
Treatment of Multiple RT1 Gingival Recessions Using a Coronally Advanced Flap Associated with L-PRF or Subgingival Connective Tissue Graft from Maxillary Tuberosity: A Randomized, Controlled Clinical Trial
 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
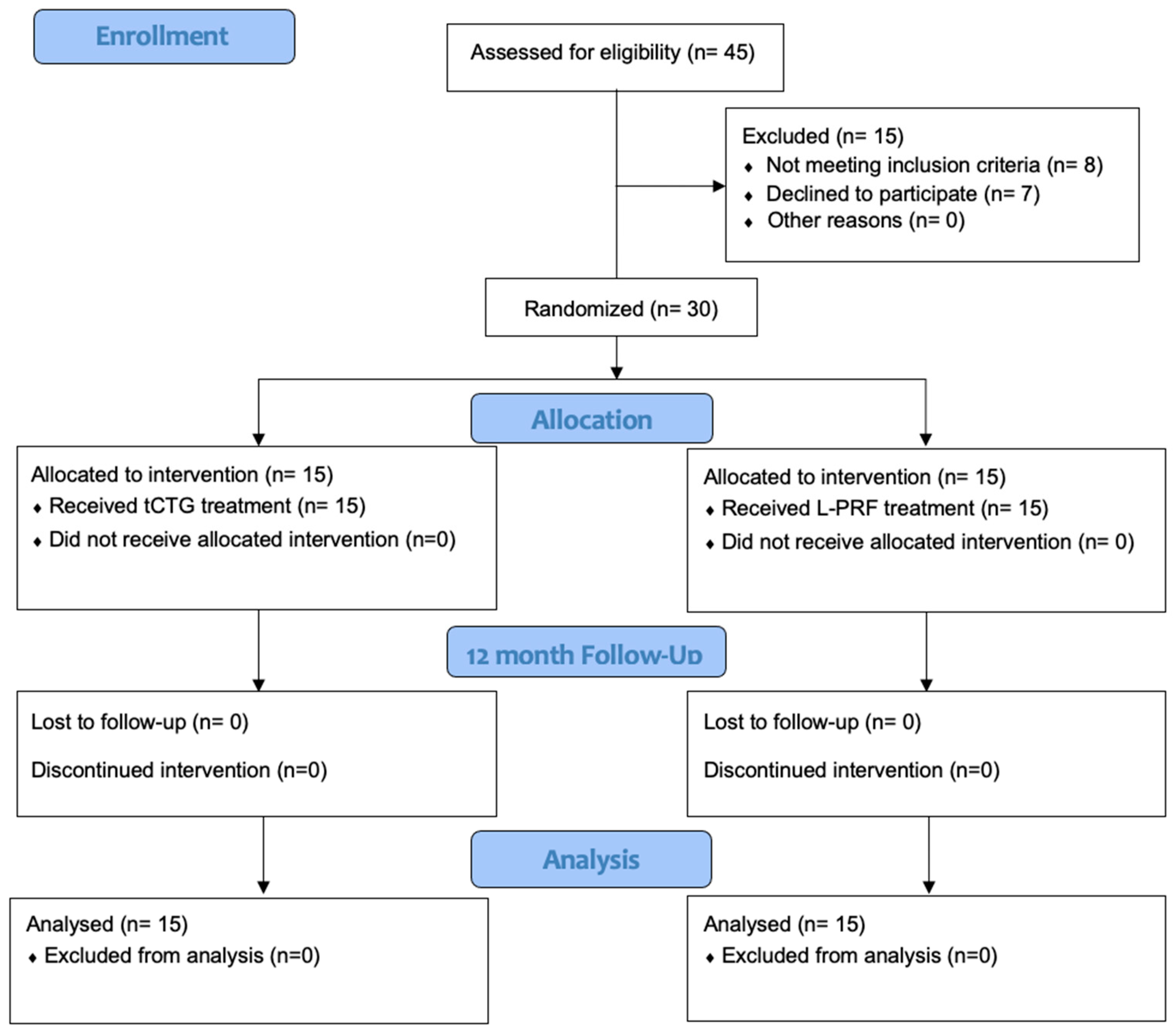
2.1. Study Design and Population
2.2. Sample Size and Randomization
2.3. Clinical Measurements
2.4. Patient-Reported Outcomes
2.5. Esthetic Outcome
2.6. Clinical Procedure
2.6.1. Pre-Surgical Treatment
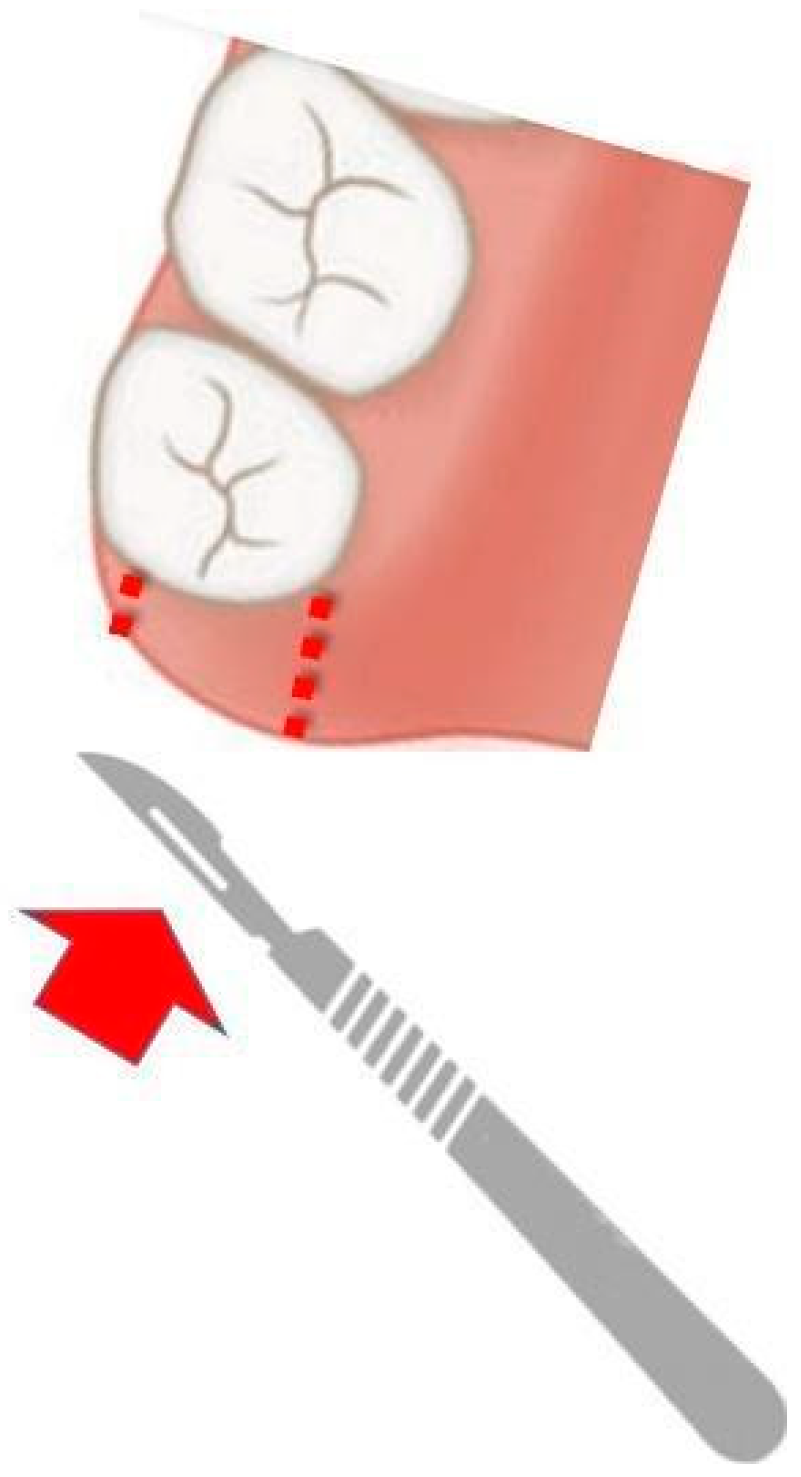
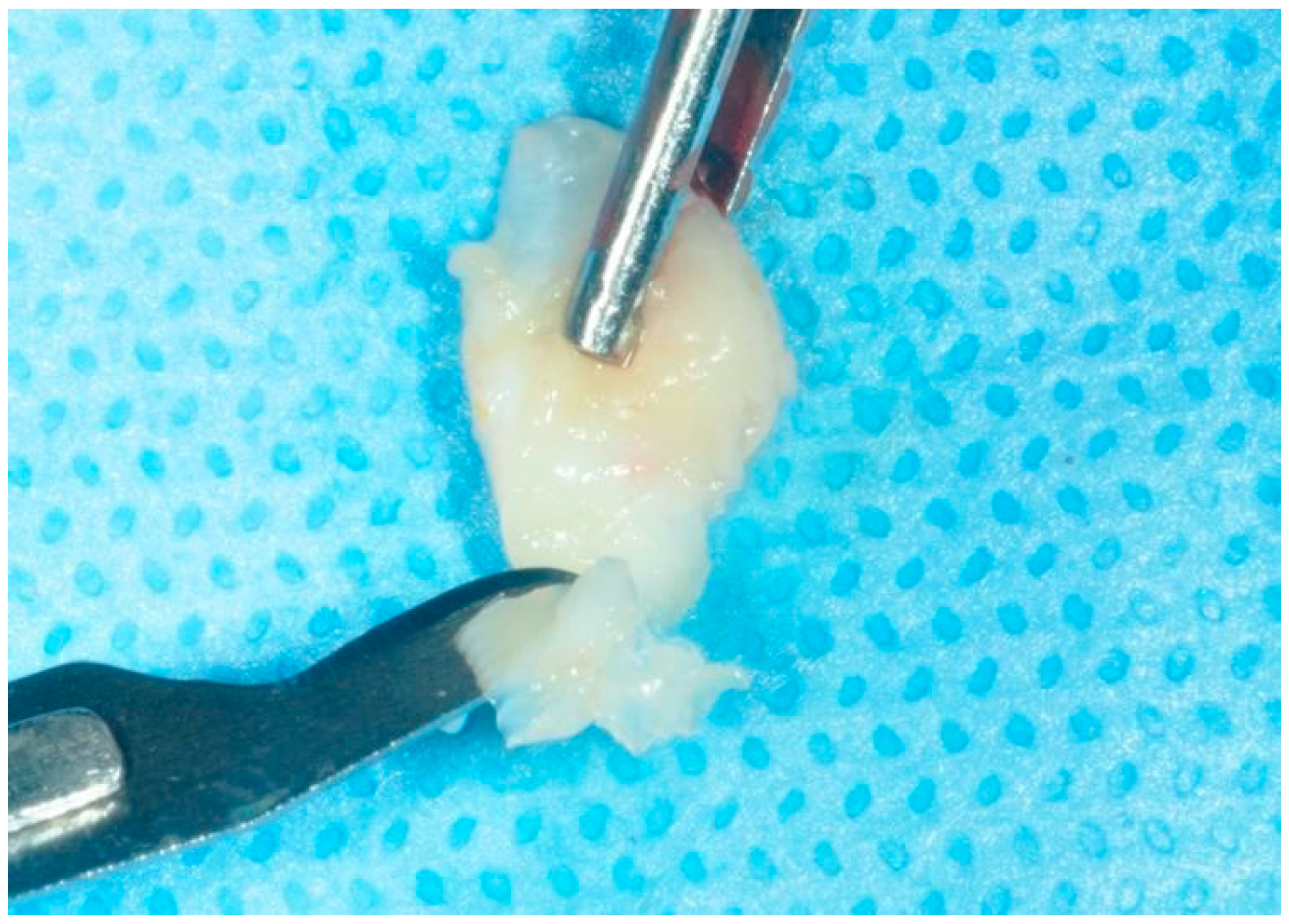
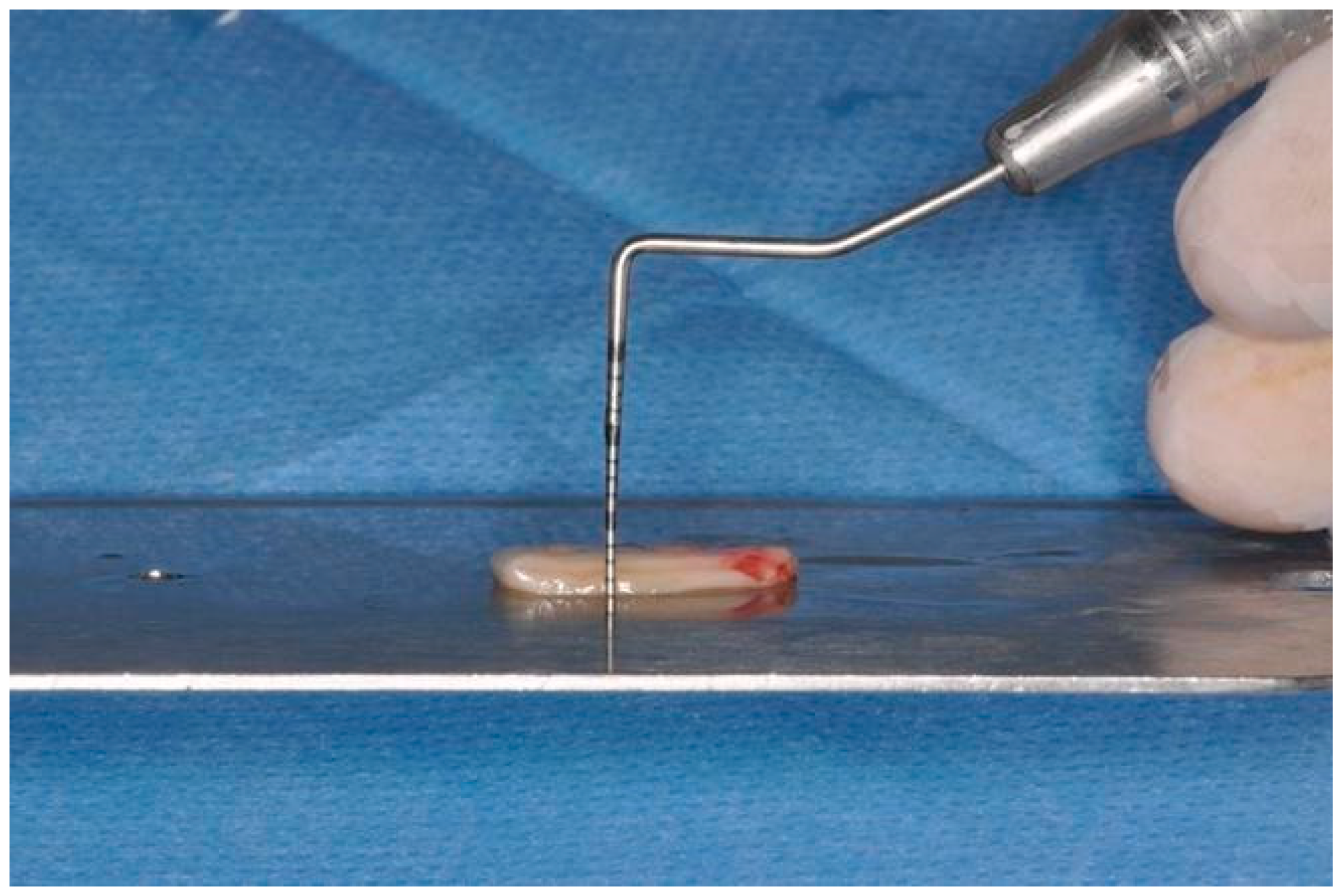
2.6.2. tCTG Preparation
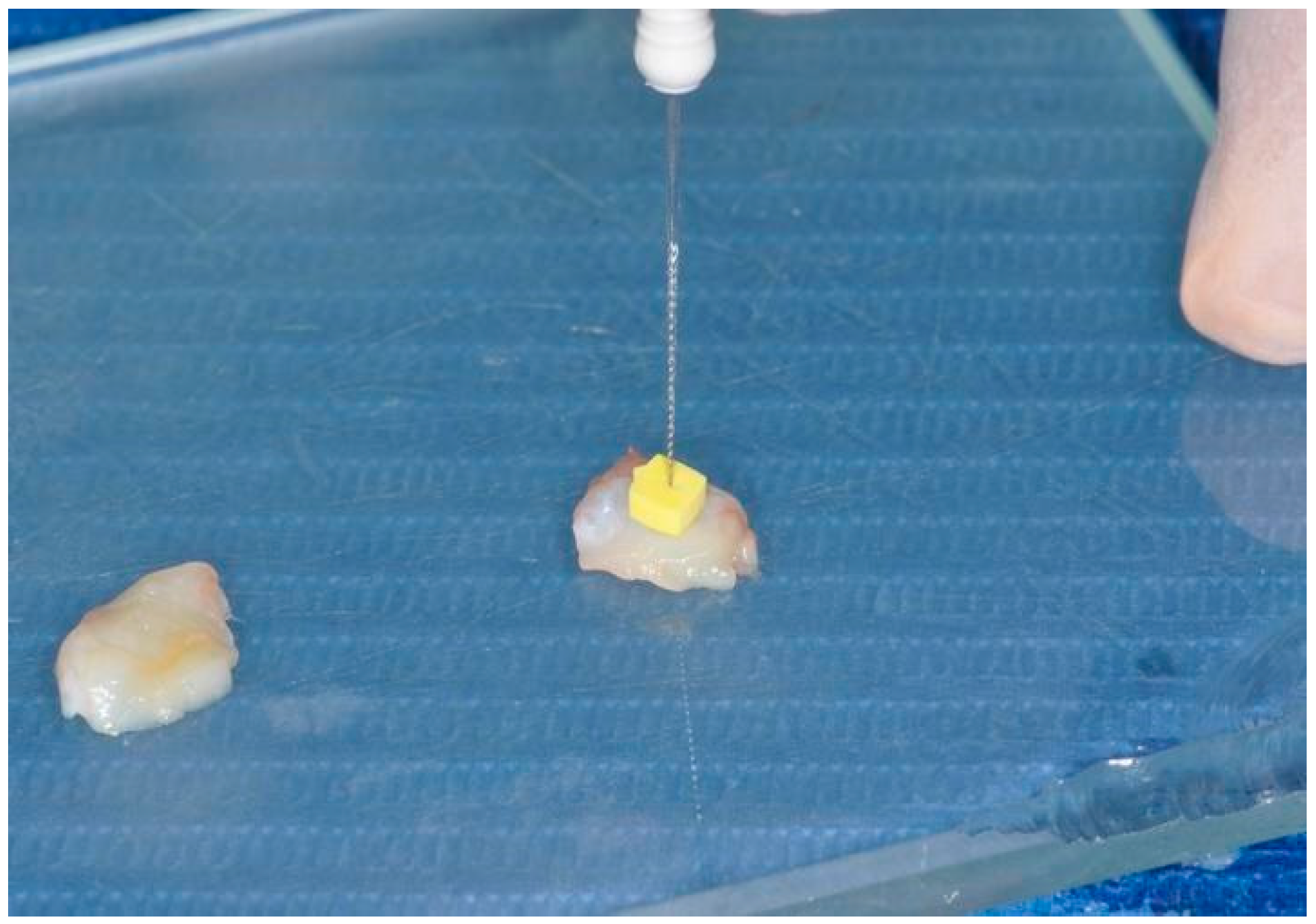
2.6.3. L-PRF Preparation
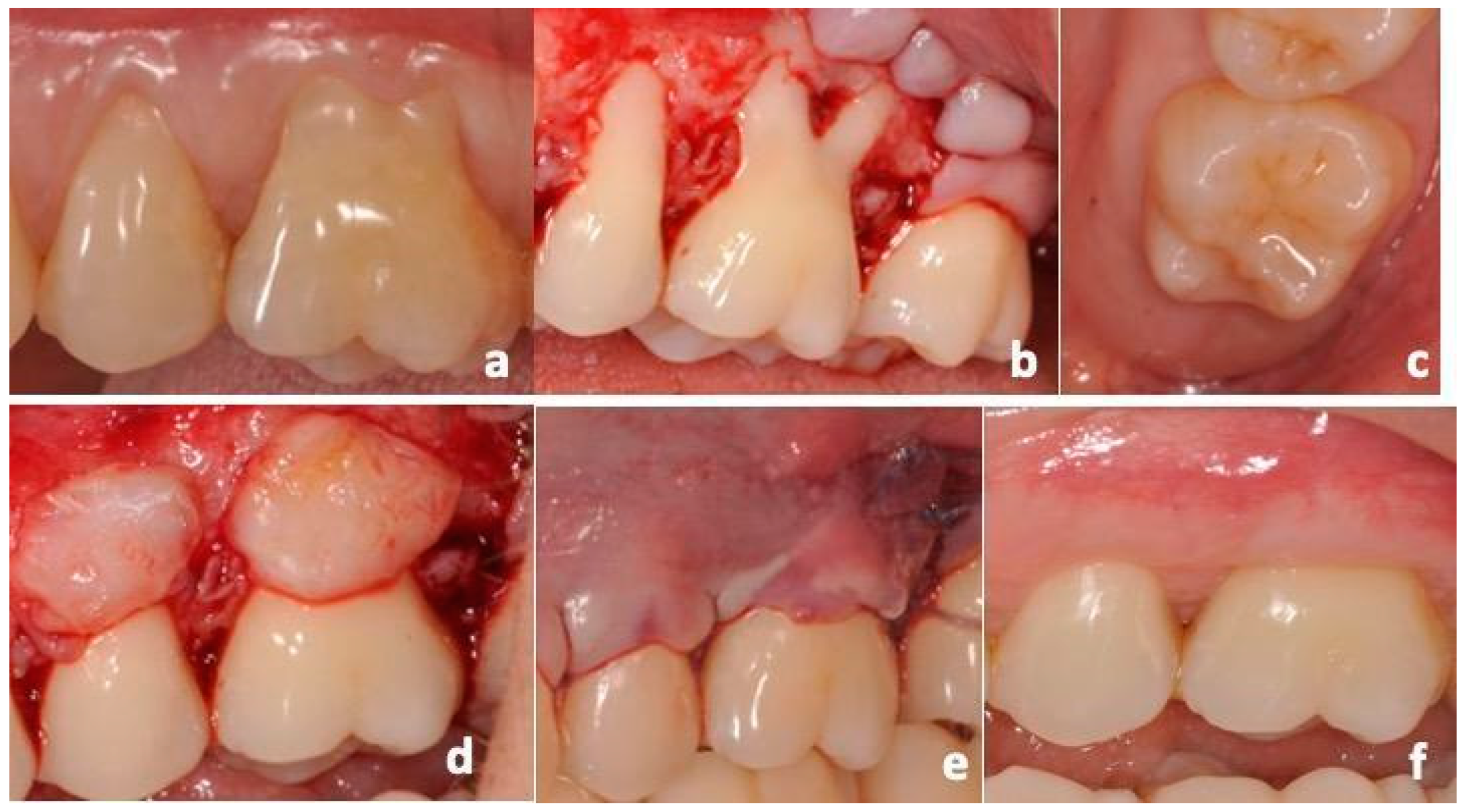
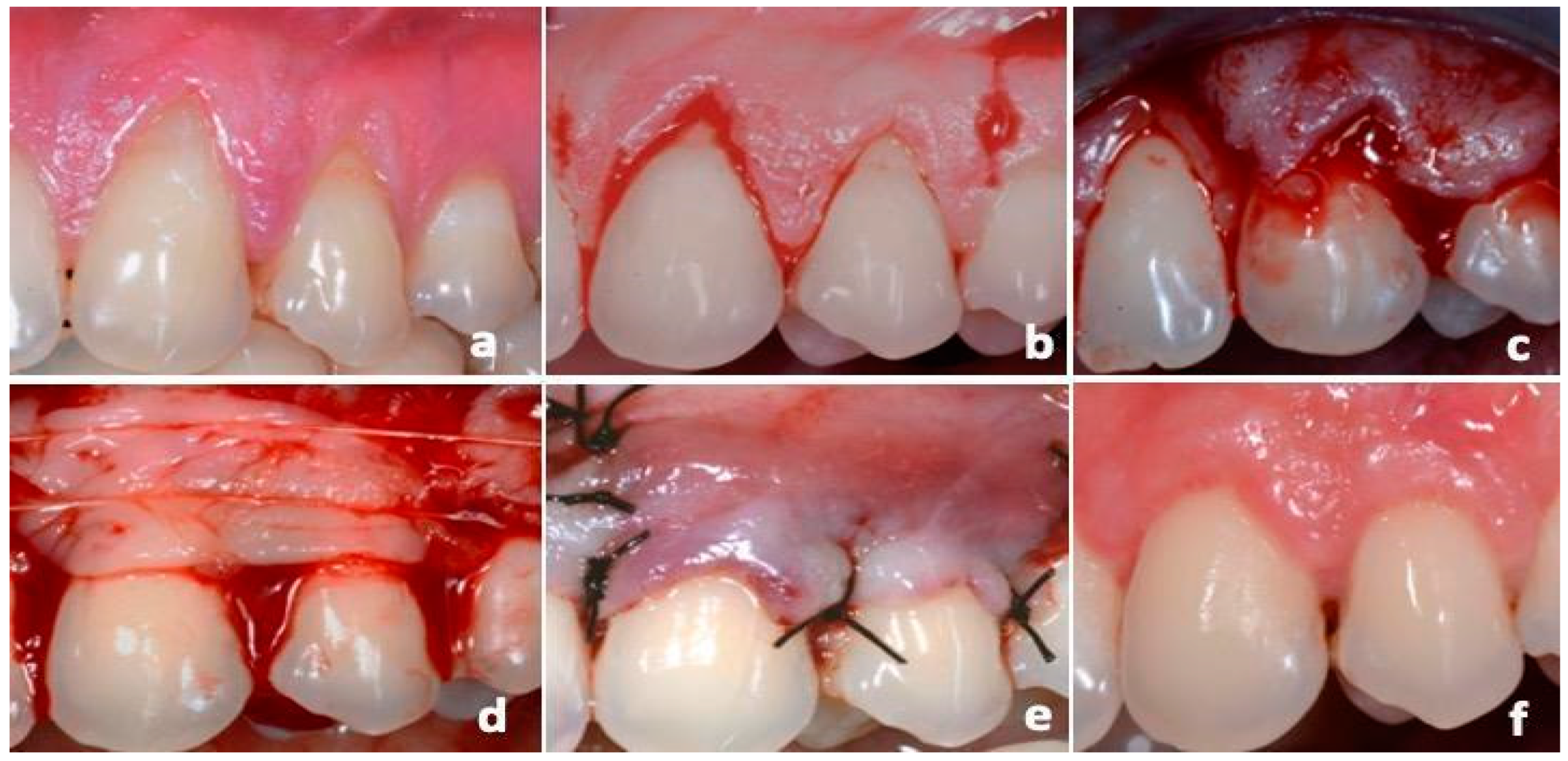
2.6.4. CAF Procedures
2.7. Postoperative Care
3. Statistical Analysis
4. Results
4.1. Study Population
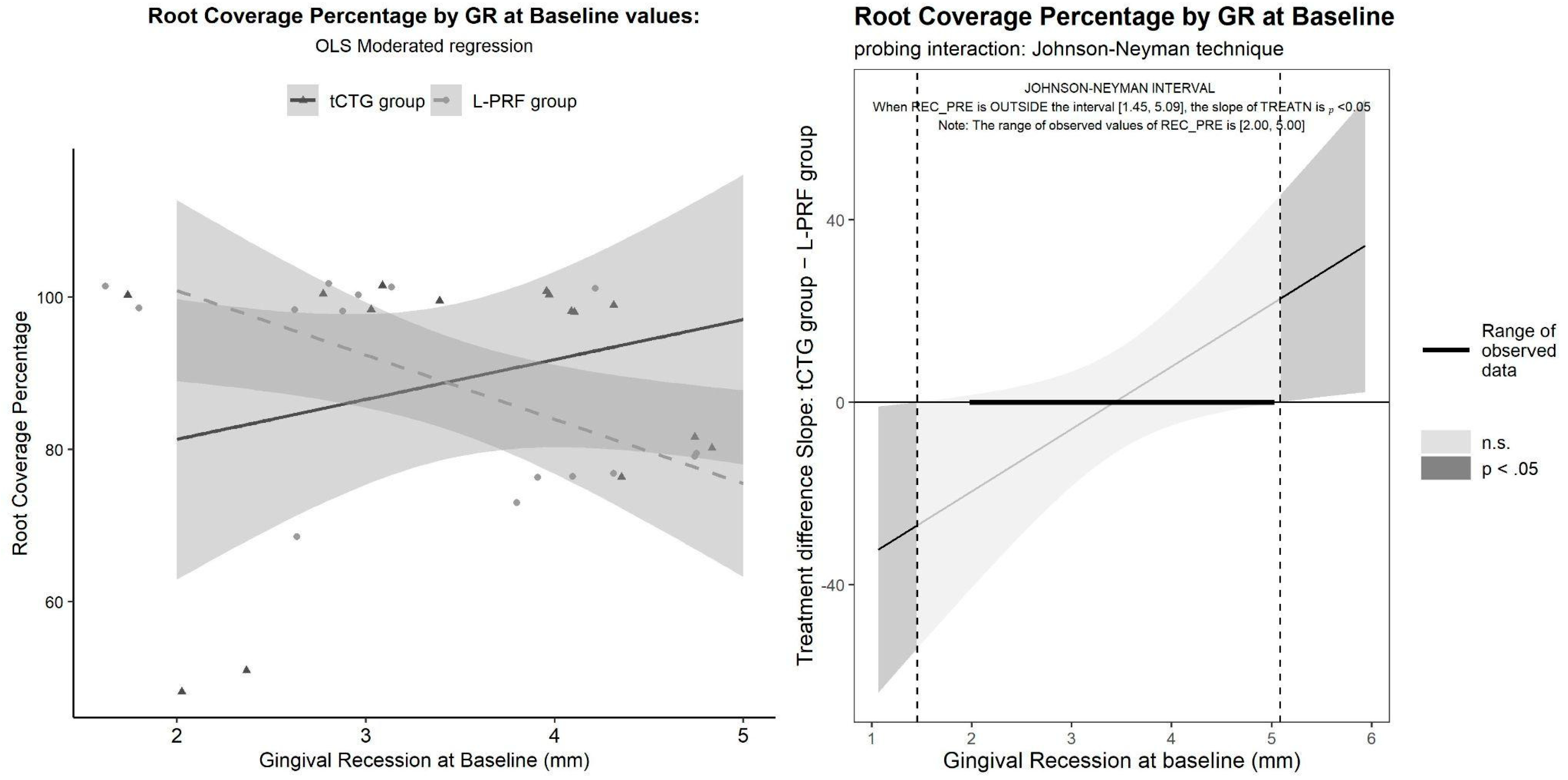
4.2. Primary Outcome, Clinical Treatment Outcomes
| Predictors | Dependent Variable | ||
| Estimates | CI | p | |
| (Intercept) | 117.73 | 85.66–149.81 | <0.001 |
| GRt0 | −8.45 | −17.41–0.52 | 0.064 |
| TREAT [tCTG] | −46.91 | −90.69–−3.13 | 0.037 |
| GRt0 × TREAT [tCTG] | 13.69 | 1.48–25.90 | 0.029 |
| Observations | 30 | ||
| R2/R2 adjusted | 0.173/0.078 | ||
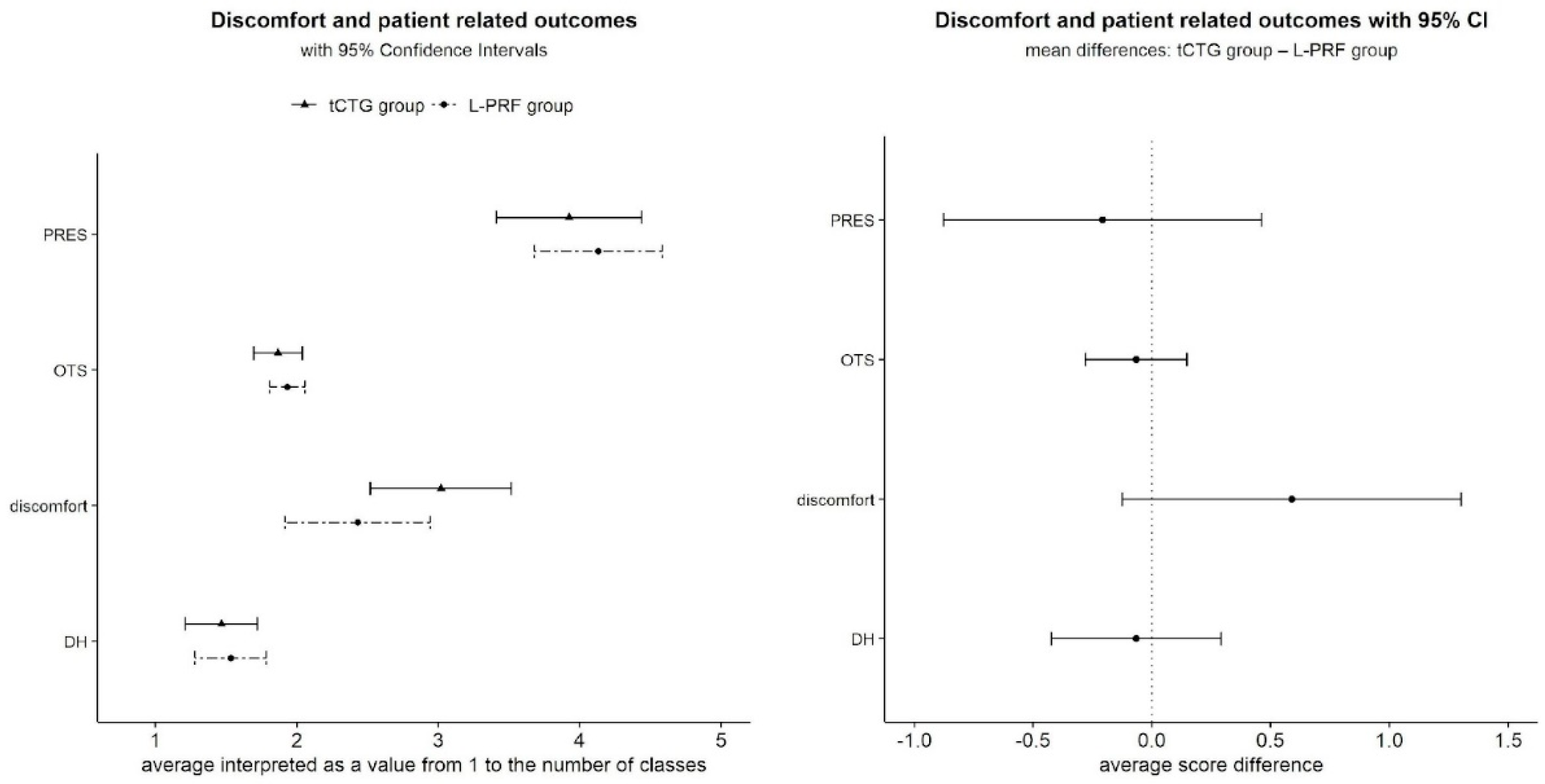
4.3. Patient-Reported Outcomes
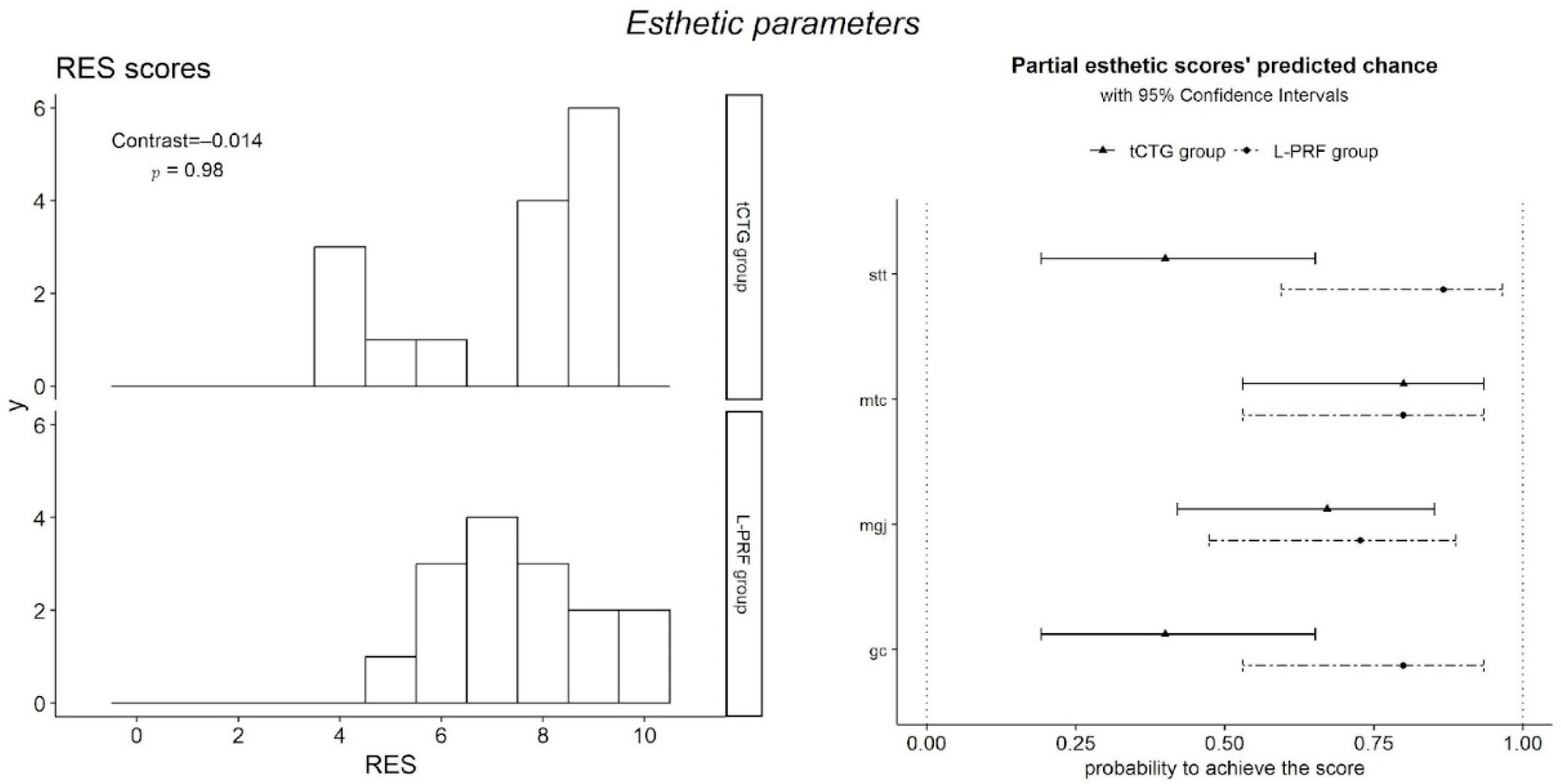
4.4. Esthetic Outcomes
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Glossary of Periodontal Terms—AAP Connect. Available online: https://members.perio.org/libraries/glossary?ssopc=1 (accessed on 20 December 2023).
- Löe, H.; Ånerud, Å.; Boysen, H. The natural history of periodontal disease in man: Prevalence, severity, and extent of gingival recession. J. Periodontol. 1992, 63, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Wennström, J.L.; Lindhe, J.; Eneroth, L. The prevalence and distribution of gingival recession in subjects with a high standard of oral hygiene. J. Clin. Periodontol. 1994, 21, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Sangnes, G.; Gjermo, P. Prevalence of oral soft and hard tissue lesions related to mechanical toothcleansing procedures. Community Dent. Oral Epidemiol. 1976, 4, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Daprile, G.; Gatto, M.R.; Checchi, L. The evolution of buccal gingival recessions in a student population: A 5-year follow-up. J. Periodontol. 2007, 78, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Agudio, G.; Nieri, M.; Rotundo, R.; Franceschi, D.; Cortellini, P.; Prato, G.P.P. Periodontal conditions of sites treated with gingival-augmentation surgery compared to untreated contralateral homologous sites: A 10- to 27-year long-term study. J. Periodontol. 2009, 80, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Tatakis, D.N. Long-Term Outcomes of Untreated Buccal Gingival Recessions: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 796–808. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mounssif, I. Periodontal plastic surgery. Periodontology 2015, 68, 333–368. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Nieri, M.; Pagliaro, U. Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J. Clin. Periodontol. 2014, 41 (Suppl. S15), S44–S62. [Google Scholar] [CrossRef] [PubMed]
- Zuhr, O.; Bäumer, D.; Hürzeler, M. The addition of soft tissue replacement grafts in plastic periodontal and implant surgery: Critical elements in design and execution. J. Clin. Periodontol. 2014, 41 (Suppl. S15), S123–S142. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Rotundo, R.; Miller, P.D.; Prato, G.P.P. Root coverage esthetic score: A system to evaluate the esthetic outcome of the treatment of gingival recession through evaluation of clinical cases. J. Periodontol. 2009, 80, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Tatakis, D.N. Periodontal soft tissue root coverage procedures: A systematic review from the AAP Regeneration Workshop. J. Periodontol. 2015, 86 (Suppl. S2), S8–S51. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mounssif, I.; Mazzotti, C.; Montebugnoli, L.; Sangiorgi, M.; Mele, M.; Stefanini, M. Does the dimension of the graft influence patient morbidity and root coverage outcomes? A randomized controlled clinical trial. J. Clin. Periodontol. 2014, 41, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Karring, T.; Lang, N.P.; Löe, H. The role of gingival connective tissue in determining epithelial differentiation. J. Periodontal Res. 1975, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dellavia, C.; Ricci, G.; Pettinari, L.; Allievi, C.; Grizzi, F.; Gagliano, N. Human palatal and tuberosity mucosa as donor sites for ridge augmentation. Int. J. Periodontics Restorative Dent. 2014, 34, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, H.C.; Atkins, J.H. Free autogenous gingival grafts. I. Principles of successful grafting. Periodontics 1968, 6, 121–129. Available online: https://www.unboundmedicine.com/medline/citation/5240496/Free_autogenous_gingival_grafts__I__Principles_of_successful_grafting_ (accessed on 20 December 2023). [PubMed]
- Sanz-Martín, I.; Rojo, E.; Maldonado, E.; Stroppa, G.; Nart, J.; Sanz, M. Structural and histological differences between connective tissue grafts harvested from the lateral palatal mucosa or from the tuberosity area. Clin. Oral Investig. 2019, 23, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Jung, U.; Um, Y.; Choi, S. Histologic observation of soft tissue acquired from maxillary tuberosity area for root coverage. J. Periodontol. 2008, 79, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, A.; Attal, U.; Chai, E.; Goultschin, J.; Boyan, B.D.; Schwartz, Z. Root coverage and pocket reduction as combined surgical procedures. J. Periodontol. 2001, 72, 1572–1579. [Google Scholar] [CrossRef] [PubMed]
- García-Caballero, L.; Gándara, M.; Cepeda-Emiliani, A.; Gallego, R.; Gude, F.; Suárez-Quintanilla, J.; Ramos-Barbosa, I.; Blanco-Carrión, J. Histological and histomorphometric study of human palatal mucosa: Implications for connective tissue graft harvesting. J. Clin. Periodontol. 2023, 50, 784–795. [Google Scholar] [CrossRef]
- Asparuhova, M.B.; Song, X.; Riedwyl, D.; van Geest, G.; Bosshardt, D.D.; Sculean, A. Differential molecular profiles and associated functionalities characterize connective tissue grafts obtained at different locations and depths in the human palate. Int. J. Oral Sci. 2023, 15, 57. [Google Scholar] [CrossRef] [PubMed]
- Amin, P.N.; Bissada, N.F.; Ricchetti, P.A.; Silva, A.P.B.; Demko, C.A. Tuberosity versus palatal donor sites for soft tissue grafting: A split-mouth clinical study. Quintessence Int. 2018, 49, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.R.; Cruz, A.; Concepción, E.; López, C.; Hou, W.; Romanos, G.E. Connective Tissue Graft vs Platelet-rich Fibrin in the Treatment of Gingival Recessions: A Randomized Split-mouth Case Series. J. Contemp. Dent. Pract. 2021, 22, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Aroca, S.; Keglevich, T.; Barbieri, B.; Gera, I.; Etienne, D. Clinical evaluation of a modified coronally advanced flap alone or in combination with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: A 6-month study. J. Periodontol. 2009, 80, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Padma, R.; Shilpa, A.; Kumar, P.A.; Nagasri, M.; Kumar, C.; Sreedhar, A. A split mouth randomized controlled study to evaluate the adjunctive effect of platelet-rich fibrin to coronally advanced flap in Miller’s class-I and II recession defects. J. Indian. Soc. Periodontol. 2013, 17, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Mancini, L.; Tarallo, F.; Quinzi, V.; Fratini, A.; Mummolo, S.; Marchetti, E. Platelet-Rich Fibrin in Single and Multiple Coronally Advanced Flap for Type 1 Recession: An Updated Systematic Review and Meta-Analysis. Medicina 2021, 57, 144. [Google Scholar] [CrossRef]
- Chambrone, L.; Barootchi, S.; Avila-Ortiz, G. Efficacy of biologics in root coverage and gingival augmentation therapy: An American Academy of Periodontology best evidence systematic review and network meta-analysis. J. Periodontol. 2022, 93, 1771–1802. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Moraschini, V.; Del Fabbro, M.; Piattelli, A.; Fujioka-Kobayashi, M.; Zhang, Y.; Saulacic, N.; Schaller, B.; Kawase, T.; Cosgarea, R.; et al. Use of platelet-rich fibrin for the treatment of gingival recessions: A systematic review and meta-analysis. Clin Oral Investig. 2020, 24, 2543–2557. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Calasans-Maia, M.D.; Dias, A.T.; de Carvalho Formiga, M.; Sartoretto, S.C.; Sculean, A.; Shibli, J.A. Effectiveness of connective tissue graft substitutes for the treatment of gingival recessions compared with coronally advanced flap: A network meta-analysis. Clin. Oral Investig. 2020, 24, 3395–3406. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: Intra-bony defects, furcation defects and periodontal plastic surgery. A systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 67–82. [Google Scholar] [CrossRef]
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. S1), S204–S213. [Google Scholar] [CrossRef]
- Cummins, D. Clinical evaluation of the efficacy of an in-office desensitizing paste containing 8% arginine and calcium carbonate in providing instant and lasting relief of dentin hypersensitivity. Am. J. Dent. 2009, 22, 8A–15A. Available online: https://www.academia.edu/47802907/Clinical_evaluation_of_the_efficacy_of_an_in_office_desensitizing_paste_containing_8_arginine_and_calcium_carbonate_in_providing_instant_and_lasting_relief_of_dentin_hypersensitivity (accessed on 19 October 2023).
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar] [CrossRef] [PubMed]
- Allen, E.P.; Miller, P.D., Jr. Coronal positioning of existing gingiva: Short term results in the treatment of shallow marginal tissue recession. J. Periodontol. 1989, 60, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Stuhr, S.; Nör, F.; Gayar, K.; Couso-Queiruga, E.; Chambrone, L.; Gamborena, I.; Kumar, P.; Avila-Ortiz, G.; Ganesan, S.M. Histological assessment and gene expression analysis of intra-oral soft tissue graft donor sites. J. Clin. Periodontol. 2023, 50, 1360–1370. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S.; Di Gianfilippo, R.; Modarressi, M.; Cairo, F.; Rasperini, G.; Wang, H.L. Acellular dermal matrix and coronally advanced flap or tunnel technique in the treatment of multiple adjacent gingival recessions. A 12-year follow-up from a randomized clinical trial. J. Clin. Periodontol. 2019, 46, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Barootchi, S.; Tavelli, L.; Di Gianfilippo, R.; Shedden, K.; Oh, T.; Rasperini, G.; Neiva, R.; Giannobile, W.V.; Wang, H. Soft tissue phenotype modification predicts gingival margin long-term (10-year) stability: Longitudinal analysis of six randomized clinical trials. J. Clin. Periodontol. 2022, 49, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Rebele, S.F.; Zuhr, O.; Schneider, D.; Jung, R.E.; Hürzeler, M.B. Tunnel technique with connective tissue graft versus coronally advanced flap with enamel matrix derivative for root coverage: A RCT using 3D digital measuring methods. Part II. Volumetric studies on healing dynamics and gingival dimensions. J. Clin. Periodontol. 2014, 41, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S.; Greenwell, H.; Wang, H.L. Is a soft tissue graft harvested from the maxillary tuberosity the approach of choice in an isolated site? J. Periodontol. 2019, 90, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, S.; Aleksic, Z.; Klokkevold, P.; Lekovic, V.; Dimitrijevic, B.; Barrie Kenney, E.; Camargo, P. Use of platelet-rich fibrin membrane following treatment of gingival recession: A randomized clinical trial. Int. J. Periodontics Restor. Dent. 2012, 32, e41–e50. [Google Scholar]
- Kuka, S.; Ipci, S.D.; Cakar, G.; Yılmaz, S. Clinical evaluation of coronally advanced flap with or without platelet-rich fibrin for the treatment of multiple gingival recessions. Clin. Oral Investig. 2018, 22, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Paolantonio, M. Treatment of gingival recessions by combined periodontal regenerative technique, guided tissue regeneration, and subpedicle connective tissue graft. A comparative clinical study. J. Periodontol. 2002, 73, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mounssif, I.; Mazzotti, C.; Stefanini, M.; Marzadori, M.; Petracci, E.; Montebugnoli, L. Coronally advanced flap with and without connective tissue graft for the treatment of multiple gingival recessions: A comparative short- and long-term controlled randomized clinical trial. J. Clin. Periodontol. 2014, 41, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Santamaria, P.; Paolantonio, M.; Romano, L.; Serroni, M.; Rexhepi, I.; Secondi, L.; Paolantonio, G.; Sinjari, B.; De Ninis, P. Gingival phenotype changes after different periodontal plastic surgical techniques: A single-masked randomized controlled clinical trial. Clin. Oral Investig. 2023, 27, 3423–3435. [Google Scholar] [CrossRef] [PubMed]
- Ehrenfest, D.M.D.; Del Corso, M.; Diss, A.; Mouhyi, J.; Charrier, J. Three-dimensional architecture and cell composition of a Choukroun’s platelet-rich fibrin clot and membrane. J. Periodontol. 2010, 81, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Rojo, E.; Stroppa, G.; Sanz-Martin, I.; Gonzalez-Martín, O.; Alemany, A.S.; Nart, J. Soft tissue volume gain around dental implants using autogenous subepithelial connective tissue grafts harvested from the lateral palate or tuberosity area. A randomized controlled clinical study. J. Clin. Periodontol. 2018, 45, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, H.; Toit, J.D.; Pontes, C.C.; Hille, J. Hyperplastic Response Following Soft Tissue Augmentation in the Esthetic Zone. Clin. Adv. Periodontics 2019, 9, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Puisys, A.; Auzbikaviciute, V.; Vindasiute-Narbute, E.; Zukauskas, S.; Razukevicus, D.; Dard, M.M. Full versus partial thickness flap to determine differentiation and over keratinization of non-keratinized mucosa. A 3-year split mouth randomized pilot study. Clin. Exp. Dent. Res. 2021, 7, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Femminella, B.; Iaconi, M.C.; Di Tullio, M.; Romano, L.; Sinjari, B.; D’Arcangelo, C.; De Ninis, P.; Paolantonio, M. Clinical Comparison of Platelet-Rich Fibrin and a Gelatin Sponge in the Management of Palatal Wounds After Epithelialized Free Gingival Graft Harvest: A Randomized Clinical Trial. J. Periodontol. 2016, 87, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Cortellini, P.; Pilloni, A.; Nieri, M.; Cincinelli, S.; Amunni, F.; Pagavino, G.; Tonetti, M.S. Clinical efficacy of coronally advanced flap with or without connective tissue graft for the treatment of multiple adjacent gingival recessions in the aesthetic area: A randomized controlled clinical trial. J. Clin. Periodontol. 2016, 43, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Rasperini, G.; Acunzo, R.; Pellegrini, G.; Pagni, G.; Tonetti, M.; Pini Prato, G.P.; Cortellini, P. Predictor factors for long-term outcomes stability of coronally advanced flap with or without connective tissue graft in the treatment of single maxillary gingival recessions: 9 years results of a randomized controlled clinical trial. J. Clin. Periodontol. 2018, 45, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Burkhardt, R. Minimal invasiveness in gingival augmentation and root coverage procedures. Periodontology 2000 2023, 91, 45–64. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Treatment | Baseline Mean ± SD (95% CI) | 12 Months Mean ± SD (95% CI) | Baseline-12 Months Mean (95% CI) | Within-Group Differences |
|---|---|---|---|---|---|
| GENDER (Male) | CAF + tCTG | 5 (33%) | |||
| CAF + L-PRF | 6 (40%) | ||||
| Between Groups Difference | NS | ||||
| AGE | CAF + tCTG | 43.67 ± 16.12 (34.74 to 52.59) | |||
| CAF + L-PRF | 43.27 ± 15.63 (34.61 to 51.92) | ||||
| Between Groups Difference | NS | ||||
| PD | CAF + tCTG | 1.27 ± 0.46 (1.01 to 1.52) | 1.8 ± 1.01 (1.24 to 2.36) | −0.53 ± 0.92 (−1.04 to -0.03) | 0.04 |
| CAF + L-PRF | 1.2 ± 0.41 (0.97 to 1.43) | 1.07 ± 0.26 (0.92 to 1.21) | 0.13 ± 0.35 (−0.06 to 0.33) | NS | |
| Between Groups Difference | NS | p = 0.011 | p = 0.013 | ||
| CAL | CAF + tCTG | 4.73 ± 0.88 (4.24 to 5.22) | 2.13 ± 0.99 (1.58 to 2.68) | 2.6 ± 1.4 (1.82 to 3.38) | <0.001 |
| CAF + L-PRF | 4.67 ± 0.9 (4.17 to 5.16) | 1.53 ± 0.52 (1.25 to 1.82) | 3.13 ± 0.64 (2.78 to 3.49) | <0.001 | |
| Between Groups Difference | NS | p = 0.047 | p = NS | ||
| GR | CAF + tCTG | 3.47 ± 0.99 (2.92 to 4.02) | 0.33 ± 0.49 (0.06 to 0.6) | 3.13 ± 1.06 (2.55 to 3.72) | <0.001 |
| CAF + L-PRF | 3.47 ± 0.92 (2.96 to 3.97) | 0.47 ± 0.52 (0.18 to 0.75) | 3 ± 0.65 (2.64 to 3.36) | <0.001 | |
| Between Groups Difference | NS | NS | NS | ||
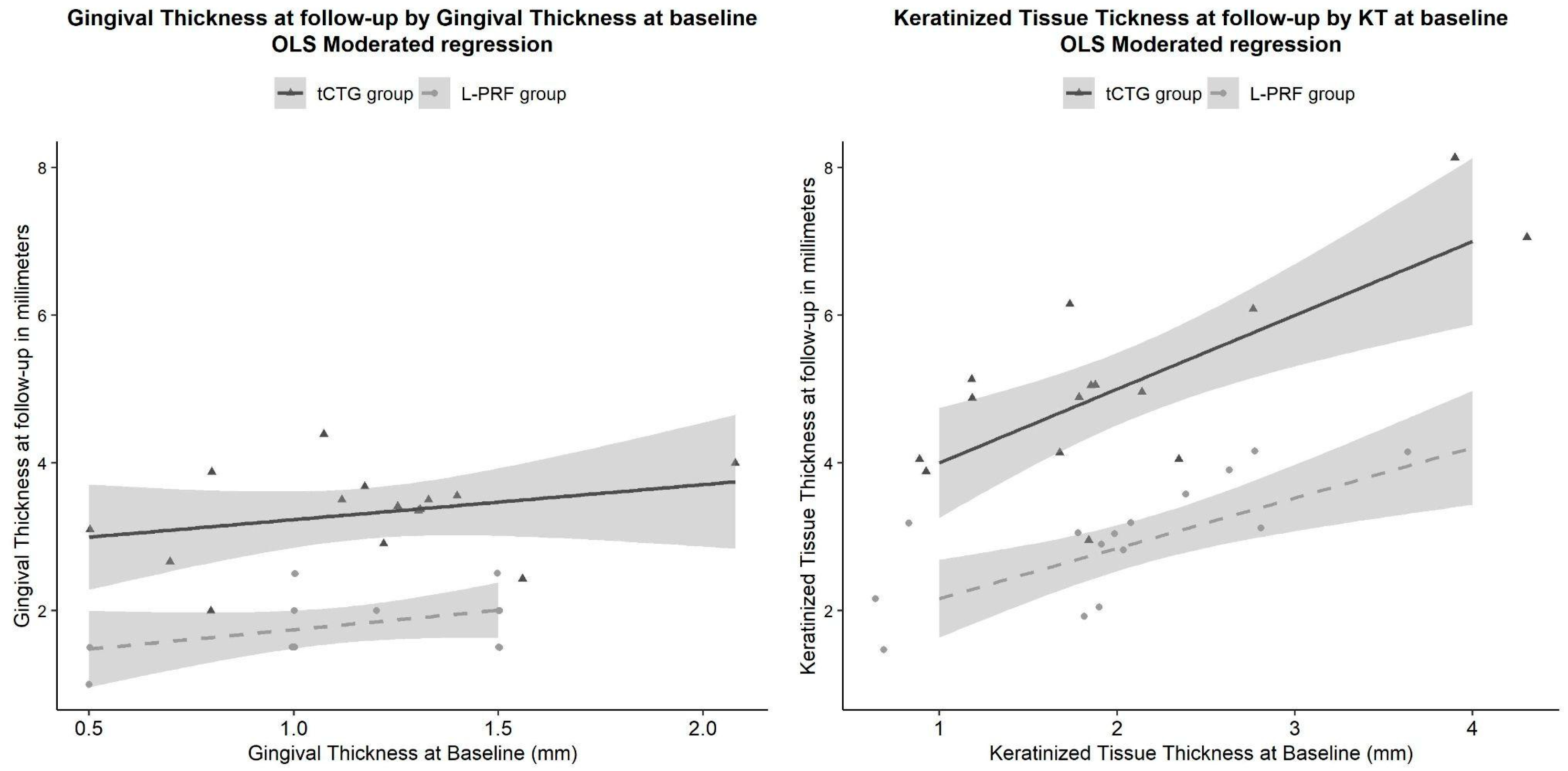
| KT | CAF + tCTG | 2.07 ± 0.96 (1.53 to 2.6) | 5.07 ± 1.28 (4.36 to 5.78) | 3 ± 0.85 (2.53 to 3.47) | <0.001 |
| CAF + L-PRF | 2.13 ± 0.83 (1.67 to 2.6) | 2.93 ± 0.78 (2.5 to 3.36) | 0.8 ± 0.59 (0.47 to 1.13) | <0.001 | |
| Between Groups Difference | NS | p < 0.001 | p < 0.001 | ||
| GT | CAF + tCTG | 1.17 ± 0.38 (0.96 to 1.39) | 3.31 ± 0.62 (2.97 to 3.66) | 2.14 ± 0.63 (1.79 to 2.49) | <0.001 |
| CAF + L-PRF | 1.11 ± 0.34 (0.93 to 1.3) | 1.8 ± 0.46 (1.55 to 2.05) | 0.69 ± 0.45 (0.44 to 0.94) | <0.001 | |
| Between Groups Difference | NS | p < 0.001 | p < 0.001 | ||
| Patients obtaining Complete Root Coverage | CAF + tCTG | 10 (67%) | |||
| CAF + L-PRF Between Groups Difference | 8 (53%) NS | ||||
| Root Coverage % | CAF + tCTG | 89 ± 18.15 (78.95 to 99.05) | |||
| CAF+ L-PRF | 88.45 ± 13.11 (81.19 to 95.71) | ||||
| Between Groups Difference | NS | ||||
| RES score | CAF + tCTG | 8 (5.5 to 9) | |||
| CAF + L-PRF | 7 (6.5 to 8.5) | ||||
| Between Groups Difference | NS | ||||
| Pain (VAS) | CAF + tCTG | 4 (3 to 5) | |||
| CAF + L-PRF | 4 (2.5 to 4) | ||||
| Between Groups Difference | NS | ||||
| Dentine Hypersensitivity | CAF + tCTG | 2 (2 to 3) | 0 (0 to 1) | ||
| CAF + L-PRF | 3 (2 to 3) | 1 (0 to 1) | |||
| Between Groups Difference | NS | NS | |||
| Patient-Related Esthetic Esthetic Score | CAF + tCTG | 9 (8.5 to 10) | |||
| CAF + L-PRF | 9 (9 to 10) | ||||
| Between Groups Difference | NS | ||||
| Overall Treatment Satisfaction | CAF + tCTG | 13 (86%) | |||
| CAF + L-PRF | 14 (93%) | ||||
| Between Groups Difference | NS |
| Parameter | Mean Difference ± SE (95% CI) | OR ± Delta SE (95% CI) | p-Value | |
|---|---|---|---|---|
| PD (in mm) | −0.667 ± 0.253 (−1.19 to −0.148) | 0.0136 | ||
| CAL (in mm) | −0.59 ± 0.29 (−1.19 to 0.00465) | 0.0517 | ||
| GR (in mm) | 0.133 ± 0.171 (−0.218 to 0.484) | 0.442 | ||
| KT (in mm) | 2.2 ± 0.266 (1.65 to 2.75) | <0.001 | ||
| GT (in mm) | 1.45 ± 0.199 (1.05 to 1.86) | <0.001 | ||
| Complete Root Coverage Fraction | 0.133 (−0.21 to 0.48) | 1.72 ± 1.32 (0.4 to 7.66) | 0.45 | |
| Root Coverage % | at GRt0=2.00 | −19.53 ± 10.28 (−40.66 to 1.6) | 0.0686 | |
| at GRt0=3.47 | 0.599 ± 5.45 (−10.61 to 11.81) | 0.91 | ||
| at GRt0=5.00 | 21.55 ± 10.61 (−0.27 to 43.4) | 0.0527 | ||
| Root Coverage % Sensitivity analysis (w/o cases 7, 13) | at any GRt0 | 8.3 ± 3.64 (0.801 to 15.8) | 0.0314 | |
| RES score | −0.207 ± 0.341 (−0.875 to 0.462) | 0.54 | ||
| Discomfort (VAS) | 0.588 ± 0.364 (−0.125 to 1.3) | 0.11 | ||
| Dentine Hypersensitivity | −0.067 ± 0.182 (−0.424 to 0.29) | 0.71 | ||
| Patient-related esthetic score (VAS) | −0.41 ± 0.677 (−1.74 to 0.917) | 0.54 | ||
| Overall treatment satisfaction | −0.067 (−0.28 to 0.14) | 0.464 ± 0.596 (0.037 to 5.75) | 0.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balice, G.; Paolantonio, M.; Serroni, M.; De Ninis, P.; Rexhepi, I.; Frisone, A.; Di Gregorio, S.; Romano, L.; Sinjari, B.; Murmura, G.; et al. Treatment of Multiple RT1 Gingival Recessions Using a Coronally Advanced Flap Associated with L-PRF or Subgingival Connective Tissue Graft from Maxillary Tuberosity: A Randomized, Controlled Clinical Trial. Dent. J. 2024, 12, 86. https://doi.org/10.3390/dj12040086
Balice G, Paolantonio M, Serroni M, De Ninis P, Rexhepi I, Frisone A, Di Gregorio S, Romano L, Sinjari B, Murmura G, et al. Treatment of Multiple RT1 Gingival Recessions Using a Coronally Advanced Flap Associated with L-PRF or Subgingival Connective Tissue Graft from Maxillary Tuberosity: A Randomized, Controlled Clinical Trial. Dentistry Journal. 2024; 12(4):86. https://doi.org/10.3390/dj12040086
Chicago/Turabian StyleBalice, Giuseppe, Michele Paolantonio, Matteo Serroni, Paolo De Ninis, Imena Rexhepi, Alessio Frisone, Stefania Di Gregorio, Luigi Romano, Bruna Sinjari, Giovanna Murmura, and et al. 2024. "Treatment of Multiple RT1 Gingival Recessions Using a Coronally Advanced Flap Associated with L-PRF or Subgingival Connective Tissue Graft from Maxillary Tuberosity: A Randomized, Controlled Clinical Trial" Dentistry Journal 12, no. 4: 86. https://doi.org/10.3390/dj12040086