
Epoxy vs. Calcium Silicate-Based Root Canal Sealers for Different Clinical Scenarios: A Narrative Review

 and
and 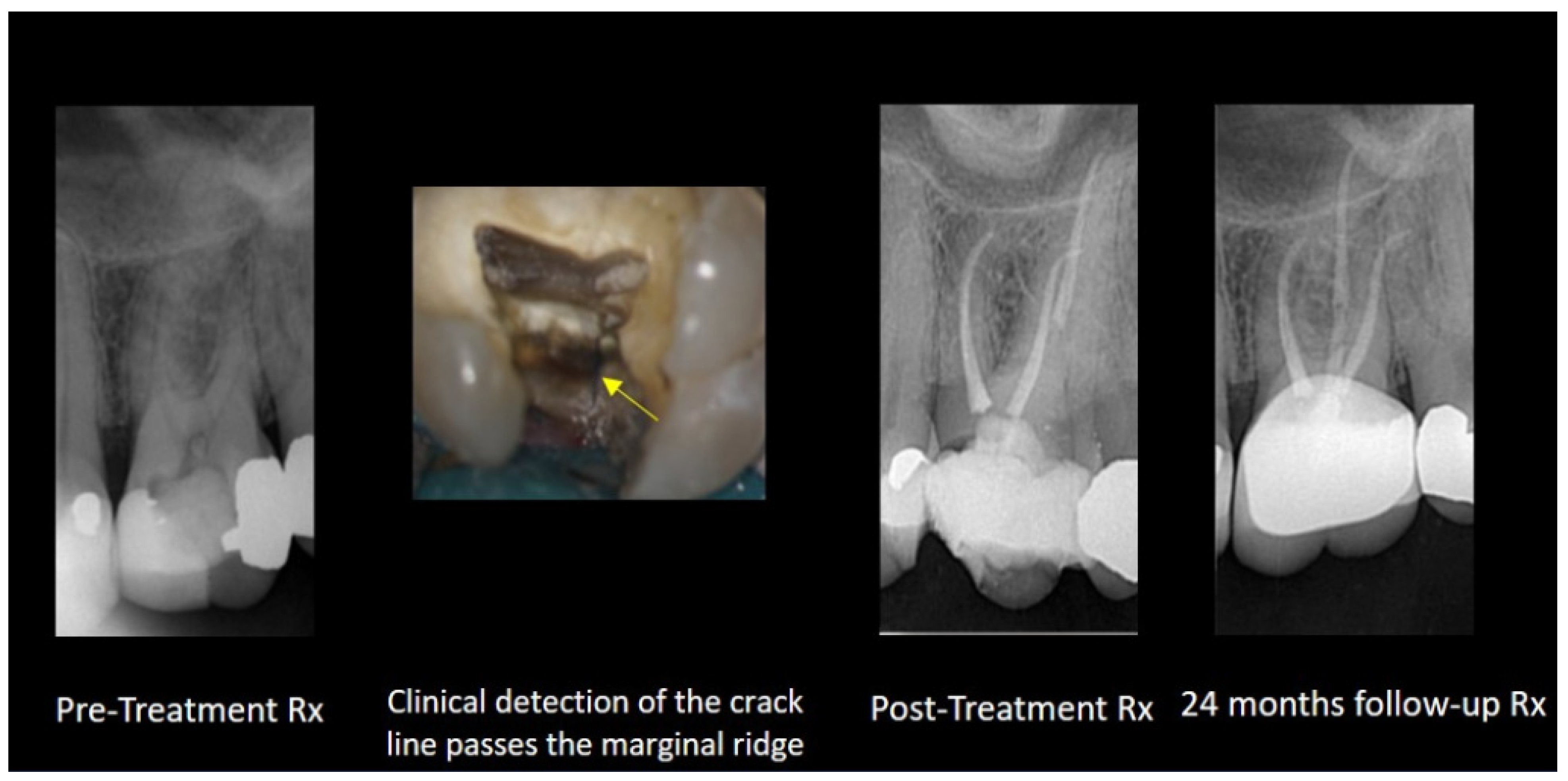{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Literature Search and Scope of the Review
1.2. Epoxy Resin-Based Sealers (ERSs)
1.3. Calcium Silicate-Based Sealers (CSSs)
2. Clinical Situations for Different Preferable Root Canal Sealers
2.1. Single vs. Multiple Appointments in Non-Vital Cases
2.2. Cracked Tooth
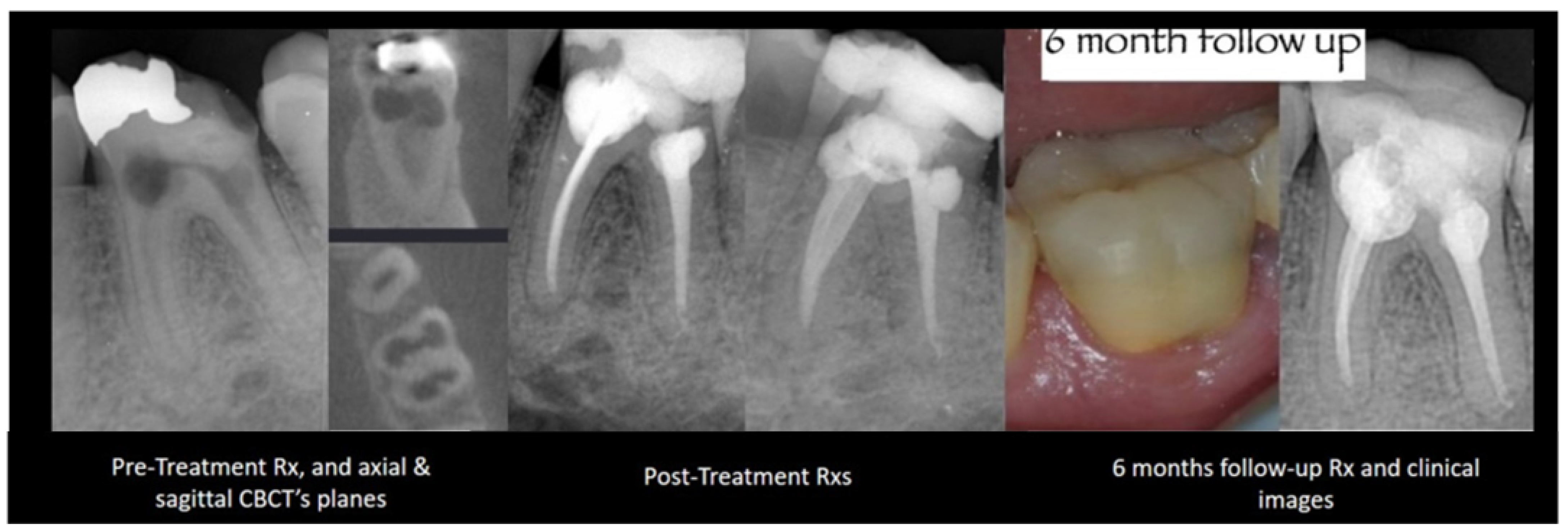
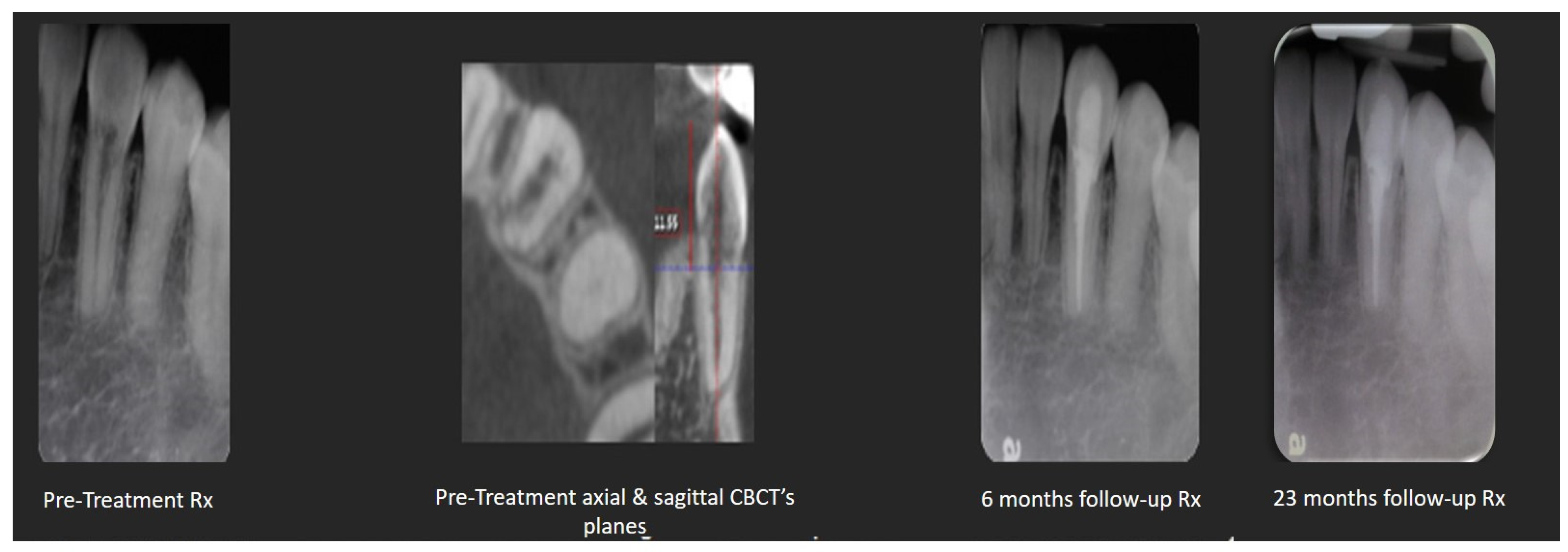
2.3. Root Canal Treatment for Teeth in Close Proximity to Anatomic Structures
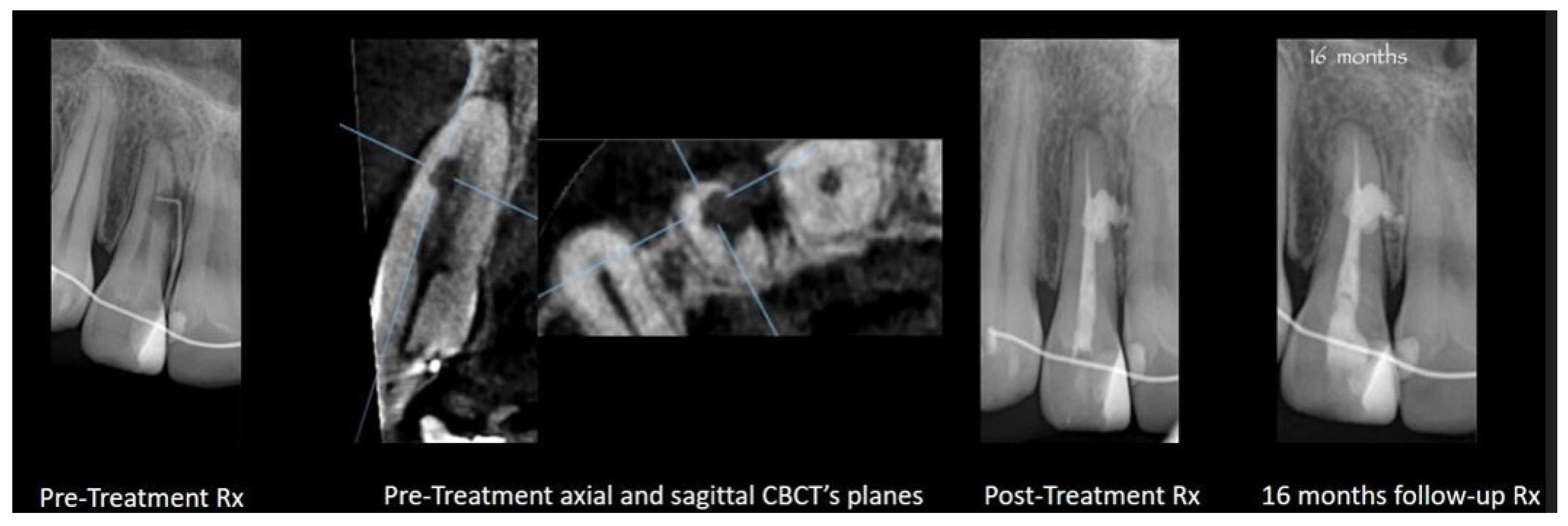
2.4. Resorptions
2.5. Non-Divergent Open Apex
2.6. Iatrogenic Aberrations
3. Endo-Perio Lesion
Ergonomic Considerations
4. Discussion
Funding
Conflicts of Interest
References
- Sundqvist, G.; Figdor, D. Essential Endodontology, 5th ed.; Blackwell Sci-Entific Publications: Oxford, MS, USA, 2003; p. 242. [Google Scholar]
- Branstetter, J.; von Fraunhofer, J.A. The physical properties and sealing action of endodontic sealer cements: A review of the literature. J. Endod. 1982, 8, 312–316. [Google Scholar] [CrossRef]
- Grossman, L. Obturation of root canal. In Endodontic Practice, 10th ed.; Grossman, L., Ed.; Lea and Febiger: Philadelphia, PA, USA, 1982; p. 297. [Google Scholar]
- Almeida, L.H.S.; Moraes, R.R.; Morgental, R.D.; Pappen, F.G. Are premixed calcium silicate–based endodontic sealers comparable to conventional materials? A systematic review of in vitro studies. J. Endod. 2017, 43, 527–535. [Google Scholar] [CrossRef]
- Chybowski, E.A.; Glickman, G.N.; Patel, Y.; Fleury, A.; Solomon, E.; He, J. Clinical outcome of non-surgical root canal treatment using a single-cone technique with Endosequence bioceramic sealer: A retrospective analysis. J. Endod. 2018, 44, 941–945. [Google Scholar] [CrossRef]
- Park, M.G.; Kim, I.R.; Kim, H.J.; Kwak, S.W.; Kim, H.C. Physicochemical properties and cytocompatibility of newly developed calcium silicate-based sealers. Aust. Endod. J. 2021, 47, 512–519. [Google Scholar] [CrossRef]
- Lee, J.K.; Kim, S.; Lee, S.; Kim, H.C.; Kim, E. In Vitro Comparison of Biocompatibility of Calcium Silicate-Based Root Canal Sealers. Materials 2019, 12, 2411. [Google Scholar] [CrossRef]
- Spångberg, L.S.; Barbosa, S.V.; Lavigne, G.D. AH26 releases formaldehyde. J. Endod. 1993, 19, 596–598. [Google Scholar] [CrossRef]
- Azar, N.G.; Heidari, M.; Bahrami, Z.S.; Shokri, F. In vitro cytotoxicity of a new epoxy resin root canal sealer. J. Endod. 2000, 26, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr.; Favieri, A.; Gahyva, S.M.; Moraes, S.R.; Lima, K.C.; Lopes, H.P. Antimicrobial activity and flow rate of newer and established root canal sealers. J. Endod. 2000, 26, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Shen, Y.; Ruse, N.D.; Haapasalo, M. Antibacterial activity of endodontic sealers by modified direct contact test against Enterococcus faecalis. J. Endod. 2009, 35, 1051–1055. [Google Scholar] [CrossRef]
- Ørstavik, D.; Eriksen, H.M.; Beyer-Olsen, E.M. Adhesive properties and leakage of root canal sealers in vitro. Int. Endod. J. 1983, 16, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Williams, M.C.; Camps, J.J.; Pashley, D.H. Adhesion of endodontic sealers to dentin and gutta-percha. J. Endod. 2002, 28, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Tagger, M.; Tagger, E.; Tjan, A.H.; Bakland, L.K. Measurement of adhesion of endodontic sealers to dentin. J. Endod. 2002, 28, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Peters, D.D. Two-year in vitro solubility evaluation of four gutta-percha sealer obturation techniques. J. Endod. 1986, 12, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, E.; Zandbiglari, T. Solubility of root-canal sealers in water and artificial saliva. Int. Endod. J. 2003, 36, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Poggio, C.; Arciola, C.R.; Dagna, A.; Colombo, M.; Bianchi, S.; Visai, L. Solubility of root canal sealers: A comparative study. Int. J. Artif. Organs 2010, 33, 676–681. [Google Scholar] [CrossRef]
- Solomonov, M.; Ben Itzhak, J. Evaluating the physical properties of one novel and two well-established epoxy resin-based root canal sealers. ENDO 2017, 11, 285–290. [Google Scholar]
- Çobankara, F.K.; Adanır, N.; Belli, S. Evaluation of the influence of smear layer on the apical and coronal sealing ability of two sealers. J. Endod. 2004, 30, 406–409. [Google Scholar] [CrossRef]
- Zmener, O.; Spielberg, C.; Lamberghini, F.; Rucci, M. Sealing properties of a new epoxy resin-based root-canal sealer. Int. Endod. J. 1997, 30, 332–334. [Google Scholar] [CrossRef]
- Kontakiotis, E.G.; Wu, M.K.; Wesselink, P.R. Effect of sealer thickness on long–term sealing ability: A 2–year follow–up study. Int. Endod. J. 1997, 30, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Re, D.; Augusti, D.; Cerutti, F.; Gagliani, M.M.; Cerutti, A.; Chambers, D.W. A Study of undergraduate learning of two obturation techniques: Thermafil® versus lateral condensation. ENDO 2009, 3, 227–234. [Google Scholar]
- Alhindi, O.H.; Atmeh, A.R.; Alhawaj, H.; Omar, O. Inflammatory response to epoxy resin and calcium silicate sealers preheated with different temperatures: An in vivo study. Clin. Oral Investig. 2023, 27, 2235–2243. [Google Scholar] [CrossRef]
- Lertchirakarn, V.; Palamara, J.E.; Messer, H.H. Load and strain during lateral condensation and vertical root fracture. J. Endod. 1999, 25, 99–104. [Google Scholar] [CrossRef]
- Ørstavik, D. Materials used for root canal obturation: Technical, biological and clinical testing. Endod. Top. 2005, 12, 25–38. [Google Scholar] [CrossRef]
- Al-Haddad, A.; Che Ab Aziz, Z.A. Bioceramic-based root canal sealers: A review. Int. J. Biomater. 2016, 2016, 9753210. [Google Scholar] [CrossRef]
- de Miranda Candeiro, G.T.; Correia, F.C.; Duarte, M.A.H.; Ribeiro-Siqueira, D.C.; Gavini, G. Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J. Endod. 2012, 38, 842–845. [Google Scholar] [CrossRef] [PubMed]
- Uzunoglu-Özyürek, E.; Erdoğan, Ö.; Türker, S.A. Effect of calcium hydroxide dressing on the dentinal tubule penetration of 2 different root canal sealers: A confocal laser scanning microscopic study. J. Endod. 2018, 44, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, J. Characterization and hydration kinetics of tricalcium silicate cement for use as a dental biomaterial. Dent. Mater. 2011, 27, 836–884. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Karabucak, B. The antimicrobial effect of bioceramic sealer on an 8-week matured Enterococcus faecalis biofilm attached to root canal dentinal surface. J. Endod. 2019, 45, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Kapralos, V.; Koutroulis, A.; Ørstavik, D.; Sunde, P.T.; Rukke, H.V. Antibacterial activity of endodontic sealers against planktonic bacteria and bacteria in biofilms. J. Endod. 2018, 44, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.C.; Tanomaru-Filho, M.; da Silva, G.F.; Delfino, M.M.; Cerri, P.S.; Guerreiro-Tanomaru, J.M. Biocompatibility and Bioactive Potential of New Calcium Silicate–based Endodontic Sealers: Bio-C Sealer and Sealer Plus BC. J. Endod. 2020, 46, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Grande, N.M.; Plotino, G.; Tay, F.R. Histologic response of human pulp and periapical tissues to tricalcium silicate–based materials: A series of successfully treated cases. J. Endod. 2020, 46, 307–317. [Google Scholar] [CrossRef] [PubMed]
- ISO-6876; Dental Root Canal Sealing Materials. International Organization for Standardization: Geneva, Switzerland, 2001.
- Elyassi, Y.; Moinzadeh, A.T.; Kleverlaan, C.J. Characterization of leachates from 6 root canal sealers. J. Endod. 2019, 45, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Zordan-Bronzel, C.L.; Torres, F.F.E.; Tanomaru-Filho, M.; Chávez-Andrade, G.M.; Bosso-Martelo, R.; Guerreiro-Tanomaru, J.M. Evaluation of physicochemical properties of a new calcium silicate–based sealer, Bio-C Sealer. J. Endod. 2019, 45, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Alzraikat, H.; Taha, N.A.; Hassouneh, L. Dissolution of a mineral trioxide aggregate sealer in endodontic solvents compared to conventional sealers. Braz. Oral Res. 2016, 30, S1806-83242016000100215. [Google Scholar] [CrossRef] [PubMed]
- Aminoshariae, A.; Primus, C.; Kulild, J.C. Tricalcium silicate cement sealers: Do the potential benefits of bioactivity justify the drawbacks? J. Am. Dent. Assoc. 2022, 153, 750–776. [Google Scholar] [CrossRef] [PubMed]
- Yassen, G.H.; Platt, J.A. The effect of nonsetting calcium hydroxide on root fracture and mechanical properties of radicular dentine: A systematic review. Int. Endod. J. 2013, 46, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, A.N.; Nikonov, S.Y.; Pancio, A.K.; Niu, L.N.; Agee, K.A.; Loushine, R.J.; Weller, R.N.; Pashley, D.H.; Tay, F.R. Effects of calcium silicate–based materials on the flexural properties of dentin. J. Endod. 2012, 38, 680–683. [Google Scholar] [CrossRef]
- Loushine, B.A.; Bryan, T.E.; Looney, S.W.; Gillen, B.M.; Loushine, R.J.; Weller, R.N.; Pashley, D.H.; Tay, F.R. Setting properties and cytotoxicity evaluation of a premixed bioceramic root canal sealer. J. Endod. 2011, 37, 673–677. [Google Scholar] [CrossRef]
- Kishen, A. Mechanisms and risk factors for fracture predilection in endodontically treated teeth. Endod. Top. 2006, 13, 57–83. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, K.D.; Lee, J.K.; Park, W.; Jeong, J.S.; Lee, Y.; Gu, Y.; Chang, S.W.; Son, W.J.; Lee, W.C.; et al. Mesiobuccal root canal anatomy of Korean maxillary first and second molars by cone-beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 111, 785–791. [Google Scholar] [CrossRef]
- Philippas, G.G.; Applebaum, E. Age factor in secondary dentin formation. J. Dent. Res. 1966, 45, 778–789. [Google Scholar] [CrossRef]
- Tziafas, D. Mechanisms controlling secondary initiation of dentinogenesis: A review. Int. Endod. J. 1994, 27, 61–74. [Google Scholar] [CrossRef]
- Bergenholtz, G.; Lindhe, J. Effect of experimentally induced marginal periodontitis and periodontal scaling on the dental pulp. J. Clin. Periodontol. 1978, 5, 59–73. [Google Scholar] [CrossRef]
- Venkatesh, S.; Ajmera, S.; Ganeshkar, S.V. Volumetric pulp changes after orthodontic treatment determined by cone-beam computed tomography. J. Endod. 2014, 40, 1758–1763. [Google Scholar] [CrossRef]
- McMichael, G.E.; Primus, C.M.; Opperman, L.A. Dentinal tubule penetration of tricalcium silicate sealers. J. Endod. 2016, 42, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Ma, J.; Shen, Y.; Haapasalo, M. Acidic pH weakens the microhardness and microstructure of three tricalcium silicate materials. Int. Endod. J. 2015, 48, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Lozano, F.J.; Collado-González, M.; López-García, S.; García-Bernal, D.; Moraleda, J.M.; Lozano, A.; Forner, L.; Murcia, L.; Oñate-Sánchez, R.E. Evaluation of changes in ion release and biological properties of NeoMTA-Plus and Endocem-MTA exposed to an acidic environment. Int. Endod. J. 2019, 52, 1196–1209. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.J.; Ferreira, C.M.; Pinto, K.P.; Barbosa, A.F.; Colaço, M.V.; Sassone, L.M. Influence of variations in the environmental pH on the solubility and water sorption of a calcium silicate-based root canal sealer. Int. Endod. J. 2021, 54, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Forghani, M.; Gharechahi, M.; Karimpour, S. In vitro evaluation of tooth discolouration induced by mineral trioxide aggregate Fillapex and iRoot SP endodontic sealers. Aust. Endod. J. 2016, 42, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Lim, M.J.; Choi, Y.; Rosa, V.; Hong, C.U.; Min, K.S. Tooth discoloration induced by a novel mineral trioxide aggregate-based root canal sealer. Eur. J. Dent. 2016, 10, 403–407. [Google Scholar] [CrossRef]
- Chen, S.J.; Karabucak, B.; Steffen, J.J.; Yu, Y.H.; Kohli, M.R. Spectrophotometric analysis of coronal tooth discoloration induced by tricalcium silicate cements in the presence of blood. J. Endod. 2020, 46, 1913–1919. [Google Scholar] [CrossRef]
- De-Deus, G.; Santos, G.O.; Monteiro, I.Z.; Cavalcante, D.M.; Simões-Carvalho, M.; Belladonna, F.G.; Silva, E.J.N.L.; Souza, E.M.; Licha, R.; Zogheib, C.; et al. Micro-CT assessment of gap-containing areas along the gutta-percha-sealer interface in oval-shaped canals. Int. Endod. J. 2022, 55, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Coşar, M.; Kandemir Demirci, G.; Çalışkan, M.K. The effect of two different root canal sealers on treatment outcome and post-obturation pain in single-visit root canal treatment: A prospective randomized clinical trial. Int. Endod. J. 2023, 56, 318–330. [Google Scholar] [CrossRef] [PubMed]
- Pirani, C.; Camilleri, J. Effectiveness of root canal filling materials and techniques for treatment of apical periodontitis: A systematic review. Int. Endod. J. 2023, 56, 436–454. [Google Scholar] [CrossRef] [PubMed]
- Weiger, R.; Rosendahl, R.; Löst, C. Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesions. Int. Endod. J. 2000, 33, 219–226. [Google Scholar] [CrossRef] [PubMed]
- De-Deus, G.; Canabarro, A. Strength of recommendation for single-visit root canal treatment: Grading the body of the evidence using a patient-centred approach. Int. Endod. J. 2017, 50, 251–259. [Google Scholar] [CrossRef]
- Lambrianidis, T.; Margelos, J.; Beltes, P. Removal efficiency of calcium hydroxide dressing from the root canal. J. Endod. 1999, 25, 85–88. [Google Scholar] [CrossRef]
- Stamos, D.; Sadeghi, E.; Haasch, G.; Gerstein, H. An in vitro comparison study to quantitate the debridement ability of hand, sonic, and ultrasonic instrumentation. J. Endod. 1987, 13, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Asawaworarit, W.; Pinyosopon, T.; Kijsamanmith, K. Comparison of apical sealing ability of bioceramic sealer and epoxy resin-based sealer using the fluid filtration technique and scanning electron microscopy. J. Dent. Sci. 2020, 15, 186–192. [Google Scholar] [CrossRef]
- Patri, G.; Agrawal, P.; Anushree, N.; Arora, S.; Kunjappu, J.J.; Shamsuddin, S.V. A scanning electron microscope analysis of sealing potential and marginal adaptation of different root canal sealers to dentin: An in vitro study. J. Contemp. Dent. Pract. 2020, 21, 73–77. [Google Scholar] [CrossRef]
- Wu, S.; Lew, H.P.; Chen, N.N. Incidence of pulpal complications after diagnosis of vital cracked teeth. J. Endod. 2019, 45, 521–525. [Google Scholar] [CrossRef]
- Chong, B.S.; Gohil, K.; Pawar, R.; Makdissi, J. Anatomical relationship between mental foramen, mandibular teeth and risk of nerve injury with endodontic treatment. Clin. Oral Investig. 2017, 21, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Lvovsky, A.; Bachrach, S.; Kim, H.C.; Pawar, A.; Levinzon, O.; Itzhak, J.B.; Solomonov, M. Relationship between root apices and the mandibular canal: A cone-beam computed tomographic comparison of 3 populations. J. Endod. 2018, 44, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Razumova, S.; Brago, A.; Howijieh, A.; Manvelyan, A.; Barakat, H.; Baykulova, M. Evaluation of the relationship between the maxillary sinus floor and the root apices of the maxillary posterior teeth using cone-beam computed tomographic scanning. J. Conserv. Dent. JCD 2019, 22, 139. [Google Scholar] [CrossRef] [PubMed]
- Stanley, E.; Strother, K.K.; Kirkpatrick, T.; Jeong, J.W. Calcium Silicate–based Sealer Extrusion into the Mandibular Canal: 3 Different Recovery Outcomes—A Report of 3 Cases. J. Endod. 2023, 49, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Ricucci, D.; Durak, C.; Tay, F. Internal root resorption: A review. J. Endod. 2010, 36, 1107–1121. [Google Scholar] [CrossRef]
- Duggal, M.; Tong, H.J.; Al-Ansary, M.; Twati, W.; Day, P.F.; Nazzal, H. Interventions for the endodontic management of non-vital traumatised immature permanent anterior teeth in children and adolescents: A systematic review of the evidence and guidelines of the European Academy of Paediatric Dentistry. Eur. Arch. Paediatr. Dent. 2017, 18, 139–151. [Google Scholar] [CrossRef]
- Hadad, A.; Azizi, H.; Ben Itzhak, J.; Solomonov, M. Simplified Approach for Obturation of Non-Divergent Open Apex with Gutta Percha & Bioceramic Sealer; ESE: Vienna, Austria, 2019. [Google Scholar]
- Eleazer, P.; Glickman, G.; McClanahan, S. AAE Glossary of Endodontic Terms; Clinical Resources; American Association of Endodontists: Chicago, IL, USA, 2020. [Google Scholar]
- Allam, C.R. Treatment of stripping perforations. J. Endod. 1996, 22, 699–702. [Google Scholar] [CrossRef]
- Main, C.; Mirzayan, N.; Shabahang, S.; Torabinejad, M. Repair of root perforations using mineral trioxide aggregate: A long-term study. J. Endod. 2004, 30, 80–83. [Google Scholar] [CrossRef]
- Lemon, R.R. Nonsurgical repair of perforation defects. Internal matrix concept. Dent. Clin. N. Am. 1992, 36, 439–457. [Google Scholar] [CrossRef]
- Bargholz, C. Perforation repair with mineral trioxide aggregate: A modified matrix concept. Int. Endod. J. 2005, 38, 59–69. [Google Scholar] [CrossRef]
- Tan, H.S.G.; Lim, K.C.; Lui, J.N.; Lai, W.M.C.; Yu, V.S.H. Postobturation pain associated with tricalcium silicate and resin-based sealer techniques: A randomized clinical trial. J. Endod. 2021, 47, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Belli, S.; Eraslan, O.; Eskitascioglu, G. Effect of root filling on stress distribution in premolars with endodontic-periodontal lesion: A finite elemental analysis study. J. Endod. 2016, 42, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Bürklein, S.; Schäfer, E. Minimally invasive endodontics. Quintessence Int. 2015, 46, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.; Khademi, J. Modern molar endodontic access and directed dentin conservation. Dent. Clin. 2010, 54, 249–273. [Google Scholar] [CrossRef] [PubMed]
- Plotino, G.; Grande, N.M.; Isufi, A.; Ioppolo, P.; Pedullà, E.; Bedini, R.; Gambarini, G.; Testarelli, L. Fracture strength of endodontically treated teeth with different access cavity designs. J. Endod. 2017, 43, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Landtwing, K. Evaluation of the normal range of vertical mandibular opening in children and adolescents with special reference to age and stature. J. Maxillofac. Surg. 1978, 6, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Khare, N.; Patil, S.B.; Kale, S.M.; Sumeet, J.; Sonali, I.; Sumeet, B. Normal mouth opening in an adult Indian population. J. Maxillofac. Oral Surg. 2012, 11, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Barros, J.; Silva, M.G.; Rôças, I.N.; Gonçalves, L.S.; Alves, F.F.; Lopes, M.A.; Pina-Vaz, I.; Siqueira, J.F., Jr. Antibiofilm effects of endodontic sealers containing quaternary ammonium polyethylenimine nanoparticles. J. Endod. 2014, 40, 1167–1171. [Google Scholar] [CrossRef] [PubMed]
- Kesler Shvero, D.; Abramovitz, I.; Zaltsman, N.; Perez Davidi, M.; Weiss, E.I.; Beyth, N. Towards antibacterial endodontic sealers using quaternary ammonium nanoparticles. Int. Endod. J. 2013, 46, 747–754. [Google Scholar] [CrossRef]
- Cardinali, F.; Camilleri, J. A critical review of the material properties guiding the clinician’s choice of root canal sealers. Clin. Oral Investig. 2023, 27, 4147–4155. [Google Scholar] [CrossRef] [PubMed]
- Raman, V.; Camilleri, J. Characterization and Assessment of Physical Properties of 3 Single Syringe Hydraulic Cement–based Sealers. J. Endod. 2024, in press. [Google Scholar] [CrossRef]
- Okamoto, M.; Matsumoto, S.; Moriyama, K.; Huang, H.; Watanabe, M.; Miura, J.; Sugiyama, K.; Hirose, Y.; Mizuhira, M.; Kuriki, N.; et al. Biological Evaluation of the Effect of Root Canal Sealers Using a Rat Model. Pharmaceutics 2022, 14, 2038. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azizi, H.; Hadad, A.; Levy, D.H.; Ben Itzhak, J.; Kim, H.-C.; Solomonov, M. Epoxy vs. Calcium Silicate-Based Root Canal Sealers for Different Clinical Scenarios: A Narrative Review. Dent. J. 2024, 12, 85. https://doi.org/10.3390/dj12040085
Azizi H, Hadad A, Levy DH, Ben Itzhak J, Kim H-C, Solomonov M. Epoxy vs. Calcium Silicate-Based Root Canal Sealers for Different Clinical Scenarios: A Narrative Review. Dentistry Journal. 2024; 12(4):85. https://doi.org/10.3390/dj12040085
Chicago/Turabian StyleAzizi, Hadas, Avi Hadad, Dan Henry Levy, Joe Ben Itzhak, Hyeon-Cheol Kim, and Michael Solomonov. 2024. "Epoxy vs. Calcium Silicate-Based Root Canal Sealers for Different Clinical Scenarios: A Narrative Review" Dentistry Journal 12, no. 4: 85. https://doi.org/10.3390/dj12040085