
Vacuum Plasma Treatment Device for Enhancing Fibroblast Activity on Machined and Rough Titanium Surfaces

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
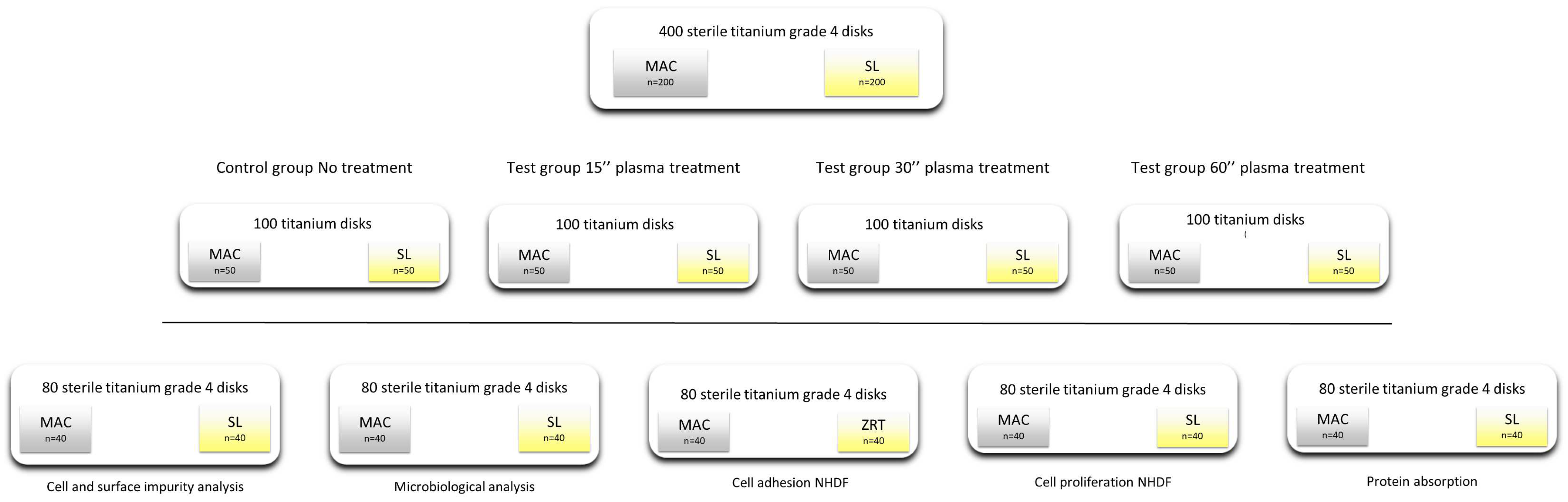
2.1. Study Design and Sample Description
2.1.1. Microbiological Analysis
2.1.2. Protein Adsorption
2.1.3. Cell Model
2.1.4. Cell Adhesion
2.1.5. Cell Proliferation
2.1.6. Cell Morphology and Focal Adhesion
2.1.7. Cell Morphology at SEM
2.2. Statistical Analysis
3. Results
3.1. Temperature
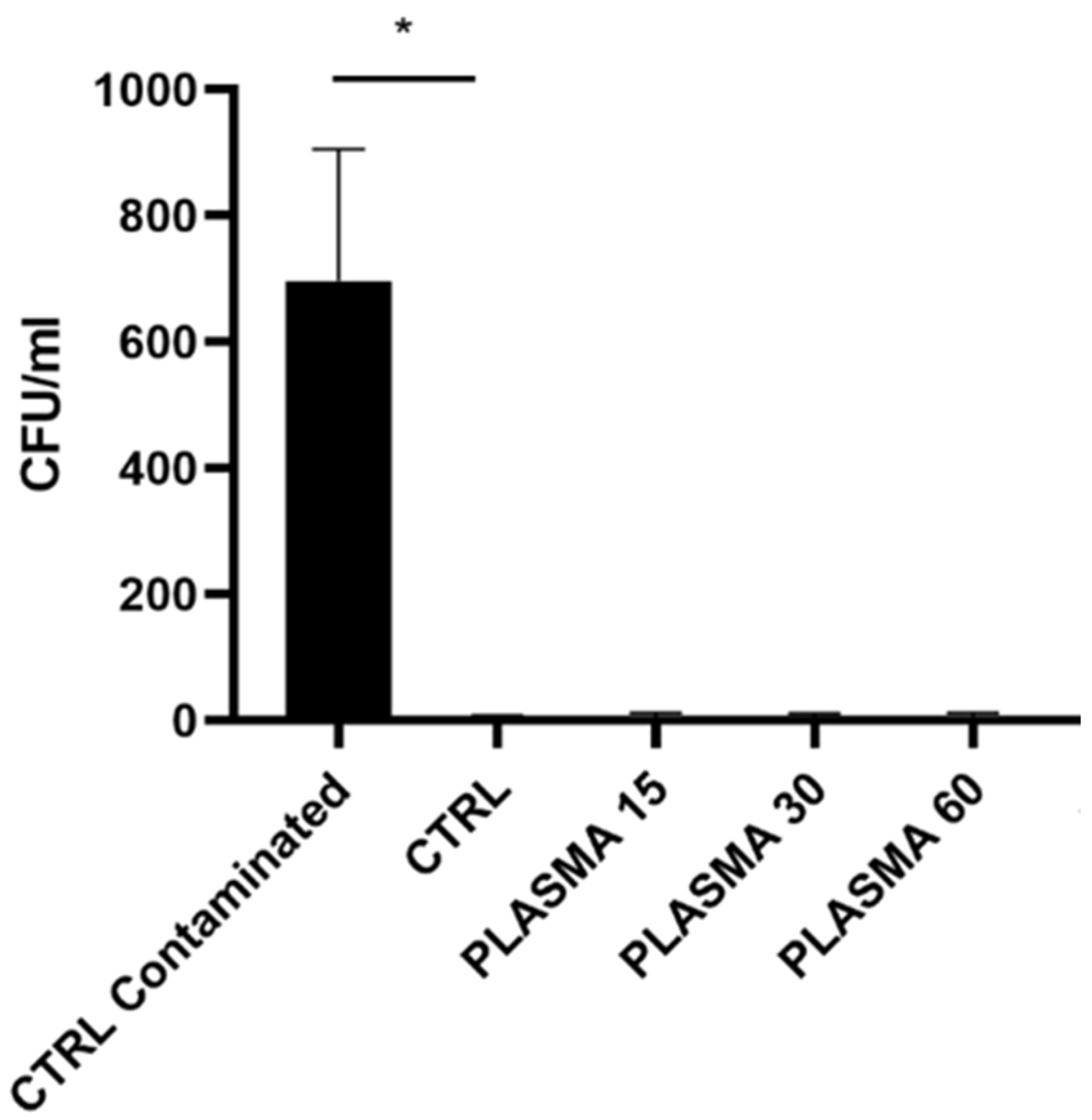
3.2. Microbiological Analysis (Table 2)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Microbiology Assay | |||
|---|---|---|---|
| Mean | Std. Dev. | p Value vs. CTRL | |
| CTRL contaminated | 697.25 | 415.913 | 0.009 |
| CTRL | 5 | 5.09902 | |
| 15″ | 7.75 | 8.341663 | 0.94 |
| 30″ | 7.25 | 7.932003 | 0.8017 |
| 60″ | 7.75 | 9.287088 | 0.7824 |
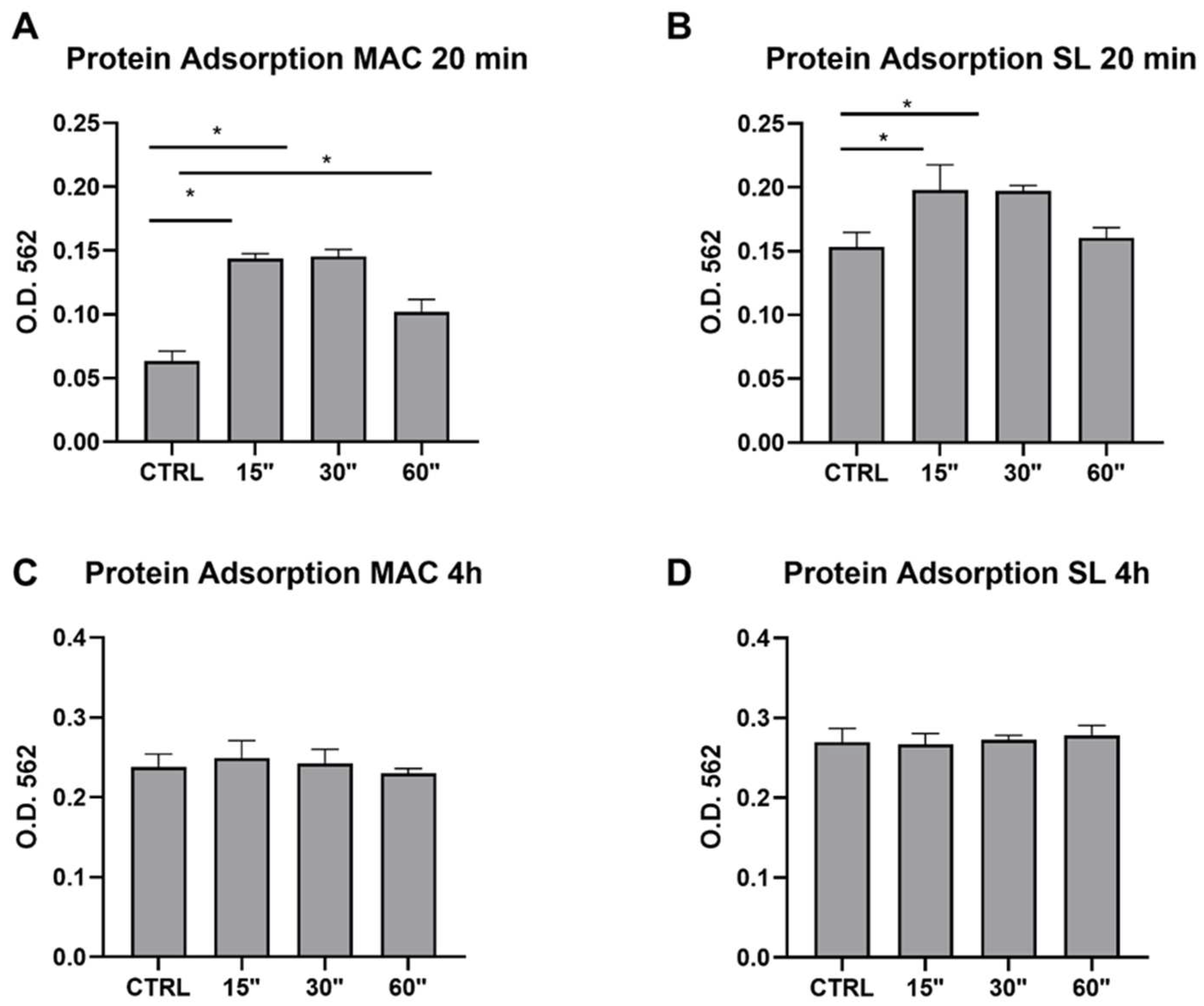
3.3. Protein Adsorption (Table 3)
| Protein Adsorption MAC 20 min | Protein Adsorption SL 20 min | ||||||
|---|---|---|---|---|---|---|---|
| Mean | Std. Dev. | p Value vs. CTRL | Mean | Std. Dev. | p Value vs. CTRL | ||
| CTRL | 0.06325 | 0.01584 | CTRL | 0.15325 | 0.022853 | ||
| 15″ | 0.1438 | 0.008614 | 0.0007 | 15″ | 0.198 | 0.039302 | 0.0282 |
| 30″ | 0.1454 | 0.0123 | 0.0008 | 30″ | 0.19725 | 0.008655 | 0.0326 |
| 60″ | 0.102 | 0.019374 | 0.285 | 60″ | 0.1605 | 0.01578 | 0.7756 |
| Protein adsorption MAC 4 h | Protein adsorption SL 4 h | ||||||
| Mean | Std. Dev. | p value vs. CTRL | Mean | Std. Dev. | p value vs. CTRL | ||
| CTRL | 0.238 | 0.027731 | CTRL | 0.269667 | 0.029501 | ||
| 15″ | 0.249333 | 0.03722 | 0.855 | 15″ | 0.267 | 0.023643 | 0.9636 |
| 30″ | 0.242667 | 0.030534 | 0.891 | 30″ | 0.272333 | 0.010263 | 0.855 |
| 60″ | 0.229667 | 0.011504 | 0.8193 | 60″ | 0.278667 | 0.020793 | 0.5526 |
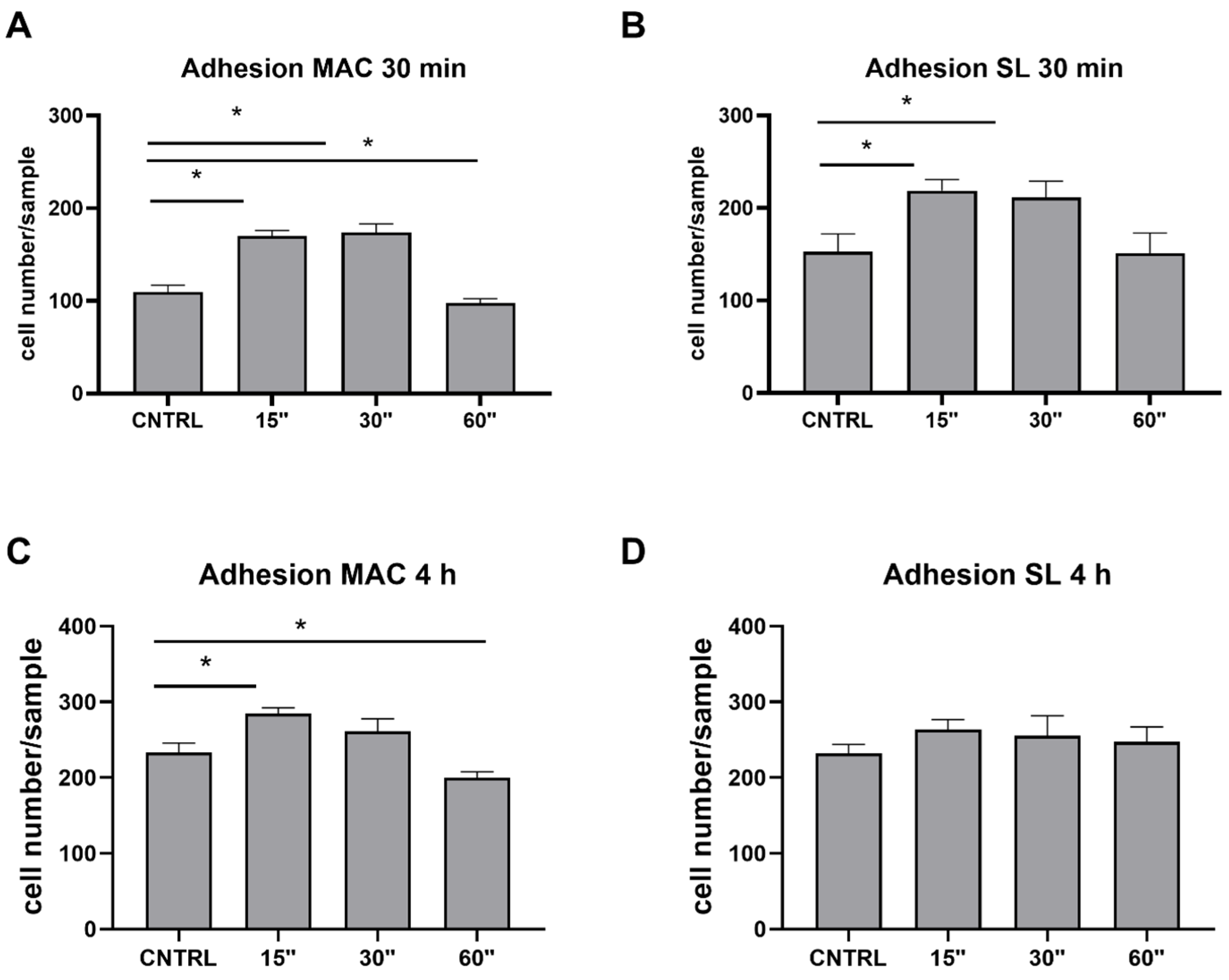
3.4. Cell Adhesion (Table 4)
| Adhesion MAC 30 min | Adhesion SL 30 min | ||||||
|---|---|---|---|---|---|---|---|
| Mean | Std. Dev. | p Value vs. CTRL | Mean | Std. Dev. | p Value vs. CTRL | ||
| CTRL | 109.6 | 16.16478 | CTRL | 152.5 | 39.128 | ||
| 15″ | 170 | 12.24745 | 0.0121 | 15″ | 218.75 | 24.12986 | 0.0109 |
| 30″ | 173.75 | 18.83923 | 0.0121 | 30″ | 211.25 | 35.84573 | 0.0335 |
| 60″ | 97.5 | 9.949874 | 0.6654 | 60″ | 151 | 44.29447 | 0.7647 |
| Adhesion MAC 4 h | Adhesion SL 4 h | ||||||
| Mean | Std. Dev. | p value vs. CTRL | Mean | Std. Dev. | p value vs. CTRL | ||
| CTRL | 233.5 | 24.90649 | CTRL | 232.25 | 23.27194 | ||
| 15″ | 284.75 | 15.6285 | 0.0392 | 15″ | 263.75 | 26.28529 | 0.1987 |
| 30″ | 261 | 33.33667 | 0.2437 | 30″ | 255.5 | 52.79836 | 0.4196 |
| 60″ | 200 | 15.40563 | 0.3698 | 60″ | 247 | 40.47221 | 0.4918 |
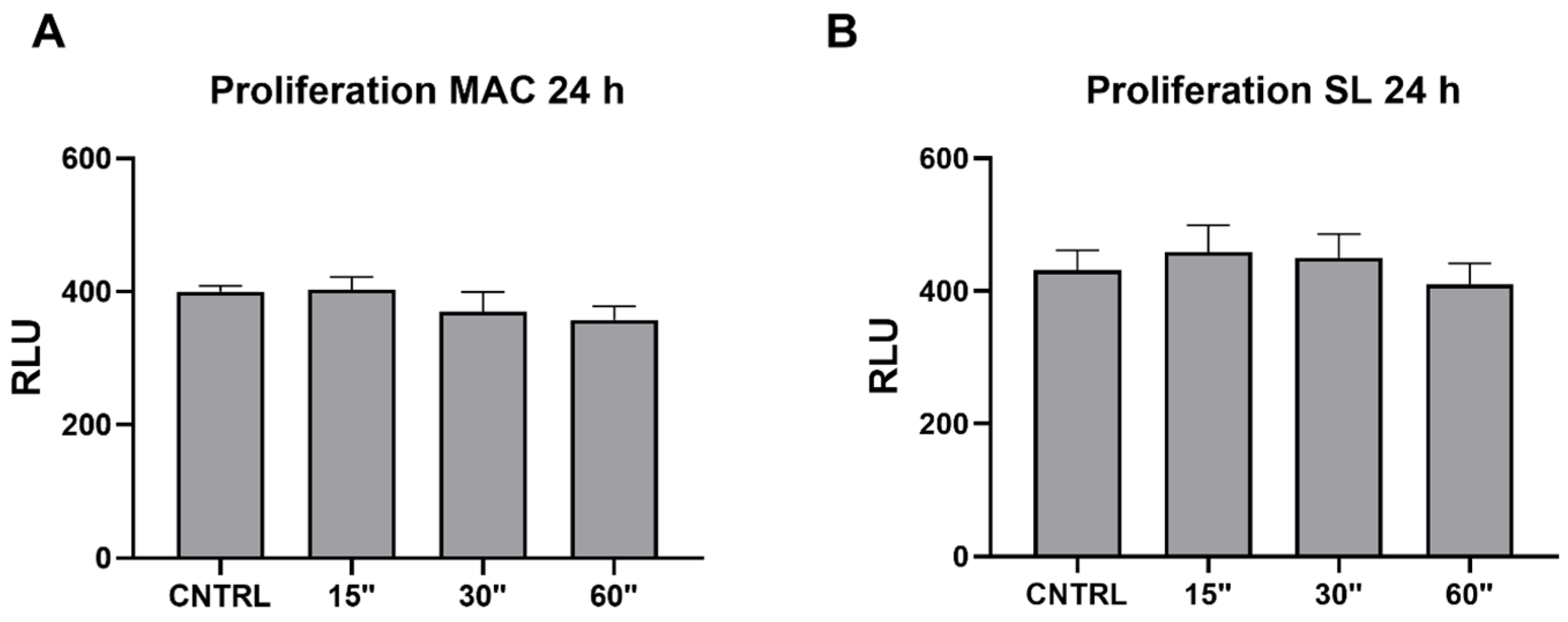
3.5. Viability (Table 5)
| Proliferation MAC 24 h | Proliferation SL 24 h | ||||||
|---|---|---|---|---|---|---|---|
| Mean | Std. Dev. | p Value vs. CTRL | Mean | Std. Dev. | p Value vs. CTRL | ||
| CTRL | 400.25 | 16.74067 | CTRL | 431.25 | 59.71809 | ||
| 15″ | 403 | 37.63863 | 0.9761 | 15″ | 458 | 81.25269 | 0.6326 |
| 30″ | 370 | 58.0804 | 0.4024 | 30″ | 449.5 | 72.8217 | 0.8111 |
| 60″ | 357.5 | 40.47633 | 0.1064 | 60″ | 410 | 63.35087 | 0.5501 |
| UV | 386.5 | 27.87472 | 0.5699 | UV | 413.25 | 35.10342 | 0.6757 |
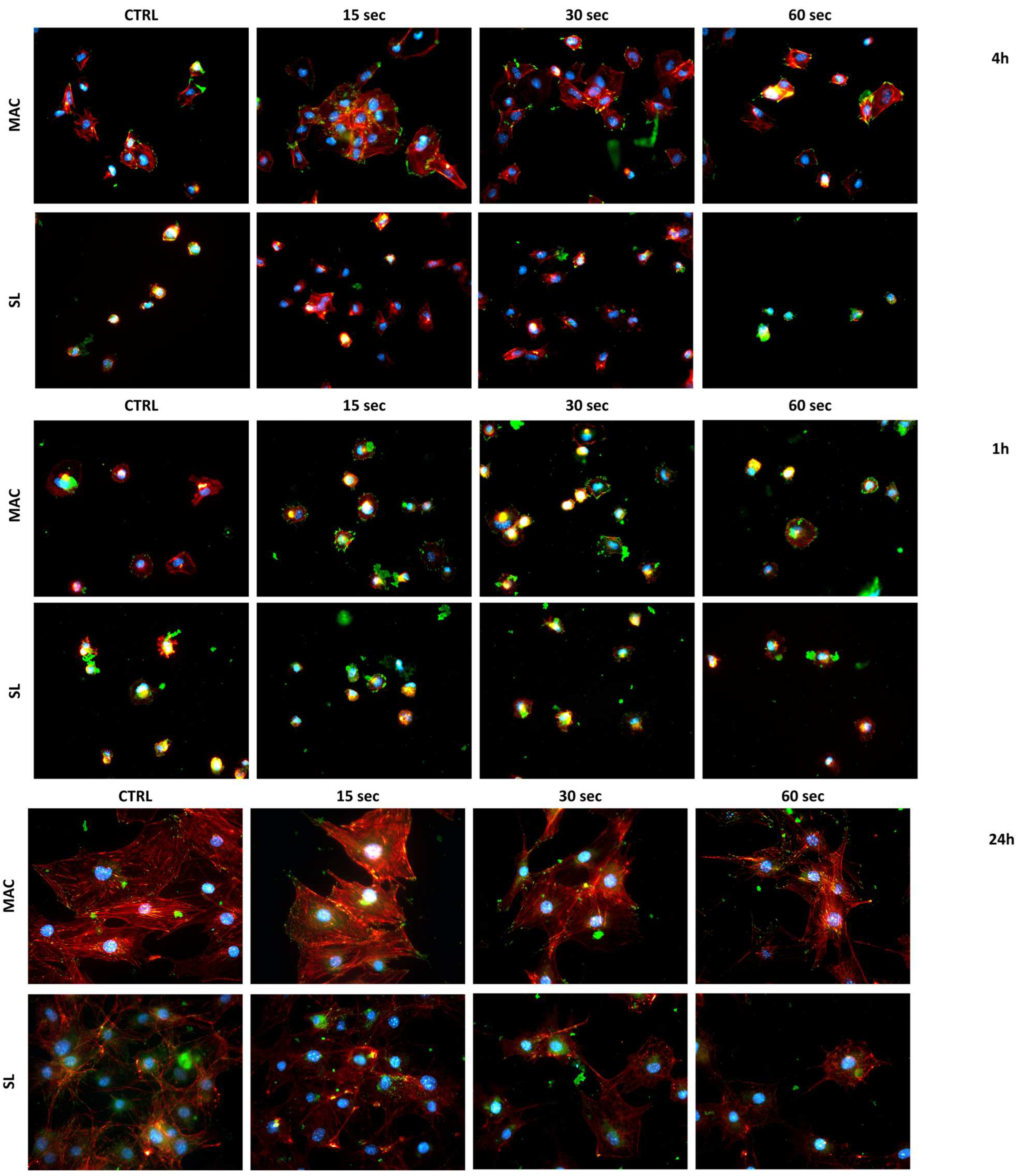
3.6. Cell Morphology
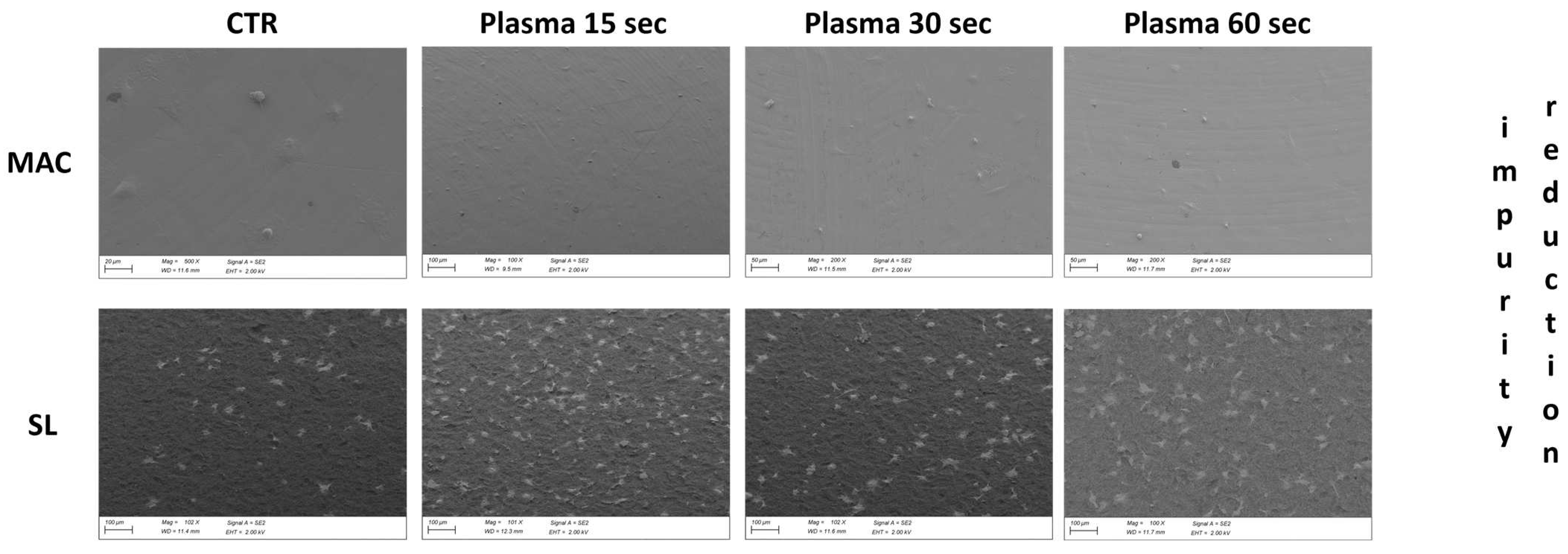
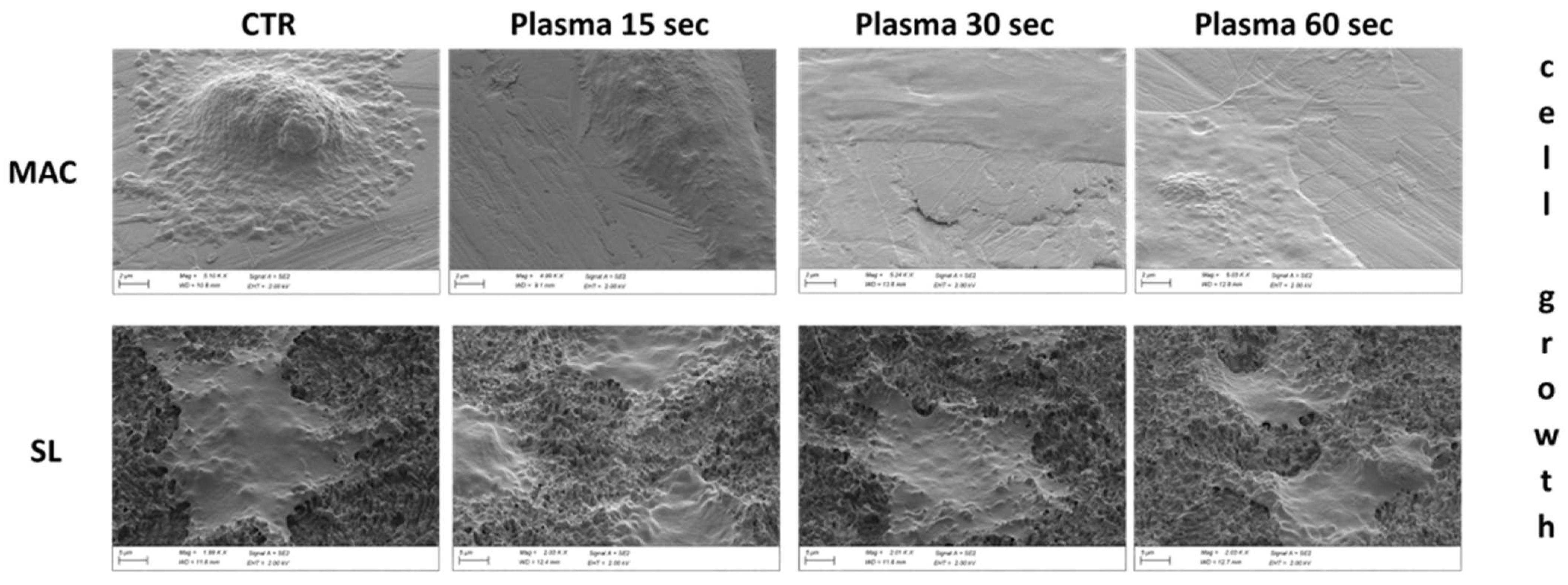
3.7. Cell Morphology at SEM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pommer, B.; Danzinger, M.; Leite Aiquel, L.; Pitta, J.; Haas, R. Long-term outcomes of maxillary single-tooth implants in relation to timing protocols of implant placement and loading: Systematic review and meta-analysis. Clin. Oral Implant. Res. 2021, 32 (Suppl. S21), 56–66. [Google Scholar] [CrossRef]
- Hermann, J.S.; Cochran, D.L.; Nummikoski, P.V.; Buser, D. Crestal bone changes around titanium implants. A radiographic evaluation of unloaded nonsubmerged and submerged implants in the canine mandible. J. Periodontol. 1997, 68, 1117–1130. [Google Scholar] [CrossRef]
- Lambrechts, T.; Doornewaard, R.; De Bruyckere, T.; Matthijs, L.; Deschepper, E.; Cosyn, J. A multicenter cohort study on the association of the one-abutment one-time concept with marginal bone loss around bone level implants. Clin. Oral Implant. Res. 2021, 32, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Hamudi, N.; Barnea, E.; Weinberg, E.; Laviv, A.; Mijiritsky, E.; Matalon, S.; Chaushu, L.; Kolerman, R. The association of the one-abutment at one-time concept with marginal bone loss around the SLA and platform switch conical abutment implants. J. Clin. Med. 2021, 11, 74. [Google Scholar] [CrossRef] [PubMed]
- Molina, A.; Sanz-Sánchez, I.; Martín, C.; Blanco, J.; Sanz, M. The effect of one-time abutment placement on interproximal bone levels and peri-implant soft tissues: A prospective randomized clinical trial. Clin. Oral Implants Res. 2017, 28, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Blazquez-Hinarejos, M.; Ayuso-Montero, R.; Jane-Salas, E.; Lopez-Lopez, J. Influence of surface modified dental implant abutments on connective tissue attachment: A systematic review. Arch. Oral Biol. 2017, 80, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Sabetrasekh, R.; Tiainen, H.; Reseland, J.E.; Will, J.; Ellingsen, J.E.; Lyngstadaas, S.P.; Haugen, H.J. Impact of trace elements on biocompatibility of titanium scaffolds. Biomed. Mater. 2010, 5, 015003. [Google Scholar] [CrossRef] [PubMed]
- Mehl, C.; Kern, M.; Zimmermann, A.; Harder, S.; Huth, S.; Selhuber-Unkel, C. Impact of Cleaning Procedures on Adhesion of Living Cells to Three Abutment Materials. Int. J. Oral Maxillofac. Implant. 2017, 32, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Choi, C.; Cha, Y.; Chang, J.S. The efficacy of convenient cleaning methods applicable for customized abutments: An in vitro study. BMC Oral Health 2021, 21, 78. [Google Scholar] [CrossRef]
- Mishra, P.K.; Wu, W.; Rozo, C.; Hallab, N.J.; Benevenia, J.; Gause, W.C. Micrometer-sized titanium particles can induce potent Th2-type responses through TLR4-independent pathways. J. Immunol. 2011, 187, 6491–6498. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Berglundh, T.; Lindhe, J. Soft tissue response to plaque formation at different implant systems. A comparative study in the dog. Clin. Oral Implants Res. 1998, 9, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, P.; Smeets, R.; Gosau, M.; Friedrich, R.E.; Madani, E.; Duddeck, D.; Fischer, C.; Tebbel, F.; Sader, R.; Hartjen, P. The Influence of an Ultrasonic Cleaning Protocol for CAD/CAM Abutment Surfaces on Cell Viability and Inflammatory Response In Vitro. In Vivo 2019, 33, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Cassinelli, C.; Götz, W.; Tarnow, D. Plasma of argon accelerates murine fibroblast adhesion in early stages of titanium disk colonization. Int. J. Oral Maxillofac. Implant. 2013, 28, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Vezeau, P.J.; Koorbusch, G.F.; Draughn, R.A.; Keller, J.C. Effects of multiple sterilization on surface characteristics and in vitro biologic responses to titanium. J. Oral Maxillofac. Surg. 1996, 54, 738–746.14. [Google Scholar] [CrossRef] [PubMed]
- Vezeau, P.J.; Keller, J.C.; Wightman, J.P. Reuse of Healing Abutments: An: In Vitro: Model of Plasma Cleaning and Common Sterilization Techniques. Implant Dent. 2000, 9, 236–246. [Google Scholar] [CrossRef]
- Corvino, E.; Pesce, P.; Mura, R.; Marcano, E.; Canullo, L. Influence of Modified Titanium Abutment Surface on Peri-implant Soft Tissue Behavior: A Systematic Review of In Vitro Studies. Int. J. Oral Maxillofac. Implant. 2020, 35, 503–519. [Google Scholar] [CrossRef] [PubMed]
- Garcia, B.; Camacho, F.; Peñarrocha, D.; Tallarico, M.; Perez, S.; Canullo, L. Influence of plasma cleaning procedure on the interaction between soft tissue and abutments: A randomized controlled histologic study. Clin. Oral Implants Res. 2017, 28, 1269–1277. [Google Scholar] [CrossRef]
- Lee, H.; Jeon, H.J.; Jung, A.; Kim, J.; Kim, J.Y.; Lee, S.H.; Kim, H.; Yeom, M.S.; Choe, W.; Gweon, B.; et al. Improvement of osseointegration efficacy of titanium implant through plasma surface teratment. Biomed. Eng. Lett. 2022, 12, 421–432. [Google Scholar] [CrossRef]
- Jeon, H.J.; Jung, A.; Kim, H.J.; Seo, J.S.; Kim, J.Y.; Yum, M.S.; Bomi, G.; Lim, Y. Enhanced Osteoblast Adhesion and Proliferation on Vacuum Plasma-Treated Implant Surface. Appl. Sci. 2022, 12, 9884. [Google Scholar] [CrossRef]
- Nevins, M.; Chen, C.Y.; Parma-Benfenati, S.; Kim, D.M. Gas Plasma Treatment Improves Titanium Dental Implant Osseointegration—A Preclinical In Vivo Experimental Study. Bioengineering 2023, 10, 1181. [Google Scholar] [CrossRef]
- Canullo, L.; Genova, T.; Pesce, P.; Nakajima, Y.; Yonezawa, D.; Mussano, F. Surface bio-functionalization using plasma of argon 486 could alter microbiological and topographic surface analysis of dental implants. Ann. Anat. 2020, 230, 151489. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.C.M.; Sordi, M.B.; Kanazawa, M.; Ravindran, S.; Henriques, B.; Silva, F.S.; Aparicio, C.; Cooper, L.F. Nano-scale modification of titanium implant surfaces to enhance osseointegration. Acta Biomater. 2019, 94, 112–131. [Google Scholar] [CrossRef] [PubMed]
- Mussano, F.; Genova, T.; Laurenti, M. Beta1-integrin and TRPV4 are involved in osteoblast adhesion to different titanium surface topographies. Appl. Surf. Sci. 2020, 507, 145112. [Google Scholar] [CrossRef]
- Canullo, L.; Penarrocha Oltra, D.; Pesce, P.; Zarauz, C.; Lattanzio, R.; Penarrocha Diago, M.; Iezzi, G. Soft tissue integration of different abutment surfaces: An experimental study with histological analysis. Clin. Oral. Implants Res. 2021, 32, 928–940. [Google Scholar] [CrossRef]
- Sculean, A.; Gruber, R.; Bosshardt, D.D. Soft tissue wound healing around teeth and dental implants. J. Clin. Periodontol. 2014, 41 (Suppl. S15), S6–S22. [Google Scholar] [CrossRef]
- Kim, M.C.; Yang, S.H.; Boo, J.-H.; Han, J.G. Surface treatment of metals using an atmospheric pressure plasma jet and their surface characteristics. Surf. Coat. Technol. 2003, 174, 839–844. [Google Scholar] [CrossRef]








| MAC | SL | |||||||
|---|---|---|---|---|---|---|---|---|
| CTRL | 15″ | 30″ | 60″ | CTRL | 15″ | 30″ | 60″ | |
| Temperature in °C | 25 | 39 | 47 | 51 | 25 | 39 | 46 | 50 |
| Seconds to 37 °C | 60 | 90 | 102 | 60 | 88 | 99 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canullo, L.; Genova, T.; Chinigò, G.; Iacono, R.; Pesce, P.; Menini, M.; Mussano, F. Vacuum Plasma Treatment Device for Enhancing Fibroblast Activity on Machined and Rough Titanium Surfaces. Dent. J. 2024, 12, 71. https://doi.org/10.3390/dj12030071
Canullo L, Genova T, Chinigò G, Iacono R, Pesce P, Menini M, Mussano F. Vacuum Plasma Treatment Device for Enhancing Fibroblast Activity on Machined and Rough Titanium Surfaces. Dentistry Journal. 2024; 12(3):71. https://doi.org/10.3390/dj12030071
Chicago/Turabian StyleCanullo, Luigi, Tullio Genova, Giorgia Chinigò, Roberta Iacono, Paolo Pesce, Maria Menini, and Federico Mussano. 2024. "Vacuum Plasma Treatment Device for Enhancing Fibroblast Activity on Machined and Rough Titanium Surfaces" Dentistry Journal 12, no. 3: 71. https://doi.org/10.3390/dj12030071