
Evaluation of Dentinal Thickness and Remaining Dentine Volume around Root Canals Using Cone-Beam Computed Tomography Scanning
Abstract
:1. Introduction
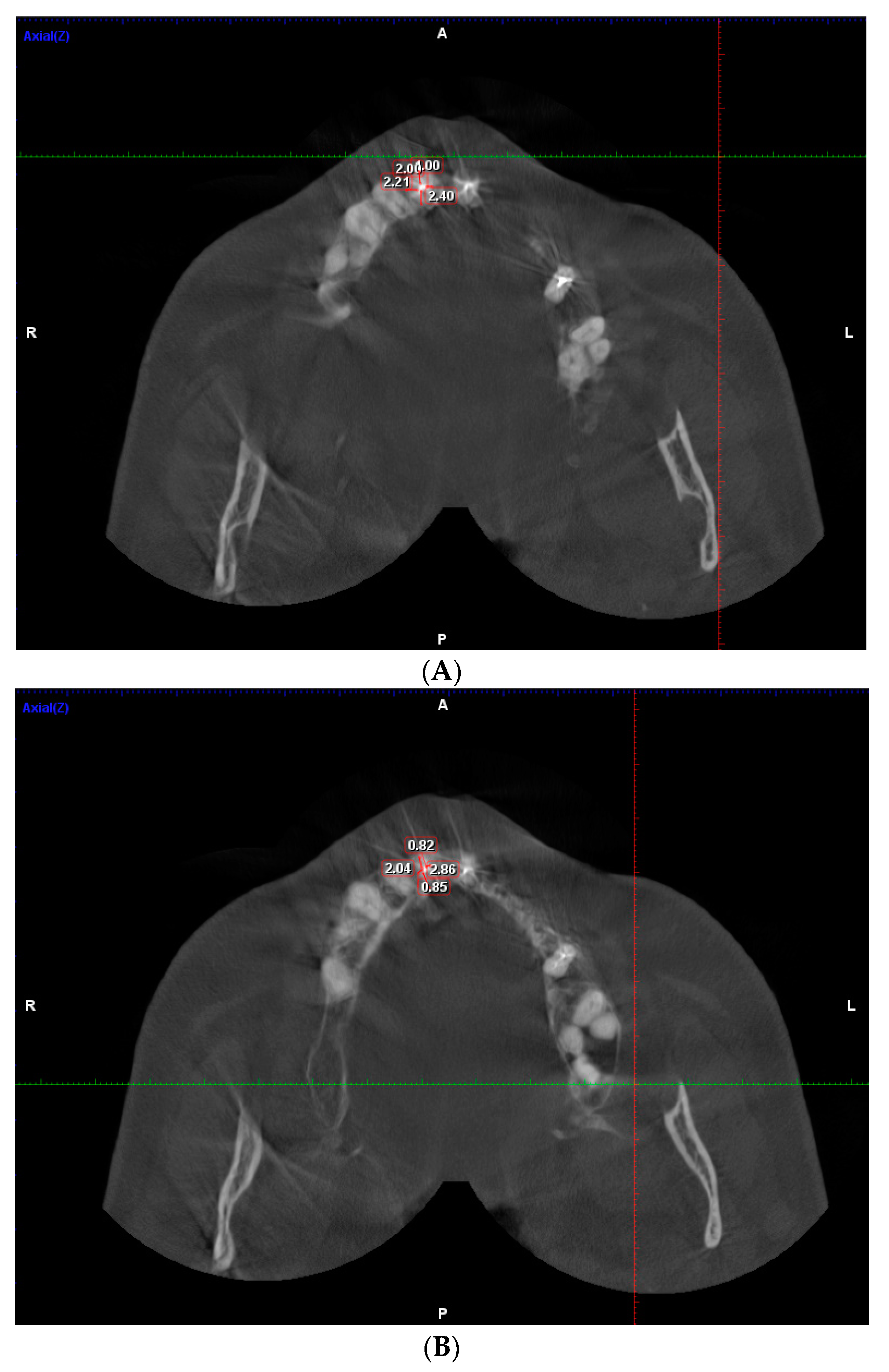
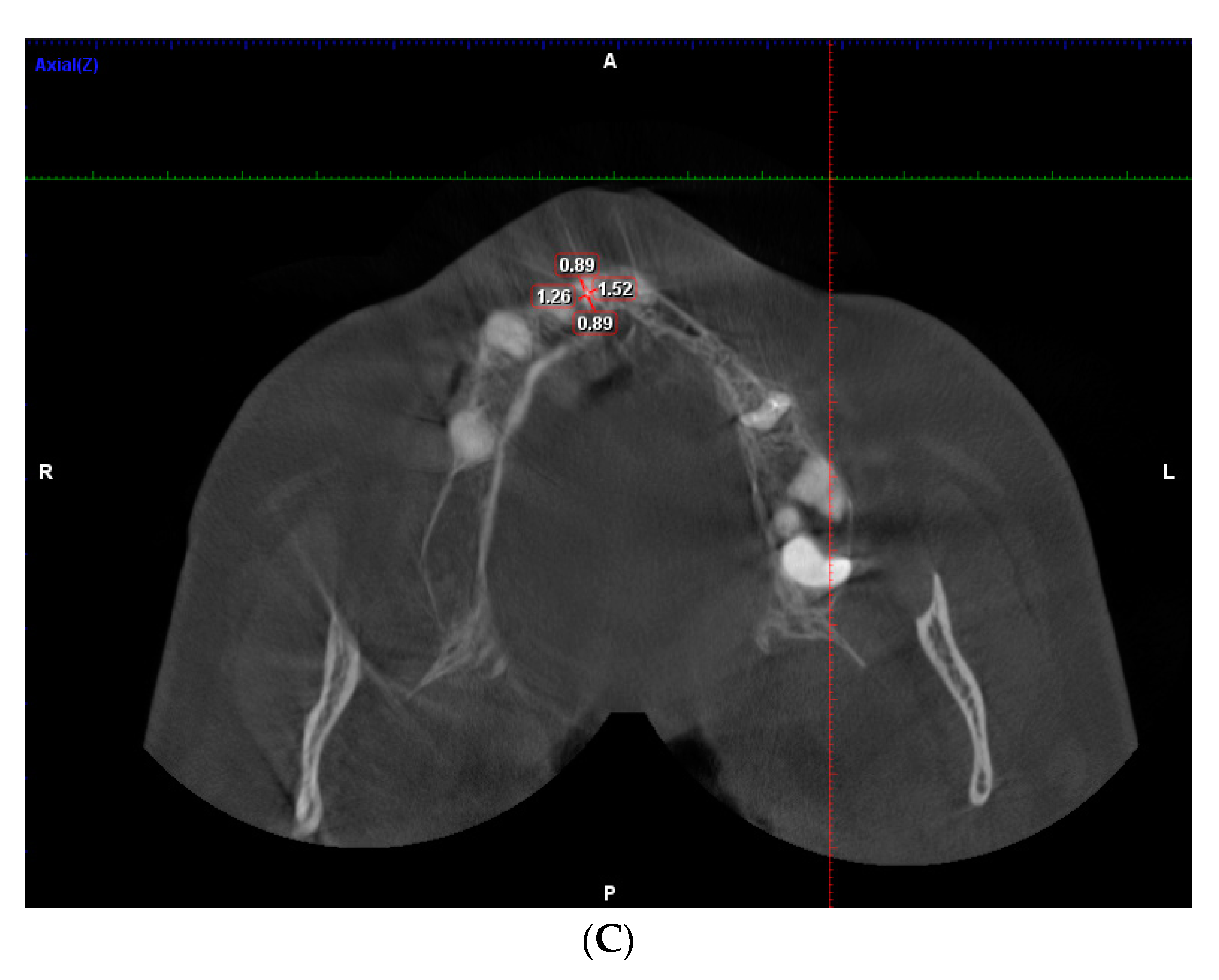
2. Materials and Methods
3. Results
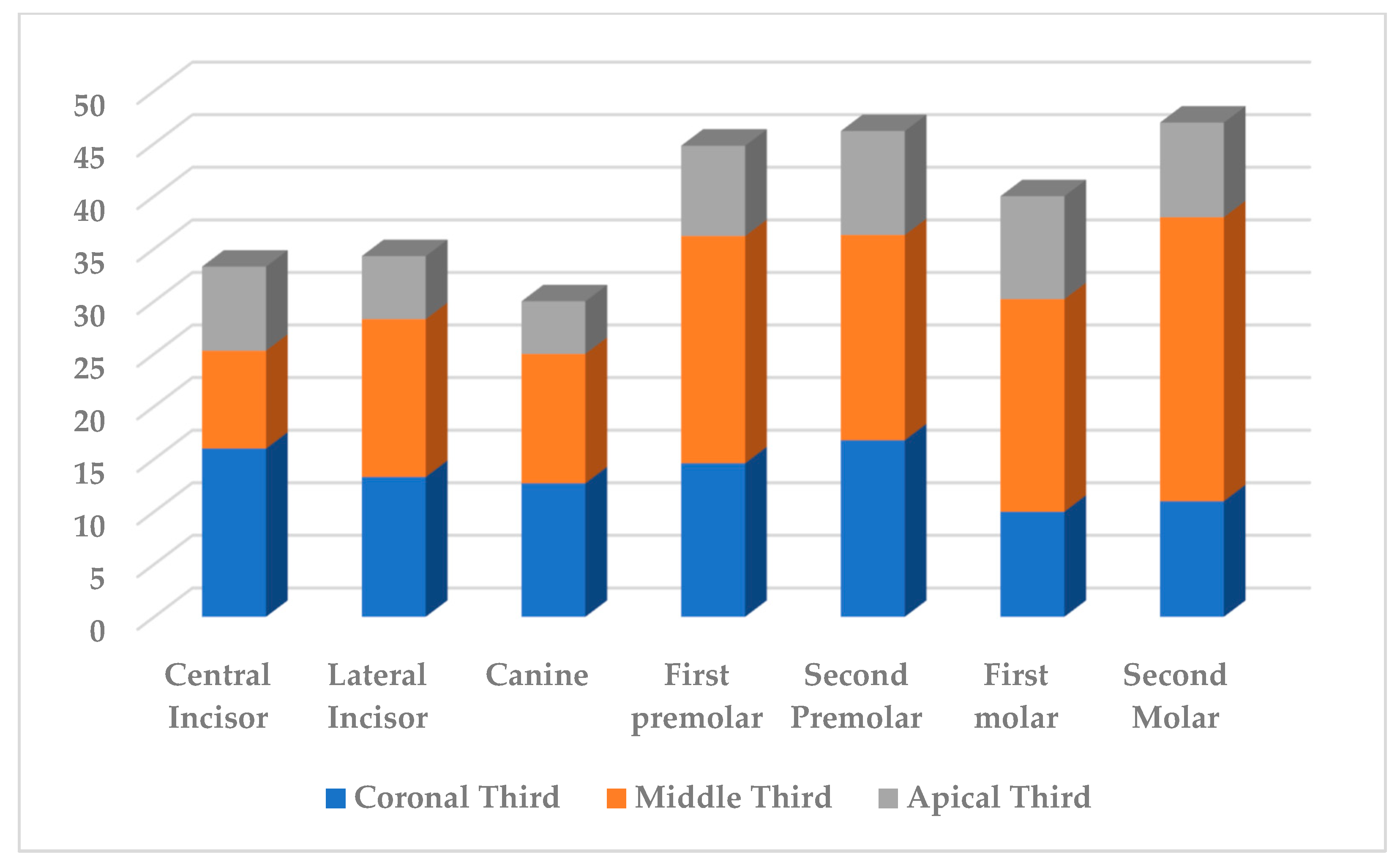
3.1. Measurment of DT of Maxillary Teeth
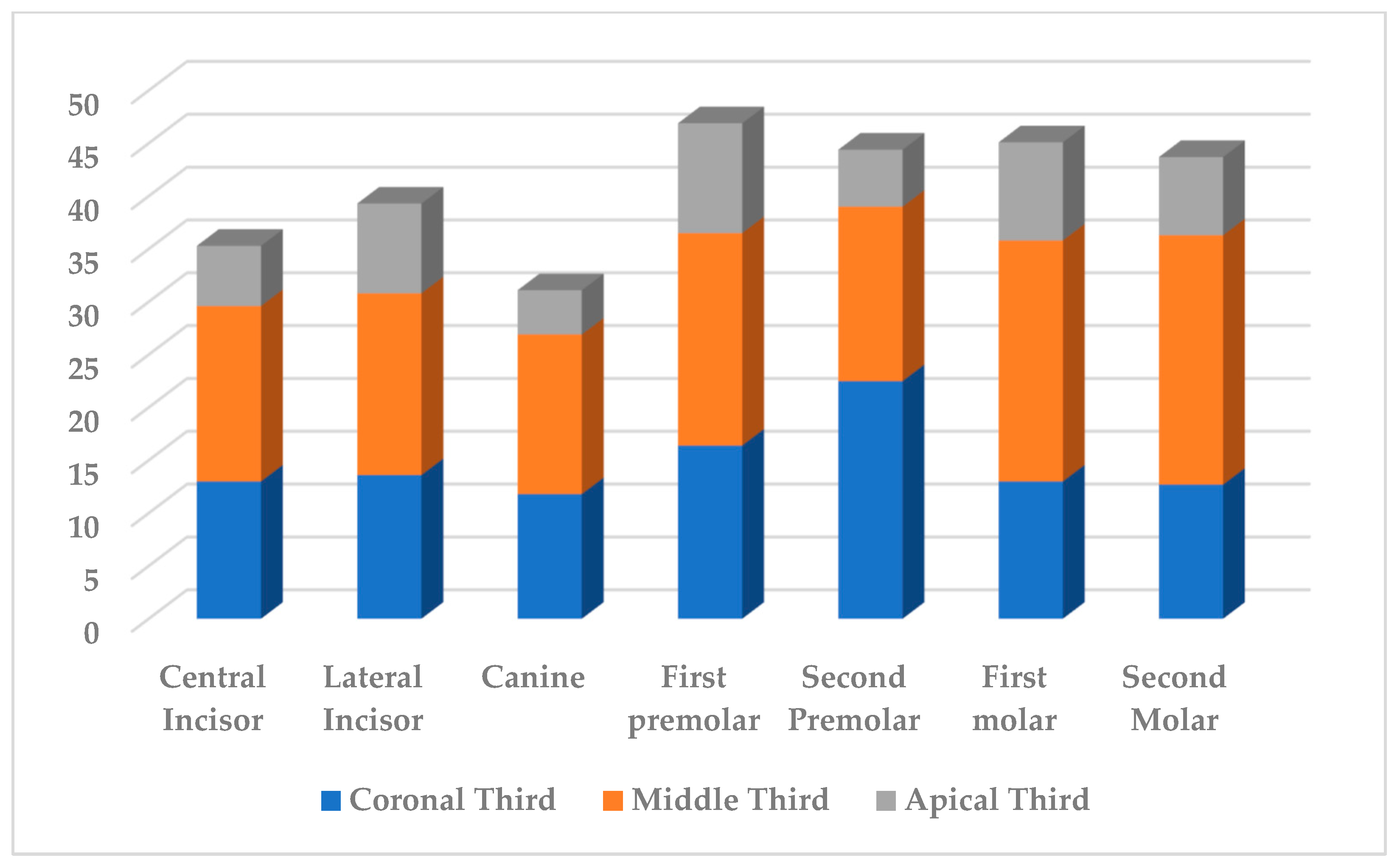
3.2. Measurment of DT Mandibular Teeth
3.3. Dentinal Thickness in Apical Part
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sorensen, J.A.; Martinoff, J.T. Intracoronal reinforcement and coronal coverage: A study of endodontically treated teeth. J. Prosthet. Dent. 1984, 51, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Reeh, E.S.; Messer, H.H.; Douglas, W.H. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J. Endod. 1989, 15, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Razumova, S.; Brago, A.; Howijieh, A.; Barakat, H.; Manvelyan, A.; Kozlova, Y. An In Vitro Evaluation Study of the Geometric Changes of Root Canal Preparation and the Quality of Endodontic Treatment. Int. J. Dent. 2020, 2020, 8883704. [Google Scholar] [CrossRef] [PubMed]
- Razumova, S.; Brago, A.; Howijieh, A.; Barakat, H.; Kozlova, Y.; Baykulova, M. Evaluation of Cross-Sectional Root Canal Shape and Presentation of New Classification of Its Changes Using Cone-Beam Computed Tomography Scanning. Appl. Sci. 2020, 10, 4495. [Google Scholar] [CrossRef]
- Lammertyn, P.A.; Rodrigo, S.B.; Brunotto, M.; Crosa, M. Furcation groove of maxillary first premolar, thickness and dental structures. J. Endod. 2009, 35, 814–817. [Google Scholar] [CrossRef]
- Halle, E.B.; Nicholls, J.I.; Hassel, H.I. An in-vitro comparison of retention between a hollow post and core and a custom hollow post andcore. J. Endod. 1984, 10, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Arunpraditkul, S.; Saengsanon, S.; Pakviwat, W. Fracture resistance of endodontically treated teeth: Three walls versus four walls of remaining coronal tooth structure. J. Prosthodont. 2009, 18, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Faria, A.C.; Rodrigues, R.C.; de Almeida Antunes, R.P.; de Mattos Mda, G.; Ribeiro, R.F. Endodontically treated teeth: Characteristics and considerations to restore them. J. Prosthodont. Res. 2011, 55, 69–74. [Google Scholar] [CrossRef]
- Bramante, C.M.; Berbert, A.; Borges, R.P. A methodology for evaluation of root canal instrumentation. J. Endod. 1987, 13, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Calt, S.; Serper, A. Smear layer removal by EGTA. J. Endod. 2000, 26, 459–461. [Google Scholar] [CrossRef]
- Wilcox, L.R.; Swift, M.L. Endodontic retreatment in small and large curved canals. J. Endod. 1991, 17, 313–315. [Google Scholar] [CrossRef]
- Leseberg, D.A.; Montgomery, S. The effects of Canal Master, Flex-R, and K-Flex instrumentation on root canal configuration. J. Endod. 1991, 17, 59–65. [Google Scholar] [CrossRef] [PubMed]
- McCann, J.T.; Keller, D.L.; LaBounty, G.L. Remaining dentin/cementum thickness after hand or ultrasonic instrumentation. J. Endod. 1990, 16, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Archer, R.; Reader, A.; Nist, R.; Beck, M.; Meyers, W.J. An in vivo evaluation of the efficacy of ultrasound after step-back preparation in mandibular molars. J. Endod. 1992, 18, 549–552. [Google Scholar] [CrossRef]
- Rödig, T.; Hülsmann, M.; Mühge, M.; Schäfers, F. Quality of preparation of oval distal root canals in mandibular molars using nickel-titanium instruments. Int. Endod. J. 2002, 35, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Peters, O.A.; Boessler, C.; Paqué, F. Root canal preparation with a novel nickel-titanium instrument evaluated with micro-computed tomography: Canal surface preparation over time. J. Endod. 2010, 36, 1068–1072. [Google Scholar] [CrossRef]
- Peters, O.A.; Peters, C.I.; Schönenberger, K.; Barbakow, F. ProTaper rotary root canal preparation: Effects of canal anatomy on final shape analysed by micro CT. Int. Endod. J. 2003, 36, 86–92. [Google Scholar] [CrossRef]
- Stern, S.; Patel, S.; Foschi, F.; Sherriff, M.; Mannocci, F. Changes in centring and shaping ability using three nickel–titanium instrumentation techniques analysed by micro-computed tomography (μCT). Int. Endod. J. 2012, 45, 514–523. [Google Scholar] [CrossRef]
- Versiani, M.A.; Pécora, J.D.; Sousa-Neto, M.D. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int. Endod. J. 2013, 46, 800–807. [Google Scholar] [CrossRef]
- Versiani, M.A.; Pécora, J.D.; Sousa-Neto, M.D. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int. Endod. J. 2011, 44, 682–687. [Google Scholar] [CrossRef]
- Yang, Y.; Shen, Y.; Ma, J.; Cao, Y.; Haapasalo, M. A Micro-Computed Tomographic Assessment of the Influence of Operator’s Experience on the Quality of WaveOne Instrumentation. J. Endod. 2016, 42, 1258–1262. [Google Scholar] [CrossRef]
- Peters, O.A.; Laib, A.; Göhring, T.N.; Barbakow, F. Changes in root canal geometry after preparation assessed by high-resolution computed tomography. J. Endod. 2001, 27, 1–6. [Google Scholar] [CrossRef]
- Peters, O.A.; Laib, A.; Rüegsegger, P.; Barbakow, F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J. Dent. Res. 2000, 79, 1405–1409. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Shen, Y.; Zhou, X.; Haapasalo, M. Remaining root dentin thickness in mesiobuccal canals of maxillary first molars after attempted removal of broken instrument fragments. Aust. Endod. J. 2015, 41, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Haralur, S.B.; Al-Qahtani, A.S.; Al-Qarni, M.M.; Al-Homrany, R.M.; Aboalkhair, A.E. Influence of remaining dentin wall thickness on the fracture strength of endodontically treated tooth. J. Conserv. Dent. 2016, 19, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Ha, W.N.; Chaves, G.S.; Decurcio, D.; Estrela, C.; Peters, O.A.; Rossi-Fedele, G. Remaining dentinal thickness after simulated post space preparation and the fit of prefabricated posts to root canal preparation shapes. J. Am. Dent. Assoc. 2021, 152, 1020–1032. [Google Scholar] [CrossRef] [PubMed]
- Versiani, M.A.; Carvalho, K.K.T.; Martins, J.N.R.; Custódio, A.L.N.; Castro, M.A.A.; Akaki, E.; Silva-Sousa, Y.T.C.S.; Sousa-Neto, M.D. Effects of root canal enlargement on unprepared areas and coronal dentine thickness of three-rooted maxillary first premolars with different root configurations: A stepwise micro-CT study. Int. Endod. J. 2022, 55, 1262–1273. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Central Incisors | Lateral Incisors | Canines | First Premolars | Second Premolars | First Molars | Second Molars |
|---|---|---|---|---|---|---|---|
| Young group | 50 intact 48 treated | 55 intact 50 treated | 55 intact 40 treated | 55 intact 48 treated | 55 intact 50 treated | 50 intact 48 treated | 55 intact 43 treated |
| Middle-age group | 55 intact 55 treated | 55 intact 55 treated | 55 intact 54 treated | 55 intact 53 treated | 55 intact 55 treated | 55 intact 50 treated | 50 intact 56 treated |
| Elderly | 55 intact 55 treated | 55 intact 54 treated | 55 intact 54 treated | 55 intact 51 treated | 54 intact 55 treated | 55 intact 60 treated | 47 intact 60 treated |
| Group | Central Incisors | Lateral Incisors | Canines | First Premolars | Second Premolars | First Molars | Second Molars |
|---|---|---|---|---|---|---|---|
| Young group | 55 intact 49 treated | 55 intact 48 treated | 55 intact 43 treated | 55 intact 49 treated | 55 intact 48 treated | 50 intact 48 treated | 55 intact 46 treated |
| Middle-age group | 55 intact 49 treated | 55 intact 50 treated | 55 intact 51 treated | 55 intact 50 treated | 55 intact 50 treated | 55 intact 53 treated | 50 intact 56 treated |
| Elderly | 55 intact 55 treated | 55 intact 60 treated | 55 intact 60 treated | 55 intact 55 treated | 50 intact 60 treated | 50 intact 60 treated | 46 intact 60 treated |
| Tooth | Largest Loss of Dentine | Least Amount Loss of Dentine | ||||
|---|---|---|---|---|---|---|
| Coronal Third | Middle Third | Apical Third | Coronal Third | Middle Third | Apical Third | |
| Central incisors | Buccal wall 27.7% (Elderly) | Mesial wall 12.1% (Elderly) | Buccal wall 13% (Middle) | Distal wall 9.4% (Young) | Mesial wall 7.8% (young) | Mesial wall 3.6% (young) |
| Lateral incisors | Palatal wall 14.7% (young) | Palatal wall 20.4% (Middle) | Mesial wall 16.9% (Middle) | Mesial wall 9.5% (young) | Mesial wall 10.3% (middle) | Buccal wall 1.7% (Middle) |
| Canines | Distal wall 16.7% (Elderly) | Distal wall 17.3% (Middle) | Mesial wall 12.1% (Elderly) | Buccal wall 8.5% (Young) | Buccal wall 11.3% (Elderly) | Distal wall 3.6% (Young) |
| First Premolar | Distal wall 21.2% (Elderly) | Mesial wall palatal root 31% (Middle) | Buccal wall palatal root 20% (Young) | Palatal wall 12.4% (Elderly) | Distal wall buccal root 14.7% (Middle) | Palatal wall Buccal root 3% (Elderly) |
| Second Premolar | Mesial wall 22.3% (Elderly) | Mesial wall 24.5% (Middle) | Distal wall 19.2% (Elderly) | Palatal wall 10.7% (Young) | Palatal wall 8.3% (Young) | Buccal wall 4.2% (Young) |
| First Molar | Distal wall 13.9% (Middle) | Distal wall Mesio-Buccal root 32.5% (Elderly) | Distal wall Mesio-Buccal root 25.5% (Middle) | Mesial wall 6.4% (Middle) | Buccal wall Disto-buccal root 13.5% (Young) | Distal wall Palatal root 1.4% (Young) |
| Second Molar | Distal wall 14.7% (Elderly) | Mesial wall Mesio-Buccal root 45.3% (Elderly) | Mesial wall Mesio-Buccal root 18.6% (Young) | Palatal wall 8.6% (Young) | Mesial wall Palatal root 13.7% (Young) | Mesial wall Palatal root 2.5% (Young) |
| Tooth | Largest Loss of Dentine | Least Amount Loss of Dentine | ||||
|---|---|---|---|---|---|---|
| Coronal Third | Middle Third | Apical Third | Coronal Third | Middle Third | Apical Third | |
| Central incisors | Distal wall 19.6% (Elderly) | Distal wall 23% (Middle) | Mesial wall 8.2% (Middle) | Lingual wall 5.4% (Young) | Buccal wall 11.1% (Young) | Buccal wall 1.6% (Young) |
| Lateral incisors | Mesial wall 19.6% (Elderly) | Distal wall 23.5% (Middle) | Distal wall 15.8% (Elderly) | Lingual wall 7.8% (Young) | Buccal wall 11.8% (Young) | Lingual wall 1.9% (Young) |
| Canines | Lingual wall 14% (Middle) | Lingual wall 13.4% (Middle) | Lingual wall 7.1% (Middle) | Mesial wall 8.8% (Young) | Mesial wall 9.4% (Young) | Distal wall 1.2% (Young) |
| First Premolar | Distal wall 21.2% (Elderly) | Lingual wall 23.2% (Elderly) | Mesial wall 19.3% (Elderly) | Mesial wall 14.1% (Middle) | Distal wall 17.7% (Young) | Buccal wall 6% (Elderly) |
| Second Premolar | Mesial wall 35.4% (Middle) | Mesial wall 21.8% (Young) | Mesial wall 11.8% (Middle) | Buccal wall 12% (Elderly) | Buccal wall 10.1% (Young) | Mesial wall 0.9% (Young) |
| First Molar | Distal wall 18.3% (Middle) | Mesial wall Distal root 40.3% (Elderly) | Buccal wall Mesial root 15.4% (Elderly) | Mesial wall 9.1% (Middle) | Lingual wall mesial root 16.4% (Young) | Lingual wall Distal root 2.9% (Middle) |
| Second Molar | Mesial wall 13.6% (Young) | Mesial wall Distal root 31.8% (Elderly) | Mesial wall Distal root 17.2% (Middle) | Buccal wall 11.1% (Young) | Lingual wall Distal root 13.6% (Young) | Buccal wall Distal root 2.1% (Young) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razumova, S.; Brago, A.; Barakat, H.; Serebrov, D.; Guryeva, Z.; Parshin, G.S.; Troitskiy, V.I. Evaluation of Dentinal Thickness and Remaining Dentine Volume around Root Canals Using Cone-Beam Computed Tomography Scanning. Dent. J. 2023, 11, 124. https://doi.org/10.3390/dj11050124
Razumova S, Brago A, Barakat H, Serebrov D, Guryeva Z, Parshin GS, Troitskiy VI. Evaluation of Dentinal Thickness and Remaining Dentine Volume around Root Canals Using Cone-Beam Computed Tomography Scanning. Dentistry Journal. 2023; 11(5):124. https://doi.org/10.3390/dj11050124
Chicago/Turabian StyleRazumova, Svetlana, Anzhela Brago, Haydar Barakat, Dimitriy Serebrov, Zoya Guryeva, Gleb S. Parshin, and Vasiliy I. Troitskiy. 2023. "Evaluation of Dentinal Thickness and Remaining Dentine Volume around Root Canals Using Cone-Beam Computed Tomography Scanning" Dentistry Journal 11, no. 5: 124. https://doi.org/10.3390/dj11050124