
Etiological Factors of Molar Incisor Hypomineralization: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
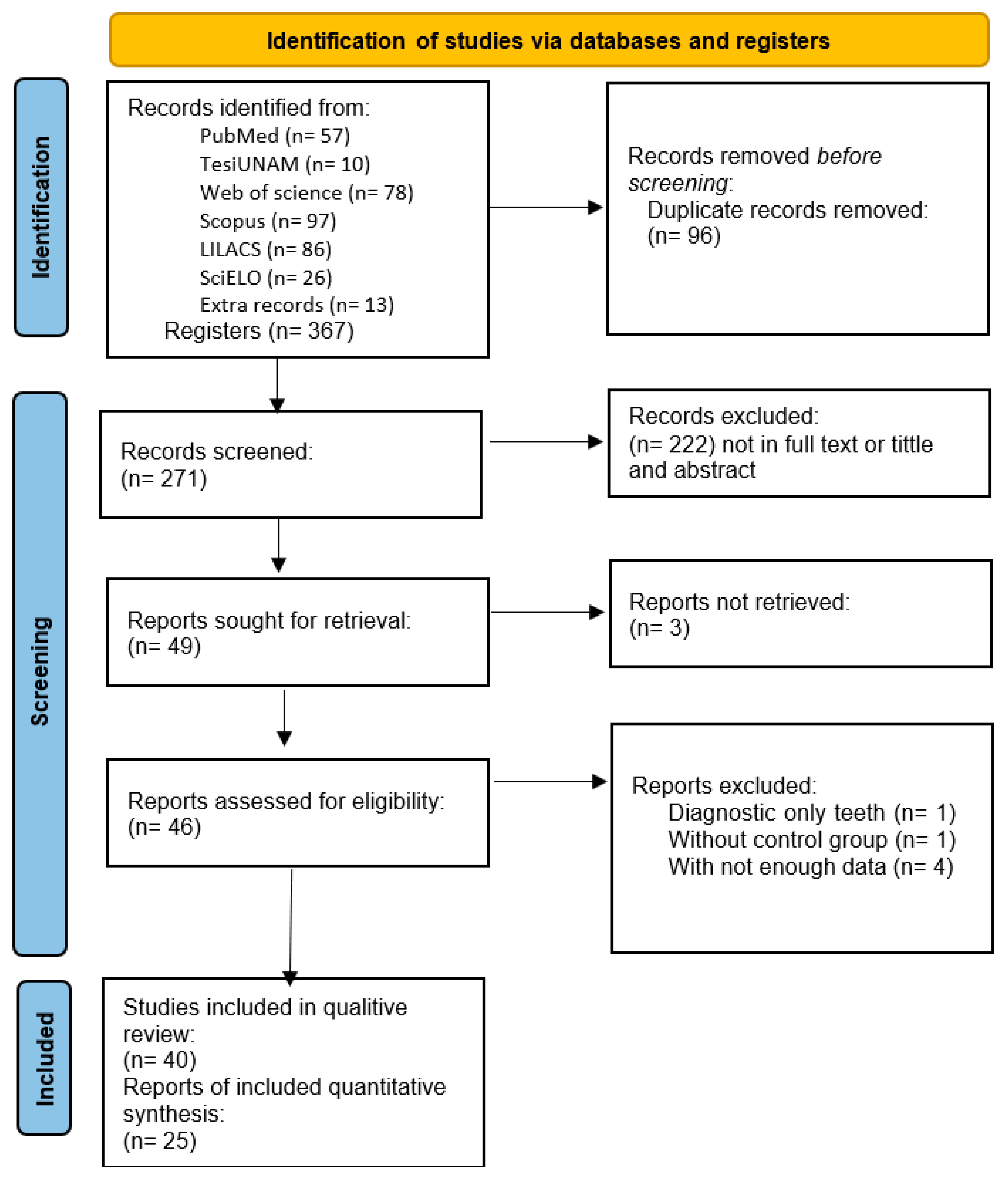
2.1. Search Strategy and Study Selection
2.2. Participants and Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Analysis and Meta-Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lygidakis, N.A.; Garot, E.; Somani, C.; Taylor, G.D.; Rouas, P.; Wong, F.S.L. Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): An updated European Academy of Paediatric Dentistry policy document. Eur. Arch. Paediatr. Dent. 2022, 23, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Weerheijm, K.L.; Duggal, M.; Mejàre, I.; Papagiannoulis, L.; Koch, G.; Martens, L.C.; Hallonsten, A.-L. Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: A summary of the European meeting on MIH held in Athens, 2003. Eur. J. Paediatr. Dent. 2003, 4, 110–113. [Google Scholar] [PubMed]
- Mittal, N. Phenotypes of Enamel Hypomineralization and Molar Incisor Hypomineralization in Permanent Dentition: Identification, Quantification and Proposal for Classification. J. Clin. Pediatr. Dent. 2016, 40, 367–374. [Google Scholar] [CrossRef]
- Negre-Barber, A.; Montiel-Company, J.M.; Boronat-Catalá, M.; Catalá-Pizarro, M.; Almerich-Silla, J.M. Hypomineralized Second Primary Molars as Predictor of Molar Incisor Hypomineralization. Sci. Rep. 2016, 6, 31929. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Kup, E. On the Etiology of Molar-Incisor Hypomineralization. Caries Res. 2016, 50, 166–169. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.B.; Machado, V.; Mascarenhas, P.; Mendes, J.J.; Botelho, J. The prevalence of molar-incisor hypomineralization: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 22405. [Google Scholar] [CrossRef] [PubMed]
- Özgül, B.M.; Sakaryalı, D.; Tirali, R.E.; Çehreli, S.B. Does MIH Affects Preoperative and Intraoperative Hypersensitivity? J. Clin. Pediatr. Dent. 2022, 46, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Kühnisch, J.; The GINI-10 Plus Study Group; Thiering, E.; Heitmüller, D.; Tiesler, C.M.T.; Grallert, H.; Heinrich-Weltzien, R.; Hickel, R.; Heinrich, J. Genome-wide association study (GWAS) for molar-incisor hypomineralization (MIH). Clin. Oral. Investig. 2014, 18, 677–682. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Martínez Díaz, J.; Ortega Chacón, V.; Muñoz Ronda, F. El diseño de preguntas clínicas en la práctica basada en la evidencia: Modelos de formulación. Enfermería Global. 2016, 15, 431–438. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The New Castle-Otawa Scale (NOS) for Assessing the Quality of Non Randomized Studies in Meta Analysis. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 3 April 2023).
- Brogårdh-Roth, S.; Matsson, L.; Klingberg, G. Molar-incisor hypomineralization and oral hygiene in 10- to-12-yr-old Swedish children born preterm. Eur. J. Oral. Sci. 2011, 119, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.F.; Costa-Silva, C.M.; Jeremias, F.; Santos-Pinto, L.; Zuanon, A.C.C.; Cordeiro, R.C.L. Molar incisor hypomineralisation: Possible aetiological factors in children from urban and rural areas. Eur. Arch. Paediatr. Dent. 2012, 13, 164–170. [Google Scholar] [CrossRef]
- Sönmez, H.; Yıldırım, G.; Bezgin, T. Putative factors associated with molar incisor hypomineralisation: An epidemiological study. Eur. Arch. Paediatr. Dent. 2013, 14, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.F.; Jeremias, F.; Costa-Silva, C.M.; Santos-Pinto, L.; Zuanon, A.C.C.; Cordeiro, R.C.L. Aetiology of molar-incisor hypomineralisation (MIH) in Brazilian children. Eur. Arch. Paediatr. Dent. 2013, 14, 233–238. [Google Scholar] [CrossRef]
- Ghanim, A.; Manton, D.; Bailey, D.; Mariño, R.; Morgan, M. Risk factors in the occurence of molar-incisor hypomineralization amongst a group of Iraqi children. Int. J. Paed Dent. 2013, 23, 197–206. [Google Scholar] [CrossRef]
- Pitiphat, W.; Luangchaichaweng, S.; Pungchanchaikul, P.; Angwaravong, O.; Chansamak, N. Factors associated with molar incisor hipomineralization in Thai children. Eur. J. Oral. Sci. 2014, 122, 265–270. [Google Scholar] [CrossRef]
- Allazzam, S.M.; Alaki, S.M.; El Meligy, O. Molar incisor hypomineralization, prevalence, and etiology. Int. J. Dent. 2014, 2014, 234508. [Google Scholar] [CrossRef]
- Tourino, L.F.P.G. Prevalence of MIH in a Municipality in Southeast Brazil. [dissertation of PhD] Bello Horizonte: Faculda de Odontología de la Universidad de Federal de Minas Gerais. 2015. Available online: https://repositorio.ufmg.br/bitstream/1843/BUBD-ACYESL/1/tese_luciana_fonseca_p_dua_gon_alves_tourino.pdf (accessed on 27 December 2022).
- Garot, E.; Manton, D.; Rouas, P. Peripartum events and molar-incisor hypomineralisation (MIH) amongst young patients in southwest France. Eur. Arch. Paediatr. Dent. 2016, 17, 245–250. [Google Scholar] [CrossRef]
- Teixeira, R.J.P.B.; Andrade, N.S.; Queiroz, L.C.C.; Mendes, F.M.; Moura, M.S.; Moura, L.F.A.D.; Lima, M.D.M. Exploring the association between genetic and environmental factors and molar incisor hypomineralization: Evidence from a twin study. Int. J. Paediatr. Dent. 2018, 28, 198–206. [Google Scholar] [CrossRef]
- Gurrusquieta, B.J.; Núñez, V.M.M.; López, M.L.A.J. Prevalence of Molar Incisor Hypomineralization in Mexican Children. J. Clin. Pediatr. Dent. 2017, 41, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Rai, A.; Singh, A.; Menon, I.; Singh, J.; Rai, V.; Aswal, G.S. Molar incisor hypomineralization: Prevalence and risk factors among 7-9 years old school children in Muradnagar, Ghaziabad. Open Dent. J. 2018, 12, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Koruyucu, M.; Özel, S.; Tuna, E.B. Prevalence and etiology of molar-incisor hypomineralization (MIH) in the city of Istanbul. J. Dent. Sci. 2018, 13, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Giuca, M.R.; Cappè, M.; Carli, E.; Lardani, L.; Pasini, M. Investigation of Clinical Characteristics and Etiological Factors in Children with Molar Incisor Hypomineralization. Int. J. Dent. 2018, 2018, 7584736. [Google Scholar] [CrossRef]
- Kılınç, G.; Çetin, M.; Köse, B.; Ellidokuz, H. Prevalence, aetiolgy and treatment of molar incisor hypomineralization in children living in Izmir city (Turkey). Int. J. Pediatr. Dent. 2019, 29, 775–782. [Google Scholar] [CrossRef]
- Mejía, J.; Restrepo, M.; González, S.; Álvarez, L.; Santos-Pinto, L.; Escobar, A. Molar Incisor Hypomineralization in Colombia: Prevalence, Severity and Associated Risk Factors. J. Clin. Pediatr. Dent. 2019, 43, 185–189. [Google Scholar] [CrossRef]
- Wogelius, P.; Viuff, J.; Haubek, D. Use of asthma drugs and prevalence of molar incisor hypomineralization. Int. J. Paediatr. Dent. 2020, 30, 734–740. [Google Scholar] [CrossRef]
- Glodkowska, N.; Emerich, K. Molar incisor hypomineralization: Prevalence and severity among children from Northern Poland. Eur. J. Paediatr. Dent. 2019, 20, 59–66. [Google Scholar] [CrossRef]
- Einollahi, M.; Hekmatfar, S.; Molaei, M. Association between molar incisor hypomineralization and both prenatal and postnatal factors in 8-10 year old children in ardebil. J. Evol. Med. Dent. Sci. 2020, 9, 3606–3610. [Google Scholar] [CrossRef]
- Padmanabhan, V.; Rahman, M.; Osama, R.; Anas, R. Molar Incisor Hypomineralization Prevalence in Arab Children in UAE and its Association with Risk Factors—A Cross Sectional Study. J. Int. Dent. Med. Res. 2021, 14, 1100–1106. [Google Scholar]
- Alhowaish, L.; Baidas, L.; Aldhubaiban, M.; Bello, L.L.; Al-Hammad, N. Etiology of Molar-Incisor Hypomineralization (MIH): A Cross-Sectional Study of Saudi Children. Children 2021, 8, 466. [Google Scholar] [CrossRef]
- Elzein, R.; Chouery, E.; Abdel-Sater, F.; Bacho, R.; Ayoub, F. Molar-incisor hypomineralisation in Lebanon: Association with prenatal, natal and postnatal factors. Eur. Arch. Paediatr. Dent. 2021, 22, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, R.N.; Basha, S.; Al-Thomali, Y.; Al Zahrani, F.S.; Ashour, A.A.; Al Shamrani, A.S.; Almutair, N.E. Frequency of molar incisor hypomineralization and associated factors among children with special health care needs. Ann. Saudi Med. 2021, 41, 238–245. [Google Scholar] [CrossRef]
- Fonseca-Souza, G.; Fatturi, A.L.; Fraiz, F.C.; Assunção, L.R.D.S.; Feltrin-Souza, J. What are the systemic factors associated with the molar-incisor hypomineralization etiology? Pesqui. Bras. Odontopediatria Clín Integr. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Mariam, S.; Goyal, A.; Dhareula, A.; Gauba, K.; Bhatia, S.K.; Kapur, A. A case-controlled investigation of risk factors associated with molar incisor hypomineralization (MIH) in 8-12 year-old children living in Chandigarh. India. Eur. Arch. Paediatr. Dent. 2022, 23, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Yadav, G.; Tripathi, A.M.; Dhinsa, K.; Arora, D.; Verma, S.; Saha, S. Molar Incisor Hypomineralization: Prevalence, Associated Risk Factors, Its Relation with Dental Caries and Various Enamel Surface Defects in 8-16-year-old Schoolchildren of Lucknow District. Int. J. Clin. Pediatr. Dent. 2022, 15, 1–8. [Google Scholar] [CrossRef]
- Almuallem, Z.; Alsuhaim, A.; Alqudayri, A.; Aljarid, S.; Alotaibi, M.M.; Alkraida, R.; Faden, R.; Mojaleed, F.; Alruwaithi, M.; Al-Huraishi, H. Prevalence and possible aetiological factors of molar incisor hypomineralisation in Saudi children: A cross-sectional study. Saudi Dent. J. 2022, 34, 36–44. [Google Scholar] [CrossRef]
- Acosta, E.; Cortes, O.; Guzman, S.; Catala, M.; Lorente, M.; Arense, J.J. Relationship between molar incisor hypomineralization, intrapartium medication and illnesses in the first year of life. Sci. Rep. 2022, 12, 1637. [Google Scholar] [CrossRef]
- Kühnisch, J.; Mach, D.; Thiering, E.; Brockow, I.; Hoffmann, U.; Neumann, C.; Heinrich-Weltzien, R.; Bauer, C.-P.; Berdel, D.; Von Berg, A.; et al. Respiratory diseases are associated with molar-incisor hypomineralizations. Swiss Dent. J. 2014, 124, 286–293. [Google Scholar]
- Wuollet, E.; Laisi, S.; Salmela, E.; Ess, A.; Alaluusua, S. Molar-incisor hypomineralization and the association with childhood illnesses and antibiotics in a group of Finnish children. Acta Odontol. Scand. 2016, 74, 416–422. [Google Scholar] [CrossRef]
- Van Der Tas, J.T.; Elfrink, M.E.; Heijboer, A.C.; Rivadeneira, F.; Jaddoe, V.W.; Tiemeier, H.; Schoufour, J.D.; Moll, H.A.; Ongkosuwito, E.; Wolvius, E.B.; et al. Foetal, neonatal and child vitamin D status and enamel hypomineralization. Community Dent. Oral. Epidemiol. 2018, 46, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Flexeder, C.; Hassan, L.K.; Standl, M.; Schulz, H.; Kühnisch, J. Is There an Association between Asthma and Dental Caries and Molar Incisor Hypomineralisation? Caries Res. 2020, 54, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Ilczuk-Rypuła, D.; Zalewska, M.; Pietraszewska, D.; Dybek, A.; Nitecka-Buchta, A.; Postek-Stefańska, L. Prevalence and Possible Etiological Factors of Molar-Incisor Hypomineralization (MIH) in Population of Silesian Children in Poland: A Pilot Retrospective Cohort Study. Int. J. Environ. Res. Public. Health. 2022, 19, 8697. [Google Scholar] [CrossRef] [PubMed]
- Bondi, A.; Cortese, S.; Ortolane, A.; Argentieri, Á. Clinical characteristics and risk factors associated with Molar Hypomineralization. Rev. Fac. De Odontol. 2010, 25, 10–15. Available online: http://odontologia.uba.ar/wp-content/uploads/2018/06/vol25_n58_2010_art1.pdf (accessed on 3 April 2023).
- Rodrigues, F.; Ribeiro, P.; Thomaz, E.; Lima, G.; Neves, A.; Ribeiro, C.; Rodrigues, F.C.N.; Ribeiro, P.H.B.; Thomaz, E.B.A.F.; Lima, G.Q.T.; et al. Molar-Incisor Hypomineralization in Schoolchildren of São Luis, Brazil Maranhão: Prevalence and Associated Factors. Pesqui. Bras. Em Odontopediatria E Clínica Integr. 2015, 15, 271–278. [Google Scholar] [CrossRef]
- Andrade, N.S.; Pontes, A.S.; Paz, H.E.D.S.; Moura, M.S.; Moura, L.D.F.A.D.D.; Lima, M.D.D.M. Molar incisor hypomineralization in HIV-infected children and adolescents. Spec. Care Dentist. 2017, 37, 28–37. [Google Scholar] [CrossRef]
- Dantas-Neta, N.B.; Figueiredo, M.S.; Lima, C.C.B.; Bendo, C.B.; De Andrade, M.M.; Lima, M.D.D.M.; Pordeus, I.A.; Paiva, S.M. Factors associated with molar-incisor hypomineralisation in schoolchildren aged 8-10 years: A case-control study. Int. J. Paediatr. Dent. 2018, 28, 570–577. [Google Scholar] [CrossRef]
- Portella, P.D.; Fraiz, F.C.; Soares, R.C.; Nagata, A.G.; Tomaz, C.D.O.; Assunção, L.R.D.S. Molar-Incisor Hypomineralization and Associated Factors: A Case- Control Study. Pesqui. Bras. Odontopediatria Clín. Integr. 2018, 18, 4320. [Google Scholar] [CrossRef]
- Ardini, Y.D.; Ismail, N.N.; Azni, N.D.M.; Harun, N.A. Molar incisor hypomineralisation: Prevalence and associated risk factors among children at the Polyclinic, Kulliyyah of Dentistry, IIUM. Mater. Today Proc. 2019, 16, 2351–2356. [Google Scholar] [CrossRef]
- Lee, D.-W.; Kim, Y.-J.; Kim, S.O.; Choi, S.C.; Kim, J.; Lee, J.H.; Kim, H.J.; Shin, J.; Lee, N.-Y.; Kim, S.-M.; et al. Factors Associated with Molar-Incisor Hypomineralization: A Population-Based Case-Control Study. Pediatr. Dent. 2020, 42, 134–140. [Google Scholar]
- Fatturi, A.L.; Wambier, L.M.; Chibinski, A.C.; Assunção, L.R.D.S.; Brancher, J.A.; Reis, A.; Souza, J.F. A systematic review and meta-analysis of systemic exposure associated with molar incisor hypomineralization. Community Dent. Oral. Epidemiol. 2019, 47, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Garot, E.; Rouas, P.; Somani, C.; Taylor, G.D.; Wong, F.; Lygidakis, N.A. An update of the aetiological factors involved in molar incisor hypomineralisation (MIH): A systematic review and meta-analysis. Eur. Arch. Paediatr. Dent. 2022, 23, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.J.; Scurrah, K.J.; Craig, J.M.; Manton, D.J.; Kilpatrick, N. Etiology of molar incisor hypomineralization—A systematic review. Community Dent. Oral. Epidemiol. 2016, 44, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Jedeon, K.; Loiodice, S.; Marciano, C.; Vinel, A.; Lavier, M.-C.C.; Berdal, A.; Babajko, S. Estrogen and bisphenol A affect male rat enamel formation and promote ameloblast proliferation. Endocrinology 2014, 155, 3365–3375. [Google Scholar] [CrossRef]
- Piedrahita, M.; Mejía, J.; Santos, L. Bisfenol A e hipomineralización molar incisiva: Review. Acta Odont Venez. 2021, 59. Available online: https://www.actaodontologica.com/ediciones/2021/1/art-5/ (accessed on 3 April 2023).
- Kim, D.; Saada, A. The social determinants of infant mortality and birth outcomes in western developed nations: A cross country systematic review. Int. J. Environ. Res. Public. Health 2013, 10, 2296–2335. [Google Scholar] [CrossRef]
- Lopes, L.B.; Machado, V.; Botelho, J.; Haubek, D. Molar-incisor hypomineralization: An umbrella review. Acta Odontol. Scand. 2021, 79, 359–369. [Google Scholar] [CrossRef]
- Laisi, S.; Ess, A.; Sahlberg, C.; Arvio, P.; Lukinmaa, P.-L.; Alaluusua, S. Amoxicillin may cause molar incisor hypomineralization. J. Dent. Res. 2009, 88, 132–136. [Google Scholar] [CrossRef]
- Tung, K.; Fujita, H.; Yamashita, Y.; Takagi, Y. Effect of turpentine-induced fever during the enamel formation of rat incisor. Arch. Oral. Biol. 2006, 51, 464–470. [Google Scholar] [CrossRef]
- de Souza, J.F.; Gramasco, M.; Jeremias, F.; Santos-Pinto, L.; Giovanini, A.F.; Cerri, P.S.; Cordeiro, R.D.C.L. Amoxicillin diminishes the thickness of the enamel matrix that is deposited during the secretory stage in rats. Int. J. Paediatr. Dent. 2016, 26, 199–210. [Google Scholar] [CrossRef]
- Feltrin-Souza, J.; Jeremias, F.; Alaluusua, S.; Sahlberg, C.; Santos-Pinto, L.; Jernvall, J.; Sova, S.; Cordeiro, R.D.C.L.; Cerri, P.S. The effect of amoxicillin on dental enamel development in vivo. Braz. Oral. Res. 2020, 34, e116. [Google Scholar] [CrossRef]
- Kuscu, O.O.; Sandalli, N.; Dikmen, S.; Ersoy, O.; Tatar, I.; Turkmen, I.; Çaglar, E. Association of amoxicillin use and molar incisor hypomineralization in piglets: Visual and mineral density evaluation. Arch. Oral. Biol. 2013, 58, 1422–1433. [Google Scholar] [CrossRef]
- Hočevar, L.; Kovač, J.; Podkrajšek, K.T.; Battelino, S.; Pavlič, A. The possible influence of genetic aetiological factors on molar-incisor hypomineralisation. Arch. Oral. Biol. 2020, 118, 104848. [Google Scholar] [CrossRef] [PubMed]
- Jeremias, F.; Bussaneli, D.G.; Restrepo, M.; Pierri, R.A.G.; de Souza, J.F.; Fragelli, C.M.B.; Secolin, R.; Maurer-Morelli, C.V.; Cordeiro, R.D.C.L.; Scarel-Caminaga, R.M.; et al. Inheritance pattern of molar-incisor hypomineralization. Braz. Oral. Res. 2021, 35, e035. [Google Scholar] [CrossRef]
- Bussaneli, D.G.; Vieira, A.R.; Santos-Pinto, L.; Restrepo, M. Molar-incisor hypomineralisation: An updated view for aetiology 20 years later. Eur. Arch. Paediatr. Dent. 2022, 23, 193–198. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Quintini, M.; Lelli, M.; Tarterini, F.; Foltran, I.; Scribante, A. Biomimetic Action of Zinc Hydroxyapatite on Remineralization of Enamel and Dentin: A Review. Biomimetics 2023, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Trapani, B.; Gallo, S.; Radu, M.; Scribante, A. Biomimetic hydroxyapatite paste for molar-incisor hypomineralization: A randomized clinical trial. Oral. Dis. 2022. [Google Scholar] [CrossRef]
- Poggio, C.; Gallo, S. Frontiers in Restorative Dentistry Biomaterials and Endodontic Instruments. Materials 2023, 16, 475. [Google Scholar] [CrossRef] [PubMed]
- Sezer, B.; Kargul, B. Effect of Remineralization Agents on Molar-Incisor Hypomineralization-Affected Incisors: A Randomized Controlled Clinical Trial. J. Clin. Pediatr. Dent. 2022, 46, 192–198. [Google Scholar] [CrossRef]
- Kühnisch, J.; Thiering, E.; Kratzsch, J.; Heinrich-Weltzien, R.; Hickel, R.; Heinrich, J.; Wichmann, H.; Sausenthaler, S.; Zutavern, A.; Chen, C.-M.; et al. Elevated serum 25(OH)-vitamin D levels are negatively correlated with molar-incisor hypomineralization. J. Dent. Res. 2015, 94, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Nørrisgaard, P.E.; Haubek, D.; Kühnisch, J.; Chawes, B.L.; Stokholm, J.; Bønnelykke, K.; Bisgaard, H. Association of High-Dose Vitamin D Supplementation During Pregnancy With the Risk of Enamel Defects in Offspring: A 6-Year Follow-up of a Randomized Clinical Trial. JAMA Pediatr. 2019, 173, 924–930. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author Names and Country | Type of Study | No. of Participants | MIH Prevalence (%) | Newcastle–Ottawa | Findings | ||
|---|---|---|---|---|---|---|---|
| S | C | E | |||||
| Brogard-Roth et al., 2010 [13] Sweden | Cross- sectional case–control study | 144 | 38 | *** | * | * | Low gestational age and low birth weight increased the risk of MIH and oral health problems (more plaque, gingival inflammation, and behavior management problems). |
| Bondi et al., 2010 [46] Argentine | Case–control | 196 | 50 | *** | ** | * | MIH presented an association with respiratory infections, special formula milk, and nonsteroidal and anti-inflammatory drugs. |
| Souza JF. et al., 2012 [14] Brazil | Cross-sectional | 903 | 19.9 | *** | * | *** | Health problems in pregnancy. History of throat infections, periods of fever, and amoxicillin intake in the postnatal stage were found to be associated with MIH. There was no correlation with birth prematurity or low weight at birth. |
| Sönmez H. et al., 2012 [15] Turkey | Cross-sectional | 3827 | 7.7 | *** | ** | *** | Prematurity, gastrointestinal problems, pneumonia, frequent fever, measles, and chickenpox before 4 years old were found to be associated with MIH. |
| Souza JF. et al., 2013 [16] Brazil | Cross-sectional | 1151 | 12.3 | *** | ** | ** | Cesarean birth, low weight, and maternal illness were not associated with MIH.The occurrence of anemia was not significant. |
| Ghanim A. et al., 2013 [17] Iraq | Cross-sectional | 823 | 18.6 | *** | * | *** | Infections and lung diseases, unexplained fever, tonsillitis, pneumonia, exposure to drugs during the first year, and breastfeeding for less than 6 months were found to be associated with MIH. |
| Kühnisch J. et al., 2013 [41] Germany | Cohort | 693 | 37.9 | ** | * | *** | There was an associationwith respiratory problems. |
| Pitiphat W. et al., 2014 [18] Thailand | Cross-sectional | 282 | 27.7 | *** | * | *** | Birth by cesarean section and poor health in the first three years were found to be associated with MIH. |
| Allazzam SM. et al., 2014 [19] Egypt | Cross-sectional | 267 | 8.6 | *** | * | ** | Many diseases during the first four years of life (tonsillitis, adenoiditis, and asthma), as well as antibiotic consumption and febrile symptoms, were found to be associated with MIH. |
| Nogueira F. et al., 2015 [47] Brazil | Case–control | 1237 | 2.5 | ** | * | ** | HMI has no association with prenatal or postnatal factors in the first three years of life. |
| Tourino L. et al., 2015 [20] Brazil | Cross-sectional | 1181 | 20.4 | *** | ** | ** | Asthma/bronchitis, high fever, and the use of antibiotics in the first four years of life were factors associated with MIH. |
| Woullet E. et al., 2016 [42] Finland | Cohort | 287 | 11.5 | **** | * | *** | Acute otitis media and the use of penicillin and macrolides were found to be associated with MIH. |
| Garot E. et al., 2016 [21] France | Cross-sectional | 819 | 8 | ** | * | ** | Hypoxia during birth and birth by cesarean section were found to be associated with MIH. |
| Barbosa T. et al., 2017 [22] Brazil | Cross-sectional | 167 | 29.3 | *** | * | * | There was a genetic influence on the occurrence of MIH; preterm birth was not related to MIH. |
| Andrade NS. et al., 2017 [48] Brazil | Case– control | 99 | 45.5 | *** | ** | ** | The prevalence of MIH and dental caries was increased in children and adolescents infected with HIV. |
| Gurrusquieta BJ. et al., 2017 [23] Mexico | Cross-sectional | 1156 | 182 | *** | * | ** | MIH was found to be associated with low weight, urinary tract infections, and allergies in the first years of life. |
| Rai A, et al., 2018 [24] India | Cross-sectional | 992 | 21.4 | *** | * | ** | Vitamin D deficiency, diabetes, or hypertension in pregnancy; prematurity or complications during delivery; and infections in the early years were found to be associated with MIH. |
| Koruyucu M. et al., 2018 [25] Turkey | Cross-sectional | 1511 | 14.2 | *** | * | ** | MIH was found to be associated with birth prematurity, diarrhea frequency, digestive system diseases, renal failure, rubeola, and chickenpox in the early years of life. |
| Van der Tas JT. et al., 2018 [43] Netherlands | Cohort | 3406 | 8.1 | **** | ** | *** | There was no association with calcium concentrations in the prenatal or postnatal stages. |
| Giuca M. et al., 2018 [26] Italy | Cross-sectional | 120 | 50 | ** | * | ** | Many infections (ear, throat, and nose) and the ingestion of antibiotics in the first years of life were riskfactors for MIH. |
| Dantas-Neta NB et al., 2018 [49] Brazil | Case– control | 744 | 19.5 | *** | ** | * | MIH was found to be associated with the presence of fever during gestation. |
| Portella PD. et al., 2018 [50] Brazil | Case–control | 93 | - | ** | * | ** | MIH was associated with prematurity and prolonged delivery. In addition, in the postnatal period, recurrent fevers in the first 3 years of life were associated with MIH. |
| Kılınç G. et al., 2019 [27] Turkey | Cross-sectional | 1237 | 11.5 | *** | * | ** | Preterm delivery, bronchitis, asthma, and high fever in early childhood were found to be associated with MIH. |
| Ardini Y. et al., 2019 [51] Malaysia | Case– control | 156 | 14.3 | ** | * | ** | Childhood illness, but not with perinatal complications or prolonged antibiotics consumption, was associated with MIH. |
| Mejía JD. et al., 2019 [28] Colombia | Cross-sectional | 1075 | 11.2 | ** | * | ** | Alterations during the last gestational trimester, premature delivery, maternal illness or infection, and/or maternal hypocalcemia and respiratory diseases were associated with MIH. |
| Woegelius P. et al., 2020 [29] Denmark | Cross-sectional | 1837 | 29.5 | **** | ** | ** | There was no association between the use of inhaled asthma medication and MIH. |
| Flexeder C. et al., 2020 [44] Germany | Cohort | 750 | 37.5 | **** | * | ** | There was an association between asthma without medication and MIH. |
| Głódkowska N. et al., 2020 [30] Poland | Cross-sectional | 2275 | 9.32 | ** | ** | ** | Exposure to higher concentrations of air pollutants and respiratory illnesses were found to be associated with MIH. |
| Einohalli M. et al., 2020 [31] Irak | Cross-sectional | 520 | 24% | *** | * | * | Asthma (or bronchitis), hospitalization history, and fever (above 38.5 °C) were factors associated with MIH. |
| Lee DW. et al., 2020 [52] Korea | Case–control | 1191 | 50 | *** | ** | ** | Maternal smoking during pregnancy and pediatric respiratory infection (suffered in early childhood) could predict MIH. |
| Padmanabhan V. et al., 2021 [32] United Arab Emirates | Cross-sectional | 1200 | 21.6 | ** | ** | * | Early-childhood illnesses (adenoiditis, tonsillitis, and asthma) were factors associated with MIH. However, high fever was notsignificantly associated with perinatal variables. |
| Alhowaish L. et al., 2021 [33] Saudi Arabia | Cross-sectional | 893 | 40.5 | *** | * | ** | Newborn jaundice was a factor associated with MIH. |
| Elzein R. et al., 2021 [34] Lebanon | Cross-sectional | 659 | 26 | *** | * | ** | Otitis media, fever, antibiotics, and the consumption of canned foods and beverages in the early years could predict MIH. Medical problems during pregnancy and mother’s medication during feeding were not significantly associated. |
| Mohamed RN. et al., 2021 [35] Saudi Arabia. | Cross- sectional. | 400 | 24.5 | **** | * | *** | Children with a breastfeeding history >18 months had a greater risk of MIH. |
| Fonseca G. et al., 2021 [36] Brazil | Cross-sectional | 731 | 12.10 | *** | ** | ** | Prematurity, prolonged delivery, and recurrent fevers could predict MIH. |
| Mariam S. et al., 2022 [37] India | Cross-sectional | 3176 | 11.72 | **** | ** | ** | Maternal anemia, preterm and low-weight birth, neonatal problems, early-childhood illnesses, medication in the first years, and socioeconomic status were associated with MIH. |
| Verma S. et al., 2022 [38] India | Cross- sectional | 5585 | 7.6% | *** | ** | ** | Mother’s illness and the intake of medications during pregnancy and by infants in the initial 4 years of life were associated with MIH. |
| Almuallem Z. et al., 2022 [39] Saudi Arabia | Cross- sectional | 1562 | 15.2 | *** | * | ** | Childhood illness (ear infections, respiratory distress, and tonsillitis) during the first three years of life showed a strong positive association with MIH. |
| Acosta E. et al., 2022 [40] Spain | Cross-sectional | 79 | 54.43 | ** | * | ** | MIH was significantly associated with the administration of Haloperidol during delivery. Additionally, serious infections and antibiotics in the first years of life could predict MIH. |
| Ilczuk-Rypuła D. et al., 2022 [45] Poland | Cohort | 613 | 6.2 | *** | ** | * | Otitis in early childhood, atopic dermatitis, and preterm birth before 38 weeks of pregnancy were significantly associated with MIH. |
| Etiologies | N Study | N Participants | Chi2 | I2 | OR (95%IC) | p-Value |
|---|---|---|---|---|---|---|
| Prenatal | ||||||
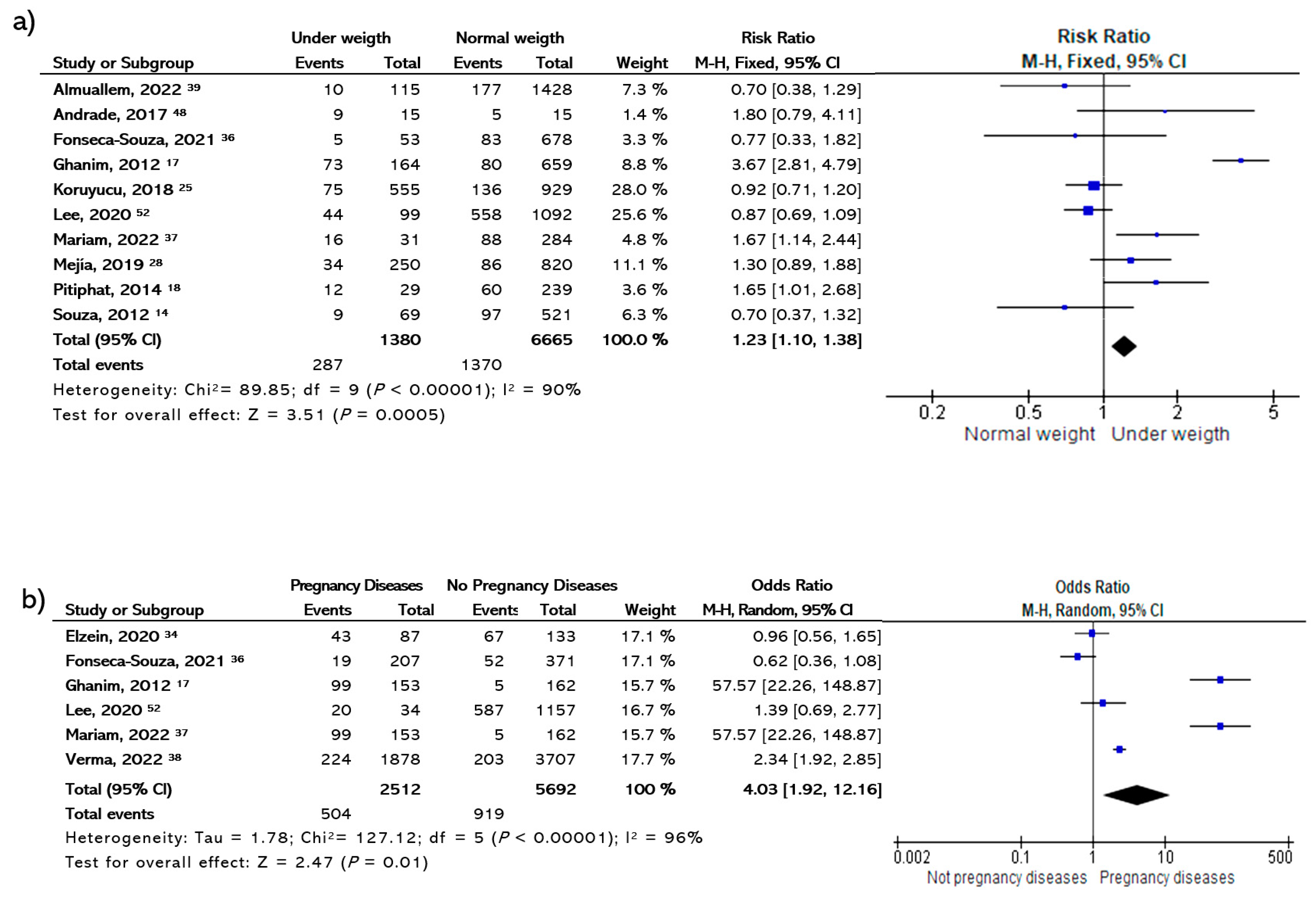
| Disease in pregnancy | 6 | 5692 | 127.12 | 96 | 4.03(1.33–12.16) | 0.01 * |
| Perinatal | ||||||
| Premature birth | 18 | 9355 | 62.16 | 77 | 1.26(0.99–1.59) | 0.06 |
| Low weight | 10 | 6665 | 89.85 | 90 | 1.23(1.10–1.38) | 0.0005 * |
| Cesarean section | 12 | 4017 | 43.06 | 77 | 0.77(0.59–1.00) | 0.05 |
| Postnatal | ||||||
| Respiratory diseases | 12 | 7455 | 249.5 | 96 | 1.51(0.79–2.37) | 0.21 |
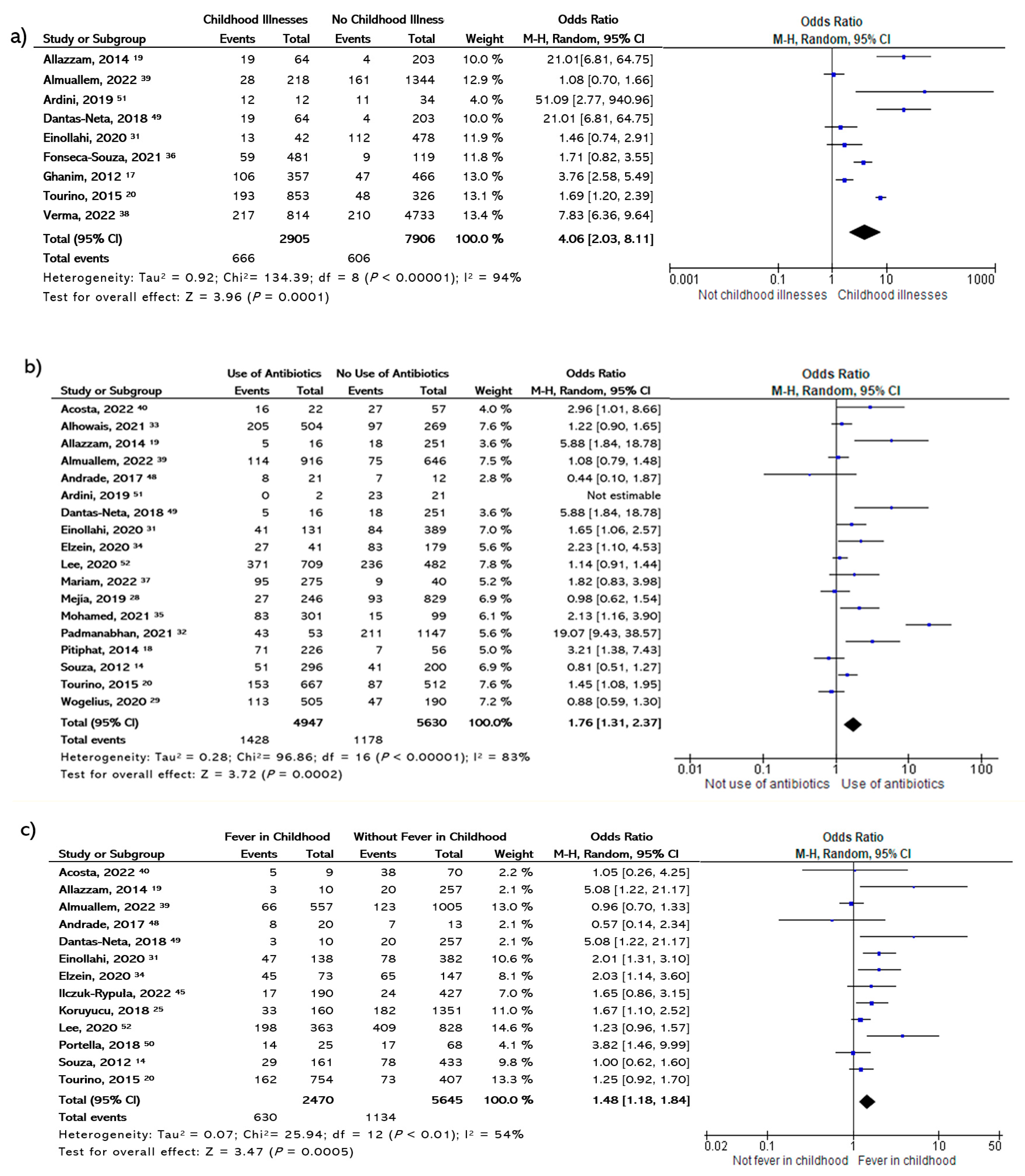
| Antibiotic consumption | 18 | 5630 | 96.86 | 83 | 1.76 (1.31–2.37) | 0.0002 * |
| General childhood illnesses | 9 | 7906 | 134.39 | 94 | 4.06(2.03–8.11) | 0.0001 * |
| High fever | 13 | 5645 | 25.94 | 54 | 1.48(1.18–1.84) | 0.0005 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juárez-López, M.L.A.; Salazar-Treto, L.V.; Hernández-Monjaraz, B.; Molina-Frechero, N. Etiological Factors of Molar Incisor Hypomineralization: A Systematic Review and Meta-Analysis. Dent. J. 2023, 11, 111. https://doi.org/10.3390/dj11050111
Juárez-López MLA, Salazar-Treto LV, Hernández-Monjaraz B, Molina-Frechero N. Etiological Factors of Molar Incisor Hypomineralization: A Systematic Review and Meta-Analysis. Dentistry Journal. 2023; 11(5):111. https://doi.org/10.3390/dj11050111
Chicago/Turabian StyleJuárez-López, María Lilia A., Leslie Vanessa Salazar-Treto, Beatriz Hernández-Monjaraz, and Nelly Molina-Frechero. 2023. "Etiological Factors of Molar Incisor Hypomineralization: A Systematic Review and Meta-Analysis" Dentistry Journal 11, no. 5: 111. https://doi.org/10.3390/dj11050111