
A Systematic Review of the Use of mHealth in Oral Health Education among Older Adults
 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Question and Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
3. Results
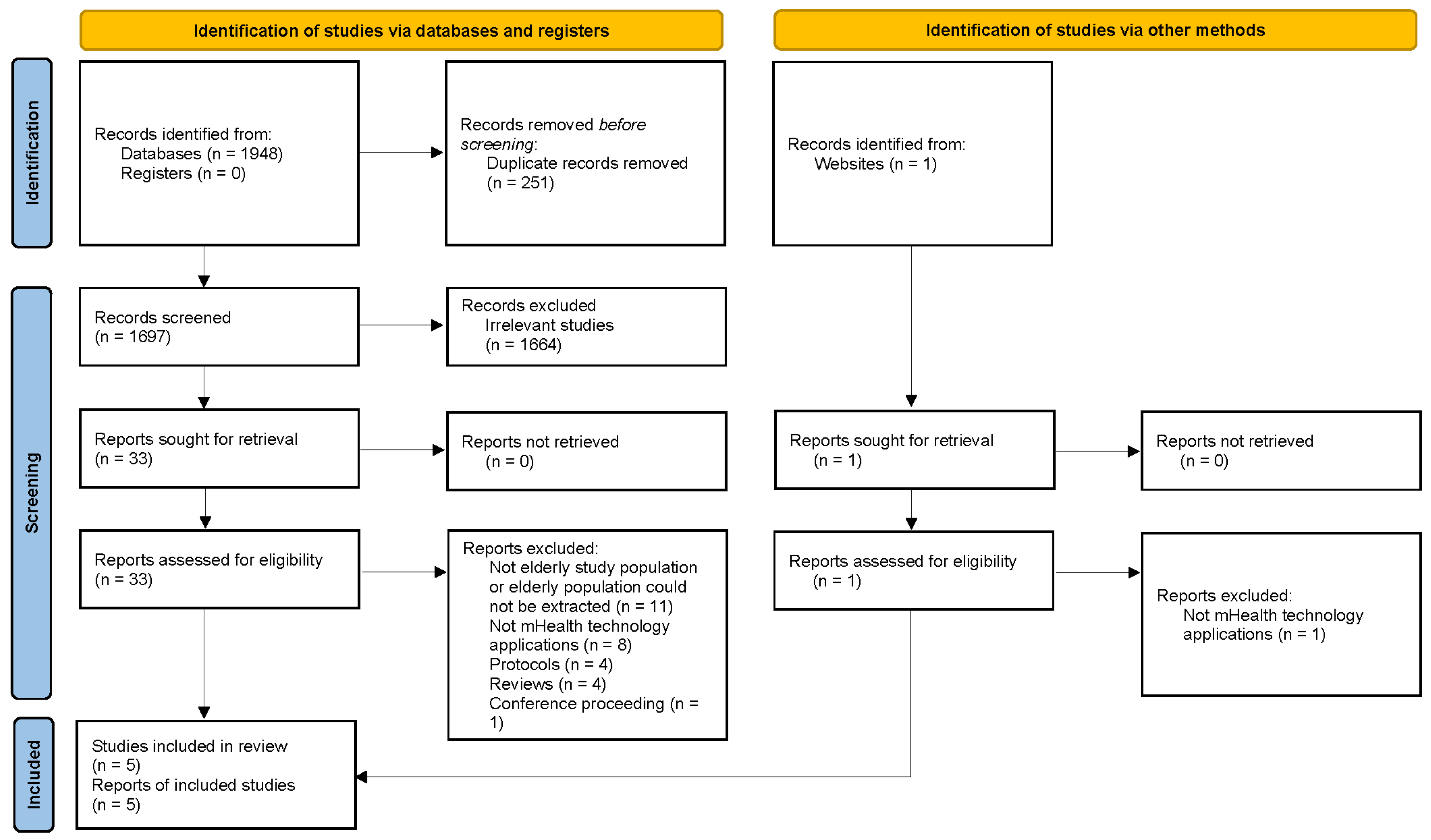
3.1. Search Results
3.2. Study Characteristics
3.3. Format and Content Delivery
3.4. Outcomes
3.4.1. Clinical Outcomes
3.4.2. Participant-Reported Outcomes
3.4.3. Qualitative Outcomes
3.4.4. Oral Health Knowledge Outcomes
3.4.5. Acceptability of mHealth Intervention(s)
3.5. Assessment of Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Criteria | Yes | No | Other (CD, NR, NA) * |
|---|---|---|---|
| 1. Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? | ✓ | ||
| 2. Was the method of randomization adequate (i.e., use of randomly generated assignment)? | ✓ | ||
| 3. Was the treatment allocation concealed (so that assignments could not be predicted)? | ✓ | ||
| 4. Were study participants and providers blinded to treatment group assignment? | ✓ | ||
| 5. Were the people assessing the outcomes blinded to the participants’ group assignments? | ✓ | ||
| 6. Were the groups similar at baseline on important characteristics that could affect outcomes (e.g., demographics, risk factors, co-morbid conditions)? | ✓ | ||
| 7. Was the overall dropout rate from the study at endpoint 20% or lower of the number allocated to treatment? | ✓ | ||
| 8. Was the differential dropout rate (between treatment groups) at endpoint 15 percentage points or lower? | ✓ | ||
| 9. Was there high adherence to the intervention protocols for each treatment group? | ✓ | ||
| 10. Were other interventions avoided or similar in the groups (e.g., similar background treatments)? | ✓ | ||
| 11. Were outcomes assessed using valid and reliable measures, implemented consistently across all study participants? | ✓ | ||
| 12. Did the authors report that the sample size was sufficiently large to be able to detect a difference in the main outcome between groups with at least 80% power? | ✓ | ||
| 13. Were the outcomes reported or sub-groups analyzed pre-specified (i.e., identified before analyses were conducted)? | ✓ | ||
| 14. Were all randomized participants analyzed in the group to which they were originally assigned, i.e., did they use an intention-to-treat analysis? | ✓ |
| Criteria | Yes | No | Other (CD, NR, NA) * |
|---|---|---|---|
| 1. Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? | ✓ | ||
| 2. Was the method of randomization adequate (i.e., use of randomly generated assignment)? | ✓ | ||
| 3. Was the treatment allocation concealed (so that assignments could not be predicted)? | ✓ | ||
| 4. Were study participants and providers blinded to treatment group assignment? | ✓ | ||
| 5. Were the people assessing the outcomes blinded to the participants’ group assignments? | ✓ | ||
| 6. Were the groups similar at baseline on important characteristics that could affect outcomes (e.g., demographics, risk factors, co-morbid conditions)? | ✓ | ||
| 7. Was the overall dropout rate from the study at endpoint 20% or lower of the number allocated to treatment? | ✓ | ||
| 8. Was the differential dropout rate (between treatment groups) at endpoint 15 percentage points or lower? | ✓ | ||
| 9. Was there high adherence to the intervention protocols for each treatment group? | CD | ||
| 10. Were other interventions avoided or similar in the groups (e.g., similar background treatments)? | ✓ | ||
| 11. Were outcomes assessed using valid and reliable measures, implemented consistently across all study participants? | ✓ | ||
| 12. Did the authors report that the sample size was sufficiently large to be able to detect a difference in the main outcome between groups with at least 80% power? | ✓ | ||
| 13. Were the outcomes reported or sub-groups analyzed pre-specified (i.e., identified before analyses were conducted)? | ✓ | ||
| 14. Were all randomized participants analyzed in the group to which they were originally assigned, i.e., did they use an intention-to-treat analysis? | ✓ |
| Criteria | Yes | No | Other (CD, NR, NA) * |
|---|---|---|---|
| 1. Was the study question or objective clearly stated? | ✓ | ||
| 2. Were eligibility/selection criteria for the study population pre-specified and clearly described? | ✓ | ||
| 3. Were the participants in the study representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest? | ✓ | ||
| 4. Were all eligible participants that met the pre-specified entry criteria enrolled? | ✓ | ||
| 5. Was the sample size sufficiently large to provide confidence in the findings? | ✓ | ||
| 6. Was the test/service/intervention clearly described and delivered consistently across the study population? | ✓ | ||
| 7. Were the outcome measures pre-specified, clearly defined, valid, reliable, and assessed consistently across all study participants? | ✓ | ||
| 8. Were the people assessing the outcomes blinded to the participants’ exposures/interventions? | ✓ | ||
| 9. Was the loss to follow-up after baseline 20% or less? Were those lost to follow-up accounted for in the analysis? | ✓ + | ||
| 10. Did the statistical methods examine changes in outcome measures from before to after the intervention? Were statistical tests performed that provided p-values for the pre-to-post changes? | ✓ | ||
| 11. Were outcome measures of interest taken multiple times before the intervention and multiple times after the intervention (i.e., did they use an interrupted time-series design)? | ✓ | ||
| 12. If the intervention was conducted at a group level (e.g., a whole hospital, a community, etc.), did the statistical analysis take into account the use of individual-level data to determine effects at the group level? | CD | ||
| Reason(s) to be considered “Poor” | + Changes in participants to keep the same sample size during the study | ||
| Criteria | Yes | No | Other (CD, NR, NA) * |
|---|---|---|---|
| 1. Was the study question or objective clearly stated? | ✓ | ||
| 2. Were eligibility/selection criteria for the study population pre-specified and clearly described? | ✓ | ||
| 3. Were the participants in the study representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest? | ✓ | ||
| 4. Were all eligible participants that met the pre-specified entry criteria enrolled? | ✓ | ||
| 5. Was the sample size sufficiently large to provide confidence in the findings? | ✓ | ||
| 6. Was the test/service/intervention clearly described and delivered consistently across the study population? | ✓ | ||
| 7. Were the outcome measures pre-specified, clearly defined, valid, reliable, and assessed consistently across all study participants? | ✓ | ||
| 8. Were the people assessing the outcomes blinded to the participants’ exposures/interventions? | ✓ | ||
| 9. Was the loss to follow-up after baseline 20% or less? Were those lost to follow-up accounted for in the analysis? | ✓ + | ||
| 10. Did the statistical methods examine changes in outcome measures from before to after the intervention? Were statistical tests performed that provided p-values for the pre-to-post changes? | ✓ | ||
| 11. Were outcome measures of interest taken multiple times before the intervention and multiple times after the intervention (i.e., did they use an interrupted time-series design)? | ✓ | ||
| 12. If the intervention was conducted at a group level (e.g., a whole hospital, a community, etc.), did the statistical analysis take into account the use of individual-level data to determine effects at the group level? | NA | ||
| Reason(s) to be considered “Poor” | + High dropout rate (33%), which was considered a fatal flaw according to guidelines [35] | ||
| Criteria | Yes | No | Other (CD, NR, NA) * |
|---|---|---|---|
| 1. Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? | ✓ | ||
| 2. Was the method of randomization adequate (i.e., use of randomly generated assignment)? | ✓ | ||
| 3. Was the treatment allocation concealed (so that assignments could not be predicted)? | ✓ | ||
| 4. Were study participants and providers blinded to treatment group assignment? | ✓ | ||
| 5. Were the people assessing the outcomes blinded to the participants’ group assignments? | ✓ | ||
| 6. Were the groups similar at baseline on important characteristics that could affect outcomes (e.g., demographics, risk factors, co-morbid conditions)? | ✓ | ||
| 7. Was the overall dropout rate from the study at endpoint 20% or lower of the number allocated to treatment? | ✓ + | ||
| 8. Was the differential dropout rate (between treatment groups) at endpoint 15 percentage points or lower? | ✓ | ||
| 9. Was there high adherence to the intervention protocols for each treatment group? | CD | ||
| 10. Were other interventions avoided or similar in the groups (e.g., similar background treatments)? | ✓ | ||
| 11. Were outcomes assessed using valid and reliable measures, implemented consistently across all study participants? | NR | ||
| 12. Did the authors report that the sample size was sufficiently large to be able to detect a difference in the main outcome between groups with at least 80% power? | ✓ | ||
| 13. Were the outcomes reported or sub-groups analyzed pre-specified (i.e., identified before analyses were conducted)? | ✓ | ||
| 14. Were all randomized participants analyzed in the group to which they were originally assigned, i.e., did they use an intention-to-treat analysis? | ✓ | ||
| Reason(s) to be considered “Poor” | + High dropout rate (55%), which was considered a fatal flaw according to guidelines [35] | ||
References
- World Population Ageing 2019; Department of Economic and Social Affairs: New York, NY, USA, 2019; p. 46.
- McMillan, A.; Wong, M.; Lo, E.; Allen, P. The impact of oral disease among the institutionalized and non-institutionalized elderly in Hong Kong. J. Oral Rehabil. 2003, 30, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Montal, S.; Tramini, P.; Triay, J.A.; Valcarcel, J. Oral hygiene and the need for treatment of the dependent institutionalised elderly. Gerodontology 2006, 23, 67–72. [Google Scholar] [CrossRef]
- Dörfer, C.E.; Becher, H.; Ziegler, C.M.; Kaiser, C.; Lutz, R.; Jörß, D.; Lichy, C.; Buggle, F.; Bültmann, S.; Preusch, M. The association of gingivitis and periodontitis with ischemic stroke. J. Clin. Periodontol. 2004, 31, 396–401. [Google Scholar] [CrossRef]
- Petersen, P.E.; Yamamoto, T. Improving the oral health of older people: The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2005, 33, 81–92. [Google Scholar] [CrossRef]
- Borg-Bartolo, R.; Roccuzzo, A.; Mourelle, P.M.; Schimmel, M.; Gambetta-Tessini, K.; Chaurasia, A.; Koca-Ünsal, R.; Tennert, C.; Giacaman, R.; Campus, G. Global prevalence of edentulism and dental caries in middle-aged and elderly persons. A systematic review and meta-analysis. J. Dent. 2022, 127, 104335. [Google Scholar] [CrossRef]
- McGrath, C.; Zhang, W.; Lo, E.C. A review of the effectiveness of oral health promotion activities among elderly people. Gerodontology 2009, 26, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.; Walls, A. Strategies to improve the quality of oral health care for frail and dependent older people. BMJ Qual. Saf. 1997, 6, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löe, H. Oral hygiene in the prevention of caries and periodontal disease. Int. Dent. J. 2000, 50, 129–139. [Google Scholar] [CrossRef]
- Mojon, P.; Rentsch, A.; Budtz-Jørgensen, E.; Baehni, P.C. Effects of an oral health program on selected clinical parameters and salivary bacteria in a long-term care facility. Eur. J. Oral Sci. 1998, 106, 827–834. [Google Scholar] [CrossRef]
- Persson, R.E.; Persson, G.R.; Powell, L.V.; Klyak, H.A. Periodontal effects of a biobehavioral prevention program. J. Clin. Periodontol. 1998, 25, 322–329. [Google Scholar] [CrossRef]
- Wong, F.M.; Ng, Y.T.; Leung, W.K. Oral health and its associated factors among older institutionalized residents—A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 4132. [Google Scholar] [CrossRef] [Green Version]
- Watt, R.G. Strategies and approaches in oral disease prevention and health promotion. Bull. World Health Organ. 2005, 83, 711–718. [Google Scholar] [PubMed]
- Kay, M.; Santos, J.; Takane, M. mHealth: New horizons for health through mobile technologies. World Health Organ. 2011, 64, 66–71. [Google Scholar]
- Shcherbina, A.; Mattsson, C.M.; Waggott, D.; Salisbury, H.; Christle, J.W.; Hastie, T.; Wheeler, M.T.; Ashley, E.A. Accuracy in Wrist-Worn, Sensor-Based Measurements of Heart Rate and Energy Expenditure in a Diverse Cohort. J. Pers. Med. 2017, 7, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Campbell, A.S.; de Ávila, B.E.-F.; Wang, J. Wearable biosensors for healthcare monitoring. Nat. Biotechnol. 2019, 37, 389–406. [Google Scholar] [CrossRef]
- Schueller, S.M.; Muñoz, R.F.; Mohr, D.C. Realizing the Potential of Behavioral Intervention Technologies. Curr. Dir. Psychol. Sci. 2013, 22, 478–483. [Google Scholar] [CrossRef]
- Blaya, J.A.; Fraser, H.S.; Holt, B. E-health technologies show promise in developing countries. Health Aff. 2010, 29, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Lindquist, A.; Johansson, P.; Petersson, G.; Saveman, B.-I.; Nilsson, G. The use of the Personal Digital Assistant (PDA) among personnel and students in health care: A review. J. Med. Internet Res. 2008, 10, e1038. [Google Scholar] [CrossRef]
- Cole-Lewis, H.; Kershaw, T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol. Rev. 2010, 32, 56–69. [Google Scholar] [CrossRef] [Green Version]
- Giraudeau, N.; Varenne, B. Advocacy for a digital oral health that leaves no one behind. JDR Clin. Transl. Res. 2022, 7, 25–28. [Google Scholar] [CrossRef]
- Fernández, C.; Maturana, C.; Coloma, S.; Carrasco-Labra, A.; Giacaman, R. Teledentistry and mHealth for promotion and prevention of oral health: A systematic review and meta-analysis. J. Dent. Res. 2021, 100, 914–927. [Google Scholar] [CrossRef] [PubMed]
- Aquilanti, L.; Santarelli, A.; Mascitti, M.; Procaccini, M.; Rappelli, G. Dental Care Access and the Elderly: What Is the Role of Teledentistry? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9053. [Google Scholar] [CrossRef] [PubMed]
- Toniazzo, M.P.; Nodari, D.; Muniz, F.W.M.G.; Weidlich, P. Effect of mHealth in improving oral hygiene: A systematic review with meta-analysis. J. Clin. Periodontol. 2019, 46, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Yu, K.F.; Liu, P.; Lee, G.H.M.; Wong, M.C.M. Can mHealth promotion for parents help to improve their children’s oral health? A Systematic Review. J. Dent. 2022, 123, 104185. [Google Scholar] [CrossRef] [PubMed]
- Vo, V.; Auroy, L.; Sarradon-Eck, A. Patients’ perceptions of mHealth apps: Meta-ethnographic review of qualitative studies. JMIR Mhealth Uhealth 2019, 7, e13817. [Google Scholar] [CrossRef] [Green Version]
- Gorini, A.; Mazzocco, K.; Triberti, S.; Sebri, V.; Savioni, L.; Pravettoni, G. A P5 Approach to m-Health: Design suggestions for advanced mobile health technology. Front. Psychol. 2018, 9, 2066. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Aging, World Health Organization. Available online: https://www.who.int/health-topics/ageing (accessed on 23 March 2023).
- Gao, X.; Lo, E.C.; Kot, S.C.; Chan, K.C. Motivational interviewing in improving oral health: A systematic review of randomized controlled trials. J. Periodontol. 2014, 85, 426–437. [Google Scholar] [CrossRef]
- Chunda, R.; Mossey, P.; Freeman, R.; Yuan, S. Health Coaching-Based Interventions for Oral Health Promotion: A Scoping Review. Dent. J. 2023, 11, 73. [Google Scholar] [CrossRef]
- Kakudate, N.; Morita, M.; Sugai, M.; Kawanami, M. Systematic cognitive behavioral approach for oral hygiene instruction: A short-term study. Patient Educ. Couns. 2009, 74, 191–196. [Google Scholar] [CrossRef]
- Kay, E.; Locker, D. A systematic review of the effectiveness of health promotion aimed at improving oral health. Database Abstr. Rev. Eff. 1998, 15, 132–144. [Google Scholar]
- Harrison, H.; Griffin, S.J.; Kuhn, I.; Usher-Smith, J.A. Software tools to support title and abstract screening for systematic reviews in healthcare: An evaluation. BMC Med. Res. Methodol. 2020, 20, 7. [Google Scholar] [CrossRef] [PubMed]
- Study Quality Assessment Tools. 2021. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 24 March 2023).
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bashi, N.; Fatehi, F.; Fallah, M.; Walters, D.; Karunanithi, M. Self-management education through mHealth: Review of strategies and structures. JMIR Mhealth Uhealth 2018, 6, e10771. [Google Scholar] [CrossRef]
- Free, C.; Phillips, G.; Watson, L.; Galli, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technologies to improve health care service delivery processes: A systematic review and meta-analysis. PLoS Med. 2013, 10, e1001363. [Google Scholar] [CrossRef]
- Lavallee, D.C.; Chenok, K.E.; Love, R.M.; Petersen, C.; Holve, E.; Segal, C.D.; Franklin, P.D. Incorporating patient-reported outcomes into health care to engage patients and enhance care. Health Aff. 2016, 35, 575–582. [Google Scholar] [CrossRef]
- Hamine, S.; Gerth-Guyette, E.; Faulx, D.; Green, B.B.; Ginsburg, A.S. Impact of mHealth chronic disease management on treatment adherence and patient outcomes: A systematic review. J. Med. Internet Res. 2015, 17, e52. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Xie, B. Health literacy in the eHealth era: A systematic review of the literature. Patient Educ. Couns. 2017, 100, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Choi, Y.Y.; Jung, E.S. Effectiveness of an oral health education programme using a mobile application for older adults: A randomised clinical trial. Gerodontology 2023, 40, 47–55. [Google Scholar] [CrossRef]
- Ki, J.Y.; Jo, S.R.; Cho, K.S.; Park, J.E.; Cho, J.W.; Jang, J.H. Effect of Oral Health Education Using a Mobile App (OHEMA) on the Oral Health and Swallowing-Related Quality of Life in Community-Based Integrated Care of the Elderly: A Randomized Clinical Trial. Int. J. Env. Res. Public Health 2021, 18, 11679. [Google Scholar] [CrossRef]
- Khalil, M.; Sorour, D.; Mousa, E.; Shaala, R. Effect of Mobile-Based Educational Program through Bluetooth and WhatsApp. Application on the Oral Health Values, Dental Literacy, and Oral Self-Efficacy among Older Adults. NILES J. Geriatr. Gerontol. 2020, 3, 42–64. [Google Scholar] [CrossRef]
- Mariño, R.J.; Marwaha, P.; Barrow, S.Y. Web-based oral health promotion program for older adults: Development and preliminary evaluation. Int. J. Med. Inf. 2016, 91, e9–e15. [Google Scholar] [CrossRef] [PubMed]
- Wanyonyi, K.; Couch, C.; John, J.; Louca, C. E-Oral health interventions for older patients in an outreach primary dental care centre: A pilot trial nested acceptability study. Gerodontology 2022, 39, 241–249. [Google Scholar] [CrossRef]
- Lee, K.H.; Choi, Y.Y.; Jung, E.S. Effectiveness of an oral health education programme for older adults using a workbook. Gerodontology 2020, 37, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Lynn, H.-G. K-Pop: Popular Music, Cultural Amnesia, and Economic Innovation in South Korea. J. Asian Stud. 2015, 74, 1047–1049. [Google Scholar] [CrossRef]
- Jin, B.-H.; Jo, A.-H.; Jeong, J.-Y.; Song, Y.-S.; Park, D.-Y.; Hwang, Y.-S.; Kim, Y.-S. The evaluation of the 2005 oral health education materials made in Korea oral health association. J. Korean Dent. Assoc. 2006, 44, 561–573. [Google Scholar]
- Kim, J.H.; Kim, H.Y. Effects of an oral self-care program on the elderly’s xerostomia and oral health-related quality of life. J. Korean Acad. Community Health Nurs. 2018, 29, 382–392. [Google Scholar] [CrossRef]
- Lee, G.R.; Kim, D.R.; Lim, H.N.; Kang, K.H. The effects of the oral care program for improving swallowing function of the elderly using welfare centers on depression, self efficacy, subjective oral health status and swallowing related quality of life. J. Korean Acad. Community Health Nurs. 2020, 31, 166–178. [Google Scholar] [CrossRef]
- Al-Sinaidi, A.A. Periodontal health and oral hygiene practice of elderly Saudis living at Riyadh Nursing Home. King Saud Univ. J. Dent. Sci. 2012, 3, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Das, D.; Menon, I.; Gupta, R.; Arora, V.; Ashraf, A.; Ahsan, I. Oral health literacy: A practical strategy towards better oral health status among adult population of Ghaziabad district. J. Fam. Med. Prim. Care 2020, 9, 764. [Google Scholar] [CrossRef]
- Catteau, C.; Faulks, D.; Mishellany-Dutour, A.; Collado, V.; Tubert-Jeannin, S.; Tardieu, C.; Hugues, P.; Roger-Leroi, V.; Hennequin, M. Using e-learning to train dentists in the development of standardised oral health promotion interventions for persons with disability. Eur. J. Dent. Educ. 2013, 17, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Ab Malik, N.; Zhang, J.; Lam, O.L.T.; Jin, L.; McGrath, C. Effectiveness of computer-aided learning in oral health among patients and caregivers: A systematic review. J. Am. Med. Inform. Assoc. 2017, 24, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palati, S.; Ramani, P.; Shrelin, H.J.; Sukumaran, G.; Ramasubramanian, A.; Don, K.; Jayaraj, G.; Santhanam, A. Knowledge, Attitude and practice survey on the perspective of oral lesions and dental health in geriatric patients residing in old age homes. Indian J. Dent. Res. 2020, 31, 22–25. [Google Scholar] [CrossRef]
- Mariño, R.; Calache, H.; Wright, C.; Schofield, M.; Minichiello, V. Oral health promotion programme for older migrant adults. Gerodontology 2004, 21, 216–225. [Google Scholar] [CrossRef]
- Mariño, R.; Calache, H.; Morgan, M. A Community-Based Culturally Competent Oral Health Promotion for Migrant Older Adults Living in Melbourne, Australia. J. Am. Geriatr. Soc. 2013, 61, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Office for Health Improvement and Disparities; Department of Health and Social Care; NHS England; NHS Improvement. Delivering Better Oral Health: An Evidence-Based Toolkit for Prevention. 2014. Available online: https://www.gov.uk/government/publications/delivering-better-oral-health-an-evidence-based-toolkit-for-prevention (accessed on 3 April 2023).
- Haleem, A.; Khan, M.K.; Sufia, S.; Chaudhry, S.; Siddiqui, M.I.; Khan, A.A. The role of repetition and reinforcement in school-based oral health education-a cluster randomized controlled trial. BMC Public Health 2016, 16, 2. [Google Scholar] [CrossRef] [Green Version]
- Busch, P.A.; Hausvik, G.I.; Ropstad, O.K.; Pettersen, D. Smartphone usage among older adults. Comput. Hum. Behav. 2021, 121, 106783. [Google Scholar] [CrossRef]
- Chau, R.C.W.; Li, G.-H.; Tew, I.M.; Thu, K.M.; McGrath, C.; Lo, W.-L.; Ling, W.-K.; Hsung, R.T.-C.; Lam, W.Y.H. Accuracy of Artificial Intelligence-Based Photographic Detection of Gingivitis. Int. Dent. J. 2023, in press. [Google Scholar] [CrossRef]
- Shen, K.L.; Huang, C.L.; Lin, Y.C.; Du, J.K.; Chen, F.L.; Kabasawa, Y.; Chen, C.C.; Huang, H.L. Effects of artificial intelligence-assisted dental monitoring intervention in patients with periodontitis: A randomized controlled trial. J. Clin. Periodontol. 2022, 49, 988–998. [Google Scholar] [CrossRef]
- El Tantawi, M.; Lam, W.Y.H.; Giraudeau, N.; Virtanen, J.I.; Matanhire, C.; Chifamba, T.; Sabbah, W.; Gomaa, N.; Al-Maweri, S.A.; Uribe, S.E.; et al. Teledentistry from research to practice: A tale of nineteen countries. Front. Oral Health 2023, 4, 1188557. [Google Scholar] [CrossRef]
- Chau, R.C.W.; Thu, K.M.; Hsung, R.T.C.; Lam, W.Y.H. Teeth Reconstruction Using Artificial Intelligence: Trends, Perspectives, and Prospects. J. Calif. Dent. Assoc. 2023, 51, 2199910. [Google Scholar] [CrossRef]

| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Author (Year), Country | Participants 1 | Interventions and Controls | Outcome(s) Measured |
|---|---|---|---|
| Lee (2023), South Korea [42] | Enrolled in a senior welfare center. 65 to 85+ years old. (Gender of recruited participants not specified.) N = 90/73. Intervention: n = 25. Control 1: n = 22. Control 2: n = 26. | Intervention Access to oral health education APP for 5 weeks, with 2 reminders per week. Control 1 30 min oral health education lecture for 5 weeks, twice a week. 15 min practice after each lecture. Control 2 No oral health education. | - Oral health knowledge. + - Oral health perception. + - Oral Health Impact Profile-14 (OHIP-14). ^ - General Oral Health Assessment Index (GOHAI). ^ - O’Leary Index. ^ - Tongue Coating Index. ^ - Löe and Silness Index. ^ |
| Ki (2021), South Korea [43] | Enrolled in a social service program. 65 to 75+ years old. (Gender of recruited participants not specified.) N = 46/40. Intervention: n = 20. Control: n = 20. | Intervention Access to oral health education APP for 6 weeks, with an unspecified number of 1-to-1 customized education sessions of up to 50 min. Control No oral health education. | - Oral health behavior. + - Number of functional teeth. ^ - Plaque Index. ^ - Tongue Coating Index. ^ - Oral frailty. + - OHIP-14. ^ - GOHAI. ^ - Dietary factors. + |
| Khalil (2020), Egypt [44] | Independent older adults in the community. 60 to 70+ years old. 26 males, 41 females. N = 67/67. Intervention: n = 67. No external control. | Intervention Access to oral health education through WhatsApp for 4 weeks, with 2 sessions per week and each lasting no more than 15 min. Control Baseline oral health status of the participants. | - Oral health knowledge. + - Oral health perception. + - Geriatric Self-Efficacy Scale for Oral Health (GSEOH). + |
| Marino (2016), Australia [45] | Independent older adults in the community. (Age of recruited participants not specified.) (Gender of recruited participants not specified.) N = 75/47. Intervention: n = 47. No external control. | Intervention 10 oral health education modules were provided on a website over 10 weeks, 1 per week. Additional sessions were provided for a catch-up. Each session lasted from 27 to 38 min. Control Baseline oral health status of the participants. | - Oral health knowledge. + - Oral health perception. + - Self-defined self-efficacy score. + |
| Wanyonyi (2022), the United Kingdom [46] | Attendees of a dental clinic. 71.7 years old (mean). 85 male, 65 female. N = 150/68. Intervention: n = 40. Control: n = 28. | Intervention Three oral health education text messages per week for 10 weeks. Control Oral health education leaflets were delivered at the dental clinic. | - Perceived helpfulness of the program. - Willingness to recommend the program to others. - OHIP-14. ^ - 12-Item General Health Questionnaire (GHQ-12). + - Unspecified clinical assessments. ^ |
| Author (Year) | Format of Delivery (mHealth Technology), Length per Session (If Applicable) | Content Delivered | Reference(s) |
|---|---|---|---|
| Lee (2023) [42] | Audio–visual materials (mobile APP on smartphones). | - Oral health problems in old adulthood: dental caries and gingival disease; dry mouth and bad breath. - Oral management: toothbrushing and denture management; diet and smoking cessation; dental scaling and periodic oral check-ups. - Oral health education video on toothbrushing. - Interactive quizzes and workbooks. | [47] |
| Ki (2021) [43] | Audio–visual materials (mobile APP on smartphones), 50 min per session. | - Trot songs (a genre of Korean popular music) [48] adapted with oral health education script. - Oral exercise education consisting of oral gum exercises and tongue exercises. - Intraoral and extraoral massage. - Customized oral hygiene intervention, including brushing and denture care methods. - Self-care of oral health. - Interactive workbooks. | [49,50,51] |
| Khalil (2020) [44] | Audio–visual materials (mobile APP on smartphones), 15 min per session. | - Importance of oral health and its indicators. - Basic components of the oral cavity and age-related changes in the oral cavity. - Risk factors for oral health problems in older adults. - Gingivitis: causes, manifestations, and management. - Tooth decay: causes, stages, complications, and how to prevent it. - Halitosis: causes and management. - Dry mouth: causes, manifestations, and management. - Tooth sensitivity; causes, manifestations, and management. - Tooth brux: causes, manifestations, and management. - Dental neuritis: causes, manifestations, and management. - First aid for tooth fractures. - Mouth ulcer: causes, manifestations, and management. - Oral cancer: manifestations. - Steps of toothbrushing, care for a toothbrush, and tooth flossing. - Components of healthy food to maintain oral health. - How to care for dentures. - Guidelines to prevent oral health problems in older adults, steps of self-examination of the oral cavity. - Interactive WhatsApp groups. | [52,53,54,55,56] |
| Marino (2016) [45] | Audio–visual materials (web-based and accessible on smartphones or computers), 27 to 38 min per session. | - Oral health and aging. - Dental caries. - Periodontal disease. - Oral cancer. - What to do with remaining teeth. - Care of dentures. - Dry mouth (xerostomia). - Oral health and nutrition. - Use of oral healthcare services. - Oral health and general health. - Interactive quizzes. | [57,58] |
| Wanyonyi (2022) [46] | Text-only materials (SMS on smartphones). | - Toothbrushing behaviors. - Flossing. - Fluoride and mouth rinse to use. - Denture cleaning. - Dry mouth. | [59] |
| Author (Year) | Clinical Outcome(s) | Participant-Reported Outcome(s) | Qualitative Outcome(s) | Oral Health Knowledge Outcome(s) | Acceptability |
|---|---|---|---|---|---|
| Lee (2023) [42] | No significant improvement: - O’Leary Index. - Tongue coating. - Löe and Silness Index. | Not reported. | Not reported. | Significant improvement in oral health knowledge. | Not reported. |
| Ki (2021) [43] | Significant improvement: - Plaque Index. No significant improvement: - Number of functional teeth. - Tongue coating. | Significant improvement: - Oral dryness. - Swallowing-related quality of life (SWAL-QoL). - Tongue pressure. | Not reported. | Not reported. | Not reported. |
| Khalil (2020) [44] | Not reported | Not reported | Not reported. | Significant improvement in oral health literacy. | Not reported. |
| Marino (2016) [45] | Not reported | Not reported. | - Improved oral health awareness. - Improved oral health behaviors. - Improved oral health perceptions. - Participants were unsatisfied with non-individualized materials. | Significant improvement in oral health knowledge. | - Strong participant support. - Positive feedback on mHealth interventions. |
| Wanyonyi (2022) [46] | Not reported. | Significant improvement: - Willingness to use dental floss. | - Improved oral health awareness. - Improved oral health behaviors. - Improved oral health perceptions. | Not reported. | - High acceptance (89%) reported. |
| Author (Year) | Type of NIH Quality Assessment Tool (Detailed Assessment) | Quality Rating (Score) |
|---|---|---|
| Lee (2023) [42] | Controlled Intervention Studies (Table A1). | Fair (10/14) |
| Ki (2021) [43] | Controlled Intervention Studies (Table A2). | Fair (9/14) |
| Khalil (2020) [44] | Before–After (Pre–Post) Studies With No Control Group (Table A3). | Poor (8/12) |
| Marino (2016) [45] | Before–After (Pre–Post) Studies With No Control Group (Table A4) | Poor (6/12) 1 |
| Wanyonyi (2022) [46] | Controlled Intervention Studies (Table A5) | Poor (8/14) 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chau, R.C.W.; Thu, K.M.; Chaurasia, A.; Hsung, R.T.C.; Lam, W.Y.-H. A Systematic Review of the Use of mHealth in Oral Health Education among Older Adults. Dent. J. 2023, 11, 189. https://doi.org/10.3390/dj11080189
Chau RCW, Thu KM, Chaurasia A, Hsung RTC, Lam WY-H. A Systematic Review of the Use of mHealth in Oral Health Education among Older Adults. Dentistry Journal. 2023; 11(8):189. https://doi.org/10.3390/dj11080189
Chicago/Turabian StyleChau, Reinhard Chun Wang, Khaing Myat Thu, Akhilanand Chaurasia, Richard Tai Chiu Hsung, and Walter Yu-Hang Lam. 2023. "A Systematic Review of the Use of mHealth in Oral Health Education among Older Adults" Dentistry Journal 11, no. 8: 189. https://doi.org/10.3390/dj11080189