
The Effect of Third Molars on the Mandibular Anterior Crowding Relapse—A Systematic Review

 ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources, Search Strategy and Study Selection
2.3. Study Selection
2.4. Data Collection
2.5. Risk of Bias in Individual Studies
3. Results
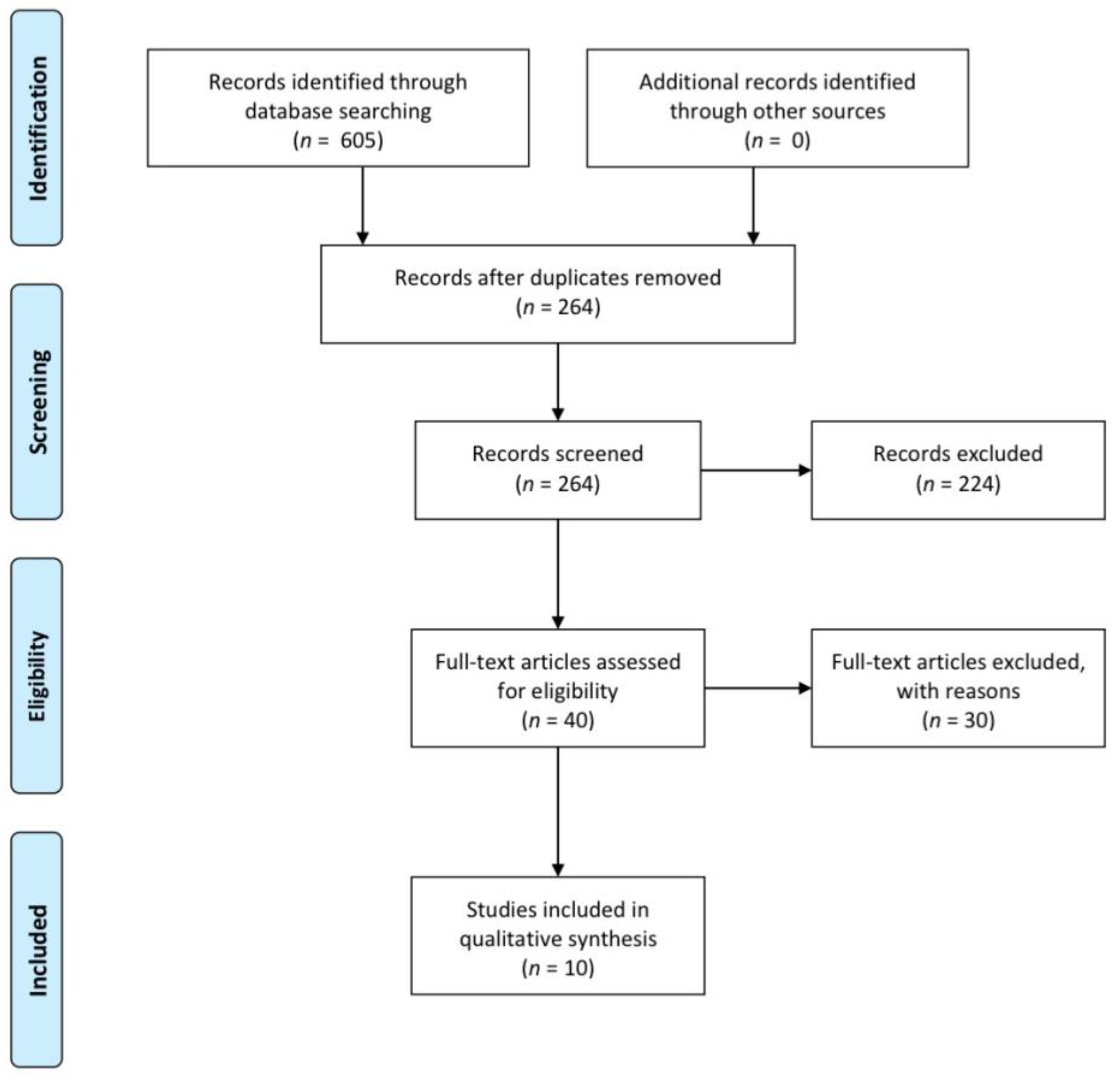
3.1. Study Selection
3.2. Study Characteristics
3.3. Within Studies Risk of Bias
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laskin, D.M. Evaluation of the third molar problem. J. Am. Dent. Assoc. 1971, 82, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Tüfekçi, E.; Svensk, D.; Kallunki, J.; Huggare, J.; Lindauer, S.J.; Laskin, D.M. Opinions of American and Swedish orthodontists about the role of erupting third molars as a cause of dental crowding. Angle Orthod. 2009, 79, 1139–1142. [Google Scholar] [CrossRef] [PubMed]
- Lindauer, S.J.; Laskin, D.M.; Tüfekçi, E.; Taylor, R.S.; Cushing, B.J.; Best, A.M. Orthodontists’ and surgeons’ opinions on the role of third molars as a cause of dental crowding. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Niedzielska, I. Third molar influence on dental arch crowding. Eur. J. Orthod. 2005, 27, 518–523. [Google Scholar] [CrossRef]
- Sidlauskas, A.; Trakiniene, G. Effect of the lower third molars on the lower dental arch crowding. Stomatologija 2006, 8, 80–84. [Google Scholar]
- Karasawa, L.H.; Rossi, A.C.; Groppo, F.C.; Prado, F.B.; Caria, P.H. Cross-sectional study of correlation between mandibular incisor crowding and third molars in young Brazilians. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e505–e509. [Google Scholar] [CrossRef] [PubMed]
- Mettes, T.G.; Nienhuijs, M.E.; van der Sanden, W.J.; Verdonschot, E.H.; Plasschaert, A.J. Interventions for treating asymptomatic impacted wisdom teeth in adolescents and adults. Cochrane Database Syst. Rev. 2005, 2, CD003879, Update in Cochrane Database Syst. Rev. 2012, 6, CD003879. [Google Scholar] [CrossRef]
- Zawawi, K.H.; Melis, M. The role of mandibular third molars on lower anterior teeth crowding and relapse after orthodontic treatment: A systematic review. Sci. World J. 2014, 2014, 615429. [Google Scholar] [CrossRef]
- Pithon, M.M.; Baião, F.C.S.; de Andrade Sant’Anna, L.I.D.; da Silva Coqueiro, R.; Maia, L.C. Influence of the presence, congenital absence, or prior removal of third molars on recurrence of mandibular incisor crowding after orthodontic treatment: Systematic review and meta-analysis. J. World Fed. Orthod. 2017, 6, 50–56. [Google Scholar] [CrossRef]
- Bishara, S.E.; Andreasen, G. Third molars: A review. Am. J. Orthod. 1983, 83, 131–137. [Google Scholar] [CrossRef]
- Richardson, M.E. The role of the third molar in the cause of late lower arch crowding: A review. Am. J. Orthod. Dentofac. Orthop. 1989, 95, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E. Third molars: A dilemma! Or is it? Am. J. Orthod. Dentofac. Orthop. 1999, 115, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Vasir, N.S.; Robinson, R.J. The mandibular third molar and late crowding of the mandibular incisors—A review. Br. J. Orthod. 1991, 18, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.C.; Peng, B.Y.; Hsieh, H.Y.; Tam, K.W. Impact of third molars on mandibular relapse in post-orthodontic patients: A meta-analysis. J. Dent. Sci. 2018, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fastlicht, J. Crowding of mandibular incisors. Am. J. Orthod. 1970, 58, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.G. Mandibular third molars and postretention crowding. Am. J. Orthod. 1974, 66, 411–430. [Google Scholar] [CrossRef]
- Ades, A.G.; Joondeph, D.R.; Little, R.M.; Chapko, M.K. A long-term study of the relationship of third molars to changes in the mandibular dental arch. Am. J. Orthod. Dentofac. Orthop. 1990, 97, 323–335. [Google Scholar] [CrossRef]
- Richardson, M.; Mills, K. Late lower arch crowding: The effect of second molar extraction. Am. J. Orthod. Dentofac. Orthop. 1990, 98, 242–246. [Google Scholar] [CrossRef]
- Little, R.M. Stability and relapse of mandibular anterior alignment: University of Washington studies. Semin. Orthod. 1999, 5, 191–204. [Google Scholar] [CrossRef]
- Van der Schoot, E.A.; Kuitert, R.B.; van Ginkel, F.C.; Prahl-Andersen, B. Clinical relevance of third permanent molars in relation to crowding after orthodontic treatment. J. Dent. 1997, 25, 167–169. [Google Scholar] [CrossRef]
- Harradine, N.W.; Pearson, M.H.; Toth, B. The effect of extraction of third molars on late lower incisor crowding: A randomized controlled trial. Br. J. Orthod. 1998, 25, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Cotrin, P.; Freitas, K.M.S.; Freitas, M.R.; Valarelli, F.P.; Cançado, R.H.; Janson, G. Evaluation of the influence of mandibular third molars on mandibular anterior crowding relapse. Acta Odontol. Scand. 2020, 78, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Al-Balkhi, K.M. The effect of different lower third molar conditions on the re-crowding of lower anterior teeth in the absence of tight interproximal contacts one-year post orthodontic treatment: A pilot study. J. Contemp. Dent. Pract. 2004, 5, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Southard, T.E.; Southard, K.A.; Weeda, L.W. Mesial force from unerupted third molars. Am. J. Orthod. Dentofac. Orthop. 1991, 99, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, K. Relationship between initial crowding and interproximal force during retention phase. J. Oral Sci. 2010, 52, 197–201. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Terada, K.; Kageyama, I.; Tsuchimochi, T.; Ishikawa, F.; Nakahara, S. Influence of third molar space on angulation and dental arch crowding. Odontology 2013, 101, 22–28. [Google Scholar] [CrossRef]
- Kahl-Nieke, B.; Fischbach, H.; Schwarze, C.W. Post-retention crowding and incisor irregularity: A long-term follow-up evaluation of stability and relapse. Br. J. Orthod. 1995, 22, 249–257. [Google Scholar] [CrossRef]
- Sheneman, J. Third molar teeth and their effect upon the lower anterior teeth; a study of forty-nine orthodontic cases 5 years after band removal. Am. J. Orthod. 1969, 55, 196. [Google Scholar] [CrossRef]
- Lindqvist, B.; Thilander, B. Extraction of third molars in cases of anticipated crowding in the lower jaw. Am. J. Orthod. 1982, 81, 130–139. [Google Scholar] [CrossRef]
- Richardson, M.E. Late lower arch crowding in relation to primary crowding. Angle Orthod. 1982, 52, 300–312. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ (Clin. Res. Ed.) 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 25 March 2023).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Massaro, C.; Miranda, F.; Janson, G.; Rodrigues de Almeida, R.; Pinzan, A.; Martins, D.R.; Garib, D. Maturational changes of the normal occlusion: A 40-year follow-up. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Yi, L.; Jeon, H.H.; Li, C.; Boucher, N.; Chung, C.H. Transverse Growth of the Maxillo-Mandibular Complex in Untreated Children: A Longitudinal Cone Beam Computed Tomography Study. Sensors 2021, 21, 6378. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E. Facial and dental changes in adolescents and their clinical implications. Angle Orthod. 2000, 70, 471–483. [Google Scholar] [CrossRef]
- Bishara, S.E.; Treder, J.E.; Damon, P.; Olsen, M. Changes in the dental arches and dentition between 25 and 45 years of age. Angle Orthod. 1996, 66, 417–422. [Google Scholar] [CrossRef]
- Garib, D.; Natsumeda, G.M.; Massaro, C.; Miranda, F.; Naveda, R.; Janson, G. Cephalometric changes during aging in subjects with normal occlusion. J. Appl. Oral Sci. 2021, 29, e20210199. [Google Scholar] [CrossRef]
- Richardson, M.E. A review of changes in lower arch alignment from seven to fifty years. Semin. Orthod. 1999, 5, 151–159. [Google Scholar] [CrossRef]
- Thilander, B. Dentoalveolar development in subjects with normal occlusion. A longitudinal study between the ages of 5 and 31 years. Eur. J. Orthod. 2009, 31, 109–120. [Google Scholar] [CrossRef]
- Tsiopas, N.; Nilner, M.; Bondemark, L.; Bjerklin, K. A 40 years follow-up of dental arch dimensions and incisor irregularity in adults. Eur. J. Orthod. 2013, 35, 230–235. [Google Scholar] [CrossRef]
- Flores-Mir, C.; Silva, E.; Barriga, M.I.; Valverde, R.H.; Lagravère, M.O.; Major, P.W. Laypersons’ perceptions of the esthetics of visible anterior occlusion. J. Can. Dent. Assoc. 2005, 71, 849. [Google Scholar] [PubMed]
- Gasparello, G.G.; Júnior, S.L.M.; Hartmann, G.C.; Meira, T.M.; Camargo, E.S.; Pithon, M.M.; Tanaka, O. The influence of malocclusion on social aspects in adults: Study via eye tracking technology and questionnaire. Prog. Orthod. 2022, 23, 4. [Google Scholar] [CrossRef]
- Tiro, A.; Nakas, E.; Arslanagic, A.; Markovic, N.; Dzemidzic, V. Perception of Dentofacial Aesthetics in School Children and Their Parents. Eur. J. Dent. 2021, 15, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Felemban, O.M.; Alharabi, N.T.; A Alamoudi, R.A.; Alturki, G.A.; Helal, N.M. Factors influencing the desire for orthodontic treatment among patients and parents in Saudi Arabia: A cross-sectional study. J. Orthod. Sci. 2022, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Relationship between Orthodontic Treatment Need and Oral Health-Related Quality of Life among 11⁻18-Year-Old Adolescents in Lithuania. Int. J. Environ. Res. Public. Health 2018, 15, 1012. [Google Scholar] [CrossRef] [PubMed]
- Laothong, W.; Cheng, H.C. Comparison of factors affecting orthodontic treatment motivation of Taiwanese and Thai patients in two hospitals. J. Dent. Sci. 2017, 12, 396–404. [Google Scholar] [CrossRef]
- Keles, F.; Bos, A. Satisfaction with orthodontic treatment. Angle Orthod. 2013, 83, 507–511. [Google Scholar] [CrossRef]
- Maia, N.G.; Normando, D.; Maia, F.A.; Ferreira, M.A.; do Socorro Costa Feitosa Alves, M. Factors associated with long-term patient satisfaction. Angle Orthod. 2010, 80, 1155–1158. [Google Scholar] [CrossRef]
- Littlewood, S.J.; Kandasamy, S.; Huang, G. Retention and relapse in clinical practice. Aust. Dent. J. 2017, 62 (Suppl. S1), 51–57. [Google Scholar] [CrossRef]
- Thilander, B. Biological basis for orthodontic relapse. Semin. Orthod. 2000, 6, 195–205. [Google Scholar] [CrossRef]
- Bjering, R.; Birkeland, K.; Vandevska-Radunovic, V. Anterior tooth alignment: A comparison of orthodontic retention regimens 5 years posttreatment. Angle Orthod. 2015, 85, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Maltha, J.C.; Vandevska-Radunovic, V.; Kuijpers-Jagtman, A.M. The biological background of relapse of orthodontic tooth movement. In Biological Mechanisms of Tooth Movement; Krishnan, V., Davidovitch, Z., Eds.; Wiley: Hoboken, NJ, USA, 2015. [Google Scholar] [CrossRef]
- Reitan, K. Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am. J. Orthod. 1967, 53, 721–745. [Google Scholar] [CrossRef] [PubMed]
- Taner, T.U.; Haydar, B.; Kavuklu, I.; Korkmaz, A. Short-term effects of fiberotomy on relapse of anterior crowding. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 617–623. [Google Scholar] [CrossRef]
- Lyros, I.; Tsolakis, I.A.; Maroulakos, M.P.; Fora, E.; Lykogeorgos, T.; Dalampira, M.; Tsolakis, A.I. Orthodontic Retainers-A Critical Review. Children 2023, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Blake, M.; Bibby, K. Retention and stability: A review of the literature. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Littlewood, S.J. Evidence-based retention: Where are we now? Semin. Orthod. 2017, 23, 229–236. [Google Scholar] [CrossRef]
- Angle, E.H. Treatment of Malocclusion of the Teeth: Angle’s System, 7th ed.; White Dental Manufacturing Co.: Philadelphia, PA, USA, 1907; Volume 3, pp. 11–17. [Google Scholar]
- Danz, J.C.; Greuter, C.; Sifakakis, I.; Fayed, M.; Pandis, N.; Katsaros, C. Stability and relapse after orthodontic treatment of deep bite cases-a long-term follow-up study. Eur. J. Orthod. 2014, 36, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Capelli, J., Jr. Mandibular growth and third molar impaction in extraction cases. Angle Orthod. 1991, 61, 223–229. [Google Scholar] [CrossRef]
- Milos, D.; Pavlic, A.; VandevskaRadunovic, V.; Zigante, M.; Matthewson, A.; Spalj, S. Craniofacial Growth in Adolescence and its Influence on the Mandibular Incisor Crowding. Acta Stomatol. Croat. 2021, 55, 37–44. [Google Scholar] [CrossRef]
- Sardarian, A.; Ghaderi, F. Prediction of the occurrence and severity of mandibular incisor crowding in the early mixed dentition using craniofacial parameters. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 701–707. [Google Scholar] [CrossRef]
- Björk, A.; Skieller, V. Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur. J. Orthod. 1983, 5, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Freitas, K.M.; de Freitas, M.R.; Henriques, J.F.; Pinzan, A.; Janson, G. Postretention relapse of mandibular anterior crowding in patients treated without mandibular premolar extraction. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 480–487. [Google Scholar] [CrossRef]
- Richardson, M.E. The etiology of late lower arch crowding alternative to mesially directed forces: A review. Am. J. Orthod. Dentofac. Orthop. 1994, 105, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Shigenobu, N.; Hisano, M.; Shima, S.; Matsubara, N.; Soma, K. Patterns of dental crowding in the lower arch and contributing factors. A statistical study. Angle Orthod. 2007, 77, 303–310. [Google Scholar] [CrossRef]
- Yilmaz, R.S.; Darling, A.I.; Levers, B.G.H. Mesial drift of human teeth assessed from ankylosed deciduous molars. Arch. Oral Biol. 1980, 25, 127–131. [Google Scholar] [CrossRef]
- Björk, A. Some biological aspects of prognathism and occlusion of the teeth. Acta Odontol. Scand. 1950, 9, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Buschang, P.H.; Shulman, J.D. Incisor crowding in untreated persons 15-50 years of age: United States, 1988–1994. Angle Orthod. 2003, 73, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Vaishali, S.; Kumar Jain, R.; Duraisamy, R. Prevalence and Associated Factors for Dental Arch Crowding in Mixed Dentition Cases Reporting to Private Dental College. Int. J. Dent. Oral Sci. 2020, 7, 1256–1260. [Google Scholar]
- Mockers, O.; Aubry, M.; Mafart, B. Dental crowding in a prehistoric population. Eur. J. Orthod. 2004, 26, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Normando, D.; Almeida, M.A.; Quintão, C.C. Dental crowding: The role of genetics and tooth wear. Angle Orthod. 2013, 83, 10–15. [Google Scholar] [CrossRef]
- Robinson, J. The causes of irregularities of the teeth. In Orthodontics: An Historical Review of Its Origin and Evolution; Weinberger, B.W., Ed.; The C. V. Mosby Company: St. Louis, MO, USA, 1926; Volume I, p. 325. [Google Scholar]
- Shanley, L.S. The influence of mandibular third molars on mandibular anterior teeth. Am. J. Orthod. 1962, 48, 786–787. [Google Scholar]
- Vego, L. A longitudinal study of mandibular arch perimeter. Angle Orthod. 1962, 32, 187–192. [Google Scholar]
- Zachrisson, B.U. Mandibular third molars and late lower arch crowding--the evidence base. World J. Orthod. 2005, 6, 180–186. [Google Scholar]
- Richardson, M. Pre-eruptive movements of the mandibular third molar. Angle Orthod. 1978, 48, 187–193. [Google Scholar] [CrossRef]
- Jung, Y.H.; Cho, B.H. Radiographic evaluation of third molar development in 6- to 24-year-olds. Imaging Sci. Dent. 2014, 44, 185–191. [Google Scholar] [CrossRef]
- Adler, P.; Adler-Hradecky, C. Eruption times of the upper and lower third molars. Acta Genet. Stat. Med. 1962, 12, 366–376. [Google Scholar] [CrossRef]
- Rakhshan, V. Congenitally missing teeth (hypodontia): A review of the literature concerning the etiology, prevalence, risk factors, patterns and treatment. Dent. Res. J. 2015, 12, 1–13. [Google Scholar] [CrossRef]
- Schonberger, S.; Shapira, Y.; Pavlidi, A.M.; Finkelstein, T. Prevalence and Patterns of Permanent Tooth Agenesis among Orthodontic Patients—Treatment Options and Outcome. Appl. Sci. 2022, 12, 12252. [Google Scholar] [CrossRef]
- Schwarze, C.W. The influence of third molar germectomy—A comparative long term study. In Transactions of the Third International Orthodontic Congress; Crosby Lockwood Staples: London, UK, 1973; pp. 551–562. [Google Scholar]
- Richardson, M.E. Orthodontic implications of lower third molar development. Dent. Update 1996, 23, 96–102. [Google Scholar]


{kind=link}
{kind=link}
| Articles | Population/Age Mean | Intervention | Compared With | Outcome of Interest of the Studies Method of Measurement | Method of Assessment | Results |
|---|---|---|---|---|---|---|
| Fastlicht, 1970 [15] | Total: 99, 60 F and39 M EG: 19 y 8 m; CG: 19 y 10 m | Participants with Class II, division 1 treated to normal occlusion. | EG: Orthodontic treatment (n = 28, 15 F, 13 M) CG: No orthodontic treatment (n = 28, 15 F, 13 M) | Mesiodistal incisor size, Intercanine width | Plaster models, cephalometric radiographs, photos before and after treatment | Crowding of mandibular incisors with existing 3rd molars: EG: p = 0.05 CG: p = 0.10 |
| Kaplan., 1974 [16] | Total: 75, 48 F and 27 M | Orthodontic treatment in Class I, Class II division 1, Class II division 2 malocclusion | Orthodontically treated subjects with mandibular 3rd molars: EG1: bilaterally erupted into function, EG2: bilaterally impacted, EG3: bilateral agenesis | Arch length, Intermolar width, Intercanine width, Lower anterior crowding, Lower anterior rotations, IMPA, Lower incisor x coordinate, Lower molar x coordinate | Plaster models Cephalometric analysis | No difference between groups |
| Ades et al., 1990 [17] | Total: 97 28 y 6 m | Orthodontic treatment in Class I, Class II division 1, Class II division 2 malocclusion | Orthodontically treated subjects with mandibular 3rd molars: EG1: impacted EG2: erupted into function EG3: congenitally absent EG4:extracted at least 10 y earlier | Irregularity index, Mandibular intercanine width, Mandibular arch length, Overbite, Overjet, IMPA, Lower incisor x coordinate, Lower incisor y coordinate, Lower incisor angle to x axis, Lower first molar x coordinate, Lower first molar y coordinate, Lower first molar angle to axis | Plaster models, Cephalometric analysis | Mandibular anterior crowding. EG1: 3rd molars erupted: x = 3.19; SD = 2.20 EG2: Bilateral 3rd molar impaction: x = 2.27; SD = 1.81 EG3: Bilateral 3rd molar agenesis: x = 2.55; SD = 1.40 EG4: Bilateral 3rd molar extraction: x = 3.25; SD = 5.34 (f = 0.3130) Intercanine width: returned to original dimension during postretention period (x: −1.7 ± 1.4 mm; p ≤ 0.01); Length of arch: diminished significantly in all groups without significant Difference between groups No difference between groups |
| Kahl-Nieke et al., 1995 [27] | Total: 226, 131 F and 95 M Pre-treatment: mean age 11.3 y; post-treatment: mean age 15.5 y; post-retention: mean age 31.2 y | Orthodontically treated subjects | T1: Pre-treatment, T2: Post-treatment, T3: Post-retention EG1: post-retention changes ≤3 mm, EG2: post-retention changes >3 mm | Intercanine width, Intermolar width, Arch length, Little irregularity index, Crowding, Overbite, Overjet, Occlusion | Plaster models | Slightly greater irregularity index in the 3rd molar group |
| van der Schoot et al., 1997 [20] | Total: 99, 60 F and 39 M Pre-treatment: mean 12.8 y; post-treatment: mean 15 y; post-retention: mean 22.3 y | Orthodontically treated subjects | EG1: Right 3rd molar (mandibular arch, n = 24; maxillary arch, n = 23), EG2: No erupted 3rd molar (mandibular arch, n = 19; maxillary arch, n = 22), EG3: Right and left 3rd molars extracted (mandibular arch, n = 47; maxillary arch, n = 37), EG4: One or both 3rd molars congenitally missing (mandibular arch, n = 8; maxillary arch, n = 7) | Arch length discrepancy of the maxillary and mandibular front/anterior teeth, Arch length discrepancy of the left and right premolar area, Irregularity index of maxillary and mandibular front/anterior teeth | Plaster models, Panoramic radiographs | No significant difference between the groups (t1, t2, and t3) regarding the irregularity index in both arches. Improvement between t1–t2, deterioration between t2–t3 (p > 0.5) |
| Harradine et al., 1998 [21] | Total: 77, 45 F and 32 M 14y 10 m | Orthodontically treated subjects without use of appliances and/or retainer bar | EG1: 3rd molar removed (n = 44), EG2: 3rd molar maintained (n = 33) | Little’s index of irregularity, Intercanine width, Arch length | Plaster models, Lateral cephalometric radiographs | Value of irregularity: 3rd molar extraction, 0.80 mm 3rd molar not extracted, 1.10 mm (p =0.55) Intercanine width: no clinical/statistical difference Arch length: small reduction, Small statistical difference (p = 0.0001) in the group with no extraction (2.1 mm) in comparison with the extraction group (1.1 mm) |
| Little, 1999 [19] | Patients pre-treatment, post-treatment, and 10 y post-retention. | EG1: Bilateral 3rd molar impaction (n = 14) EG2: Erupted 3rd molars (n = 32) EG3: Bilateral agenesis of 3rd molars (n = 17) | Incisal irregularity index, Arch length, Intercanine width | Plaster models, Lateral cephalometric radiographs | The incisal irregularity increased in all groups; Arch length: reduced in all groups; Intercanine width: reduced in all groups | |
| Al-Balkhi, 2004 [23] | Total: 32 14–19 y | Orthodontically treated subjects without retainer in the lower arch | EG1: Re-crowded lower incisors EG2: Uncrowded lower incisors | Crowding | Panoramic evaluation, plaster models. | EG1 ≈ EG2 |
| Okazaki, 2010 [25] | Total: 40, 36 F and 4 M mean 23.9 y | Orthodontically treated subjects with four premolars extracted, Wrap-around retainer | T1: 0–3 m T2: 3–6 m T3: 6–12 m T4: 12–18 m | Interproximal force (IPF) evaluation in mandibular anterior region Irregularity index | Mandibular arch Plaster casts | Correlations between IPF and irregularity index: T1, T2: p > 0.05 T3, T4: p < 0.05 |
| Cotrin et al., 2019 [22] | Total: 108 | Orthodontically treated subjects | T1: Pre-treatment T2: Post-treatment T3: At least 3y post-retention EG1: 72 (39 F, 33 M) EG2: 36 (18 F, 18 M) | Little’s irregularity index | Plaster casts | EG1 ≈ EG2 |
| Signalling Questions | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Summary |
| Fastlicht, 1970 [15] | L | H | L | H | L | L | L | L | L | H |
| Kaplan., 1974 [16] | H | L | U | L | U | U | U | L | L | H |
| Ades et al., 1990 [17] | H | H | L | L | L | L | L | L | L | H |
| Kahl-Nieke et al., 1995 [27] | H | H | U | L | U | U | U | L | L | H |
| van der Schoot et al., 1997 [20] | H | H | U | L | U | U | L | L | L | H |
| Harradine et al., 1998 [21] | L | L | L | L | L | L | L | L | L | L |
| Little 1999 [19] | H | H | U | H | U | U | U | U | L | H |
| Al-Balkhi, 2004 [23] | L | L | U | H | U | U | U | L | L | H |
| Okazaki, 2010 [25] | L | L | H | L | H | U | L | L | L | H |
| Cotrin et al., 2019 [22] | U | L | U | L | U | U | L | L | L | L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyros, I.; Vasoglou, G.; Lykogeorgos, T.; Tsolakis, I.A.; Maroulakos, M.P.; Fora, E.; Tsolakis, A.I. The Effect of Third Molars on the Mandibular Anterior Crowding Relapse—A Systematic Review. Dent. J. 2023, 11, 131. https://doi.org/10.3390/dj11050131
Lyros I, Vasoglou G, Lykogeorgos T, Tsolakis IA, Maroulakos MP, Fora E, Tsolakis AI. The Effect of Third Molars on the Mandibular Anterior Crowding Relapse—A Systematic Review. Dentistry Journal. 2023; 11(5):131. https://doi.org/10.3390/dj11050131
Chicago/Turabian StyleLyros, Ioannis, Georgios Vasoglou, Theodoros Lykogeorgos, Ioannis A. Tsolakis, Michael P. Maroulakos, Eleni Fora, and Apostolos I. Tsolakis. 2023. "The Effect of Third Molars on the Mandibular Anterior Crowding Relapse—A Systematic Review" Dentistry Journal 11, no. 5: 131. https://doi.org/10.3390/dj11050131