
Pre-Chemotherapy Dental Screening: Is There Additional Diagnostic Value for a Panoramic Radiograph?

Abstract
:1. Introduction
2. Materials and Methods
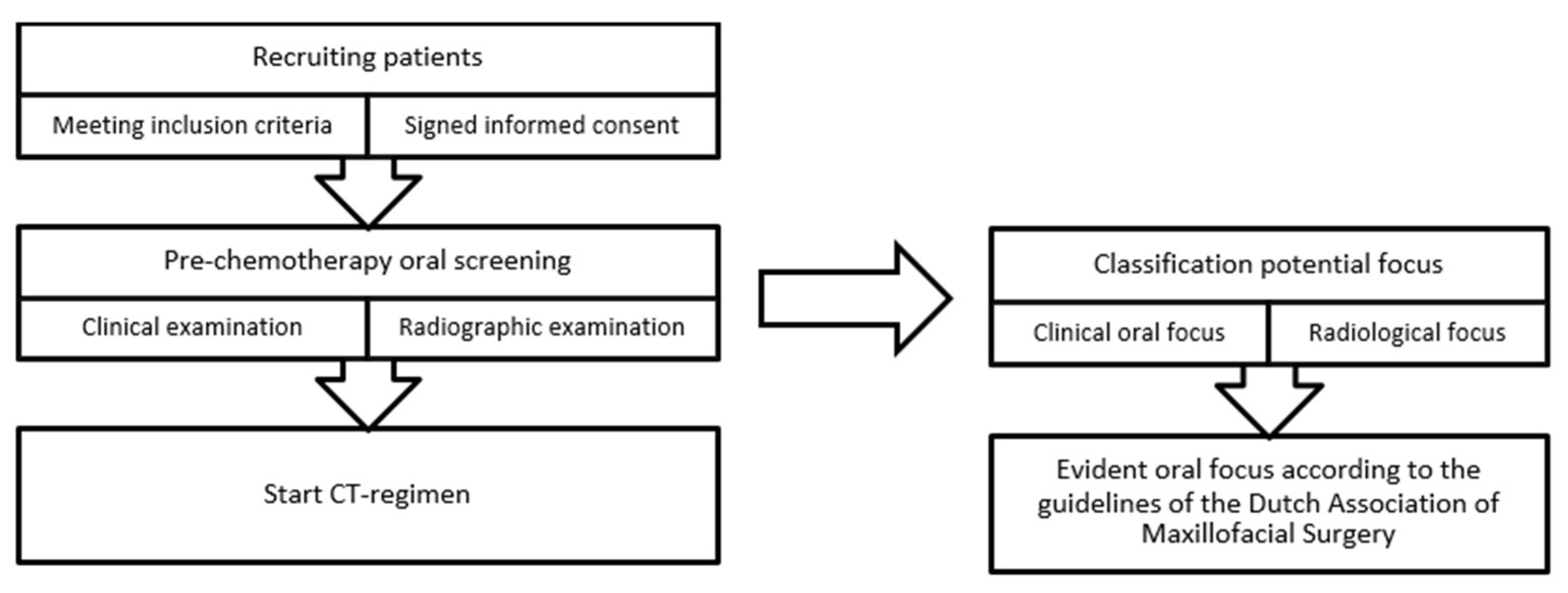
2.1. Pre-Chemotherapy Oral Screening
- Evaluation of dental habits (interval of regular dental visits, oral hygiene habits) and oral complaints over the last three months,
- Intraoral screening for mucosal and dental pathology (e.g., mucosal infections, caries/caries profunda, clinically visible root remnants, partially impacted teeth),
- Periodontal screening using the Dutch Periodontal Screening Index (DPSI), assessed per sextant [17]. The highest score was used for analysis,
- Screening for peri-implant mucositis and peri-implantitis.
- Marginal alveolar bone loss,
- peri-implant alveolar bone loss,
- The presence of periapical lesions of endodontically and non-endodontically treated teeth,
- (Partially) impacted teeth,
- Root remnants,
- Other radiographic abnormalities.
2.2. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Combined Findings of the Clinical Examination and the Panoramic Radiograph
3.3. Findings of Clinical Evaluation Only
3.4. Findings on the Panoramic Radiographs
3.5. Added Diagnostic Value of Panoramic Radiography
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Patient demographics (N = 93) | |||
| No. of patients (N) | Percentage (%) | ||
| Gender | Male | 28 | 30.1 |
| Female | 65 | 69.9 | |
| Age | Mean 54.0 years | ||
| Range 18–78 years | |||
| SD 15.6 | |||
| BMI | Mean 25.3 | ||
| Range 16.8–44.3 | |||
| SD 5.5 | |||
| Smoking | Yes | 14 | 15.1 |
| No | 58 | 62.4 | |
| Quit | 21 | 22.6 | |
| Current alcohol use | Yes | 31 | 33.3 |
| No | 62 | 66.7 | |
| ASA classification | ASA I | 52 | 55.9 |
| ASA II | 36 | 38.7 | |
| ASA III | 5 | 5.4 | |
| WHO performance status | WHO 0 | 56 | 60.2 |
| WHO 1 | 34 | 36.6 | |
| WHO 2 | 3 | 3.2 | |
| Tumor and treatment characteristics (N = 93) | |||
| No. of patients (N) | Percentage (%) | ||
| Tumor subgroup | Gynecological | 44 | 47.3 |
| Upper GI tract | 20 | 21.5 | |
| Sarcoma | 12 | 12.9 | |
| Urinary tract | 6 | 6.5 | |
| Lymphoma | 5 | 5.4 | |
| Breast | 4 | 4.3 | |
| Lower GI tract | 2 | 2.2 | |
| Treatment goal | Curative | 61 | 65.6 |
| Palliative | 32 | 34.4 | |
| (BMI = Body Mass Index, ASA = American Society of Anesthesiologists, WHO = World Health Organization, GI = Gastrointestinal). | |||
Appendix B
| No. of Patients (N) | Percentage (%) | ||
| Oral hygiene habits | Brushing; twice daily | 70 | 75.3 |
| Brushing; daily | 15 | 16.1 | |
| Brushing; >twice daily | 7 | 7.6 | |
| Never | 1 | 1.1 | |
| Dental visits | Twice a year | 59 | 63.4 |
| Every year | 22 | 23.7 | |
| Sporadically | 7 | 7.5 | |
| Never | 5 | 5.4 | |
| Patients with implants | Yes | 7 | 7.5 |
| No | 86 | 92.5 | |
| Number of teeth per patient | Mean 25 | ||
| Range 8–32 | |||
| SD 5.2 | |||
References
- Lyman, G.H.; Abella, E.; Pettengell, R. Risk factors for febrile neutropenia among patients with cancer receiving chemotherapy: A systematic review. Crit. Rev. Oncol./Hematol. 2014, 90, 190–199. [Google Scholar] [CrossRef]
- Lucas, A.J.; Olin, J.L.; Coleman, M.D. Management and Preventive Measures for Febrile Neutropenia. Pharm. Ther. 2018, 43, 228–232. [Google Scholar]
- Kochanek, M.; Schalk, E.; von Bergwelt-Baildon, M.; Beutel, G.; Buchheidt, D.; Hentrich, M.; Henze, L.; Kiehl, M.; Liebregts, T.; von Lilienfeld-Toal, M.; et al. Management of sepsis in neutropenic cancer patients: 2018 guidelines from the Infectious Diseases Working Party (AGIHO) and Intensive Care Working Party (iCHOP) of the German Society of Hematology and Medical Oncology (DGHO). Ann. Hematol. 2019, 98, 1051–1069. [Google Scholar] [CrossRef]
- Zecha, J.; Raber-Durlacher, J.E.; Laheij, A.; Westermann, A.M.; Epstein, J.B.; de Lange, J.; Smeele, L.E. The impact of the oral cavity in febrile neutropenia and infectious complications in patients treated with myelosuppressive chemotherapy. Support Care Cancer 2019, 27, 3667–3679. [Google Scholar] [CrossRef] [PubMed]
- Oral complications of cancer therapies: Diagnosis, prevention, and treatment. Natl. Inst. Health Consens. Dev. Conf. Consens. Statement 1989, 7, 1–11.
- American Dental Association, Council on Scientific Affairs, Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. U.S. Department of health and human services, Public Health Service, Food and Drug Administration, 2012. Available online: https://www.fda.gov/media/84818/download (accessed on 15 January 2023).
- Department of Scientific Information, Evidence Synthesis & Translation Research, ADA Science & Research Institute, LLC. Cancer Therapies and Dental Considerations. Last Updated: 30 August 2022. Available online: https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/cancer-therapies-and-dental-considerations (accessed on 15 January 2023).
- U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Dental and Craniofacial Research, Oral Complications of Cancer Treatment: What the Dental Team Can Do. Oral Health, Cancer Care, and You: Fitting the Pieces Together. Reprinted Sept 2009, Publication No. 09–4372. Available online: https://www.nidcr.nih.gov/sites/default/files/2017-09/oral-complications-cancer-dental-team.pdf (accessed on 15 January 2023).
- Supportive, P.D.Q.; Palliative Care Editorial, B. Oral Complications of Chemotherapy and Head/Neck Radiation (PDQ®): Health Professional Version. In PDQ Cancer Information Summaries; National Cancer Institute (US): Bethesda, MD, USA, 2002. [Google Scholar]
- Epstein, J.B.; Rea, G. The value of panoramic radiographic examination in patients with leukemia before medical management. Oral Surg. Oral Med. Oral Pathol. 1992, 74, 736–741. [Google Scholar] [CrossRef] [PubMed]
- Gortzak, R.A.; Baart, J.A.; Allard, R.H.; van der Waal, I. Dental focus examination: A proposal for a more nuanced approach. Ned. Tijdschr. Tandheelkd. 2013, 120, 440–444. [Google Scholar] [CrossRef]
- Choi, J.W. Assessment of panoramic radiography as a national oral examination tool: Review of the literature. Imaging Sci. Dent. 2011, 41, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yong, C.W.; Robinson, A.; Hong, C. Dental Evaluation Prior to Cancer Therapy. Front. Oral Health 2022, 3, 876941. [Google Scholar] [CrossRef]
- Horner, K.; Eaton, K. (Eds.) Selection Criteria for Dental Radiography, 3rd ed.; Faculty of General Dental Practice: London, UK, 2018; ISBN 978-1-9999761-0-1. Available online: https://cgdent.uk/wp-content/uploads/2021/08/FGDP-SCDR-ALL-Web.pdf (accessed on 15 January 2023).
- Martínez Beneyto, Y.; Alcaráz Banos, M.; Pérez Lajarin, L.; Rushton, V.E. Clinical justification of dental radiology in adult patients: A review of the literature. Med. Oral Patol. Oral Cir. Bucal. 2007, 12, E244–E251. [Google Scholar]
- Zecha, J.A.E.M.; Raber-Durlacher, J.E.; Laheij, A.M.G.A.; Westermann, A.M.; de Lange, J.; Smeele, L.E. The Potential Contribution of Dental Foci and Oral Mucositis to Febrile Neutropenia in Patients Treated with Myelosuppressive Chemotherapy for Solid Tumors and Lymphoma. Front. Oral Health 2022, 3, 940044. [Google Scholar] [CrossRef] [PubMed]
- Van der Velden, U. The Dutch periodontal screening index validation and its application in The Netherlands. J. Clin. Periodontol. 2009, 36, 1018–1024. [Google Scholar] [CrossRef]
- Dutch Association of Oral and Maxillofacial Surgery (NVMKA), Guideline Focusonderzoek. 2021 Version 1.1 11/2021. Available online: https://www.nvmka.nl/system/files/Focusonderzoek%20NVMKA%201.1.pdf (accessed on 15 January 2023).
- Donker, A.E.; van Merkesteyn, J.P.; Bredius, R.G.; van Weel-Sipman, M.H. Value of panoramic radiographs in paediatric pre-bone marrow transplantation oral evaluation. Int. J. Oral Maxillofac. Surg. 2002, 31, 170–172. [Google Scholar] [CrossRef]
- Gortzak, R.A.; van der Waal, I.; Allard, R.H. Diagnosing and treatment of dental foci in Dutch medical centres. Ned. Tijdschr. Tandheelkd. 2007, 114, 287–291. [Google Scholar] [PubMed]
- Guggenheimer, J.; Mayher, D.; Eghtesad, B. A survey of dental care protocols among US organ transplant centers. Clin. Transpl. 2005, 19, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Jansma, J.; Stegenga, B. Examination for focal infections: Sensible or superfluous? Ned. Tijdschr. Tandheelkd. 2006, 113, 328–333. [Google Scholar]
- Jansma, J.; Vissink, A. Dental foci. Role, treatment and prophylaxis in patients at risk. Ned. Tijdschr. Tandheelkd. 1998, 105, 52–56. [Google Scholar] [PubMed]
- Newman, H.N. Focal infection. J. Dent. Res. 1996, 75, 1912–1919. [Google Scholar] [CrossRef]
- Schuurhuis, J.M.; Span, L.F.; Stokman, M.A.; van Winkelhoff, A.J.; Vissink, A.; Spijkervet, F.K. Effect of leaving chronic oral foci untreated on infectious complications during intensive chemotherapy. Br. J. Cancer 2016, 114, 972–978. [Google Scholar] [CrossRef]
- Schuurhuis, J.M.; Stokman, M.A.; Roodenburg, J.L.; Reintsema, H.; Langendijk, J.A.; Vissink, A.; Spijkervet, F.K. Efficacy of routine pre-radiation dental screening and dental follow-up in head and neck oncology patients on intermediate and late radiation effects. A retrospective evaluation. Radiother. Oncol. 2011, 101, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Schuurhuis, J.M.; Stokman, M.A.; Witjes, M.J.; Dijkstra, P.U.; Vissink, A.; Spijkervet, F.K. Evidence supporting pre-radiation elimination of oral foci of infection in head and neck cancer patients to prevent oral sequelae. A systematic review. Oral Oncol. 2015, 51, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Schuurhuis, J.M.; Stokman, M.A.; Witjes, M.J.; Langendijk, J.A.; van Winkelhoff, A.J.; Vissink, A.; Spijkervet, F.K. Head and neck intensity modulated radiation therapy leads to an increase of opportunistic oral pathogens. Oral Oncol. 2016, 58, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Schuurhuis, J.M.; Stokman, M.A.; Witjes, M.J.H.; Reintsema, H.; Langendijk, J.A.; Vissink, A.; Spijkervet, F.K.L. Patients with advanced periodontal disease before intensity-modulated radiation therapy are prone to develop bone healing problems: A 2-year prospective follow-up study. Support. Care Cancer 2018, 26, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Spijkervet, F.K.L.; Schuurhuis, J.M.; Stokman, M.A.; Witjes, M.J.H.; Vissink, A. Should oral foci of infection be removed before the onset of radiotherapy or chemotherapy? Oral Dis. 2021, 27, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Stegenga, B.; Vissink, A.; de Bont, L.G.M. MKA-chirurgie. Handboek voor Mondziekten, Kaak- en Aangezichtschirurgie. 2013. Available online: https://www.uitgeverijvangorcum.nl/media/1/9789023249269_inkijk.pdf (accessed on 9 April 2023).
- Machado, V.; Proença, L.; Morgado, M.; Mendes, J.J.; Botelho, J. Accuracy of Panoramic Radiograph for Diagnosing Periodontitis Comparing to Clinical Examination. J. Clin. Med. 2020, 9, 2313. [Google Scholar] [CrossRef]
- Nardi, C.; Calistri, L.; Grazzini, G.; Desideri, I.; Lorini, C.; Occhipinti, M.; Mungai, F.; Colagrande, S. Is Panoramic Radiography an Accurate Imaging Technique for the Detection of Endodontically Treated Asymptomatic Apical Periodontitis? J. Endod. 2018, 44, 1500–1508. [Google Scholar] [CrossRef]
- Corbet, E.F.; Ho, D.K.; Lai, S.M. Radiographs in periodontal disease diagnosis and management. Aust. Dent. J. 2009, 54 (Suppl. 1), S27–S43. [Google Scholar] [CrossRef]
- Lockhart, P.B.; Brennan, M.T.; Thornhill, M.; Michalowicz, B.S.; Noll, J.; Bahrani-Mougeot, F.K.; Sasser, H.C. Poor oral hygiene as a risk factor for infective endocarditis-related bacteremia. J. Am. Dent. Assoc. 2009, 140, 1238–1244. [Google Scholar] [CrossRef]
- Nishi, H.; Ohta, K.; Kuramoto, Y.; Shigeishi, H.; Obayashi, T.; Yoshioka, Y.; Konishi, M.; Munenaga, S.; Nagoshi, H.; Yoshida, T.; et al. Periodontal inflamed surface area in oral cavity associated with febrile neutropenia in patients with hematologic malignancy undergoing chemotherapy. Sci. Rep. 2022, 12, 2483. [Google Scholar] [CrossRef]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Tibúrcio-Machado, C.S.; Michelon, C.; Zanatta, F.B.; Gomes, M.S.; Marin, J.A.; Bier, C.A. The global prevalence of apical periodontitis: A systematic review and meta-analysis. Int. Endod. J. 2021, 54, 712–735. [Google Scholar] [CrossRef] [PubMed]
- den Boer, J.C.L.; van der Sanden, W.J.M.; Bruers, J.J.M. Developments in oral health care in the Netherlands between 1995 and 2018. BMC Oral Health 2020, 20, 192. [Google Scholar] [CrossRef] [PubMed]
- Melkos, A.B.; Massenkeil, G.; Arnold, R.; Reichart, P.A. Dental treatment prior to stem cell transplantation and its influence on the posttransplantation outcome. Clin. Oral Investig. 2003, 7, 113–115. [Google Scholar] [CrossRef]
- Santos, P.S.; Coracin, F.L.; Barros, J.C.; Dulley, F.L.; Nunes, F.D.; Magalhaes, M.G. Impact of oral care prior to HSCT on the severity and clinical outcomes of oral mucositis. Clin. Transplant. 2011, 25, 325–328. [Google Scholar] [CrossRef]
- Tsuji, K.; Shibuya, Y.; Akashi, M.; Furudoi, S.; Yakushijin, K.; Kawamoto, S.; Okamura, A.; Matsuoka, H.; Komori, T. Prospective study of dental intervention for hematopoietic malignancy. J. Dent. Res. 2015, 94, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Graber, C.J.; de Almeida, K.N.; Atkinson, J.C.; Javaheri, D.; Fukuda, C.D.; Gill, V.J.; Barrett, A.J.; Bennett, J.E. Dental health and viridans streptococcal bacteremia in allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transpl. 2001, 27, 537–542. [Google Scholar] [CrossRef]
- de Oliveira, M.C.Q.; Lebre Martins, B.N.F.; Santos-Silva, A.R.; Rivera, C.; Vargas, P.A.; Lopes, M.A.; Vechiato-Filho, A.J.; Brandão, T.B.; Prado-Ribeiro, A.C. Dental treatment needs in hospitalized cancer patients: A retrospective cohort study. Support. Care Cancer 2020, 28, 3451–3457. [Google Scholar] [CrossRef]
- Elad, S.; Thierer, T.; Bitan, M.; Shapira, M.Y.; Meyerowitz, C. A decision analysis: The dental management of patients prior to hematology cytotoxic therapy or hematopoietic stem cell transplantation. Oral Oncol. 2008, 44, 37–42. [Google Scholar] [CrossRef]
- Bishay, N.; Petrikowski, C.G.; Maxymiw, W.G.; Lee, L.; Wood, R.E. Optimum dental radiography in bone marrow transplant patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1999, 87, 375–379. [Google Scholar] [CrossRef]
- Toljanic, J.A.; Bedard, J.F.; Larson, R.A.; Fox, J.P. A prospective pilot study to evaluate a new dental assessment and treatment paradigm for patients scheduled to undergo intensive chemotherapy for cancer. Cancer 1999, 85, 1843–1848. [Google Scholar] [CrossRef]
- Mauramo, M.; Grolimund, P.; Egli, A.; Passweg, J.; Halter, J.; Waltimo, T. Dissociations of oral foci of infections with infectious complications and survival after haematopoietic stem cell transplantation. PLoS ONE 2019, 14, e0225099. [Google Scholar] [CrossRef] [PubMed]
- Ortigara, G.B.; Bonzanini, L.I.L.; Schulz, R.E.; Ferrazzo, K.L. Late radiation effects in survivors of head and neck cancer: State of the science. Crit. Rev. Oncol. Hematol. 2021, 162, 103335. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.E.; Doerr, W.; Hovan, A.; Pinto, A.; Saunders, D.; Elting, L.S.; Spijkervet, F.K.; Brennan, M.T. Osteoradionecrosis in cancer patients: The evidence base for treatment-dependent frequency, current management strategies, and future studies. Support. Care Cancer 2010, 18, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| advanced periodontitis (periodontal probing depth of ≥6 mm; DPSI 4) |
| profound dental caries |
| periapical pathology due to an infection of the root canal |
| (partially) impacted teeth |
| remaining roots with surrounding pathology |
| Findings of Combined Clinical and Radiological Evaluation (N = 93) | |||||
|---|---|---|---|---|---|
| No. of patients (N) | Percentage (%) | ||||
| Oral focus present | Yes | 46 | 49.5 | ||
| No | 47 | 50.5 | |||
| Multiple oral foci | Yes | 16 | 17.2 | ||
| No | 77 | 82.8 | |||
| Clinical focus (N = 93) | Radiological focus (N = 93) | ||||
| No. of patients (N) * | Percentage (%) | No. of patients (N) * | Percentage (%) | ||
| Yes | 33 | 35.5 | Yes | 46 | 49.5 |
| Advanced periodontitis (pockets ≥ 6 mm) | 25 | 26.9 | Periodontal bone loss ** | 25 | 26.9 |
| Furcation involvement | 14 | 15.1 | Periapical lesion | 29 | 31.2 |
| Partially impacted third molar | 7 | 7.5 | Partially impacted third molar | 8 | 8.6 |
| Retained roots | 6 | 6.5 | Retained roots | 8 | 8.6 |
| Profound caries | 6 | 6.5 | Profound caries | 7 | 7.5 |
| Peri-implantitis | 1 | 1.1 | Peri-implant bone loss | 1 | 1.1 |
| No | 60 | 64.5 | No | 47 | 50.5 |
| Dutch Periodontal Screening index [17] | No. of patients (N) | Percentage (%) | |||
| Score 0 | 1 | 1.1 | |||
| Score 1 | 1 | 1.1 | |||
| Score 2 | 19 | 20.4 | |||
| Score 3− | 39 | 41.9 | |||
| Score 3+ | 8 | 8.6 | |||
| Score 4 | 25 | 26.9 | |||
| Total | 93 | 100 | |||
| Periapical Pathology (N = 93) | ||
|---|---|---|
| Number of teeth | 2361 | |
| Number of teeth with periapical lesions | 63 | |
| 2.67% | ||
| Number of endodontically treated teeth | 135 | |
| Number of endodontically treated teeth with periapical lesions | 41 | |
| 30.4% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zecha, J.A.E.M.; Laheij, A.M.G.A.; Raber-Durlacher, J.E.; Westermann, A.M.; de Lange, J.; Smeele, L.E. Pre-Chemotherapy Dental Screening: Is There Additional Diagnostic Value for a Panoramic Radiograph? Dent. J. 2023, 11, 122. https://doi.org/10.3390/dj11050122
Zecha JAEM, Laheij AMGA, Raber-Durlacher JE, Westermann AM, de Lange J, Smeele LE. Pre-Chemotherapy Dental Screening: Is There Additional Diagnostic Value for a Panoramic Radiograph? Dentistry Journal. 2023; 11(5):122. https://doi.org/10.3390/dj11050122
Chicago/Turabian StyleZecha, Judith A. E. M., Alexa M. G. A. Laheij, Judith E. Raber-Durlacher, Anneke M. Westermann, Jan de Lange, and Ludwig E. Smeele. 2023. "Pre-Chemotherapy Dental Screening: Is There Additional Diagnostic Value for a Panoramic Radiograph?" Dentistry Journal 11, no. 5: 122. https://doi.org/10.3390/dj11050122