1. Introduction
The development of digital technology, viaCAD (computer-aideddesign) and CAM (computer-aided manufacturing) systems, contributed to the improvement and simplification ofboth diagnosis and treatment planning in orthodontics.
The three-stage process of the digital workflow includes the following: the acquisition of digital images of patients’ dental arches, the manipulation of these images usingspecific dental software, and finally, the 3D printing files [
1].
Orthodontic measurements from digital study models can be useful for assessing the need for orthodontic treatment and dental parameters, such as the Bolton index, and as already demonstrated in the literature, all analysed dental casts can potentially be transformed into 3D images [
2].
The Bolton analysis is carried out by orthodontists to measure possible disproportions between the upper and lower dental arches and was developed by Wayne Bolton in 1958 to measure the ideal ratio between the mesiodistal diameters of the teeth of the upper arch compared to those of the lower arch. The mesiodistal diameters, at the contact points, of all elements from the central incisors to the first molars must first be calculated for each dental arch.
Digital models could be used in decisionmaking and treatment planning [
3,
4], as there are many studies in the literature that support the validity of the digital measurements of the dental arches for the measurements of both the anterior and total coefficients of the Bolton analysis [
5,
6].
As demonstrated in the scientific literature [
7], the rotational and translational movements of teeth can be analysed and reproduced with great precision using digital configurations, and in more complex orthodontic treatments, a preliminary virtual plan has the potential to allow a significant reduction in errors with a greater probability of predicting the final orthodontic outcome.
Furthermore, digital technologies and artificial intelligence may allow greater opportunities for such planning, as they can be applied in the early stages of the clinical examination to develop a simultaneous virtual plan of all stages of treatment [
8].
Recently, it has been shown that 3D printing can be a method used todigitally design and then produce customisable clear aligners with greater precision as an alternative to conventional orthodontic appliances while also offering greater fit and effectiveness [
9].
In the present study, using an extraoral scanner and specific dental software, the average length values of the upper and lower jaws of adolescent patients were compared with those of a hypothetical nickel–titanium wire, and the accuracy of the measurements of the anterior and total Bolton index coefficients were calculated.
In the present retrospective study, dental cast models were already available; therefore, we decided to use an extraoral scanner instead of an intraoral scanner.
The aim of the study was to establish the average measurements of upper and lower arch lengths and the anterior and total Bolton coefficients of an Italian adolescent population. Moreover, the aim of this study was to evaluate the reliability of digital dental measurements.
2. Materials and Methods
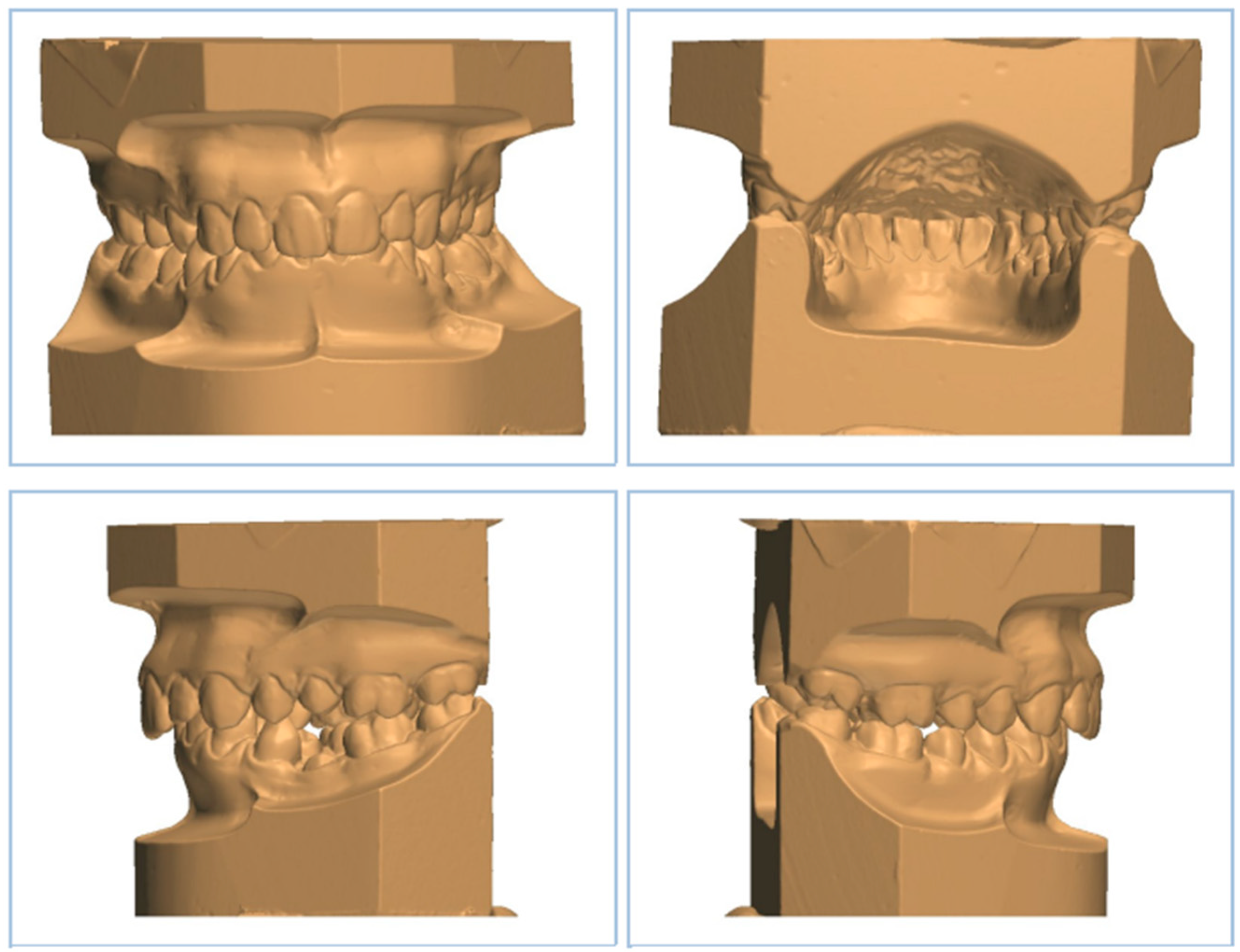
In the present study, all operations were carried out by the same operator who analysed the dental measurements of 138 dental casts using the Ortho3Shape software (
Figure 1).
The parameters that were measured are as follows: current length of the dental casts, length of a hypothetical nickel–titanium orthodontic wire, and anterior and total Bolton coefficients.
2.1. Selection Criteria
The inclusion criteria were as follows:
- -
Caucasian ethnicity;
- -
Permanent dentition;
- -
Class I and absence of severe malocclusions;
- -
Absence of dental extractions or extensive tooth reconstructions;
- -
Absence of previous maxillo-facial surgery;
- -
Absence of previous removable or fixed orthodontic treatments;
- -
Three-dimensional dental casts scanned usingOrtho3shape software.
The exclusion criteria were as follows:
- -
Presence of deciduous teeth;
- -
Teeth with severe rotation;
- -
Dental agenesis;
- -
Oligodontia.
2.2. Clinical Procedures
In the present study, the mesiodistal diameter of each tooth from the right canine to the left canine was measured to obtain the anterior Bolton index, both in the upper and in the lower dental arch.
Furthermore, in order to measure the total coefficient, the mesiodistal diameter of each tooth from the right molar to the left molar was measured.
The mean value of the length of a hypothetical nickel–titanium orthodontic wire of the upper and lower jaws was calculated on the basis of the dental cast measurements obtained usingthe Ortho3Shape software.
Then, the mean value was compared with the length of upper and lower dental arches.
Furthermore, to confirm the accuracy of the measurements of the anterior and total Bolton coefficients, our measurements were compared with those found in the study by A. Anand Kumar et al. [
10].
2.3. Statistical Analysis
Sample size calculation was performed with a confidence level of 95%, a power of 80%, a population variance of 1000, and a hypothesized difference of 10 based on the Bolton analysis of a previous study [
10].
Each measurement was evaluated twice by the same operator, with an interval of 2 weeks between the two evaluations. Intra-observer variability was calculated by using Cohen’s Kappa coefficient, and we found that the K coefficient was between 0.9 and 0.97.
The mean values of digital casts were measured, and Student’s T test was adopted with a level of significance set at p < 0.05.
The statistical analysis was carried outusing theSPSS (Statistical Package for Social Sciences, Chigago, IL, USA) 22.0 program.
The mean values of the anterior and total Bolton coefficients were compared with those obtained by A. Anand Kumar et al. in order to assess possible differences [
10].
The study conducted by A. Anand Kumar et al. included a sample of 50 adults with similar inclusion criteria of our study:
- -
Full permanent dentition from right first molar to left first molar in both the upper and lower arches;
- -
Absence of previous or current orthodontic treatment;
- -
Absence of severe dental crowding [
10].
Statistically significant differences were measured between the two groups by using Student’s t test (p < 0.05).
3. Results
The results of the present study are reported in
Table 1,
Table 2,
Table 3 and
Table 4. Moreover, the mean values of the anterior and total Bolton indexes were compared with those calculated by A. Anand Kumar et al. [
10] with respect to CBCT and dental casts (
Table 5).
3.1. Digitaldental Casts Analysis
We found that the length of the upper arch was 92.13 mm, while the mean value of a hypothetical length of a nickel–titanium orthodontic wire of the upper arch was 103.79 (
Table 1).
Moreover, it was observed that the length of the hypothetical nickel–titanium orthodontic wire of the upper arch was 11.66 mm longer than the one calculated usingdigital casts.
We observed that the lower arch measured on dental casts was 88.26 mm, while the mean value calculated for the hypothetical length of a nickel–titanium orthodontic wire was 94.71 mm (
Table 2).
It was observedthat the mean value of the hypothetical length of a nickel-titanium orthodontic wire of the lower arch was 6.45 mm longer than the one measured in the lower arch.
3.2. Bolton Analysis Comparison between Our Study and A. Anand Kumar et al.’s Study [10]
Anterior coefficient (Bolton): In the study by A. Anand Kumar et al., the mean value of the anterior Bolton coefficient of the 50 examined subjects was 0.76 for both CBCT and dental casts measurements while we obtained a value of 0.79 [
10] in our study (
Table 5).
Total coefficient (Bolton): In the study by A. Anand Kumar et al., the mean value of the total Bolton coefficient of the 50 examined subjects was 0.91 for both CBCT and dental casts measurements, while in our study, the value was 0.94 [
10] (
Table 5).
3.3. Comparisonof Anterior and Total Bolton Coefficients between the Two Studies
A significant difference was observed by the student t-test between the two studies both for the anterior coefficient (p: 0.0028; p < 0.05) and for the total coefficient (p: 0.0009; p < 0.05).
4. Discussion
In the present study, dental casts were digitized usinga 3D extraoral scanner to obtain STL (stereolithography:standard triangulation language) files viaCAD/CAM technology, which allows the surface data of the dental arches to be saved on the computer asthree-dimensional images [
11,
12,
13].
STL files can allow clinicians to quickly obtain information for diagnostic purposes [
14] and to digitally measure arch width, dental arches discrepancies, Bolton index discrepancies, overjet, and overbite. Moreover, they can be used for the simulation of teeth movements [
15,
16] and allow an efficient digital workflow with significant time savings for the orthodontist [
17,
18].
In addition, the importance of using a computer-aided design and manufacturing system in the indirect orthodontic bonding technique was previously demonstrated in the literature, and it guarantees high accuracy and precision [
19].
Furthermore, digital dental casts may be displayed with symmetrical bases in order to evaluate possible dental arch asymmetries and increase teeth measurement accuracy [
20].
In the present study, we evaluated the STL files of dental casts, and we performed a comparison between an ideal orthodontic wire and upper and lower dental arch lengths in a sample of adolescent patients.
We found that the average value of the length of a hypothetical orthodontic nickel–titanium wire of the ideal upper arch was 11.66 mm longer than the average value of the upper arch length that we measured on dental casts.
Furthermore, we observed that the average length value of anideal hypothetical lower arch nickel–titanium orthodontic wire was 6.45 mm longer than the average length value of the lower arch measured on dental casts.
A comparison was performed between the results of the present study and those found in the study of A. Anand Kumar et al. [
10] that included 50 patients, and we observed that the mean values of both the anterior and total coefficient of the Bolton index were very similar [
10]; therefore, we confirmed the reliability of the digital measurements performed usingorthodontic software. These measurements may be useful inestablishingthe average values of the upper and lower dental arches and the anterior and total Bolton index in an Italian adolescent population.
A limitation of the present study was the use of an extraoral scanner on wax dental casts instead of the use on an intraoral scanner. New intraoral scanners may be useful in future studiesthat aim toobtain dental arches measurements viaan easier and faster method.
5. Conclusions
The results of the present study showed that digital orthodontics and the reproduction of 3D digital models usingdental scanners are helpful for orthodontic diagnoses and treatment planning. These results confirm the findings of previous studies reported in the literature [
17,
18], and they are useful inestablishing the average measurements of the upper and lower arch lengths and the anterior and total Bolton coefficients of an Italian adolescent population.
In our study, the mean value of the anterior coefficients of the Bolton index was similar with those found in the study conducted by A. Anand Kumar et al., confirming the reliability of digital measurements [
10].
However, in future studies, it will be preferable to use intraoral scanners (IOSs) that ensure greater accuracy, requiring only one step and ensuring a better result for the patient in comparison to extraoral scanners.
Author Contributions
Conceptualization, M.P.; methodology, M.P.; validation, M.R.G.; formal analysis, E.C.; investigation, M.P.; resources, M.R.G.; data curation, F.G.; writing—original draft preparation, F.G.; writing—review and editing, D.T.; visualization, D.T.; supervision, E.C., D.T., M.R.G. and M.P.; project administration, M.R.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author [Pasini, M.; Carli, E.; Giambastiani, F.; Giuca, M.R.; Tripodi, D.], upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ardila, C.M.; Elorza-Durán, A.; Arrubla-Escobar, D. Efficacy of CAD/CAM Technology in Interventions Implemented in Orthodontics: A Scoping Review of Clinical Trials. Biomed. Res. Int. 2022, 2022, 5310555. [Google Scholar] [CrossRef] [PubMed]
- Bosio, J.A.; Rozhitsky, F.; Jiang, S.S.; Mukherjee, P.; Cangialosi, T.J. Comparison of Scanning Times for Different Dental Cast Materials Using an Intraoral Scanner; Rutgers School of Dental Medicine: Newark, NJ, USA, 2017. [Google Scholar]
- Ferreira, J.B.; Christovam, I.O.; Alencar, D.S.; da Motta, A.F.J.; Mattos, C.T.; Cury-Saramago, A. Accuracy and reproducibility of dental measurements on tomographic digital models: A systematic review and meta-analysis. Dentomaxillofac. Radiol. 2017, 46, 20160455. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, L.; Sabbagh, H.; Wichelhaus, A.; Kessler, A. Bracket transfer accuracy with two different three-dimensional printed transfer trays vs silicone transfer trays. Angle Orthod. 2022, 92, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zheng, Y.; Zhang, Z.; Zhang, Z.; Wu, L.; Liu, J.; Yang, W.; Wang, J. Customized maxillary incisor position relative to dentoskeletal and soft tissue patterns in Chinese women: A retrospective study. Korean J. Orthod. 2022, 52, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Kustrzycka, D.; Marschang, T.; Mikulewicz, M.; Grzebieluch, W. Comparison of the Accuracy of 3D Images Obtained fromDifferent Types of Scanners: A Systematic Review. J. Healthc. Eng. 2020, 2020, 8854204. [Google Scholar] [CrossRef] [PubMed]
- Sabbagh, H.; Heger, S.M.; Stocker, T.; Baumert, U.; Wichelhaus, A.; Hoffmann, L. Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy. Materials 2022, 15, 3853. [Google Scholar] [CrossRef] [PubMed]
- Nota, A.; Chegodaeva, A.D.; Ryakhovsky, A.N.; Vykhodtseva, M.A.; Pittari, L.; Tecco, S. One-Stage Virtual Plan of a Complex Orthodontic/Prosthetic Dental Rehabilitation. Int. J. Environ. Res. Public Health 2022, 19, 1474. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Phillip, A.; Kumar, S.; Rawat, A.; Priya, S.; Kumaran, V. Digital model as an alternative to plaster model in assessment of space analysis. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. S2), S465–S469. [Google Scholar] [CrossRef] [PubMed]
- Moura, W.; Henriques, J.F.C.; Gambardela-Tkacz, C.M.; Cotrin, P.; Garib, D.; Janson, G. Mandibular incisor inclination and gingival recession after treatment with the Jasper Jumper: A 10-year follow-up. Prog. Orthod. 2021, 22, 45. [Google Scholar] [CrossRef] [PubMed]
- De Morais Alves da Cunha, T.; da Silva Barbosa, I.; Palma, K.K. Orthodontic digital workflow: Devices and clinical applications. Dent. Press J. Orthod. 2021, 26, e21spe6. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.-N.; Lee, D.-H. Accuracy of Mobile Device-Compatible 3D Scanners for Facial Digitization: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e22228. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, T.; Marano, G.; Aulakh, R. Five-to-five clear aligner therapy: Predictable orthodontic movement for general dentist to achieve minimally invasive dentistry. BMC Oral Health 2021, 21, 671. [Google Scholar] [CrossRef] [PubMed]
- Pachêco-Pereira, C.; De Luca Canto, G.; Major, P.W.; Flores-Mir, C. Variation of orthodontic treatment decision-making based on dental model type: A systematic review. Angle Orthod. 2015, 85, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Faus-Matoses, I.; Barona, C.G.; Zubizarreta-Macho, Á.; Paredes-Gallardo, V.; Faus-Matoses, V. A Novel Digital Technique for Measuring the Accuracy of an Indirect Bonding Technique Using Fixed Buccal Multibracket Appliances. J. Pers. Med. 2021, 11, 932. [Google Scholar] [CrossRef] [PubMed]
- Jaber, S.T.; Hajeer, M.Y.; Khattab, T.Z.; Mahaini, L. Evaluation of the fused deposition modeling and the digital light processing techniques in terms of dimensional accuracy of printing dental models used for the fabrication of clear aligners. Clin. Exp. Dent. Res. 2021, 7, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Etemad-Shahidi, Y.; Qallandar, O.B.; Evenden, J.; Alifui-Segbaya, F.; Ahmed, K.E. Accuracy of 3-Dimensionally Printed Full-Arch Dental Models: A Systematic Review. J. Clin. Med. 2020, 9, 3357. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, G.; Campobasso, A.; Caldara, G.; Battista, G.; Lo Muzio, E.; Mandelli, G.; Ambrosi, A.; Gastaldi, G. Accuracy of 3-dimensional-printed customized transfer tray using a flash-free adhesive system in digital indirect bonding: An in vivo study. Am. J. Orthod. Dentofac. Orthop. 2023; in press. [Google Scholar]
- Proffit, W.R.; Fields, H.W., Jr.; Larson, B.; Sarver, D.M. Contemporary Orthodontics, 6th ed.; Elsevier: Filadelfia, PA, USA, 2019. [Google Scholar]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}