
In Vitro Risk Assessment of Dental Acid Erosion Caused by Long-Term Exposure to Oral Liquid Bandages


Abstract
:1. Introduction
2. Materials and Methods
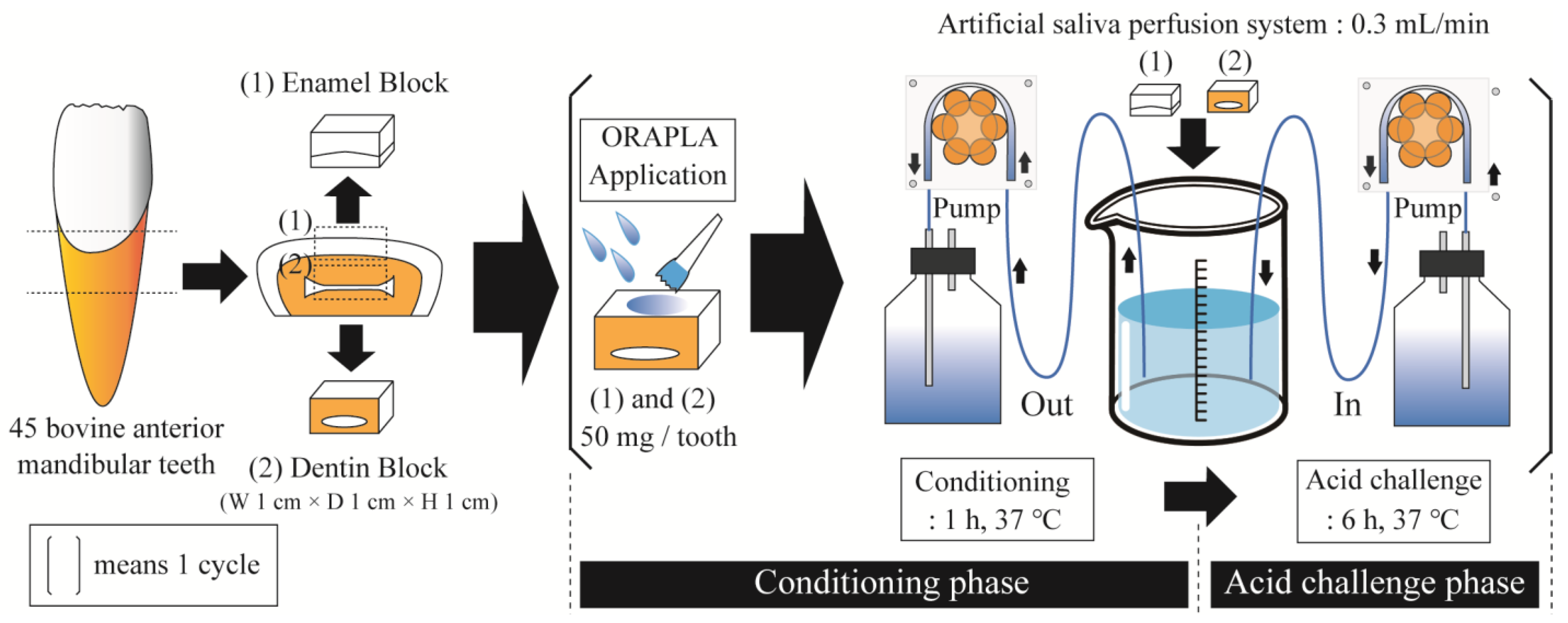
2.1. Preparation of Enamel and Dentin Samples
2.2. Acid Challenge Experiment with Artificial Salivary Circulation
2.3. 3D Laser Microscopy
2.4. Micro-Vickers Hardness Measurement
2.5. Cross-Section and Surface Morphology by Scanning Electron Microscopy (SEM)
2.6. Statistical Analysis
3. Results
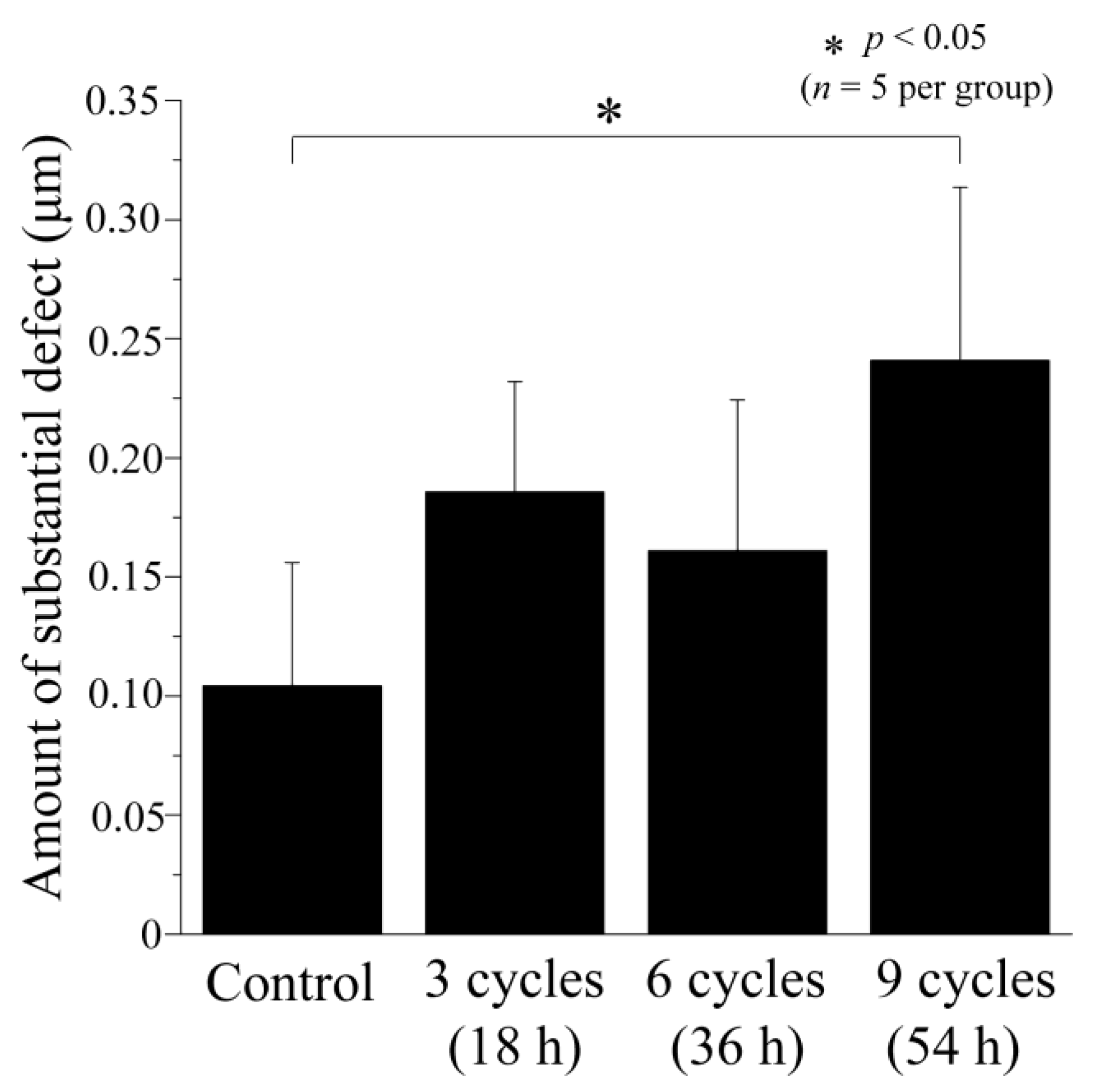
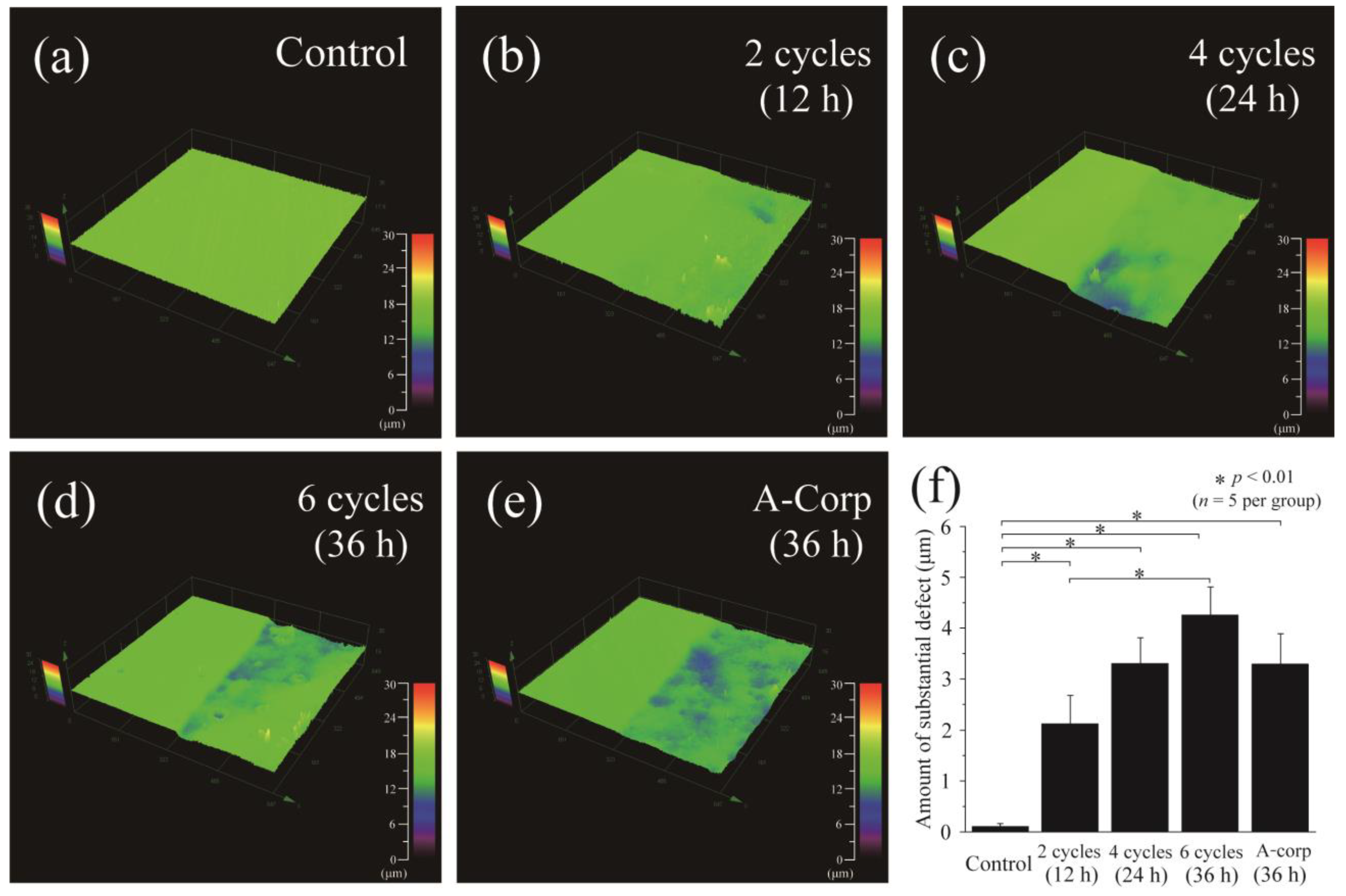
3.1. Step Height Profiles after Acid Challenge: Enamel
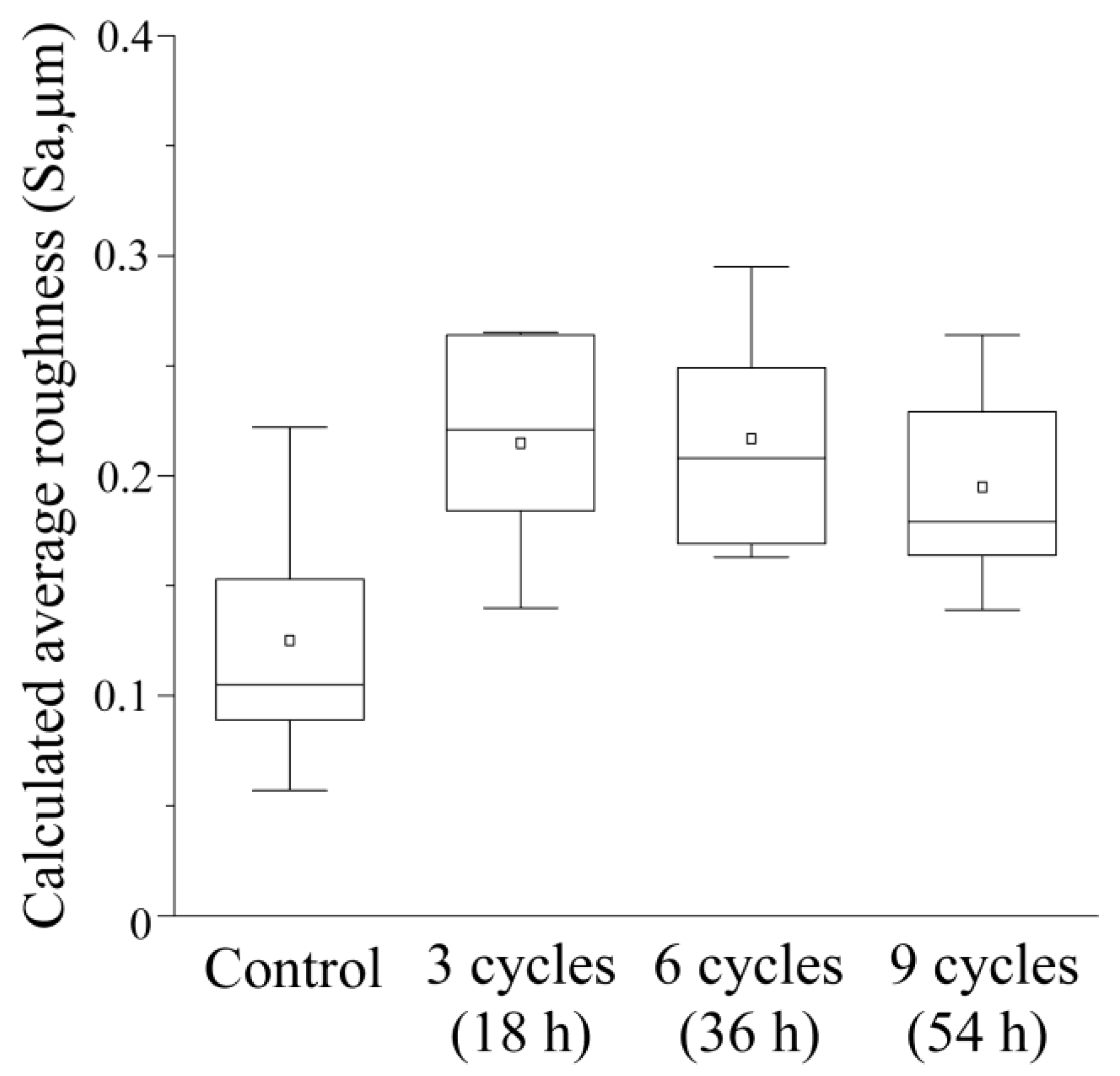
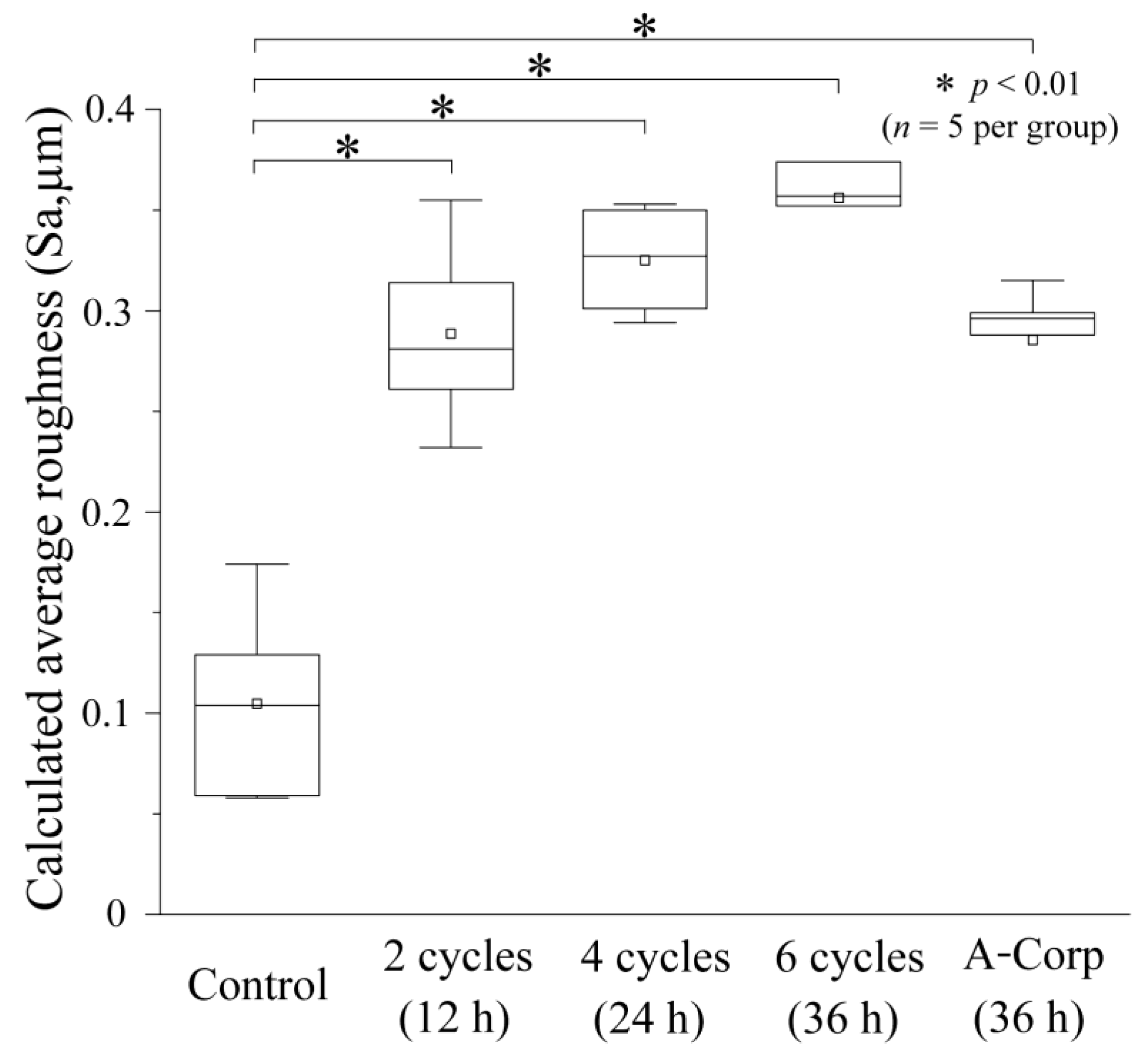
3.2. Average Roughness (Sa) after Acid Challenge: Enamel
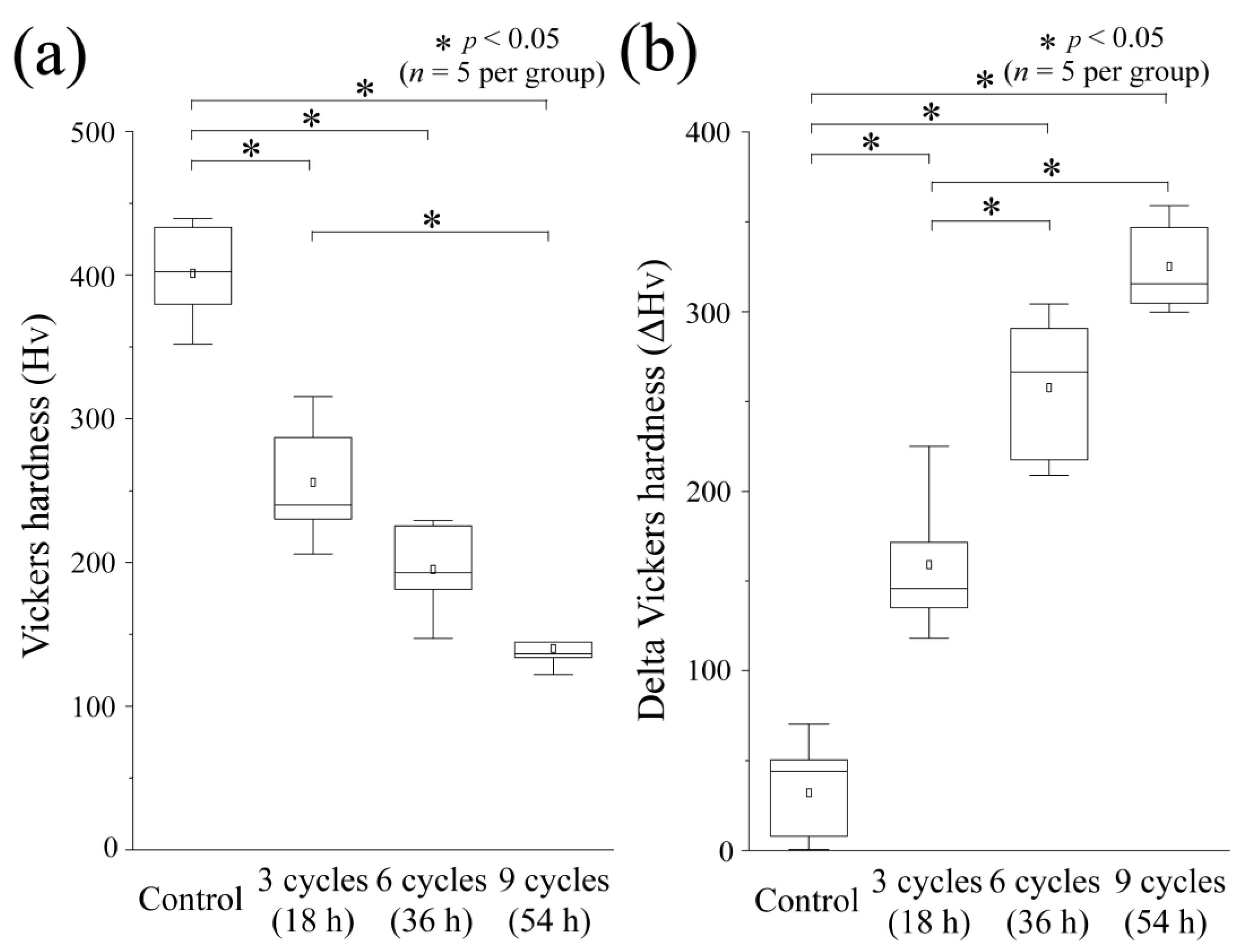
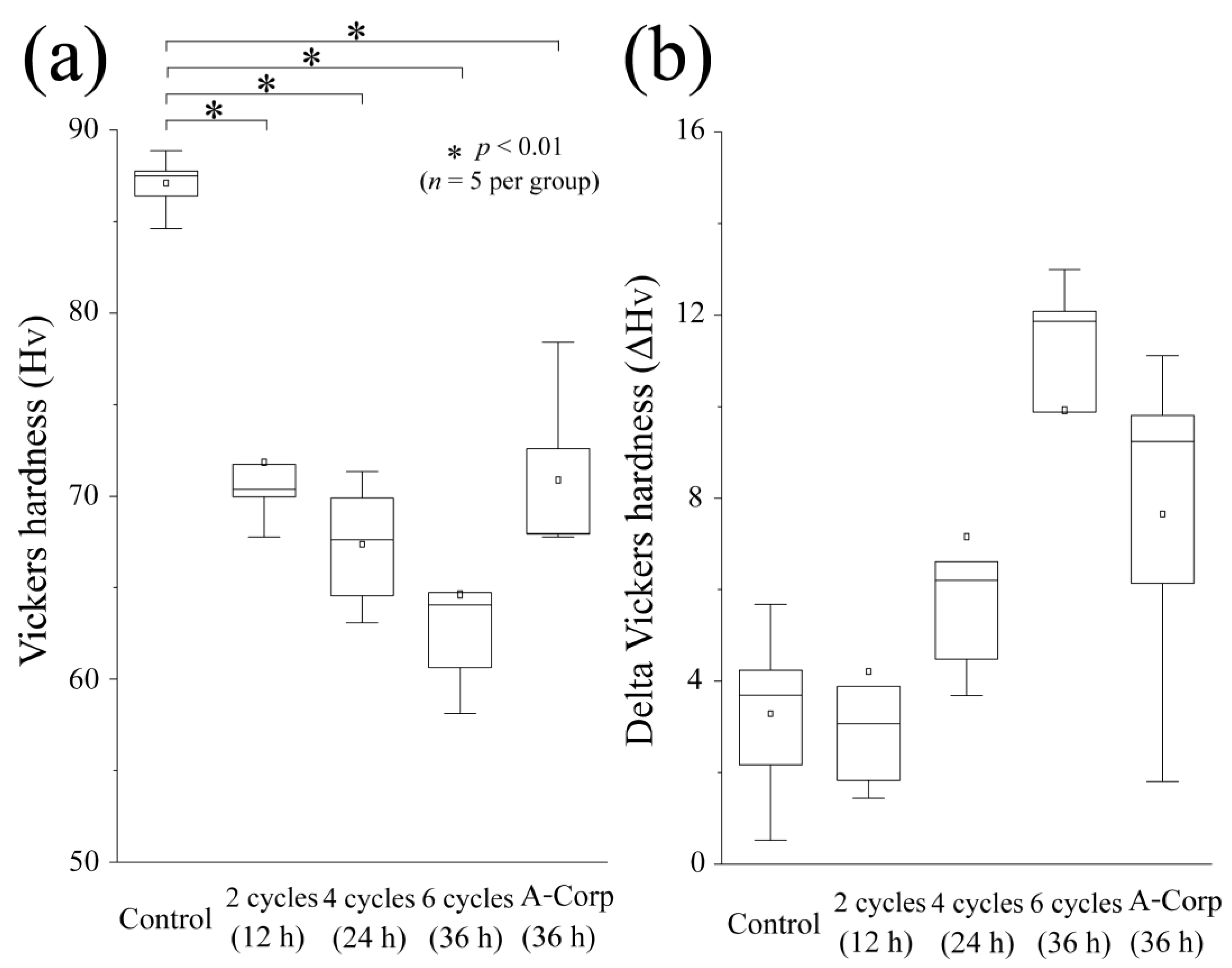
3.3. Vickers Hardness and Its Changes after Acid Challenge: Enamel
3.4. Step Height Profiles after Acid Challenge: Dentin
3.5. Average Roughness after Acid Challenge: Dentin
3.6. Vickers Hardness and Its Changes after Acid Challenge: Dentin
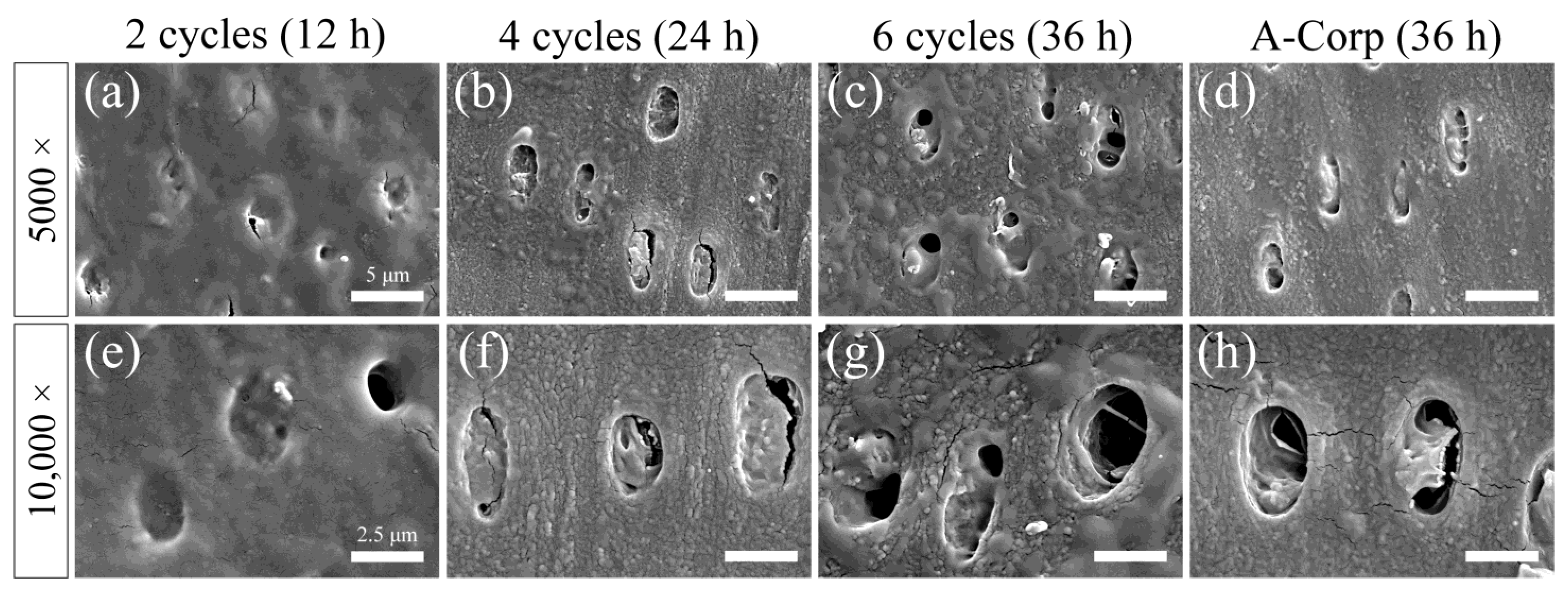
3.7. Surface SEM Observations after Acid Challenge: Dentin
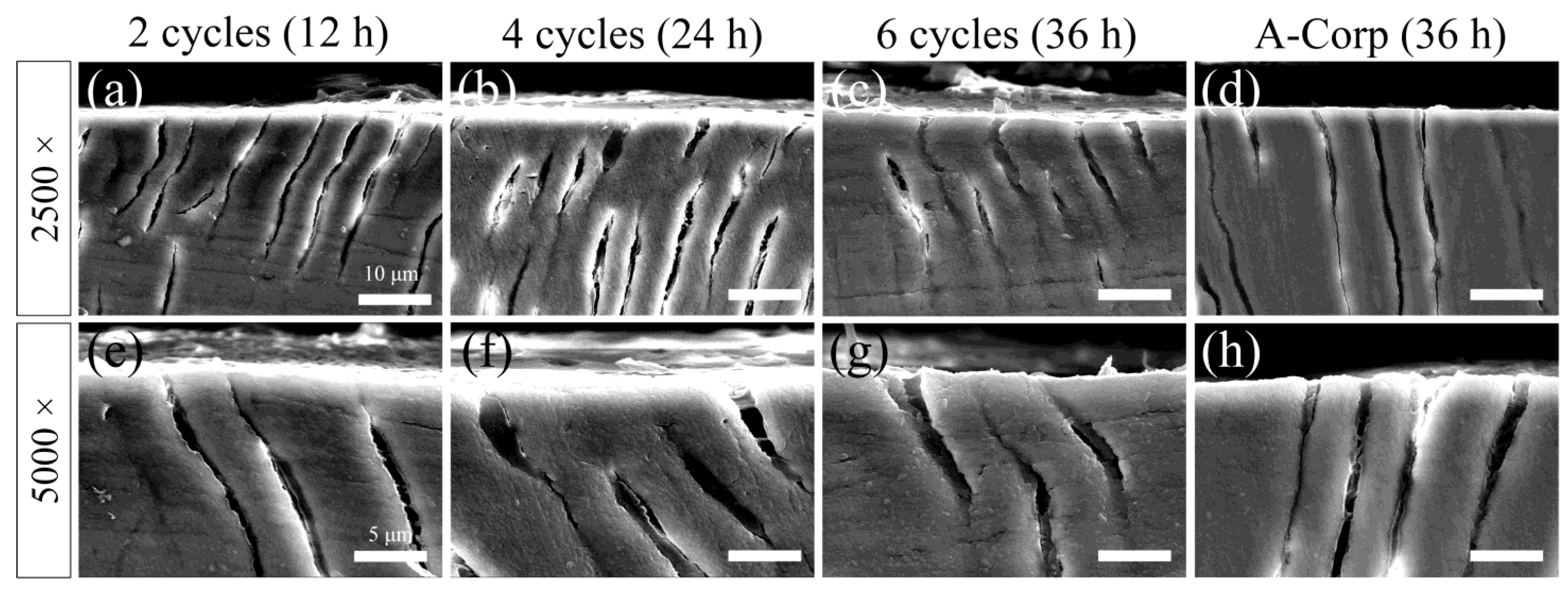
3.8. Cross-Sectional SEM Observations after Acid Challenge: Dentin
4. Discussion
4.1. Assessment of Dental Erosion Risk: Enamel
4.2. Risk Assessment of Dental Erosion: Dentin
4.3. Limitations and Generalizability to the Human Oral Environment
4.4. Future Directions
4.5. Benefits and Clinical Dental Applications of Oral Liquid Bandages
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lussi, A.; Jaeggi, T.; Scharer, S. The influence of different factors on in vitro enamel erosion. Caries Res. 1993, 27, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Horvat Aleksijević, L.; Prpić, J.; Muhvić Urek, M.; Pezelj-Ribarić, S.; Ivančić-Jokić, N.; Peršić Bukmir, R.; Aleksijević, M.; Glažar, I. Oral mucosal lesions in childhood. Dent. J. 2022, 10, 214. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Sonis, S.; Diz, P.D. Oral mucositis. Oral Dis. 2006, 12, 229–241. [Google Scholar] [CrossRef]
- Saikaly, S.K.; Saikaly, T.S.; Saikaly, L.E. Recurrent aphthous ulceration: A review of potential causes and novel treatments. J. Dermatolog. Treat. 2018, 29, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.G.; Cohen, D.M.; Clark, A.N. Ulcerated lesions of the oral mucosa: Clinical and histologic review. Head Neck Pathol. 2019, 13, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Pulito, C.; Cristaudo, A.; Porta, C.L.; Zapperi, S.; Blandino, G.; Morrone, A.; Strano, S. Oral mucositis: The hidden side of cancer therapy. J. Exp. Clin. Cancer Res. 2020, 39, 210. [Google Scholar] [CrossRef] [PubMed]
- Bardellini, E.; Veneri, F.; Amadori, F.; Conti, G.; Majorana, A. Photobiomodulation therapy for the management of recurrent aphthous stomatitis in children: Clinical effectiveness and parental satisfaction. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e549–e553. [Google Scholar] [CrossRef]
- Bakshi, S.S.; Bakshi, S. Recurrent aphthous stomatitis. Arch. Med. Health Sci. 2019, 7, 317. [Google Scholar] [CrossRef]
- Gendreau, L.; Loewy, Z.G. Epidemiology and etiology of denture stomatitis. J. Prosthodont. 2011, 20, 251–260. [Google Scholar] [CrossRef]
- Keefe, D.M.; Schubert, M.M.; Elting, L.S.; Sonis, S.T.; Epstein, J.B.; Raber-Durlacher, J.E.; Migliorati, C.A.; McGuire, D.B.; Hutchins, R.D.; Peterson, D.E.; et al. Updated clinical practice guidelines for the prevention and treatment of mucositis. Cancer 2007, 109, 820–831. [Google Scholar] [CrossRef]
- Clinical Practice Guideline, the Japanese Orthodontic Society. Available online: https://www.jos.gr.jp/guideline (accessed on 10 August 2023).
- Daugėlaitė, G.; Užkuraitytė, K.; Jagelavičienė, E.; Filipauskas, A. Prevention and treatment of chemotherapy and radiotherapy induced oral mucositis. Medicina 2019, 55, 25. [Google Scholar] [CrossRef] [PubMed]
- Madani, F.M.; Kuperstein, A.S. Normal variations of oral anatomy and common oral soft tissue lesions: Evaluation and management. Med. Clin. N. Am. 2014, 98, 1281–1298. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; Lee, H.E.; Ro, Y.S.; Lee, C.W. Three cases of “morsicatio labiorum”. Ann. Dermatol. 2012, 24, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Kuddushi, M.; Shah, A.A.; Ayranci, C.; Zhang, X. Recent advances in novel materials and techniques for developing transparent wound dressings. J. Mater. Chem. B 2023, 11, 6201–6224. [Google Scholar] [CrossRef] [PubMed]
- Samuels, N.; Saffer, A.; Wexler, I.D.; Oberbaum, M. Localized reduction of gingival inflammation using site-specific therapy with a topical gingival patch. J. Clin. Dent. 2012, 23, 64–67. [Google Scholar] [PubMed]
- Nishimura, F.; Okazaki, K.; Kono, Y.; Komori, K.; Nomoto, S. Compressive behavior and micro Vickers hardness of human enamel and dentin. J. Jpn. Soc. Dent. Mater. Devices 1986, 5, 449–454. [Google Scholar] [CrossRef]
- Benjakul, P.; Chuenarrom, C. Association of dental enamel loss with the PH and titratable acidity of beverages. J. Dent. Sci. 2011, 6, 129–133. [Google Scholar] [CrossRef]
- Wang, Y.L.; Chang, C.C.; Chi, C.W.; Chang, H.H.; Chiang, Y.C.; Chuang, Y.C.; Chang, H.H.; Huang, G.F.; Liao, Y.S.; Lin, C.P. Erosive potential of soft drinks on human enamel: An in vitro study. J. Formos. Med. Assoc. 2014, 113, 850–856. [Google Scholar] [CrossRef]
- Dugmore, C.R.; Rock, W.P. A multifactorial analysis of factors associated with dental erosion. Br. Dent. J. 2004, 196, 283–286; discussion 273. [Google Scholar] [CrossRef]
- Lussi, A.; Jaeggi, T. Erosion—Diagnosis and risk factors. Clin. Oral Investig. 2008, 12 (Suppl. S1), S5–S13. [Google Scholar] [CrossRef]
- Lussi, A.; Carvalho, T.S. Erosive tooth wear: A multifactorial condition of growing concern and increasing knowledge. Erosive Tooth Wear 2014, 25, 1–15. [Google Scholar] [CrossRef]
- Humphrey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow, and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef]
- Amano, O.; Mizobe, K.; Bando, Y.; Sakiyama, K. Anatomy and histology of rodent and human major salivary glands: -overview of the Japan salivary gland society-sponsored workshop-. Acta Histochem. Cytochem. 2012, 45, 241–250. [Google Scholar] [CrossRef]
- Dawes, C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in Man. J. Dent. Res. 1987, 66, 648–653. [Google Scholar] [CrossRef]
- Lussi, A.; Schlueter, N.; Rakhmatullina, E.; Ganss, C. Dental erosion—An overview with emphasis on chemical and histopathological aspects. Caries Res. 2011, 45 (Suppl. 1), 2–12. [Google Scholar] [CrossRef]
- Buonocore, M.G. Dissolution rates of enamel and dentin in acid buffers. J. Dent. Res. 1961, 40, 561–570. [Google Scholar] [CrossRef]
- Carpenter, G.; Cotroneo, E.; Moazzez, R.; Rojas-Serrano, M.; Donaldson, N.; Austin, R.; Zaidel, L.; Bartlett, D.; Proctor, G. Composition of enamel pellicle from dental erosion patients. Caries Res. 2014, 48, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Good, N.E.; Winget, G.D.; Winter, W.; Connolly, T.N.; Izawa, S.; Singh, R.M. Hydrogen ion buffers for biological research. Biochemistry 1966, 5, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Llena-Puy, C. The rôle of saliva in maintaining Oral Health and as an aid to diagnosis. Med. Oral Patol. Oral Cir. Bucal 2006, 11, E449–E455. [Google Scholar]
- Mazzoleni, S.; Gargani, A.; Parcianello, R.G.; Pezzato, L.; Bertolini, R.; Zuccon, A.; Stellini, E.; Ludovichetti, F.S. Protection against dental erosion and the remineralization capacity of non-fluoride toothpaste, fluoride toothpaste and fluoride varnish. Appl. Sci. 2023, 13, 1849. [Google Scholar] [CrossRef]
- Wiegand, A.; Attin, T. Influence of fluoride on the prevention of erosive lesions—A review. Oral Health Prev. Dent. 2003, 1, 245–253. [Google Scholar]
- Schlueter, N.; Klimek, J.; Ganss, C. Efficacy of tin-containing solutions on erosive mineral loss in enamel and dentine in situ. Clin. Oral Investig. 2011, 15, 361–367. [Google Scholar] [CrossRef]
- Whelton, H.P.; Spencer, A.J.; Do, L.G.; Rugg-Gunn, A.J. Fluoride revolution and dental caries: Evolution of policies for global use. J. Dent. Res. 2019, 98, 837–846. [Google Scholar] [CrossRef]
- ten Cate, J.M.; Duijsters, P.P. Influence of fluoride in solution on tooth demineralization. I. Chemical Data. Caries Res. 1983, 17, 193–199. [Google Scholar] [CrossRef] [PubMed]
- ten Cate, J.M.; Duijsters, P.P.E. Influence of fluoride in solution on tooth demineralization. II. Microradiographical Data. Caries Res. 1983, 17, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Youichi, I.; Mitsumasa, T.; Masato, M.; Tsuyoshi, K.; Yoshinori, T. Distribution of Flunoride in human enamel surfaces (III). J. Dent. Health 1980, 30, 371–375. [Google Scholar] [CrossRef]
- Buzalaf, M.A.R.; Hannas, A.R.; Kato, M.T. Saliva and dental erosion. J. Appl. Oral Sci. 2012, 20, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Suh, K.I.; Lee, J.Y.; Chung, J.W.; Kim, Y.K.; Kho, H.S. Relationship between salivary flow rate and clinical symptoms and behaviours in patients with dry mouth. J. Oral Rehabil. 2007, 34, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Moreno, G.; Cabrera-Ayala, M.; Aguilar-Salvatierra, A.; Guardia, J.; Ramírez-Fernández, M.P.; González-Jaranay, M.; Calvo-Guirado, J.L. Evaluation of the efficacy of a topical sialogogue spray containing malic acid 1% in elderly people with xerostomia: A double-blind, randomized clinical trial. Gerodontology 2014, 31, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Scaramucci, T.; Borges, A.B.; Lippert, F.; Frank, N.E.; Hara, A.T. Sodium fluoride effect on erosion–abrasion under Hyposalivatory simulating conditions. Arch. Oral Biol. 2013, 58, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Satou, R.; Yamagishi, A.; Takayanagi, A.; Suzuki, S.; Birkhed, D.; Sugihara, N. Comparison of interproximal delivery and flow characteristics by dentifrice dilution and application of prepared toothpaste delivery technique. PLoS ONE 2022, 17, e0276227. [Google Scholar] [CrossRef] [PubMed]
- Baran, I.; Nalçacı, R. Self-reported denture hygiene habits and oral tissue conditions of complete denture wearers. Arch. Gerontol. Geriatr. 2009, 49, 237–241. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | pH | Amount Use | Composition |
|---|---|---|---|
| ORAPLA (Experimental drug) | 4.67 | 300 mg | Carboxyvinyl polymer (acidic causative agent), Gelled hydrocarbon, Sodium alginate, Aluminium lactate |
| A-Corp (Anonymous, over-the-counter drug) | 5.58 | 300 mg | Carboxyvinyl polymer (acidic causative agent), Gelled hydrocarbon, Xylitol, Hypromellose, L-Menthol |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satou, R.; Sugihara, N. In Vitro Risk Assessment of Dental Acid Erosion Caused by Long-Term Exposure to Oral Liquid Bandages. Dent. J. 2024, 12, 70. https://doi.org/10.3390/dj12030070
Satou R, Sugihara N. In Vitro Risk Assessment of Dental Acid Erosion Caused by Long-Term Exposure to Oral Liquid Bandages. Dentistry Journal. 2024; 12(3):70. https://doi.org/10.3390/dj12030070
Chicago/Turabian StyleSatou, Ryouichi, and Naoki Sugihara. 2024. "In Vitro Risk Assessment of Dental Acid Erosion Caused by Long-Term Exposure to Oral Liquid Bandages" Dentistry Journal 12, no. 3: 70. https://doi.org/10.3390/dj12030070