

Materials and Applications of 3D Printing Technology in Dentistry: An Overview

Abstract
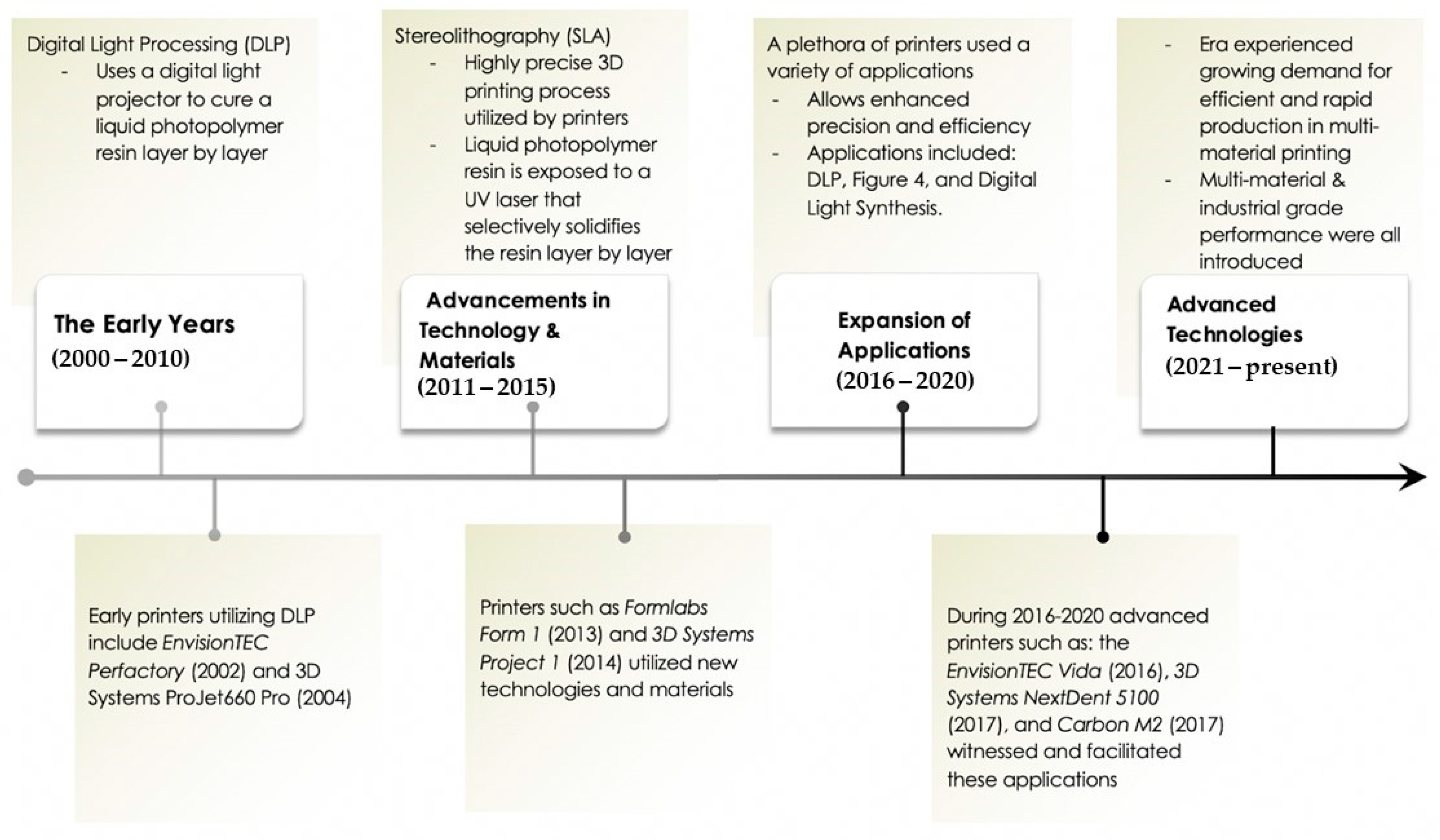
:1. Introduction
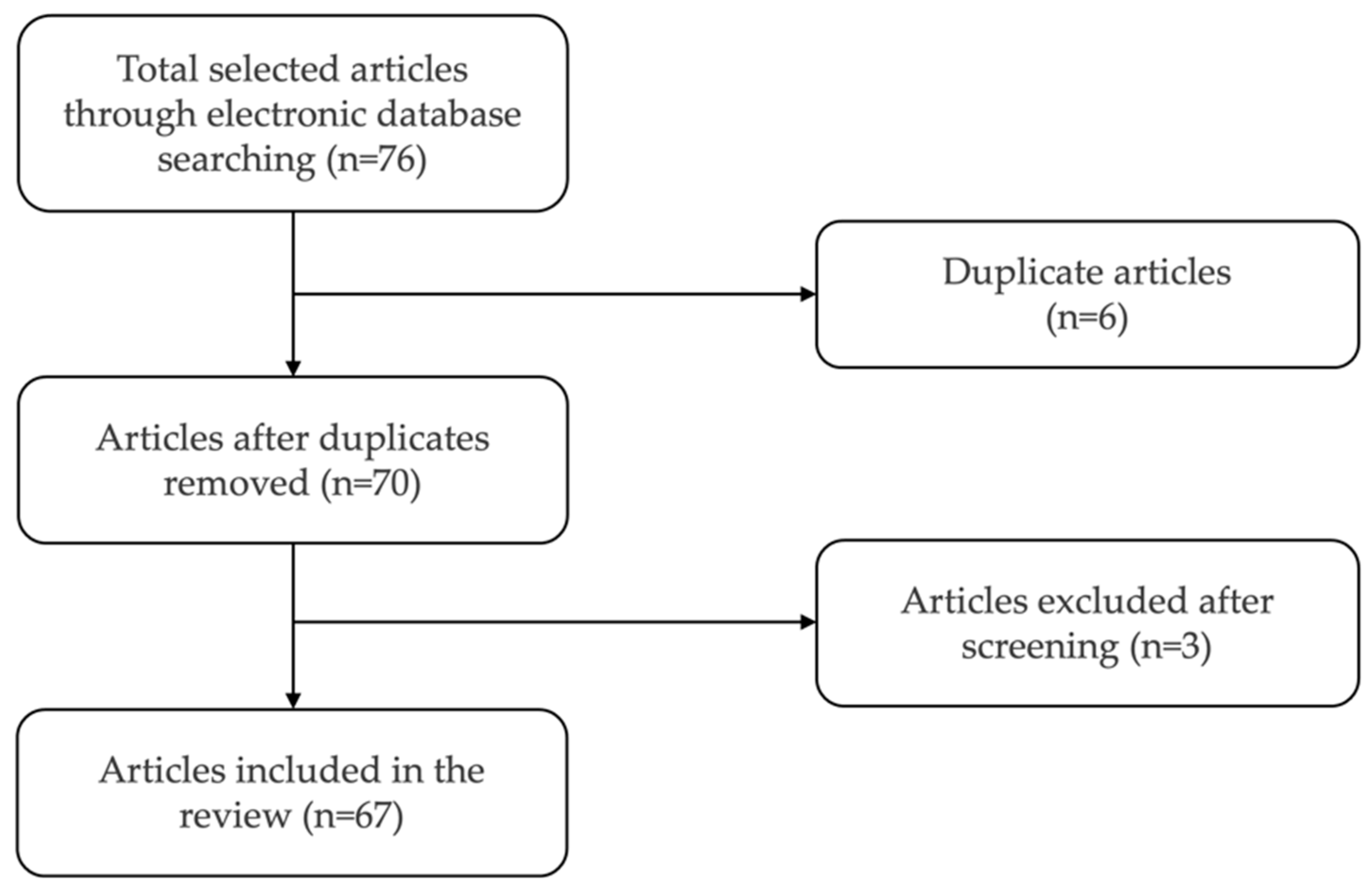
2. Methods
3. Three-Dimensional Printing Technologies
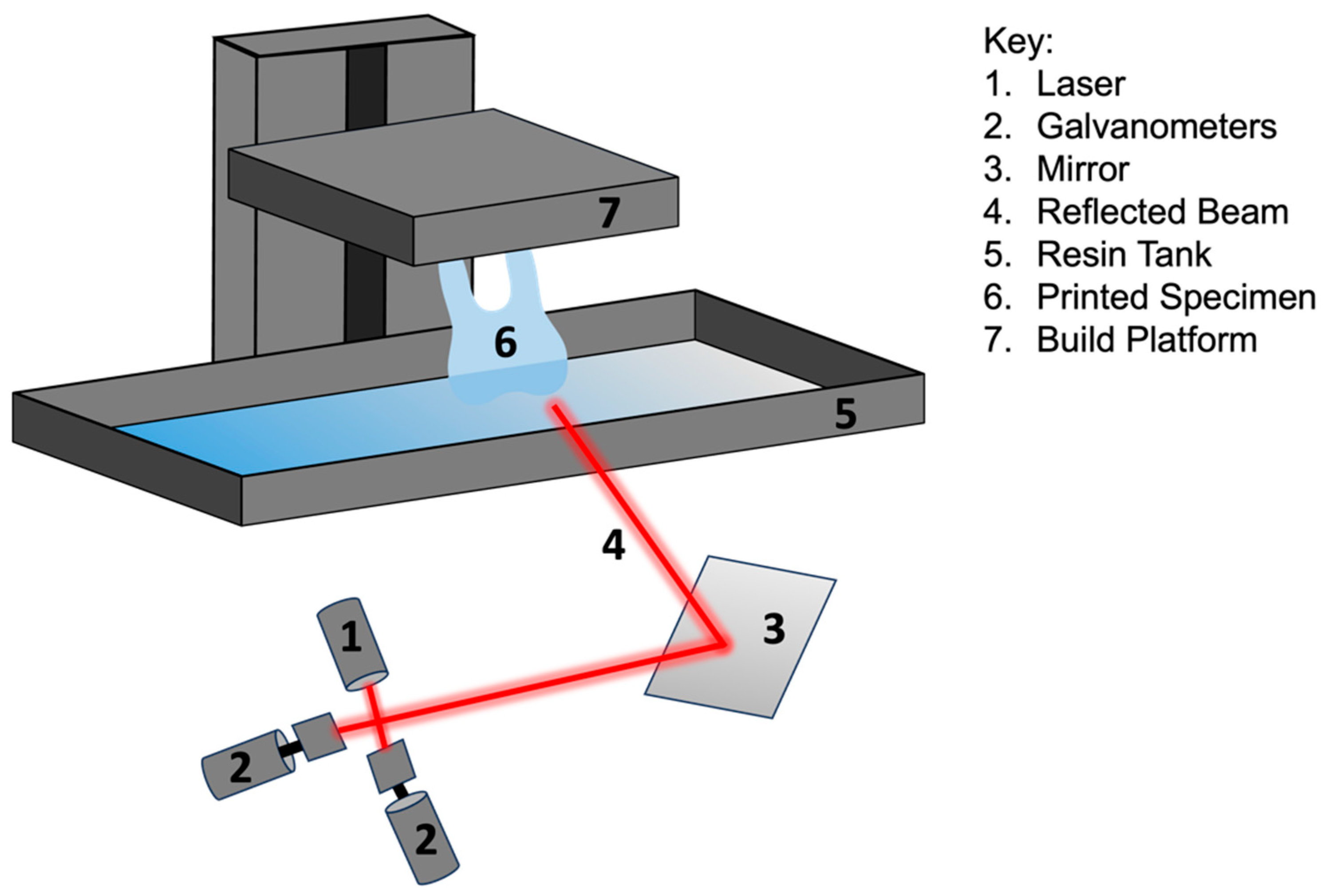
3.1. Stereolithography (SLA)
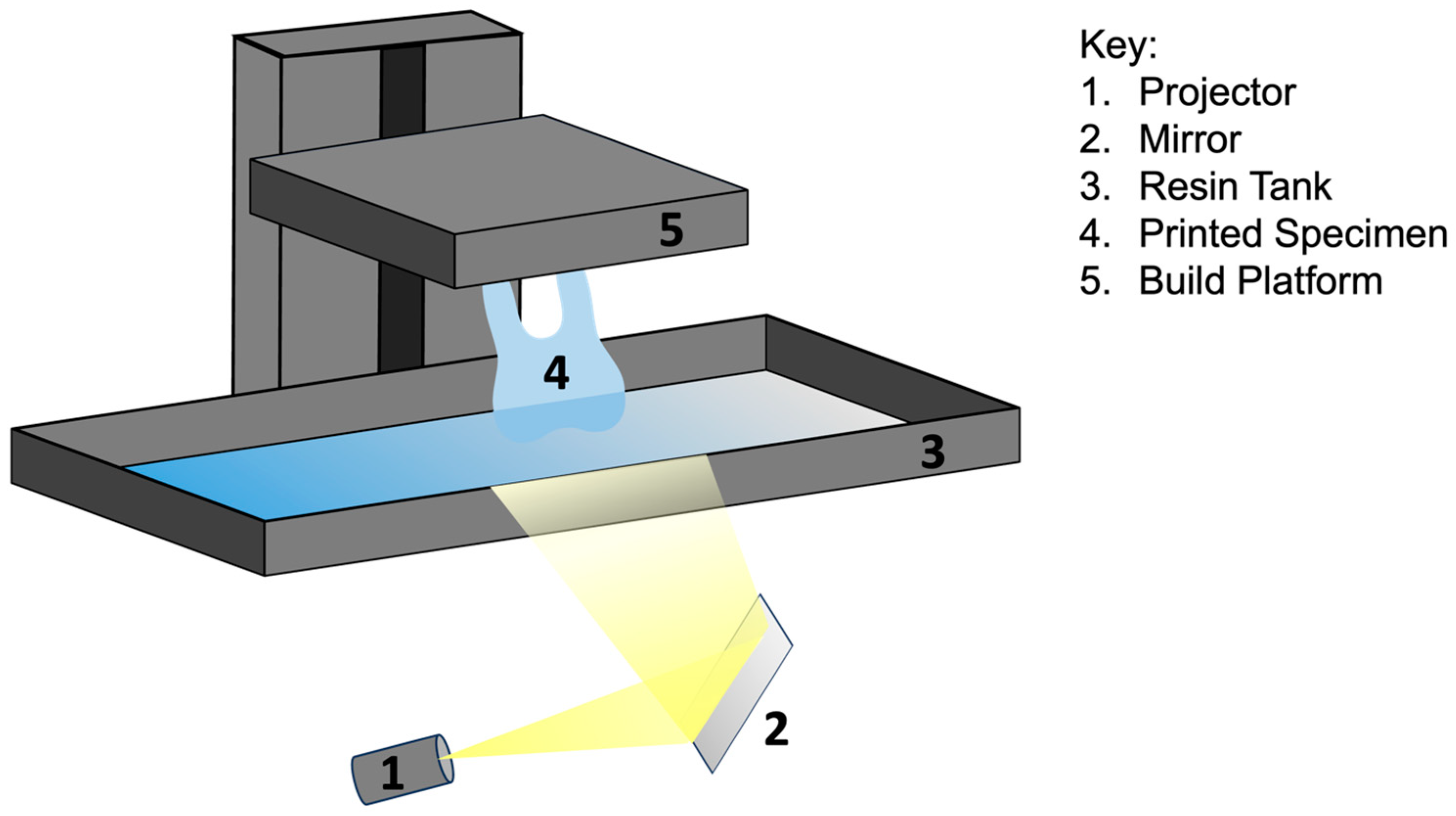
3.2. Digital Light Processing (DLP)
3.3. Fused Deposition Modeling (FMD)
3.4. Selective Laser Sintering (SLS)
3.5. Photopolymer Jetting
3.6. Powder Binder Jetting
3.7. Laser Bioprinting (LAB)
4. Dental Materials in 3D Print Technology
4.1. Synthetic Polymers
4.2. Metals
4.3. Ceramics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Density (g/cm3) | Martens Hardness (N/mm2) | Vickers Hardness (GPa) | Tensile Strength (MPa) | Elastic Modulus (GPa) | Bending Strength (MPa) |
|---|---|---|---|---|---|---|
| Cortical bone * [30] | 1.92 | NP | NP | 104–121 | 6–30 | 225 |
| Dentin * [30] | NP | 468.2 ± 30.8 | NP | 104 | 12–18.6 | NP |
| Dental enamel [30] | NP | 2263.6 ± 405.2 | NP | 47.5 | 40–83 | NP |
| PEEK * [30] | 1.3 | 189.55 ± 16.89 | NP | 87.53–100 | 3–4 | 99.25–170 |
| PEEK, FDM [30] | NP | NP | NP | 97.34 | 2.6–3.45 | 104.65 |
| PMMA * [26,30] | 1.18 | 180 | 19.9 ± 1.0 | NP | 2.3 ± 0.3 | 85 ± 16 |
| PMMA, SLA [26] | NP | NP | 18.1 ± 1.0 | NP | 1.2 ± 0.3 | 95 ± 9 |
| PMMA, DLP [26] | NP | NP | 14.7 ± 1.5 | NP | 0.7 ± 0.2 | 37 ± 6 |
| PLA * [31] | 1.25 | NP | NP | 59 | 3500 | 106 |
| PLA, FDM [31] | NP | NP | NP | 28–48 | 2000 | NP |
| Ti * [30] | 4.5 | 300–400 | NP | 954–976 | 102–110 | NP |
| Ti, SLS [28] | 4.42 | NP | 38 | 1089 | 129 | NP |
| CoCr * [30] | 6.5 | 1200 | 350 | 680 | 205 | 800–1400 |
| CoCr, SLS [28] | 8.3 | NP | 350–450 | 1100 | 200 | NP |
| ZrO2 * [32] | NP | 5000–15,000 | NP | 115–711 | 100–250 | 177–1000 |
| ZrO2, SLA [32] | 5.97 | NP | 12.6 | NP | 209.4 | 300–1000 |
| Al2O3 * [32] | NP | 22,000 | NP | 267 | 380 | 500 |
| Al2O3, SLA [32] | NP | NP | NP | NP | NP | 271.7–273.8 |
5. Applications of 3D Printing in Dentistry
5.1. Prosthodontics
5.1.1. Crown and Fixed Partial Dentures (FPD)
5.1.2. Complete and Removable Partial Dentures (RPD)
5.2. Implantology
5.3. Oral and Maxillofacial
5.3.1. Surgical Guides and Templates
5.3.2. Custom Implants
5.3.3. Maxillofacial Prostheses
5.4. Orthodontics
5.5. Endodontics
5.6. Periodontics
5.6.1. Scaffolds for Hard and Soft Tissue Regeneration
5.6.2. Gingivectomy Surgical Guide
6. Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dawood, A.; Marti Marti, B.; Sauret-Jackson, V. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Park, J.; Kim, S.; Heo, S.; Koak, J. Flexural strength of 3D-printing resin materials for provisional fixed dental prosthesis. Materials 2020, 13, 3970. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.; Papaioannou, W.; Papdopoulou, E.; Dalampira, M.; Tsolakis, A. Comparison in terms of accuracy between DLP and LCD printing technology for dental model printing. Dent. J. 2022, 10, 181. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.; Gizani, S.; Panayi, N.; Antonopoulos, G.; Tsolakis, A. Three-dimensional printing technology in orthodontics for dental models: A systematic review. Children 2022, 9, 1106. [Google Scholar] [CrossRef]
- Rungrojwittayakul, O.; Kan, J.; Shiozaki, K.; Swamidass, R.; Goodacre, B.; Goodacre, C.; Lazada, J. Technologies of printers with different designs of model base. J. Prosthodont. 2020, 29, 124–128. [Google Scholar] [CrossRef]
- Schweiger, J.; Edelhoff, D.; Guth, J. 3D printing in digital prosthetic dentistry: An overview of recent developments in additive manufacturing. J. Clin. Med. 2021, 10, 2010. [Google Scholar] [CrossRef]
- Muzaffar, A.; Zafar, H. Application of 3D printing technology in dentistry: A review. Saudi J. Dent. Res. 2018, 11, 1670–1675. [Google Scholar]
- Ma, T.; Peng, T.; Lin, Y.; Zhang, M.; Ren, G. Effect of internal structures on the accuracy of 3D printed full-arch dentition preparation models in different printing systems. J. Adv. Prosthodont. 2023, 15, 145–154. [Google Scholar] [CrossRef]
- Moser, N.; Santander, P.; Quast, A. From 3D imaging to 3D printing in dentistry—A practice guide. Int. J. Comput. Dent. 2018, 21, 345–346. [Google Scholar]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.; Jiang, H. A review of 3D printing in dentistry: Technologies, affecting factors, and applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef]
- Della Bona, A.; Cantelli, V.; Britto, V.T.; Collares, K.F.; Stansbury, J.W. 3D printing restorative materials using a stereolithographic technique: A systematic review. Dent. Mater. 2021, 37, 336–350. [Google Scholar] [CrossRef] [PubMed]
- Khorsandi, D.; Fahimipour, A.; Abasian, P.; Saber, S.S.; Seyedi, M.; Ghanavati, S.; Ahmad, A.; De Stephanis, A.A.; Taghavinezhaddilami, F.; Leonova, A.; et al. 3D and 4D printing in dentistry and maxillofacial surgery: Printing techniques, materials, and applications. Acta Biomater. 2021, 122, 26–49. [Google Scholar] [CrossRef] [PubMed]
- Al Hamad, K.Q.; Al-Rashdan, B.A.; Ayyad, J.Q.; Al Omrani, L.M.; Sharoh, A.M.; Al Nimri, A.M.; Al-Kaff, F.T. Additive Manufacturing of Dental Ceramics: A Systematic Review and Meta-Analysis. J. Prosthodont. 2022, 31, e67–e86. [Google Scholar] [CrossRef] [PubMed]
- SLA vs. DLP: Guide to Resin 3D Printers. Available online: https://formlabs.com/blog/resin-3d-printer-comparison-sla-vs-dlp/ (accessed on 7 July 2023).
- The Main Benefits and Disadvantages of Voxel Modeling. Available online: https://blog.spatial.com/the-main-benefits-and-disadvantages-of-voxel-modeling (accessed on 7 July 2023).
- Cailleaux, S.; Sanchez-Ballester, N.M.; Gueche, Y.A.; Bataille, B.; Soulairol, I. Fused Deposition Modeling (FDM), the new asset for the production of tailored medicines. J. Control. Release 2021, 10, 821–841. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Li, H.; Xu, L.; Wang, Y. Selective laser sintering versus conventional lost-wax casting for single metal copings: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 128, 897–904. [Google Scholar] [CrossRef]
- Goguta, L.; Lungeanu, D.; Negru, R.; Birdeanu, M.; Jivanescu, A.; Sinescu, C. Selective Laser Sintering versus Selective Laser Melting and Computer Aided Design—Computer Aided Manufacturing in Double Crowns Retention. J. Prosthodont. Res. 2021, 65, 371–378. [Google Scholar] [CrossRef]
- Chen, J.; Zhao, L.; Zhou, K. Multi-Jet Fusion 3D Voxel Printing of Conductive Elastomers. Adv. Mater. 2022, 34, e2205909. [Google Scholar] [CrossRef]
- Lee, Y.C.; Zheng, J.; Kuo, J.; Acosta-Vélez, G.F.; Linsley, C.S.; Wu, B.M. Binder Jetting of Custom Silicone Powder for Direct Three-Dimensional Printing of Maxillofacial Prostheses. 3D Print. Addit. Manuf. 2022, 9, 520–534. [Google Scholar] [CrossRef]
- Ahn, S.H.; Lee, J.; Park, S.A.; Kim, W.D. Three-dimensional bio-printing equipment technologies for tissue engineering and regenerative medicine. Tissue Eng. Regen. Med. 2016, 13, 663–676. [Google Scholar] [CrossRef]
- Guerrero-Girones, J.; Lopez-Garcia, S.; Pecci-Lloret, M.R.; Pecci-Lloret, M.P.; Rodriguez Lozano, F.J.; Garcia-Bernal, D. In vitro biocompatibility testing of 3D printing and conventional resins for occlusal devices. J. Dent. 2022, 123, 104163. [Google Scholar] [CrossRef]
- Kim, G.T.; Go, H.B.; Yu, J.H.; Yang, S.Y.; Kim, K.M.; Choi, S.H.; Kwon, J.S. Cytotoxicity, colour stability and dimensional accuracy of 3D printing resin with three different photoinitiators. Polymers 2022, 14, 979. [Google Scholar] [CrossRef] [PubMed]
- Wuersching, S.N.; Hickel, R.; Edelhoff, D.; Kollmuss, M. Initial biocompatibility of novel resins for 3D printed fixed dental prostheses. Dent. Mater. 2022, 38, 1587–1597. [Google Scholar] [CrossRef]
- Valenti, C.; Isabella Federici, M.; Masciotti, F.; Marinucci, L.; Xhimitiku, I.; Cianetti, S.; Pagano, S. Mechanical properties of 3D-printed prosthetic materials compared with milled and conventional processing. J. Prosthet. Dent. 2022. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Wesemann, C.; Spies, B.C.; Sterzenbach, G.; Beuer, F.; Kohal, R.; Wemken, G.; Krügel, M.; Pieralli, S. Polymers for conventional, subtractive, and additive manufacturing of occlusal devices differ in hardness and flexural properties but not in wear resistance. Dent. Mater. 2021, 37, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Prpić, V.; Schauperl, Z.; Ćatić, A.; Dulčić, N.; Čimić, S. Comparison of mechanical properties of 3D-printed, CAD/CAM, and conventional denture base materials. J. Prosthodont. 2020, 29, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Özcan, M. Additive Manufacturing Technologies used for 3D Metal Printing in Dentistry. Curr. Oral Health Rep. 2017, 4, 201–208. [Google Scholar] [CrossRef]
- Al Jabbari, Y.S.; Koutsoukis, T.; Barmpagadaki, X.; Zinelis, S. Metallurgical and interfacial characterization of PFM Co-Cr dental alloys fabricated via casting, milling or selective laser melting. Dent. Mater. 2014, 30, e79–e88. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Liu, Y.; Peng, B.; Chen, M.; Liu, Z.; Li, Z.; Kuang, H.; Gong, B.; Li, Z.; Sun, H. Peek for oral applications: Recent advances in mechanical and adhesive properties. Polymers 2023, 15, 386. [Google Scholar] [CrossRef]
- Farah, S.; Anderson, D.G.; Langer, R. Physical and mechanical properties of PLA, and their functions in widespread applications —A comprehensive review. Adv. Drug Deliv. Rev. 2016, 107, 367–392. [Google Scholar] [CrossRef]
- Galante, R.; Figueiredo-Pina, C.G.; Serro, A.P. Additive manufacturing of ceramics for dental applications: A review. Dent. Mater. 2019, 35, 825–846. [Google Scholar] [CrossRef]
- Tahayeri, A.; Morgan, M.; Fugolin, A.P.; Bompolaki, D.; Athirasala, A.; Pfeifer, C.S.; Ferracane, J.L.; Bertassoni, L.E. 3D printed versus conventional cured provisional crown and bridge dental materials. Dent. Mater. 2018, 34, 192–200. [Google Scholar] [CrossRef] [PubMed]
- van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.N.; Lee, K.B.; Lee, D.H. Fit of interim crowns fabricated using photopolymer jetting 3D printing. J. Prosthet. Dent. 2017, 118, 208–215. [Google Scholar] [CrossRef]
- Lee, W.S.; Lee, D.H.; Lee, K.B. Evaluation of internal fit of interim crown fabricated with CAD/CAM milling and 3D printing system. J. Adv. Prosthodont. 2017, 9, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Alqahtani, N.M.; Addas, M.K.; Alfarsi, M.A. Marginal and internal fit of provisional crowns fabricated using 3D printing technology. Technol. Health Care 2020, 28, 635–642. [Google Scholar] [CrossRef]
- Hacker, T.; Heydecke, G.; Reissmann, D.R. Impact of procedures during prosthodontic treatment on patients’ perceived burden. J. Dent. 2015, 43, 51–57. [Google Scholar] [CrossRef]
- Kim, J.-E.; Kim, N.-H.; Shin, J.-S. Fabrication of complete, removable dental prosthesis from a digital intraoral impression for a patient with excessively tight reconstructed lip after oral can treatment: A clinical report. J. Prosthet. Dent. 2017, 117, 205–208. [Google Scholar] [CrossRef]
- Hu, F.; Pei, Z.; Wen, Y. Using intraoral scanning technology for three-dimensional printing of Kennedy class I removable partial denture metal framework: A clinical report. J. Prosthodont. 2019, 28, e473–e476. [Google Scholar] [CrossRef]
- Gan, N.; Ruan, Y.; Sun, J.; Xiong, Y.; Jiao, T. Comparison of adaptation between the major connectors fabricated from intraoral digital impression and extraoral digital impressions. Sci. Rep. 2018, 8, 529. [Google Scholar] [CrossRef]
- Yoon, S.N.; Oh, K.C.; Lee, S.J.; Han, J.S.; Yoon, H.I. Tissue surface adaptation of CAD-CAM maxillary and mandibular complete denture bases manufactured by digital light processing: A clinical study. J. Prosthet. Dent. 2020, 124, 682–689. [Google Scholar] [CrossRef]
- Bilgin, M.S.; Baytaroglu, E.N.; Erdem, A.; Dilber, E. A review of computer-aided design/computer-aided manufacture techniques for removable denture fabrication. Eur. J. Dent. 2016, 10, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Bajunaid, S.O.; Altwaim, B.; Alhassan, M.; Alammari, R. The fit accuracy of removable partial denture metal frameworks using conventional and 3D printed techniques: An in vitro study. J. Contemp. Dent. Pract. 2019, 20, 476–481. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral. Maxillofac. Implant. 2014, 29, S25–S42. [Google Scholar] [CrossRef] [PubMed]
- Alzit, F.R.; Cade, R.; Naveau, A.; Babilotte, J.; Meglioli, M.; Catros, S. Accuracy of commercial 3D printers for the fabrication of surgical guides in dental implantology. J. Dent. 2022, 117, 103909. [Google Scholar] [CrossRef] [PubMed]
- Skjerven, H.; Riis, U.H.; Herlofsson, B.B.; Ellingsen, J.E. In vivo accuracy of implant placement using a full digital planning modality and stereolithographic guides. Int. J. Oral. Maxillofac. Implant. 2019, 34, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, G.; Nitsch, S.; Edelmayer, M.; Janijic, K.; Muller, A.S.; Agis, H. 3D printing-encompassing the facets of dentistry. Front. Bioeng. Biotechnol. 2018, 6, 172. [Google Scholar] [CrossRef] [PubMed]
- Erickson, D.M.; Chance, D.; Schmitt, S.; Mathis, J. An opinion survey of reported benefits from the use of stereolithographic models. J. Oral Maxillofac. Surg. 1999, 57, 1040–1043. [Google Scholar] [CrossRef] [PubMed]
- Polley, J.W.; Figueroa, A.A. Orthognathic positioning system: Intraoperative system to transfer virtual surgical plan to operating field during orthognathic surgery. J. Oral Maxillofac. Surg. 2013, 71, 911–920. [Google Scholar] [CrossRef]
- Barazanchi, A.; Li, K.C.; Al-Amleh, B.; Lyons, K.; Waddell, J.N. Additive technology: Update on current materials and applications in dentistry. J. Prosthodont. 2017, 26, 156–163. [Google Scholar] [CrossRef]
- Sherwood, R.G.; Murphy, N.; Kearns, G.; Barry, C. The use of 3D printing technology in the creation of patient-specific facial prostheses. Ir. J. Med. Sci. 2020, 189, 1215–1221. [Google Scholar] [CrossRef]
- Martorelli, M.; Gerbino, S.; Giudice, M.; Ausiello, P. A comparison between customized clear and removable orthodontic appliances manufactured using RP and CNC techniques. Dent. Mater. 2013, 29, e1–e10. [Google Scholar] [CrossRef]
- Gerard Bradley, T.; Teske, L.; Eliades, G.; Zinelis, S.; Eliades, T. Do the mechanical and chemical properties of Invisalign TM appliances change after use? A retrieval analysis. Eur. J. Orthod. 2015, 38, 27–31. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef]
- Tecco, S.; Nota, A.; Pittari, L.; Clerici, C.; Mangano, F.; Gherlone, E.F. Full-digital workflow for TMDs Management: A case series. Healthcare 2023, 11, 790. [Google Scholar] [CrossRef]
- Buniag, A.G.; Pratt, A.M.; Ray, J.J. Targeted endodontic microsurgery: A retrospective outcomes assessment of 24 cases. J. Endod. 2021, 47, 762–769. [Google Scholar] [CrossRef]
- Buchgreitz, J.; Buchgreitz, M.; Mortensen, D.; Bjorndal, L. Guided access cavity preparation sing cone-beam computed tomography and optical surface scans—An ex vivo study. Int. Endod. J. 2016, 49, 790–795. [Google Scholar] [CrossRef]
- Zehnder, M.S.; Connert, T.; Weiger, R.; Krastl, G.; Kuhl, S. Guided endodontics: Accuracy of a novel method for guided access cavity preparation and root canal location. Int. Endod. J. 2016, 49, 966–972. [Google Scholar] [CrossRef]
- Connert, T.; Zehnder, M.S.; Weiger, R.; Kuhl, S.; Krast, L.G. Microguided endodontics: Accuracy of a miniaturized technique for apically extended access cavity preparation in anterior teeth. J. Endod. 2017, 43, 787–790. [Google Scholar] [CrossRef]
- Strbac, G.D.; Schnappauf, A.; Giannis, K.; Moritz, A.; Ulm, C. Guided Modern endodontic surgery: A novel approach for guided osteotomy and root resection. J. Endod. 2017, 43, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kratchman, S. Modern endodontic surgery concepts and practice: A review. J. Endod. 2006, 32, 601–623. [Google Scholar] [CrossRef]
- Salah, M.; Tayebi, L.; Moharamzadeh, K.; Naini, F.B. Three-dimensional bio-printing and bone tissue engineering: Technical innovations and potentional applications in maxillofacial reconstructive surgery. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 18. [Google Scholar] [CrossRef] [PubMed]
- Nesic, D.; Schaefer, B.M.; Sun, Y.; Saulacic, N. 3D printing approach in dentistry: The future for personalized oral soft tissue regeneration. J. Clin. Med. 2020, 7, 2238. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.; Haleem, A.; Singh, R.P.; Rab, S.; Suman, R.; Kumar, L. Significance of 4D printing for dentistry: Materials, process, and potentials. J. Oral Biol. Craniofacial Res. 2022, 3, 388–395. [Google Scholar] [CrossRef]




| 3D Technology | Advantages | Disadvantages |
|---|---|---|
| Stereolithography (SLA) |
|
|
| Digital light processing (DLP) |
|
|
| Fused deposition modeling (FDM) |
|
|
| Selective laser sintering (SLS) and selective laser melting (SLM) |
|
|
| Photopolymer jetting |
|
|
| Powder binder printing |
|
|
| 3D laser bioprinting (LAB) |
|
|
| Specialty | Applications | Technology | Advantages |
|---|---|---|---|
| Prosthodontics | Crowns and fixed partial dentures | SLA, DLP, photopolymer jetting |
|
| Complete dentures | SLA, DLP |
| |
| Removable partial dentures | SLS, SLM, EBM |
| |
| Implantology | Surgical guide | SLA, DLP, photopolymer jetting |
|
| Custom tray | SLA, FDM |
| |
| Oral and maxillofacial | Surgical guide and template | SLA, DLP, photopolymer jetting |
|
| Custom implants | SLS, photopolymer jetting |
| |
| Maxillofacial prostheses | SLA, photopolymer jetting, SLS, FDM |
| |
| Orthodontics | Aligners | SLA, DLP, FDM |
|
| Orthotic appliances | SLA |
| |
| Endodontics | Surgical guide | SLA, photopolymer jetting |
|
| Periodontics | Scaffolds for hard and soft tissue regeneration | LAB |
|
| Gingivectomy surgical guide | SLA, DLP, photopolymer jetting |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, M.; Radomski, K.; Lopez, D.; Liu, J.T.; Lee, J.D.; Lee, S.J. Materials and Applications of 3D Printing Technology in Dentistry: An Overview. Dent. J. 2024, 12, 1. https://doi.org/10.3390/dj12010001
Jeong M, Radomski K, Lopez D, Liu JT, Lee JD, Lee SJ. Materials and Applications of 3D Printing Technology in Dentistry: An Overview. Dentistry Journal. 2024; 12(1):1. https://doi.org/10.3390/dj12010001
Chicago/Turabian StyleJeong, Min, Kyle Radomski, Diana Lopez, Jack T. Liu, Jason D. Lee, and Sang J. Lee. 2024. "Materials and Applications of 3D Printing Technology in Dentistry: An Overview" Dentistry Journal 12, no. 1: 1. https://doi.org/10.3390/dj12010001