/1.73 m2 | 0.016 | 0.875 | 0.007 | 0.973 | 0.012 | 0.920 |
| Log10 ([β2M]s × 103), mg/L | 0.084 | 0.345 | −0.176 | 0.483 | 0.126 | 0.196 |
| Log10[(Eβ2M/Ccr × 103], µg/L | 0.139 | 0.225 | 0.354 | 0.166 | 0.077 | 0.555 |
| Log2[(ECd/Ccr) × 105], µg/L | 0.321 | <0.001 | 0.143 | 0.467 | 0.394 | <0.001 |
| Gender | 0.110 | 0.275 | − | − | − | − |
| Smoking | 0.294 | 0.003 | 0.496 | 0.025 | 0.097 | 0.285 |
| Diabetes | −0.175 | 0.060 | −0.511 | 0.029 | −0.079 | 0.452 |
| Hypertension | 0.143 | 0.078 | 0.164 | 0.473 | 0.181 | 0.050 |
| Adjusted R2 | 0.197 | <0.001 | 0.197 | 0.109 | 0.193 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yimthiang, S.; Pouyfung, P.; Khamphaya, T.; Vesey, D.A.; Gobe, G.C.; Satarug, S. Evidence Linking Cadmium Exposure and β2-Microglobulin to Increased Risk of Hypertension in Diabetes Type 2. Toxics 2023, 11, 516. https://doi.org/10.3390/toxics11060516
Yimthiang S, Pouyfung P, Khamphaya T, Vesey DA, Gobe GC, Satarug S. Evidence Linking Cadmium Exposure and β2-Microglobulin to Increased Risk of Hypertension in Diabetes Type 2. Toxics. 2023; 11(6):516. https://doi.org/10.3390/toxics11060516
Chicago/Turabian StyleYimthiang, Supabhorn, Phisit Pouyfung, Tanaporn Khamphaya, David A. Vesey, Glenda C. Gobe, and Soisungwan Satarug. 2023. "Evidence Linking Cadmium Exposure and β2-Microglobulin to Increased Risk of Hypertension in Diabetes Type 2" Toxics 11, no. 6: 516. https://doi.org/10.3390/toxics11060516