
Oral Manifestations in Monkeypox: A Scoping Review on Implications for Oral Health

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
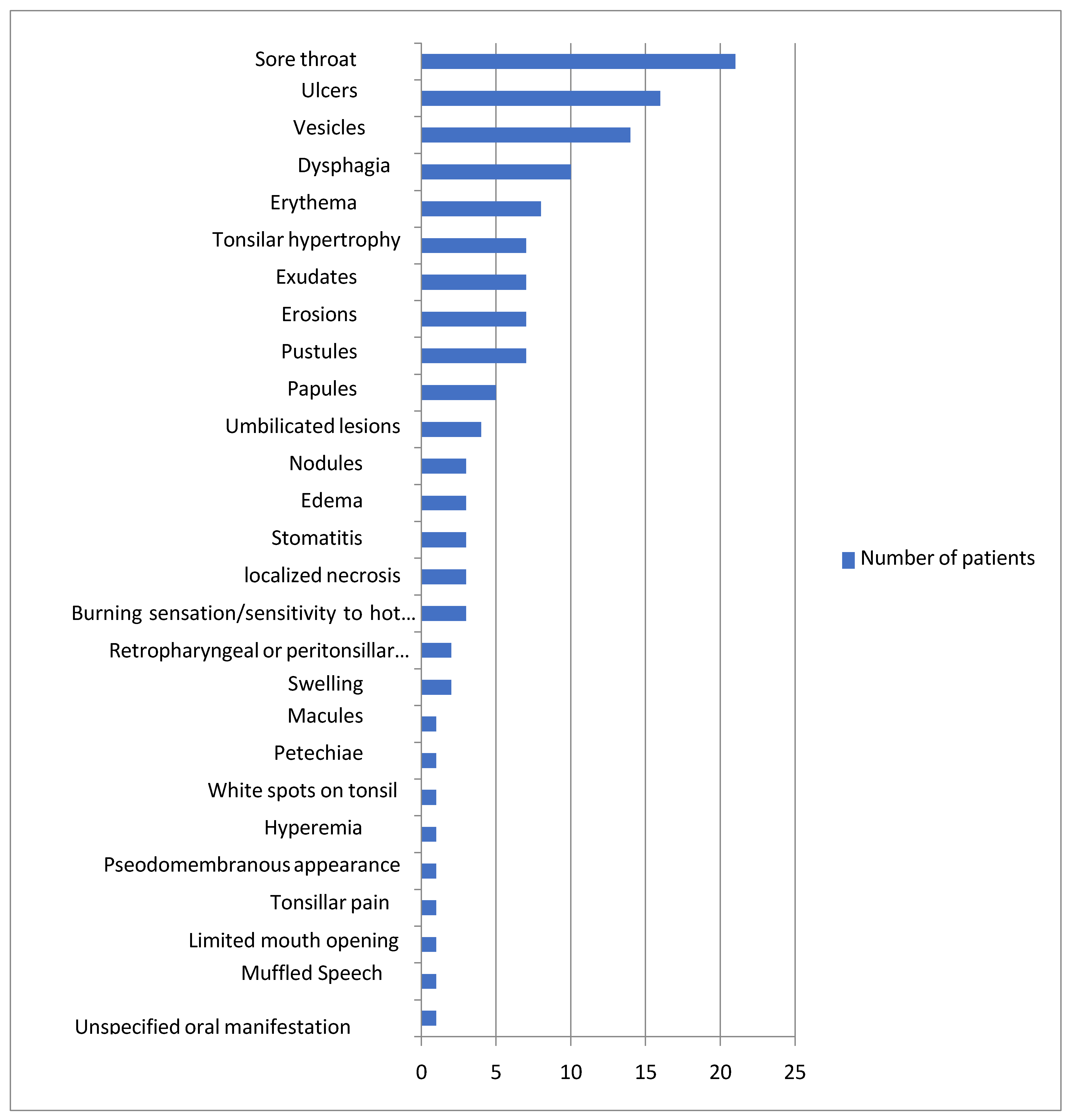
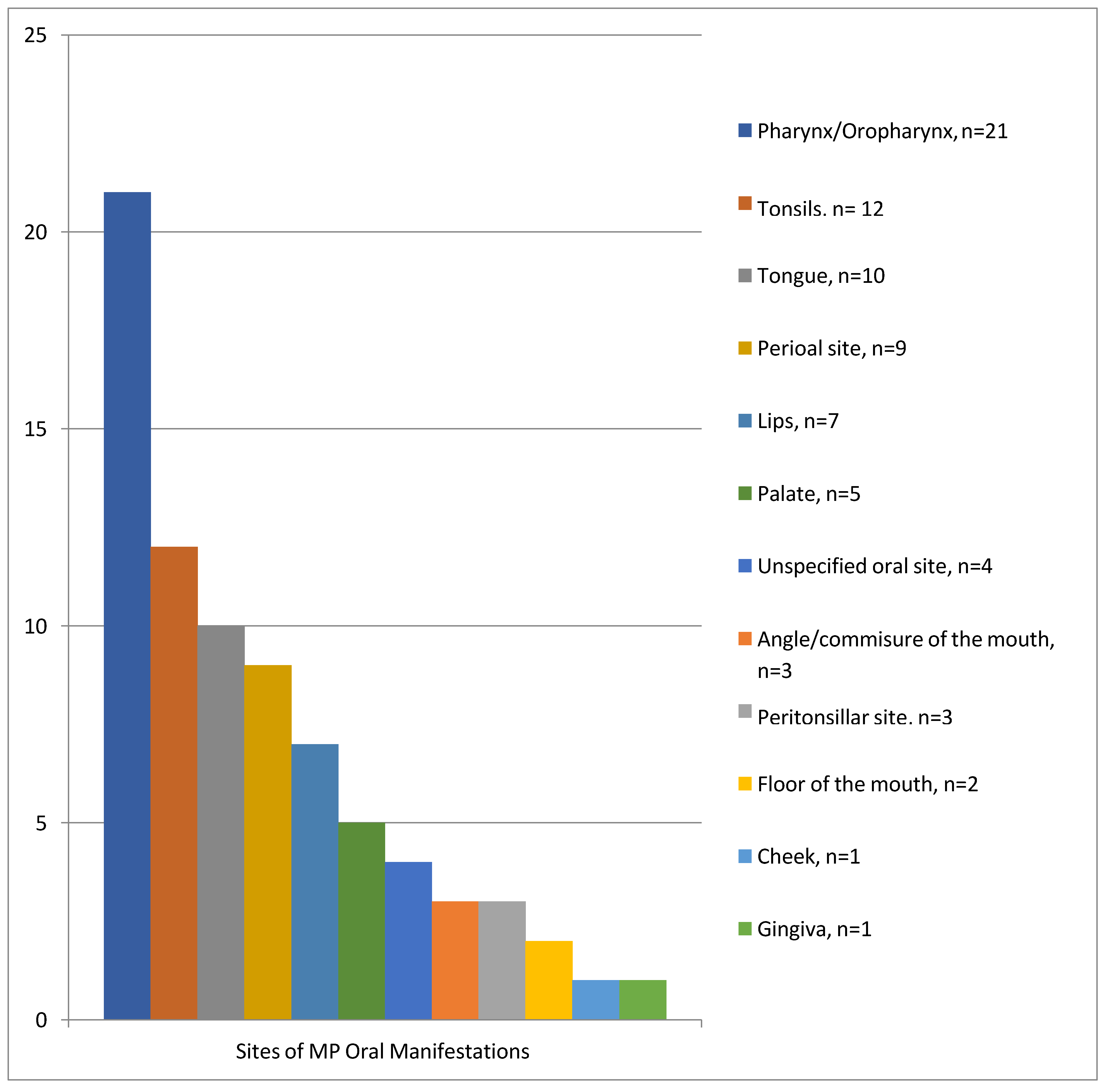
4.1. Oral Manifestations
4.2. Differential Diagnosis
4.2.1. Herpes Simplex Virus
4.2.2. Varicella Zoster Virus
4.2.3. Epstein-Barr Virus
4.2.4. Coxsackie Virus
4.2.5. Syphilis
4.2.6. Gonorrhea
4.2.7. Scarlet Fever
4.2.8. Tuberculosis
4.2.9. Management of Monkeypox
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- About Mpox. 22 July 2022. Available online: https://www.cdc.gov/poxvirus/monkeypox/about/index.html (accessed on 1 December 2022).
- Monkeypox: How It Spreads, Who’s at Risk—Here’s What You Need to Know|UN News. 2022. Available online: https://news.un.org/en/story/2022/07/1123212 (accessed on 1 December 2022).
- Cohen, J. Is an old virus up to new tricks? Science 1997, 277, 312–313. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, B.; Valdelvira, R.; Akdis, C.A. Monkeypox outbreak in Europe, UK, North America, and Australia: A changing trend of a zoonotic disease. Allergy 2022, 77, 2284–2286. [Google Scholar] [CrossRef] [PubMed]
- Multi-Country Monkeypox Outbreak: Situation Update. 2022. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396 (accessed on 1 December 2022).
- Antinori, A.; Mazzotta, V.; Vita, S.; Carletti, F.; Tacconi, D.; Lapini, L.E.; D’abramo, A.; Cicalini, S.; Lapa, D.; Pittalis, S.; et al. Epidemiological, clinical and virological characteristics of four cases of monkeypox support transmission through sexual contact, Italy, May 2022. Eurosurveillance 2022, 27, 2200421. [Google Scholar] [CrossRef] [PubMed]
- Kozlov, M. Monkeypox Goes Global: Why Scientists Are on Alert. 20 May 2022. Available online: https://www.nature.com/articles/d41586-022-01421-8 (accessed on 1 December 2022).
- Petersen, E.; Kantele, A.; Koopmans, M.; Asogun, D.; Yinka-Ogunleye, A.; Ihekweazu, C.; Zumla, A. Human Monkeypox. Infect. Dis. Clin. N. Am. 2019, 33, 1027–1043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, M.J.; Rathish, B.; Zahra, F. Mpox (Monkeypox). StatPearls 2022, 34662033. Available online: https://www.ncbi.nlm.nih.gov/books/NBK574519/ (accessed on 1 December 2022).
- Noe, S.; Zange, S.; Seilmaier, M.; Antwerpen, M.H.; Fenzl, T.; Schneider, J.; Spinner, C.D.; Bugert, J.J.; Wendtner, C.-M.; Wölfel, R. Clinical and virological features of first human monkeypox cases in Germany. Infection 2022, 51, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Monkeypox. 19 May 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 1 December 2022).
- La Voce di New York. Italy’s Monkeypox Cases Are All Men. 3 June 2022. Available online: https://lavocedinewyork.com/en/news/2022/06/03/italys-monkeypox-cases-are-all-men/ (accessed on 1 December 2022).
- Lanese, N. Monkeypox May Present with Unusual Symptoms, CDC Warns. 2 August 2022. Available online: https://www.livescience.com/unusual-monkeypox-symptoms-cdc (accessed on 1 December 2022).
- Hammerschlag, Y.; MacLeod, G.; Papadakis, G.; Sanchez, A.A.; Druce, J.; Taiaroa, G.; Savic, I.; Mumford, J.; Roberts, J.; Caly, L.; et al. Monkeypox infection presenting as genital rash, Australia, May 2022. Eurosurveillance 2022, 27, 2200411. [Google Scholar] [CrossRef]
- Ng, O.T.; Lee, V.; Marimuthu, K.; Vasoo, S.; Chan, G.; Lin, R.T.; Leo, Y.S. A case of imported monkeypox in Singapore. Lancet Infect. Dis. 2019, 19, 1166. [Google Scholar] [CrossRef]
- Reynolds, M.; McCollum, A.; Nguete, B.; ShongoLushima, R.; Petersen, B. Improving the Care and Treatment of Monkeypox Patients in Low-Resource Settings: Applying Evidence from Contemporary Biomedical and Smallpox Biodefense Research. Viruses 2017, 9, 380. [Google Scholar] [CrossRef] [Green Version]
- Iamaroon, A. Oral manifestations of Monkeypox: Brief review. Dent. Med. Probl. 2022, 59, 483–487. [Google Scholar] [CrossRef]
- Wiyeh, A.; Ochodo, E.; Dube, K.R.; Wiysonge, C. A scoping review of tools used to assess the quality of reporting of case report and case series studies. Abstr. 25th Cochrane Colloq. Edinb. UK Cochrane Database Syst. Rev. 2018, 9, CD201801. [Google Scholar] [CrossRef]
- Peters, S.M.; Hill, N.B.; Halepas, S. Oral manifestations of Monkeypox: A report of 2 cases. J. Oral Maxillofac. Surg. 2022, 80, 1836–1840. [Google Scholar] [CrossRef] [PubMed]
- Sejvar, J.J.; Chowdary, Y.; Schomogyi, M.; Stevens, J.; Patel, J.; Karem, K.; Fischer, M.; Kuehnert, M.J.; Zaki, S.R.; Paddock, C.D.; et al. Human Monkeypox Infection: A Family Cluster in the Midwestern United States. J. Infect. Dis. 2004, 190, 1833–1840. [Google Scholar] [CrossRef] [PubMed]
- Matias, W.R.; Koshy, J.M.; Nagami, E.H.; Kovac, V.; Moeng, L.R.; Shenoy, E.S.; Hooper, D.C.; Madoff, L.C.; Barshak, M.B.; Johnson, J.A.; et al. Tecovirimat for the Treatment of Human Monkeypox: An Initial Series From Massachusetts, United States. Open Forum Infect. Dis. 2022, 9, ofac377. [Google Scholar] [CrossRef]
- Ajmera, K.M.; Goyal, L.; Pandit, T.; Pandit, R. Monkeypox—An emerging pandemic. IDCases 2022, 29, e01587. [Google Scholar] [CrossRef] [PubMed]
- Costello, V.; Sowash, M.; Gaur, A.; Cardis, M.; Pasieka, H.; Wortmann, G.; Ramdeen, S. Imported Monkeypox from International Traveler, Maryland, USA, 2021. Emerg. Infect. Dis. 2022, 28, 1002–1005. [Google Scholar] [CrossRef]
- Anderson, M.G.; Frenkel, L.D.; Homann, S.; Guffey, J. A case of severe monkeypox virus disease in an American child: Emerging infections and changing professional values. Pediatr. Infect. Dis. J. 2003, 22, 1093–1096. [Google Scholar] [CrossRef]
- Reed, K.D.; Melski, J.W.; Graham, M.B.; Regnery, R.L.; Sotir, M.J.; Wegner, M.V.; Kazmierczak, J.J.; Stratman, E.J.; Li, Y.; Fairley, J.A.; et al. The Detection of Monkeypox in Humans in the Western Hemisphere. N. Engl. J. Med. 2004, 350, 342–350. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Martínez, Y.; Rodríguez-Morales, A.J.; Franco-Paredes, C.; Chastain, D.B.; Gharamti, A.A.; Barahona, L.V.; Henao-Martínez, A.F. Monkeypox—A description of the clinical progression of skin lesions: A case report from Colorado, USA. Ther. Adv. Infect. Dis. 2022, 9, 204993612211177. [Google Scholar] [CrossRef]
- Eisenstadt, R.; Liszewski, W.J.; Nguyen, C.V. Recognizing Minimal Cutaneous Involvement or Systemic Symptoms in Monkeypox. JAMA Dermatol. 2022, 158, 1457–1458. [Google Scholar] [CrossRef]
- Wong, K.; Chaudhary, M.; Magadia, R. A Case of Monkeypox Infection in an Unvaccinated HIV-Positive Male in Rural Alabama. Cureus 2022, 14, e31383. [Google Scholar] [CrossRef]
- Schlabe, S.; Boesecke, C.; Isselstein, J. Ulcer at corner of mouth as first sign of infection with monkeypox virus. Dtsch. Int. 2022, 119, 511. [Google Scholar] [CrossRef] [PubMed]
- Pisano, L.; Turco, M.; Mancuso, F.R.; Lastrucci, I.; Pimpinelli, N. Atypical oral presentation of Monkeypox virus: A report of two cases from Florence, Italy. Travel Med. Infect. Dis. 2022, 50, 102457. [Google Scholar] [CrossRef] [PubMed]
- Ambrogio, F.; Laface, C.; De Caro, A.P.; Loconsole, D.; Centrone, F.; Lettini, T.; Cazzato, G.; Bonamonte, D.; Foti, C.; Chironna, M.; et al. Peri-oral Monkeypox Virus Infection: A Clinical Report with Confirmatory Polymerase Chain Reaction Findings. Vaccines 2022, 11, 36. [Google Scholar] [CrossRef] [PubMed]
- Pisano, L.; Lagi, F.; Turco, M.; Gaggioli, S.; Bartoloni, A.; Pimpinelli, N. Monkeypox: A novel pitfall in clinical dermatology. Travel Med. Infect. Dis. 2022, 50, 102480. [Google Scholar] [CrossRef] [PubMed]
- Crosato, A.; Bertolozzi, G.; Zanetti, E.; Ricchetti, R.; Bellinvia, M. Monkeypox virus infection in an Italian man: A case report. J. Med. Case Rep. 2023, 17, 37. [Google Scholar]
- Eltvedt, A.K.; Christiansen, M.; Poulsen, A. A case report of Monkeypox in a 4-year-old boy from the DR Congo: Challenges of diagnosis and management. Case Rep. Pediatr. 2020, 2020, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Jang, Y.R.; Lee, M.; Shin, H.; Kim, J.-W.; Choi, M.-M.; Kim, Y.M.; Kim, J.; Na, H.K. The First Case of Monkeypox in the Republic of Korea. J. Korean Med. Sci. 2022, 37, e224. [Google Scholar] [CrossRef]
- Yadav, P.D.; Reghukumar, A.; Sahay, R.R.; K, S.; Shete, A.M.; Raman, A.; Vk, P.; Abraham, P.; Benson, R.; Sm, S.; et al. First two cases of Monkeypox virus infection in travellers returned from UAE to India, July 2022. J. Infect. 2022, 85, e145–e148. [Google Scholar] [CrossRef]
- Vaughan, A.; Aarons, E.; Astbury, J.; Balasegaram, S.; Beadsworth, M.; Beck, C.R.; Chand, M.; O’connor, C.; Dunning, J.; Ghebrehewet, S.; et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Eurosurveillance 2018, 23, 1800509. [Google Scholar] [CrossRef] [Green Version]
- Amos, D.; Collins, J.; Walker, D.T. Monkeypox presenting as supraglottitis in an immunocompromised patient. BMJ Case Rep. 2023, 16, e252213. [Google Scholar] [CrossRef] [PubMed]
- Oprea, C.; Ianache, I.; Piscu, S.; Tardei, G.; Nica, M.; Ceausu, E.; Popescu, C.P.; Florescu, S.A. First report of monkeypox in a patient living with HIV from Romania. Travel Med. Infect. Dis. 2022, 49. [Google Scholar] [CrossRef] [PubMed]
- Bížová, B.; Veselý, D.; Trojánek, M.; Rob, F. Coinfection of syphilis and monkeypox in HIV positive man in Prague, Czech Republic. Travel Med. Infect. Dis. 2022, 49, 102368. [Google Scholar] [CrossRef] [PubMed]
- Davido, B.; D’anglejan, E.; Baudoin, R.; Dahmane, L.; Chaud, A.; Cortier, M.; Vauloup-Fellous, C.; De Truchis, P.; Ghosn, J. Monkeypox outbreak 2022: An unusual case of peritonsillar abscess in a person previously vaccinated against smallpox. J. Travel Med. 2022, 29. [Google Scholar] [CrossRef]
- Benslama, L.; Foy, J.; Bertolus, C. Monkeypox oral lesions. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 596. [Google Scholar] [CrossRef]
- de Lima, E.L.; Barra, L.A.C.; Borges, L.M.S.; Medeiros, L.A.; Tomishige, M.Y.S.; Santos, L.d.S.L.A.; da Silva, A.J.D.; Rodrigues, C.C.M.; de Azevedo, L.C.F.; Villas-Boas, L.S.; et al. First case report of monkeypox in Brazil: Clinical manifestations and differential diagnosis with sexually transmitted infections. Rev. Inst. Med. Trop. Sao Paulo 2022, 64, e54. [Google Scholar] [CrossRef]
- Lopes, P.S.; Haddad, G.R.; Miot, H.A. Sexually-transmitted monkeypox: Report of two cases. An. Bras. De Dermatol. 2022, 97, 783–785. [Google Scholar] [CrossRef]
- Martins-Filho, P.R.; de Souza, M.F.; Góis, M.A.O.; Bezerra, G.V.B.; Gonçalves, C.C.A.; Nascimento, R.d.S.; Valdez, C.F.; Tanuri, A.; Damaso, C.R.; dos Santos, C.A. Unusual epidemiological presentation of the first reports of monkeypox in a low-income region of Brazil. Travel Med. Infect. Dis. 2022, 50, 102466. [Google Scholar] [CrossRef]
- de Sousa, D.; Patrocínio, J.; Frade, J.; Correia, C.; Borges-Costa, J.; Filipe, P. Human monkeypox coinfection with acute HIV: An exuberant presentation. Int. J. STD AIDS 2022, 33, 936–938. [Google Scholar] [CrossRef]
- Lucer, K.; Romero, J.; Torres, C. Two cases of monkeypox in Colombia. Rev. Da Soc. De Med. Trop. 2022, 55, e0637. [Google Scholar]
- Gandhi, P.A.; Patro, S.K.; Sandeep, M.; Satapathy, P.; Shamim, M.A.; Kumar, V.; Aggarwal, A.K.; Padhi, B.K.; Sah, R. Oral manifestation of the Monkeypox virus: A systematic review and meta-analysis. Eclinicalmedicine 2023, 56, 101817. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Fontoura, D.D.S.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; et al. Clinical features and novel presentations of human Monkeypox in a central London Centre during the 2022 outbreak: Descriptive case series. BMJ 2022, 378, e072410. [Google Scholar] [CrossRef] [PubMed]
- Girometti, N.; Byrne, R.; Bracchi, M.; Heskin, J.; McOwan, A.; Tittle, V.; Gedela, K.; Scott, C.; Patel, S.; Gohil, J.; et al. Demographic and clinical characteristics of confirmed human monkeypox virus cases in individuals attending a sexual health centre in London, UK: An observational analysis. Lancet Infect. Dis. 2022, 22, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Català, A.; Clavo-Escribano, P.; Riera-Monroig, J.; Martín-Ezquerra, G.; Fernandez-Gonzalez, P.; Revelles-Peñas, L.; Simon-Gozalbo, A.; Rodríguez-Cuadrado, F.J.; Castells, V.G.; Gomar, F.J.D.L.T.; et al. Monkeypox outbreak in Spain: Clinical and epidemiological findings in a prospective cross-sectional study of 185 cases. Br. J. Dermatol. 2022, 187, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: A prospective observational cohort study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef]
- Ogoina, D.; Izibewule, J.H.; Ogunleye, A.; Ederiane, E.; Anebonam, U.; Neni, A.; Oyeyemi, A.; Etebu, E.N.; Ihekweazu, C. The 2017 human monkeypox outbreak in Nigeria—Report of outbreak experience and response in the Niger Delta University Teaching Hospital, Bayelsa State, Nigeria. PLoS ONE 2019, 14, e0214229. [Google Scholar] [CrossRef] [Green Version]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox virus infection across 16 countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Smallpox. 8 February 2022. Available online: https://www.cdc.gov/smallpox/index.html (accessed on 1 March 2023).
- Harberger, S.; Graber, M. Bacterial Pharyngitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Somro, A.; Akram, M.; Khan, M.I.; Asif, H.M.; Abdul, S.; Shah, S.M.A.; Shaheen, G.; Ahmad, K.; Ur Rehman, M.R. Pharyngitis and sore throat: A review. Afr. J. Biotechnol. 2011, 10, 6190–6197. [Google Scholar]
- Middleton, D.B. An approach to pediatric upper respiratory infections. Am. Fam. Physician 1991, 44, 33–40. [Google Scholar]
- Stillerman, M.; Bernstein, S.H. Streptococcal pharyngitis. Evaluation of clinical syndromes in diagnosis. Am. J. Dis. Child. 1961, 101, 476–489. [Google Scholar] [CrossRef]
- Saini, M.; Brizuela, M. Bacterial Infections of the Oral Mucosa. [Updated 2023 Mar 19]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK574500/ (accessed on 1 March 2023).
- Johnston, C.; Corey, L. Current Concepts for Genital Herpes Simplex Virus Infection: Diagnostics and Pathogenesis of Genital Tract Shedding. Clin. Microbiol. Rev. 2016, 29, 149–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darji, K.; Frisch, S.; Boakye, E.A.; Siegfried, E. Characterization of children with recurrent eczema herpeticum and response to treatment with interferon-gamma. Pediatr. Dermatol. 2017, 34, 686–689. [Google Scholar] [CrossRef] [PubMed]
- Van Heerden, W. Oral manifestations of viral infections. S. Afr. Fam. Pract. 2006, 48, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Ragab, N.F.; Habib, M.A.; Ghozzi, M.Y. Serological Assessment of Acyclovir Treatment of Herpes Genitalis. Arch. Androl. 1989, 23, 147–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The UNITY Study Group. Assessment of the efficacy and safety of Tecovirimat in patients with monkeypox virus disease (UNITY). Lancet Infect. Dis. 2021, 21, 713–722. [Google Scholar]
- Freer, G.; Pistello, M. Varicella-zoster virus infection: Natural history, clinical manifestations, immunity and current and future vaccination strategies. New Microbiol. 2018, 41, 95–105. [Google Scholar]
- Centers for Disease Control and Prevention. Chickenpox (Varicella) for Healthcare Professionals. Centers for Disease Control and Prevention. 21 October 2022. Available online: https://www.cdc.gov/chickenpox/hcp/index.htm (accessed on 5 March 2023).
- Portilla-Robertson, J.; Ramos-Baena, J.D.; Jacinto-Alemán, L.F.; Leyva-Huerta, E.R. Epstein–Barr virus-positive ulcer in the oral cavity. J. Oral Maxillofac. Pathol. 2021, 25 (Suppl. S1), S46–S50. [Google Scholar] [CrossRef]
- Cohen, J.I. Optimal treatment for chronic active Epstein-Barr virus disease. Pediatr. Transplant. 2009, 13, 393–396. [Google Scholar] [CrossRef] [Green Version]
- Kimura, H.; Hoshino, Y.; Hara, S.; Sugaya, N.; Kawada, J.; Shibata, Y.; Kojima, I.S.; Nagasaka, T.; Kuzushima, K.; Morishima, T. Differences between T cell-type and natural killer cell-type chronic active Epstein-Barr virus infection. J. Infect. Dis. 2005, 191, 531–539. [Google Scholar] [CrossRef]
- Saoji, V.A. Hand, foot and mouth disease in Nagpur. Indian J. Dermatol. Venereol. Leprol. 2008, 74, 133–135. [Google Scholar] [CrossRef]
- Guerra, A.M.; Orille, E.; Waseem, M. Hand Foot and Mouth Disease. [Updated 2022 Oct 9]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK431082/ (accessed on 2 March 2023).
- Nelson, B.R.; Edinur, H.A.; Abdullah, M.T. Compendium of hand, foot and mouth disease data in Malaysia from years 2010–2017. Data Brief 2019, 24, 103868. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.-H.; Huang, S.-W.; Hsieh, W.-S.; Cheng, C.-K.; Chang, C.-F.; Wang, Y.-F.; Wang, J.-R. Enterovirus A71 Containing Codon-Deoptimized VP1 and High-Fidelity Polymerase as Next-Generation Vaccine Candidate. J. Virol. 2019, 93, e02308–e02318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saguil, A.; Kane, S.F.; Lauters, R.; Mercado, M.G. Hand-Foot-and-Mouth Disease: Rapid Evidence Review. Am. Fam. Physician 2019, 100, 408–414. [Google Scholar] [PubMed]
- Kim, B.; Moon, S.; Bae, G.R.; Lee, H.; Pai, H.; Oh, S.H. Factors associated with severe neurologic complications in patients with either hand-foot-mouth disease or herpangina: A nationwide observational study in South Korea, 2009–2014. PLoS ONE 2018, 13, e0201726. [Google Scholar] [CrossRef]
- Mohapatra, S.; Mohandas, R. Monkeypox and hand-foot-mouth disease outbreak in India: A double trouble? J. Pure Appl. Microbiol. 2022, 16 (Suppl. S1), 3138–3143. [Google Scholar] [CrossRef]
- B’krong, N.T.T.C.; Minh, N.N.Q.; Qui, P.T.; Chau, T.T.H.; Nghia, H.D.T.; Do, L.A.H.; Nhung, N.N.; Chau, N.V.V.; Thwaites, G.; Van Tan, L.; et al. Enterovirus serotypes in patients with central nervous system and respiratory infections in Viet Nam 1997–2010. Virol. J. 2018, 15, 69. [Google Scholar] [CrossRef]
- Abedi, G.R.; Watson, J.T.; Pham, H.; Nix, W.A.; Oberste, M.S.; Gerber, S.I. Enterovirus and Human Parechovirus Surveillance—United States, 2009–2013. MMWR. Morb. Mortal. Wkly. Rep. 2015, 64, 940–943. [Google Scholar] [CrossRef]
- Takeuchi, Y.; Nihon, R. Herpangina. Jpn. J. Clin. Med. 2007, 65 (Suppl. S3), 355–358. [Google Scholar]
- Tudor, M.E.; Al Aboud, A.M.; Leslie, S.W.; Gossman, W. Syphilis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ficarra, G.; Carlos, R. Syphilis: The renaissance of an old disease with oral implications. Head Neck Pathol. 2009, 3, 195–206. [Google Scholar] [CrossRef] [Green Version]
- Leuci, S.; Martina, S.; Adamo, D.; Ruoppo, E.; Santarelli, A.; Sorrentino, R.; Favia, G. Mignogna Oral Syphilis: A retrospective analysis of 12 cases and a review of the literature. Oral Dis. 2013, 19, 738–746. [Google Scholar] [CrossRef]
- Eccleston, K.; Collins, L.; Higgins, S.P. Primary syphilis. Int. J. Std. Aids. 2008, 19, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Minhas, S.; Sajjad, A.; Kashif, M.; Taj, F.; Waddani, H.A.; Khurshid, Z. Oral Ulcers Presentation in Systemic Diseases: An Update. Open Access Maced. J. Med. Sci. 2019, 7, 3341–3347. [Google Scholar] [CrossRef] [Green Version]
- Mortazavi, H.; Safi, Y.; Baharvand, M.; Rahmani, S. Diagnostic Features of Common Oral Ulcerative Lesions: An Updated Decision Tree. Int. J. Dent. 2016, 2016, 7278925. [Google Scholar] [CrossRef] [Green Version]
- Compilato, D.; Amato, S.; Campisi, G. Resurgence of syphilis: A diagnosis based on unusual oral mucosa lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, e45–e49. [Google Scholar] [CrossRef] [PubMed]
- Mungmunpuntipantip, R.; Wiwanitkit, V. Syphilis and Monkeypox: An Issue in Sexual Medicine. Medeni. Med. J. 2022, 37, 298–299. [Google Scholar] [CrossRef] [PubMed]
- Springer, C.; Salen, P. Gonorrhea. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Javanbakht, M.; Westmoreland, D.; Gorbach, P. Factors Associated With Pharyngeal Gonorrhea in Young People: Implications for Prevention. Sex. Transm. Dis. 2018, 45, 588–593. [Google Scholar] [CrossRef]
- Managing scarlet fever. Drug Ther. Bull. 2017, 55, 102. [CrossRef]
- Chalker, V.; The Scarlet Fever Incident Management Team; Jironkin, A.; Coelho, J.; Al-Shahib, A.; Platt, S.; Kapatai, G.; Daniel, R.; Dhami, C.; Laranjeira, M.; et al. Genome analysis following a national increase in Scarlet Fever in England 2014. BMC Genom. 2017, 18, 224. [Google Scholar] [CrossRef] [Green Version]
- Hübner, J.; Jansson, A. Scharlach-Alarm. Lassen Sie sichnichtverrücktmachen! [Scarlet fever]. MMW Fortschritte der Medizin. 2012, 154, 57–58. [Google Scholar] [CrossRef]
- Mpox (Monkeypox): Diagnostic Testing. GOV.UK. (n.d.). Available online: https://www.gov.uk/guidance/monkeypox-diagnostic-testing (accessed on 5 March 2023).
- Centers for Disease Control and Prevention. Rheumatic Fever: All You Need to Know. Centers for Disease Control and Prevention. 27 June 2022. Available online: https://www.cdc.gov/groupastrep/diseases-public/rheumatic-fever.html (accessed on 5 March 2023).
- Pekiner, F.N.; Erseven, G.; Borahan, M.O.; Gümrü, B. Natural barrier in primary tuberculosis inoculation: Oral mucous membrane. Int. J. Tuberc. Lung Dis. 2006, 10, 1418. [Google Scholar]
- Eng, H.L.; Lu, S.Y.; Yang, C.H.; Chen, W.J. Oral tuberculosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 81, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Nuwal, P.; Gupta, M.L.; Gupta, R.C.; Dixit, R.K. Primary tuberculosis of soft palate. Indian J. Chest Dis. Allied Sci. 2001, 43, 119–121. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention. TB Testing & Diagnosis. Centers for Disease Control and Prevention. 3 May 2022. Available online: https://www.cdc.gov/tb/topic/testing/default.htm (accessed on 5 March 2023).
- Centers for Disease Control and Prevention. Monkeypox: Information for Clinicians. 2023. Available online: https://www.cdc.gov/poxvirus/mpox/clinicians/treatment.html (accessed on 13 March 2023).
- Centers for Disease Control and Prevention. Monkeypox: Information for Clinicians—Pain Management. 2022. Available online: https://www.cdc.gov/poxvirus/mpox/clinicians/pain-management.html (accessed on 13 March 2023).
- World Health Organization. Clinical Management and Infection Prevention and Control for Monkeypox: Interim Rapid Response Guidance. 2022. Available online: https://www.who.int/publications/i/item/WHO-MPX-Clinical-and-IPC-2022.1 (accessed on 13 March 2023).



{kind=link}
{kind=link}
| Author and Year of Publication | Study Design | Country | Number of Patients | Gender | Age | Number of Patients with Oral/Perioral Manifestations | Oral/Perioral Manifestation | Oral/Perioral Manifestation Site | Treatment | Oral or Perioral Manifestation as One of the Initial Signs/Symptoms of the Disease |
|---|---|---|---|---|---|---|---|---|---|---|
| Anderson et al., 2003 [24] | Case report | USA | 1 | Female (1) | School age | 1 | Red macules, vesicles, retropharyngeal phlegmon, dysphagia, and sore throat | Macules in the mouth and pharynx, vesicles on the tongue and peritonsillar area, abscess in the retropharyngeal area, and sore throat (pharynx) | IV ampicillin/sulbactam | No |
| Reed et al., 2004 [25] | Case series | USA | 11 | Male (5), Female (6) | 3–43 years old | 10 | Sore throat: 55% (n = 6), Pharyngitis: 27% (n = 3), tonsillar hypertrophy: 18% (n = 2), tonsillar erosions: 18% (n = 2), and other lesions in the buccal mucosa (frequency was not mentioned) | Pharynx (n = 6), tonsils (n = 4), and lesions found on the buccal mucosa (frequency was not mentioned) | IV acyclovir, valacyclovir | No |
| Sejvar et al., 2004 [20] | Case series | USA | 3 | Male (1), Female (2) | 33 years old (male) | 3 | Sore throat | Pharynx | No medical care was provided | No |
| 30 years old (female) | Papule and sore throat | Papule in the cheek, and sore throat (pharynx) | Bolus of Prednisone, resulting in subsequent improvement in dyspnea | Yes | ||||||
| 6 years old (female) | Enlarged tonsils; pharyngeal erythema and edema; profuse, thick exudates; and sore throat | Tonsils and pharynx | Antimicrobial treatment (cefdinir), antipyretics, lorazepam, IV ceftriaxone, IV acyclovir, IV phenobarbital, and IV midazolam | No | ||||||
| Vaughan et al., 2018 [37] | Case report | UK | 2 | Male (2) | Middle-aged | 1 | Vesicles | Vesicles on the mucosal surface of the mouth | NM | No |
| Middle-aged | No oral/perioral manifestation | No oral/perioral manifestation | NM | No | ||||||
| Eltvedt et al., 2020 [34] | Case report | Republic of Congo | 1 | Male (1) | 4 years old | 1 | Stomatitis and vesiculopapular rash | Vesiculopapular rash on the lips | IV amoxicillin–clavulanic acid, retinol tablets, antibiotic eye drops, and paracetamol. Then, changed to IV (ceftriaxone) and morphine. | No |
| Costello et al., 2022 [23] | Case report | USA | 1 | Male (1) | 28 years old | 1 | Erosions and a pustule | Erosions on oral mucosa and a pustule in the lower mucosal lip | IV acyclovir | No |
| Noe et al., 2022 [10] | Case report | Germany | 2 | Male (2) | 26 years old | 1 | White spots and dysphagia | White spots on tonsils | Topical zinc oxide suspension | Yes |
| 32 years old | No oral/perioral manifestation | No oral/perioral manifestation | Topical zinc oxide suspension | No | ||||||
| Jang et al., 2022 [35] | Case report | Republic of Korea | 1 | Male (1) | 34 years old | 1 | Erosions covered with crust and sore throat | Erosions in the perioral area and sore throat (pharynx) | NM | Yes |
| de Sousa et al., 2022 [46] | Case report | Portugal | 1 | Male (1) | 24 years old | 1 | Umbilicated papule and ulcer | An umbilicated papule on the upper lip and an ulcer on the dorsal surface of the tongue | Symptomatic care with paracetamol and tramadol, and topical antibiotic (fusidic acid) | No |
| Ajmera et al.,2022 [22] | Case report | USA | 1 | Male (1) | 26 years old | 1 | Rash as tender umbilicated pox-like lesions/papules, swelling, sore throat, pain on swallowing, burning sensation, and oral thrush | Rash (umbilicated lesions) on the tongue and perioral rash (umbilicated pox-like lesions), swelling of the tongue, and sore throat (pharynx) | Antibiotic therapy (IV vancomycin, IV piperacillin), IV dexamethasone, IV acyclovir and IV fluconazole, magic mouthwash, Valtrex, IM penicillin, tecovirimat, and supportive care | Yes |
| Yadav et al., 2022 [36] | Case report | India | 2 | Male (2) | 35 years old | 1 | Umbilicated vesicular rashes, edema, and sore throat | Vesicular rashes found in the oral cavity (tip of the tongue) and lips, edema of the upper lip, and sore throat (pharynx) | Oral acyclovir | Yes |
| 31 years old | No oral/perioral manifestation | No oral/perioral manifestation | NM | No | ||||||
| Schlabe et al., 2022 [29] | Case report | Germany | 1 | Male (1) | 51 years old | 1 | Ulcer, vesicles, swelling, and muffled speech | Vesicles turned ulcers on the left mouth corner/commissure, vesicles on the palate, and swelling of the base of the tongue leading to muffled speech | Antiviral medication (tecovirimat) | Yes |
| Ortiz-Martínez et al., 2022 [26] | Case report | USA | 1 | Male (1) | 36 years old | 1 | Sore throat, bilateral enlarged tonsils, and oropharyngeal erythema | Sore throat and erythema (oropharynx), and tonsils | IM penicillin G, doxycycline, ceftriaxone, and amoxicillin–clavulanate | Yes |
| Davido et al., 2022 [41] | Case report | France | 1 | Male (1) | 48 years old | 1 | Limited mouth opening, abscess, and swallowing disorder | Peritonsillar abscess on clinical examination, but CT scan revealed peritonsillar abscess swelling in the piriform sinus | Antimicrobial therapy (IV amoxicillin/clavulanate, IV ceftriaxone, and oral metronidazole) and drainage | Yes |
| Matias et al., 2022 [21] | Case report | USA | 3 | Male (3) | 20s | 2 | Pruritic vesiculopustular lesions | Oropharynx | Antiviral therapy (tecovirimat) | No |
| 20s | Tonsillar enlargement and pain, edema, pustular lesions, and odynophagia | Enlargement of the left palatine tonsil, and pustular lesions on the gingiva | Antiviral therapy (tecovirimat) | Yes | ||||||
| 40s | No oral/perioral manifestation | No oral/perioral manifestation | Antiviral therapy (tecovirimat) | No | ||||||
| Lima et al., 2022 [43] | Case report | Brazil | 1 | Male (1) | 41 years old | 1 | The lesions followed a vesicle–pustule–ulcerated lesion pattern with a well defined border and a central crust surrounded by erythema, along with another ulcer | The lesions that followed the common pattern were seen above the upper lip, while the ulcerated lesion was in the oropharynx | Antiviral therapy (valaciclovir), antibiotics (doxycycline, azithromycin, ceftriaxone, and amoxicillin–clavulanate), and antipyretics (dipyrone) | Yes |
| Lopes et al., 2022 [44] | Case report | Brazil | 2 | Male (2) | 28 years old | 2 | Ulcero-crusted lesion with vesiculopustular borders and necrotic, exudative background, and localized erythema | Rima oris/angle of the mouth | Paracetamol and cleaning of the lesions with antiseptics | Yes |
| 28 years old | Lesion with vesiculopustular borders, central necrotic tissue, and an erythematous base | Rima oris/angle of the mouth | Paracetamol and cleaning of the lesions with antiseptics | Yes | ||||||
| Eisenstadt et al., 2022 [27] | Case report | USA | 1 | Male (1) | 20s | 1 | Sore throat and honey-colored, superficial crusted ulcer | Sore throat (pharynx) and an ulcer on the perioral skin | 2% mupirocin ointment for presumed impetigo and 5% imiquimod cream for presumed condyloma | Yes |
| Oprea et al., 2022 [39] | Case report | Romania | 1 | Male (1) | 26 years old | 1 | Hyperemia of the pharynx with pseudo-membranous appearance, petechiae, thrush, and dysphagia | Hyperemia in the pharynx and petechiae on the palate | Symptomatic treatment, fluids, and topical treatment | No |
| Bížová et al., 2022 [40] | Case report | Czech Republic | 1 | Male (1) | 34 years old | 1 | Ulcer | Ulcer on the left tonsil | Cephalosporins | Yes |
| Peters et al., 2022 [19] | Case report | USA | 2 | Male (2) | 38 years old | 2 | Sensitivity to hot food, ulcer, and vasculo-ulcerative lesions | Sensitivity to hot food in the tongue, ulcer at the tip and midline of the tongue, and vasculo-ulcerative lesions on the anterior ventral tongue surface | Antiviral medication (tecovirimat) | Yes |
| 30 years old | Nodule, ulcer, and sore throat | Nodule on the tip of the tongue, ulcer on the anterior dorsal surface of the tongue, and sore throat (pharynx) | NM | Yes | ||||||
| Wong et al., 2022 [28] | Case report | USA | 1 | Male (1) | 52 years old | 1 | Odynophagia, and tonsillar hypertrophy with exudates. Vesicles and sore throat (pharyngeal pain) | Bilateral tonsillar hypertrophy with exudates, vesicles on the pharynx, and sore throat | Supportive therapy | Yes |
| Benslama et al., 2022 [42] | Case report | France | 1 | Male (1) | 34 years | 1 | Canker sores (ulcers) (target/cockade-shaped) surrounded by white halo, and difficulty swallowing | Ulcers at the tip of the tongue and floor of the mouth | Antimicrobial therapy (amoxicillin), local antiseptics (chlorhexidine), and general and local analgesics (paracetamol, xylocaine). | Yes |
| Lucer et al., 2022 [47] | Case report | Columbia | 2 | Male (2) | 26 years old | 1 | Pruritic lesions in the mouth, ulcer, and pustules | Ulcer in the lower lip, pustules in the right soft palate | Supportive therapy, opiods for rectal pain, and tecovirimat | No |
| 37 years old | No oral/perioral manifestation | No oral/perioral manifestation | Opiods for rectal pain and tecovirimat | No | ||||||
| Pisano et al., 2022 [30] | Case report | Italy | 2 | Male (2) | 45 years old | 2 | Dysphagia, sore throat, ulcerated nodule, erosive lesion with erythema, and enlarged tonsil with exudates deviating the uvula | Sore throat (pharynx), ulcerated nodule on the lateral border of the tongue, erythematic erosive lesion on the palate deviating the uvula, and enlarged tonsils | NM | Yes |
| 69 years old | Ulcer and sore throat | Ulcer on the floor of the mouth and sore throat (pharynx) | NM | Yes | ||||||
| Pisano et al., 2022 [32] | Case report | Italy | 1 | Male (1) | 54 years old | 1 | Nodules covered with scaly crusts with burning sensation | Lesions present in the perioral region | Systemic amoxicillin–clavulanic acid, and 2% fusidic acid ointment | No |
| Martin-Filho et al., 2022 [45] | Cross-sectional study | Brazil | 3 | Male (1), Female (2) | 28 years old (female) | 2 | Sore throat and oral lesions (unspecified type) | Sore throat (pharynx) and lesions in the oropharynx, oral mucosa, and lips | No medical care was needed | Yes |
| 24 years old (male) | Sore throat | Sore throat (pharynx) | No medical care was needed | No | ||||||
| 12 years old (female) | No oral/perioral manifestation | No oral/perioral manifestation | No medical care was needed | No | ||||||
| Ambrogio et al., 2022 [31] | Case report | Italy | 2 | Male (2) | 39 years old | 2 | Exudative erythematous plaque covered with vesicles, ulcer with central erosive area | Exudative erythematous plaque covered with vesicles on the chin, ulcer with central erosive area on the lower lip | Supportive therapy | No |
| NM | Exudative ulcer | Exudative ulcer on the chin | Supportive therapy | No | ||||||
| Crosato et al., 2023 [33] | Case report | Italy | 1 | Male (1) | 46 years old | 1 | Vesicle, followed by erosion, expansion, ulceration, and necrosis with umbilication of the lesion, and there was a papulo-vesicular rash | Ulcerated vesicle on the chin and papulo-vesicular rash in the oral cavity | Biopsy of the chin lesion, isolation of the patient, and no treatment was performed | Yes |
| Amos et al., 2023 [38] | Case report | UK | 1 | Male (1) | 40s | 1 | Sore throat, odynophagia, hoarse voice, erythema, thick white exudates, vesicle, and ulcers | Sore throat (pharynx), bilateral peritonsillar erythema, right tonsillar exudates, vesicle in the left posterior palate, white patches of exudates and ulcers on the right base of the tongue | Nebulized epinephrine, IV dexamethasone, IV broad-spectrum antibiotics, IV fluids, analgesia, heparin, and oral anticoagulant | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issa, A.W.; Alkhofash, N.F.; Gopinath, D.; Varma, S.R. Oral Manifestations in Monkeypox: A Scoping Review on Implications for Oral Health. Dent. J. 2023, 11, 132. https://doi.org/10.3390/dj11050132
Issa AW, Alkhofash NF, Gopinath D, Varma SR. Oral Manifestations in Monkeypox: A Scoping Review on Implications for Oral Health. Dentistry Journal. 2023; 11(5):132. https://doi.org/10.3390/dj11050132
Chicago/Turabian StyleIssa, Asmaa Wajeeh, Nada Fayyad Alkhofash, Divya Gopinath, and Sudhir Rama Varma. 2023. "Oral Manifestations in Monkeypox: A Scoping Review on Implications for Oral Health" Dentistry Journal 11, no. 5: 132. https://doi.org/10.3390/dj11050132