
Accuracy of Zygomatic Implant Placement Using a Full Digital Planning and Custom-Made Bone-Supported Guide: A Retrospective Observational Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Sample
2.3. Data Collection Method
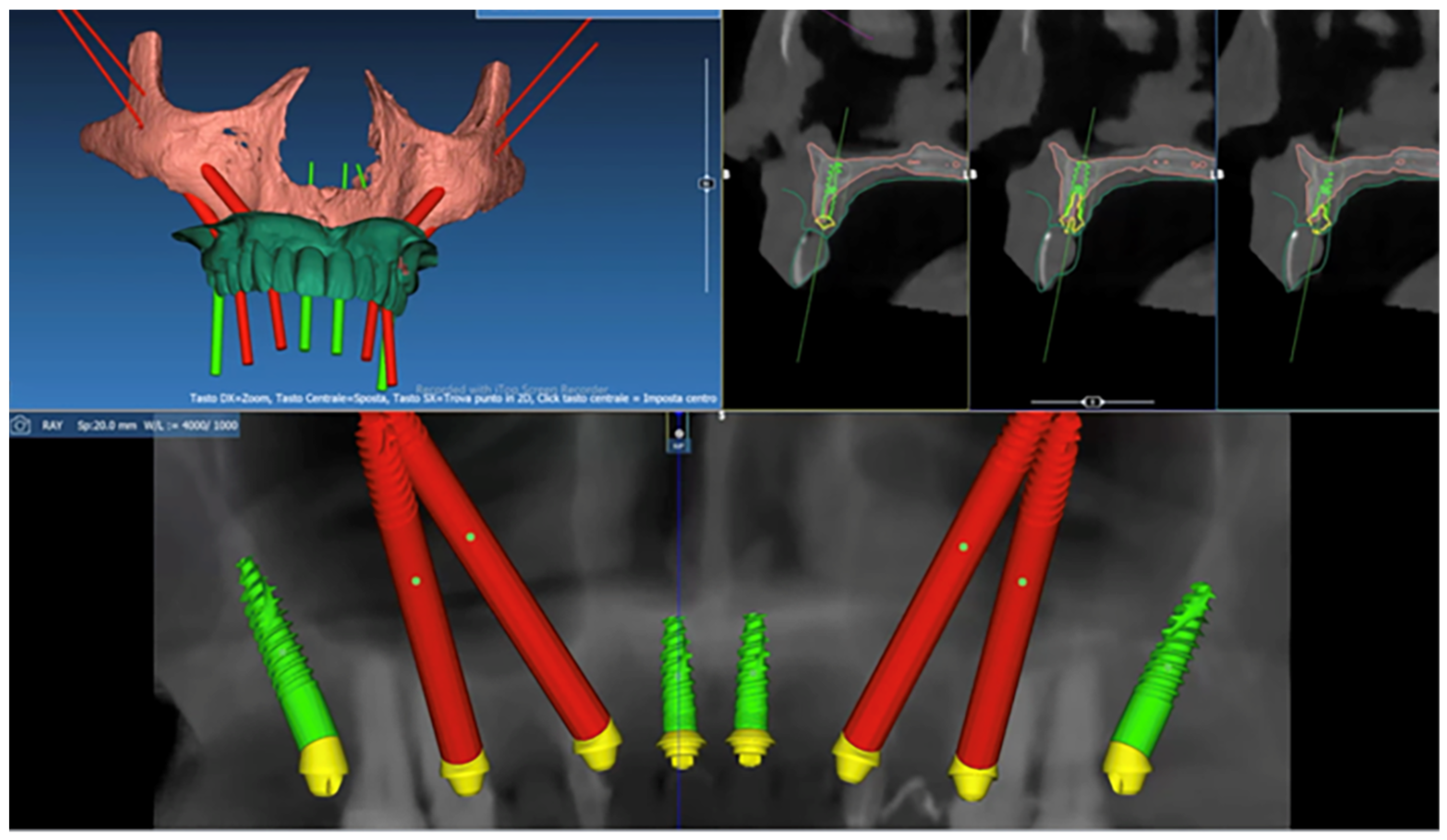
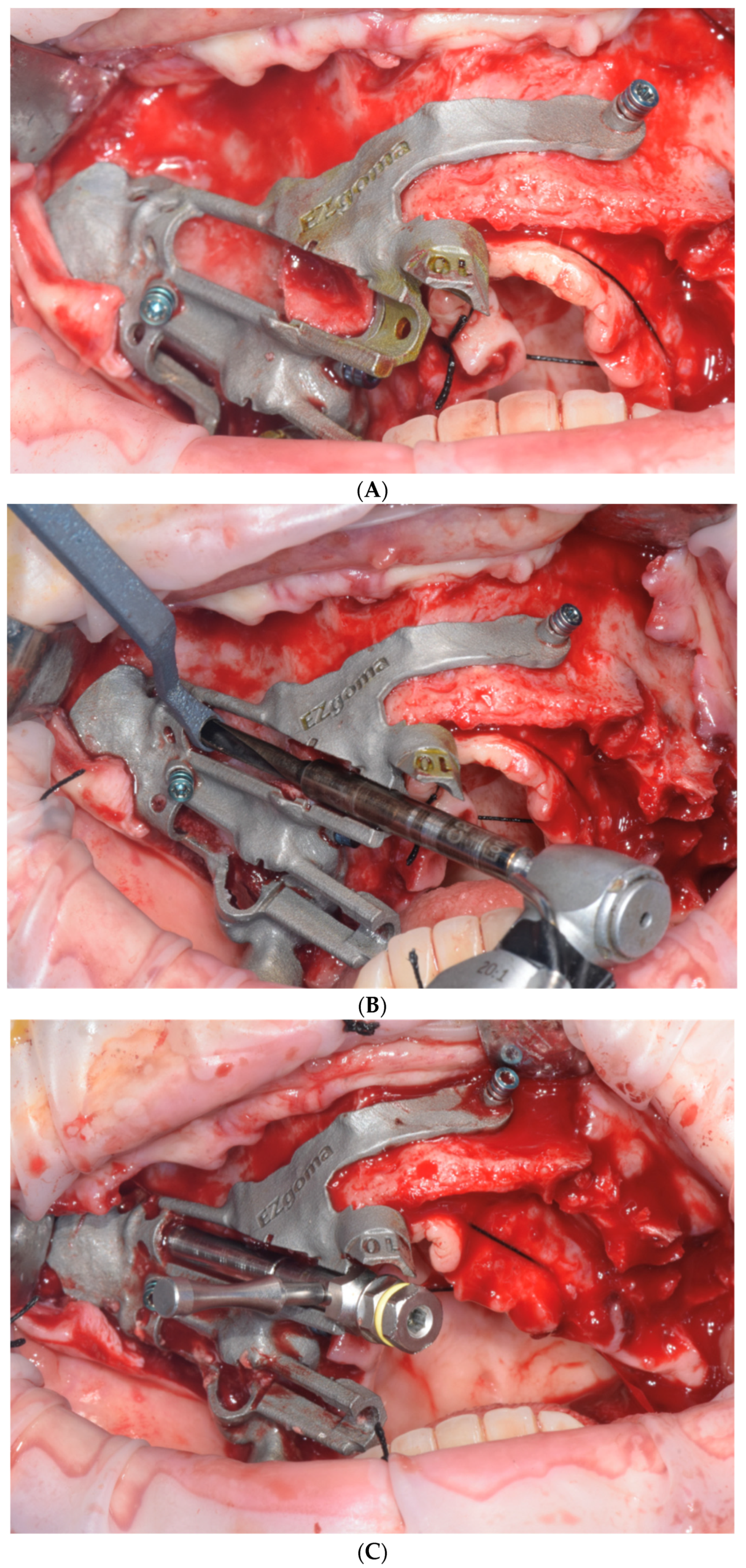
2.4. Surgical Procedure
2.5. Comparative 3D Analysis
2.6. Qualitative Analysis
2.7. Quantitative Analysis
2.8. Study Variables and Outcomes
- -
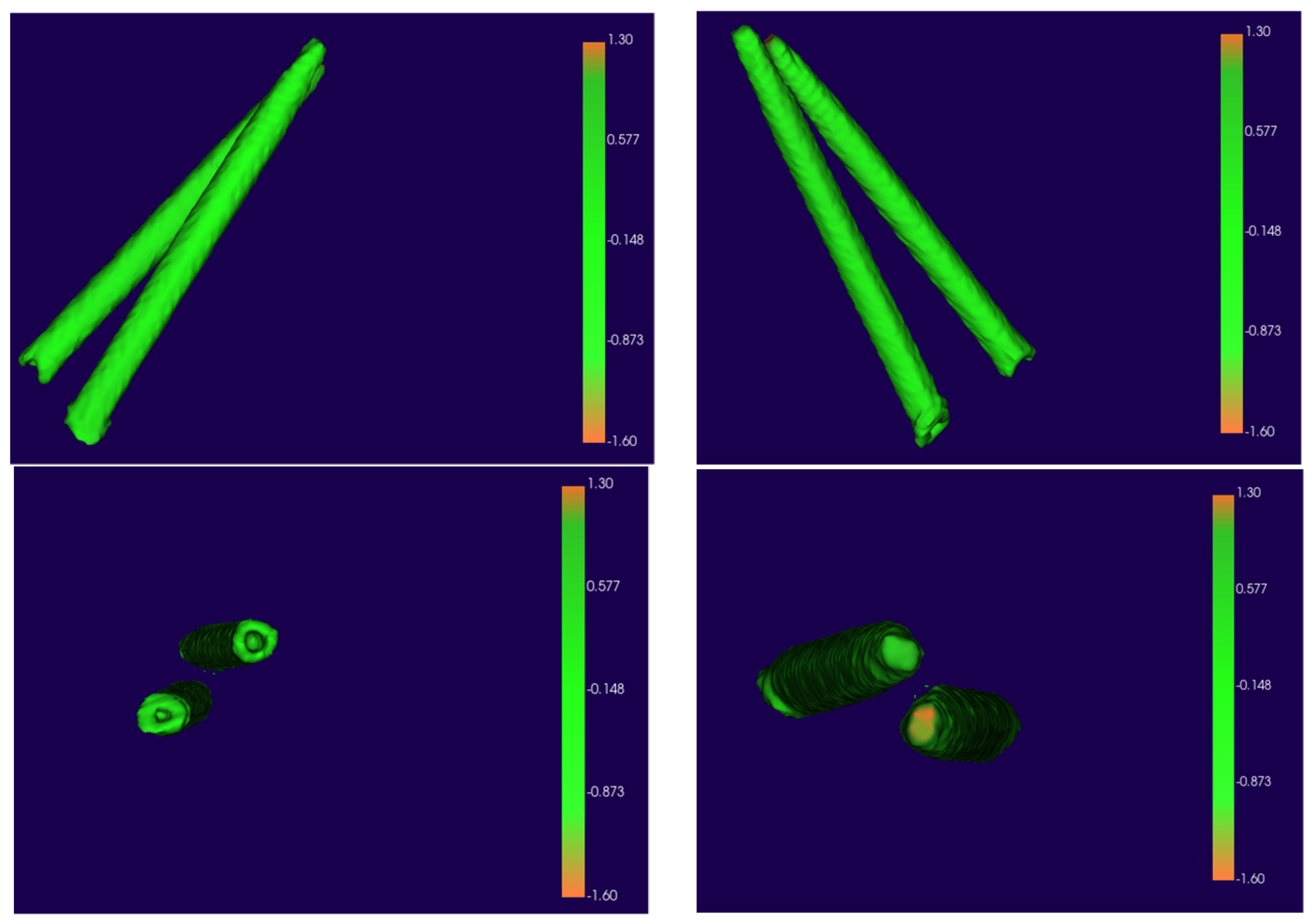
- An operator-independent calculation recorded the mean displacement between the planned and T2 ZIs comparing the 3D surface meshes.
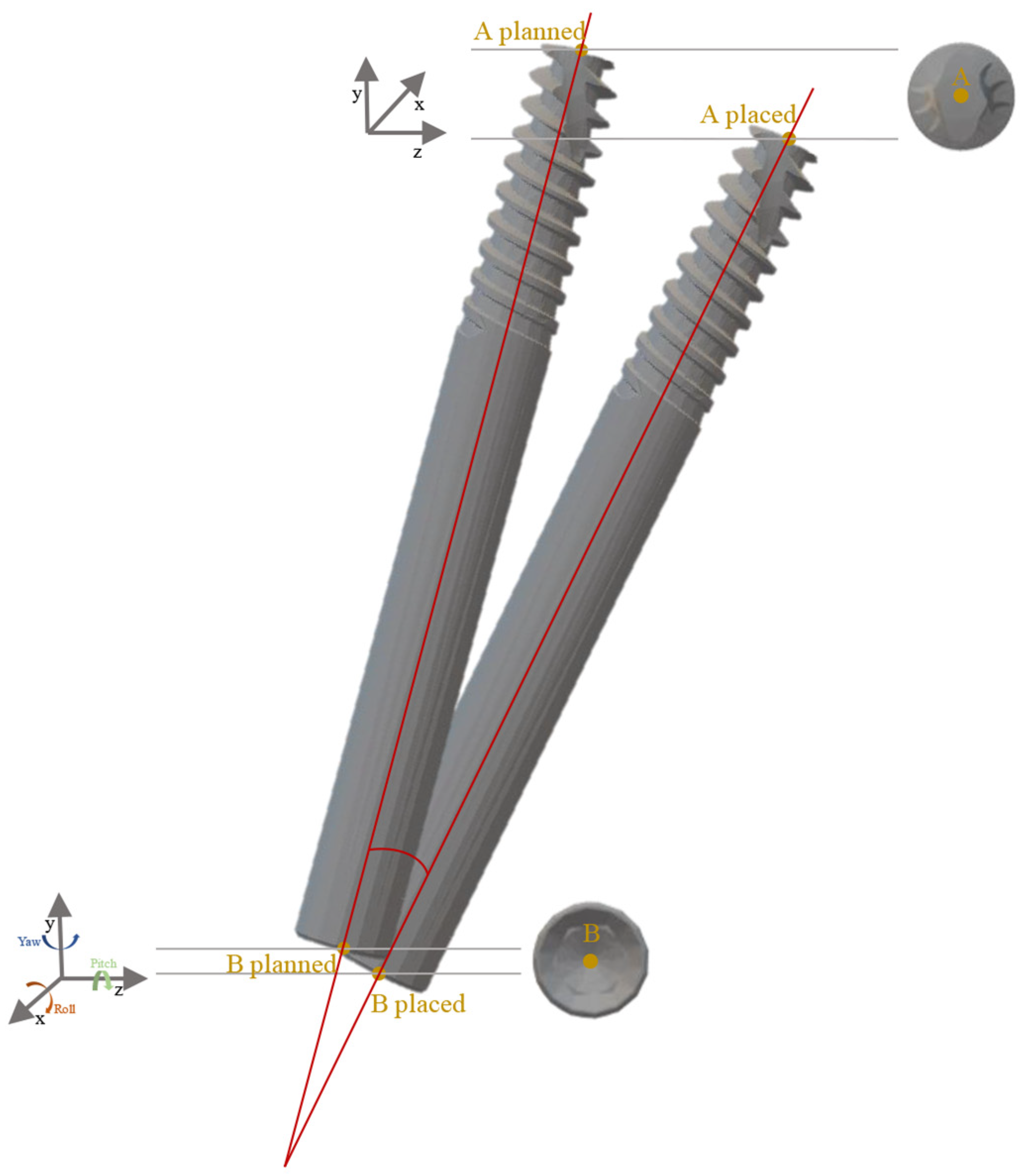
- -
- Linear differences at the implant’s apex and base were recorded in anteroposterior (X-axis), upper–lower (Y-axis), and medio-lateral (Z-axis) directions in mm.
- -
- The angular deviation between the planned and T2 ZIs was determined, calculating yaw, pitch, and roll of the long axis of each implant (°).
2.9. Statistical Analysis
3. Results
3.1. Qualitative Analysis
3.2. Quantitative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Block, M.S.; Emery, R.W. Static or Dynamic Navigation for Implant Placement—Choosing the Method of Guidance. J. Oral Maxillofac. Surg. 2016, 74, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Geng, W.; Liu, C.; Su, Y.; Li, J.; Zhou, Y. Accuracy of different types of computer-aided design/ computer-aided manufacturing surgical guides for dental implant placement. Int. J. Clin. Exp. Med. 2015, 8, 8442–8449. [Google Scholar] [PubMed]
- Varga, E., Jr.; Antal, M.; Major, L.; Kiscsatári, R.; Braunitzer, G.; Piffkó, J. Guidance means accuracy: A randomized clinical trial on freehand versus guided dental implantation. Clin. Oral Implant. Res. 2020, 31, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Besimo, C.E.; Lambrecht, J.T.; Guindy, J.S. Accuracy of implant treatment planning utilizing template-guided reformatted computed tomography. Dentomaxillofacial Radiol. 2000, 29, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.; Mangano, C.; Mijiritsky, E.; Krebs, M.; Hauschild, U.; Fortin, T. Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials. BMC Oral Health 2017, 17, 150. [Google Scholar] [CrossRef]
- Van Steenberghe, D. Accuracy of drilling guides for transfer from three-dimensional CT-based planning to placement of zygoma implants in human cadavers. Clin. Oral Implant. Res. 2023, 14, 131–136. [Google Scholar] [CrossRef]
- Chow, J. A novel device for template-guided surgery of the zygomatic implants. Int. J. Oral Maxillofac. Surg. 2016, 45, 1253–1255. [Google Scholar] [CrossRef]
- Birkfellner, W.; Solar, P.; Gahleitner, A.; Huber, K.; Kainberger, F.; Kettenbach, J.; Homolka, P.; Diemling, M.; Watzek, G.; Bergmann, H. In-vitro assessment of a registration protocol for image guided implant dentistry. Clin. Oral Implant. Res. 2001, 12, 69–78. [Google Scholar] [CrossRef]
- Ozan, O.; Turkyilmaz, I.; Ersoy, A.E.; McGlumphy, E.A.; Rosenstiel, S.F. Clinical Accuracy of 3 Different Types of Computed Tomography-Derived Stereolithographic Surgical Guides in Implant Placement. J. Oral Maxillofac. Surg. 2009, 67, 394–401. [Google Scholar] [CrossRef]
- Schiroli, G.; Angiero, F.; Silvestrini-Biavati, A.; Benedicenti, S. Zygomatic implant placement with flapless computer-guided surgery: A proposed clinical protocol. J. Oral Maxillofac. Surg. 2011, 69, 2979–2989. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer Technology Applications in Surgical Implant Dentistry: A Systematic Review. Int. J. Oral Maxillofac. Implants 2014, 29, 25–42. [Google Scholar]
- Hung, K.F.; Ai, Q.Y.; Fan, S.C.; Wang, F.; Huang, W.; Wu, Y.Q. Measurement of the zygomatic region for the optimal placement of quad zygomatic implants. Clin. Implant Dent. Relat. Res. 2017, 19, 841–848. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Oliveira, D.R.; Custódio, A.L. Accuracy evaluation of computed tomography-derived stereolithographic surgical guides in zygomatic implant placement in human cadavers. J. Oral Implantol. 2010, 36, 345–355. [Google Scholar] [CrossRef]
- Cassetta, M.; Di Mambro, A.; Giansanti, M.; Stefanelli, L.V.; Cavallini, C. The intrinsic error of a stereolithographic surgical template in implant guided surgery. Int. J. Oral Maxillofac. Surg. 2013, 42, 264–275. [Google Scholar] [CrossRef]
- Flügge, T.V.; Nelson, K.; Schmelzeisen, R.; Metzger, M.C. Three-dimensional plotting and printing of an implant drilling guide: Simplifying guided implant surgery. J. Oral Maxillofac. Surg. 2013, 71, 1340–1346. [Google Scholar] [CrossRef]
- Pellegrino, G.; Bellini, P.; Cavallini, P.F.; Ferri, A.; Zacchino, A.; Taraschi, V.; Marchetti, C.; Consolo, U. Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience on Implant Placement Accuracy and Operating Time. An in Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 2153. [Google Scholar] [CrossRef]
- Salmi, M.; Paloheimo, K.S.; Tuomi, J.; Wolff, J.; Mäkitie, A. Accuracy of medical models made by additive manufacturing (rapid manufacturing). J. Cranio-Maxillofac. Surg. 2013, 41, 603–609. [Google Scholar] [CrossRef]
- Lal, K.; White, G.S.; Morea, D.N.; Wright, R.F. Use of stereolithographic templates for surgical and prosthodontic implant planning and placement. Part I. The concept. J. Prosthodont. 2006, 15, 51–58. [Google Scholar] [CrossRef]
- Grecchi, E.; Stefanelli, L.V.; Grecchi, F.; Grivetto, F.; Franchina, A.; Pranno, N. A novel guided zygomatic implant surgery system compared to free hand: A human cadaver study on accuracy. J. Dent. 2022, 119, 103942. [Google Scholar] [CrossRef]
- Mediavilla Guzmán, A.; Riad Deglow, E.; Zubizarreta-Macho, Á.; Agustín-Panadero, R.; Hernández Montero, S. Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study. J. Clin. Med. 2019, 8, 2123. [Google Scholar] [CrossRef]
- D’haese, J.; Van De Velde, T.; Komiyama, A.; Hultin, M.; De Bruyn, H. Accuracy and Complications Using Computer-Designed Stereolithographic Surgical Guides for Oral Rehabilitation by Means of Dental Implants: A Review of the Literature. Clin. Implant Dent. Relat. Res. 2012, 14, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ye, M.; Lin, Y.; Wu, Y.; Wang, C. Image guided oral implantology and its application in the placement of zygoma implants. Comput. Methods Programs Biomed. 2009, 93, 162–173. [Google Scholar]
- Xing Gao, B.; Iglesias-Velázquez, O.; GF Tresguerres, F.; Rodríguez González Cortes, A.; FTresguerres, I.; Ortega Aranegui, R.; López-Pintor, R.M.; López-Quiles, J.; Torres, J. Accuracy of digital planning in zygomatic implants. Int. J. Implant Dent. 2021, 7, 65. [Google Scholar] [CrossRef] [PubMed]
- Naitoh, M.; Ariji, E.; Okumura, S.; Ohsaki, C.; Kurita, K.; Ishigami, T. Can implants be correctly angulated based on surgical templates used for osseointegrated dental implants? Clin. Oral Implant. Res. 2000, 11, 409–414. [Google Scholar] [CrossRef]
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implant. Res. 2012, 23, 112–123. [Google Scholar] [CrossRef]
- Grecchi, F.; Stefanelli, L.V.; Grivetto, F.; Grecchi, E.; Siev, R.; Mazor, Z.; Del Fabbro, M.; Pranno, N.; Franchina, A.; Di Lucia, V.; et al. A novel guided zygomatic and pterygoid implant surgery system: A human cadaver study on accuracy. Int. J. Environ. Res. Public Health 2021, 18, 6142. [Google Scholar] [CrossRef]
- Laederach, V.; Mukaddam, K.; Payer, M.; Filippi, A.; Kühl, S. Deviations of different systems for guided implant surgery. Clin. Oral Implant. Res. 2017, 28, 1147–1151. [Google Scholar] [CrossRef]
- Tatakis, D.N.; Chien, H.H.; Parashis, A.O. Guided implant surgery risks and their prevention. Periodontology 2000 2019, 811, 194–208. [Google Scholar] [CrossRef]
- Widmann, G.; Stoffner, R.; Bale, R. Errors and error management in image-guided craniomaxillofacial surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 701–715. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Variables | Study Sample |
|---|---|
| Patients | 19 |
| Implants | 59 |
| Sex | |
| Female (%) | 11 (57.9) |
| Age (years) | 61 ± 3 |
| Number of placed implants for each patient (%) | |
| 2 | 6 (31.5) |
| 3 | 1 (5.3) |
| 4 | 12 (63.2) |
| Min | Q1 | Q2 | Q3 | Max | Mean | SD | |
|---|---|---|---|---|---|---|---|
| Surface displacement | |||||||
| Right | 0.042 | 0.2 | 0.26 | 0.31 | 0.48 | 0.26 | 0.12 |
| Left | 0.014 | 0.15 | 0.23 | 0.3 | 0.49 | 0.22 | 0.15 |
| X-axis | |||||||
| A_R_AI | 0.03 | 0.25 | 0.41 | 0.58 | 1.96 | 0.52 | 0.51 |
| A_R_PI | 0.013 | 0.21 | 0.37 | 0.58 | 2.5 | 0.58 | 0.7 |
| B_R_AI | 0.01 | 0.06 | 0.3 | 0.57 | 0.81 | 0.34 | 0.26 |
| B_R_PI | 0.04 | 0.09 | 0.22 | 0.52 | 0.63 | 0.31 | 0.23 |
| A_L_AI | 0.06 | 0.18 | 0.63 | 0.84 | 1.57 | 0.63 | 0.48 |
| A_L_PI | 0.14 | 0.24 | 0.39 | 0.59 | 1.04 | 0.45 | 0.27 |
| B_L_AI | 0.008 | 0.15 | 0.21 | 0.45 | 0.9 | 0.32 | 0.25 |
| B_L_PI | 0.07 | 0.17 | 0.29 | 0.47 | 2.1 | 0.47 | 0.56 |
| Y-axis | |||||||
| A_R_AI | 0.21 | 0.54 | 1.04 | 1.68 | 2.2 | 1.12 | 0.63 |
| A_R_PI | 0.63 | 1.26 | 1.9 | 2.04 | 3.35 | 1.78 | 0.8 |
| B_R_AI | 0.006 | 0.2 | 0.46 | 0.75 | 1.7 | 0.54 | 0.46 |
| B_R_PI | 0.06 | 0.16 | 0.43 | 0.68 | 1.2 | 0.47 | 0.38 |
| A_L_AI | 0.27 | 0.58 | 0.97 | 1.45 | 2.34 | 1.04 | 0.57 |
| A_L_PI | 0.07 | 0.73 | 0.84 | 1.64 | 3 | 1.2 | 0.95 |
| B_L_AI | 0.036 | 0.44 | 0.77 | 0.94 | 1.69 | 0.78 | 0.48 |
| B_L_PI | 0.08 | 0.12 | 0.29 | 0.5 | 1.05 | 0.38 | 0.34 |
| Z-axis | |||||||
| A_R_AI | 0.02 | 0.65 | 1.05 | 1.63 | 2.6 | 1.14 | 0.76 |
| A_R_PI | 0.32 | 0.9 | 1.55 | 1.98 | 4.1 | 1.63 | 1.12 |
| B_R_AI | 0.02 | 0.26 | 0.5 | 0.57 | 1.09 | 0.48 | 0.32 |
| B_R_PI | 0.23 | 0.38 | 0.62 | 0.9 | 1.5 | 0.72 | 0.43 |
| A_L_AI | 0.1 | 0.7 | 0.99 | 1.6 | 2.7 | 1.17 | 0.65 |
| A_L_PI | 0.14 | 0.7 | 0.93 | 1.36 | 2.36 | 1.07 | 0.6 |
| B_L_AI | 0.02 | 0.36 | 0.7 | 0.89 | 1.89 | 0.68 | 0.45 |
| B_L_PI | 0.08 | 0.23 | 0.66 | 0.8 | 1.22 | 0.62 | 0.38 |
| 3D distance | |||||||
| A_R_AI | 0.46 | 1.14 | 1.65 | 2.3 | 3.66 | 1.78 | 0.92 |
| A_R_PI | 0.96 | 2.16 | 2.44 | 3.28 | 4.62 | 2.67 | 1.16 |
| B_R_AI | 0.23 | 0.6 | 0.79 | 1.13 | 2.03 | 0.89 | 0.47 |
| B_R_PI | 0.3 | 0.62 | 0.8 | 1.25 | 1.98 | 0.97 | 0.5 |
| A_L_AI | 0.56 | 1.2 | 1.56 | 2.2 | 3.83 | 1.75 | 0.87 |
| A_L_PI | 1 | 1.2 | 1.48 | 2.4 | 3.6 | 1.84 | 0.85 |
| B_L_AI | 0.31 | 0.88 | 1.03 | 1.3 | 2.65 | 1.15 | 0.59 |
| B_L_PI | 0.1 | 0.57 | 0.8 | 1.14 | 2.4 | 0.95 | 0.63 |
| Min | Q1 | Q2 | Q3 | Max | Mean | SD | |
|---|---|---|---|---|---|---|---|
| Yaw | |||||||
| R_AI | 0.12 | 0.27 | 0.33 | 0.74 | 1.76 | 0.56 | 0.45 |
| R_PI | 0.62 | 1.1 | 1.28 | 1.8 | 2.58 | 1.45 | 0.6 |
| L_AI | 0.12 | 0.23 | 0.4 | 0.8 | 1.9 | 0.56 | 0.49 |
| L_PI | 0.2 | 0.42 | 0.96 | 1.95 | 2.83 | 1.22 | 0.98 |
| Pitch | |||||||
| R_AI | 0.03 | 0.19 | 0.21 | 0.46 | 1.99 | 0.43 | 0.5 |
| R_PI | 0.12 | 0.64 | 1.04 | 1.73 | 2.24 | 1.18 | 0.7 |
| L_AI | 0.12 | 0.36 | 0.5 | 0.83 | 1.45 | 0.61 | 0.4 |
| L_PI | 0.27 | 0.89 | 1.4 | 2.35 | 2.65 | 1.49 | 0.84 |
| Roll | |||||||
| R_AI | 0.02 | 0.16 | 0.35 | 0.78 | 1.46 | 0.53 | 0.49 |
| R_PI | 0.08 | 0.5 | 0.83 | 2.67 | 3.28 | 1.41 | 1.23 |
| L_AI | 0.16 | 0.37 | 0.44 | 0.64 | 1.6 | 0.6 | 0.4 |
| L_PI | 0.06 | 0.68 | 1.02 | 1.3 | 4.18 | 1.16 | 1.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallo, F.; Zingari, F.; Bolzoni, A.; Barone, S.; Giudice, A. Accuracy of Zygomatic Implant Placement Using a Full Digital Planning and Custom-Made Bone-Supported Guide: A Retrospective Observational Cohort Study. Dent. J. 2023, 11, 123. https://doi.org/10.3390/dj11050123
Gallo F, Zingari F, Bolzoni A, Barone S, Giudice A. Accuracy of Zygomatic Implant Placement Using a Full Digital Planning and Custom-Made Bone-Supported Guide: A Retrospective Observational Cohort Study. Dentistry Journal. 2023; 11(5):123. https://doi.org/10.3390/dj11050123
Chicago/Turabian StyleGallo, Francesco, Francesco Zingari, Alessandro Bolzoni, Selene Barone, and Amerigo Giudice. 2023. "Accuracy of Zygomatic Implant Placement Using a Full Digital Planning and Custom-Made Bone-Supported Guide: A Retrospective Observational Cohort Study" Dentistry Journal 11, no. 5: 123. https://doi.org/10.3390/dj11050123