
Efficacy of Periodontal Endoscopy during Subgingival Debridement to Treat Periodontitis: A Systematic Review of Randomized Clinical Trials



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Record
2.2. Studies Qualification
2.3. Selection Criteria
2.4. Search Strategy
2.5. Review Process
2.6. Data Collection
2.7. Quality Evaluation
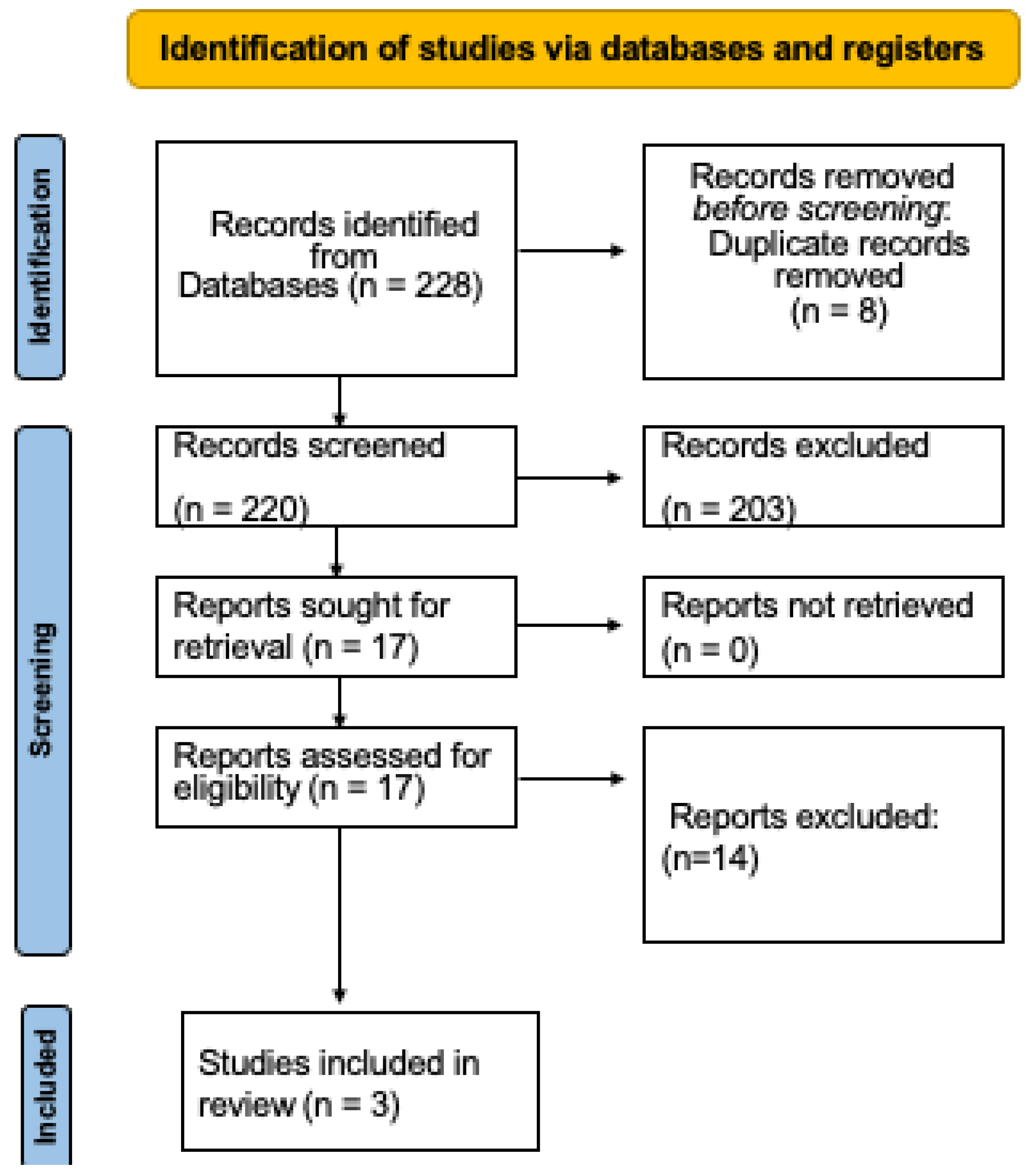
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pretzl, B.; Sälzer, S.; Ehmke, B.; Schlagenhauf, U.; Dannewitz, B.; Dommisch, H.; Eickholz, P.; Jockel-Schneider, Y. Administration of systemic antibiotics during non-surgical periodontal therapy-a consensus report. Clin. Oral Investig. 2019, 23, 3073–3085. [Google Scholar] [CrossRef] [PubMed]
- Ardila, C.M.; Vivares-Builes, A.M. Clinical Efficacy of Treatment of Endodontic-Periodontal Lesions: A Systematic Scoping Review of Experimental Studies. Int. J. Environ. Res. Public Health 2022, 19, 13649. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- West, N.; Chapple, I.; Claydon, N.; D’Aiuto, F.; Donos, N.; Ide, M.; Needleman, I.; Kebschull, M.; British Society of Periodontology and Implant Dentistry Guideline Group Participants. BSP implementation of European S3—Level evidence-based treatment guidelines for stage I-III periodontitis in UK clinical practice. J. Dent. 2021, 106, 103562. [Google Scholar] [CrossRef]
- Rams, T.E.; Manos, M.P. Comparative In Vitro Evaluation of WHO Periodontal Probe and #11/12 Dental Explorer for Subgingival Calculus Detection. J. Contemp. Dent. Pract. 2021, 22, 13–17. [Google Scholar]
- Naicker, M.; Ngo, L.H.; Rosenberg, A.J.; Darby, I.B. The effectiveness of using the perioscope as an adjunct to non-surgical periodontal therapy: Clinical and radiographic results. J. Periodontol. 2022, 93, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Kalsi, A.S.; Bomfim, D.I.; Hussain, Z. Factors affecting decision making at reassessment of periodontitis. Part 4: Treatment options for residual periodontal pockets. Br. Dent. J. 2019, 227, 967–974. [Google Scholar] [CrossRef]
- Wang, C.Y.; Yang, Y.H.; Li, H.; Lin, P.Y.; Su, Y.T.; Kuo, M.Y.; Tu, Y.K. Adjunctive local treatments for patients with residual pockets during supportive periodontal care: A systematic review and network meta-analysis. J. Clin. Periodontol. 2020, 47, 1496–1510. [Google Scholar] [CrossRef]
- Ardila, C.M.; Bedoya-García, J.A.; Arrubla-Escobar, D.E. Antibiotic resistance in periodontitis patients: A systematic scoping review of randomized clinical trials. Oral Dis. 2022. [CrossRef]
- Ardila, C.M.; Bedoya-García, J.A. Clinical and Microbiological Efficacy of Adjunctive Systemic Quinolones to Mechanical Therapy in Periodontitis: A Systematic Review of the Literature. Int. J. Dent. 2022, 2022, 4334269. [Google Scholar] [CrossRef]
- Krajewski, A.; Perussolo, J.; Gkranias, N.; Donos, N. Influence of periodontal surgery on the subgingival microbiome-A systematic review and meta-analysis. J. Periodontal Res. 2023, 58, 308–324. [Google Scholar] [CrossRef] [PubMed]
- Estrin, N.E.; Moraschini, V.; Zhang, Y.; Romanos, G.E.; Sculean, A.; Miron, R.J. Combination of Nd:YAG and Er:YAG lasers in non-surgical periodontal therapy: A systematic review of randomized clinical studies. Lasers Med. Sci. 2022, 37, 2737–2743. [Google Scholar] [CrossRef]
- Kuang, Y.; Hu, B.; Chen, J.; Feng, G.; Song, J. Effects of periodontal endoscopy on the treatment of periodontitis: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2017, 148, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Geisinger, M.L.; Mealey, B.L.; Schoolfield, J.; Mellonig, J.T. The effectiveness of subgingival scaling and root planing: An evaluation of therapy with and without the use of the periodontal endoscope. J. Periodontol. 2007, 78, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Graetz, C.; Schorr, S.; Christofzik, D.; Dörfer, C.E.; Sälzer, S. How to train periodontal endoscopy? Results of a pilot study removing simulated hard deposits in vitro. Clin. Oral Investig. 2020, 24, 607–617. [Google Scholar] [CrossRef]
- Wilson, T.G.; Harrel, S.K.; Nunn, M.E.; Francis, B.; Webb, K. The relationship between the presence of tooth-borne subgingival deposits and inflammation found with a dental endoscope. J. Periodontol. 2008, 79, 2029–2035. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Blue, C.M.; Lenton, P.; Lunos, S.; Poppe, K.; Osborn, J. A pilot study comparing the outcome of scaling/root planing with and without Perioscope™ technology. J. Dent. Hyg. JDH 2013, 87, 152–157. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Wu, J.; Lin, L.; Xiao, J.; Zhao, J.; Wang, N.; Zhao, X.; Tan, B. Efficacy of scaling and root planning with periodontal endoscopy for residual pockets in the treatment of chronic periodontitis: A randomized controlled clinical trial. Clin. Oral Investig. 2022, 26, 513–521. [Google Scholar] [CrossRef]
- Zhang, Y.H.; Li, H.X.; Yan, F.H.; Tan, B.C. Clinical effects of scaling and root planing with an adjunctive periodontal endoscope for residual pockets: A randomized controlled clinical study. West China J. Stomatol. 2020, 38, 532–536. [Google Scholar]
- Fardal, Ø.; Johannessen, A.C.; Linden, G.J. Tooth loss during maintenance following periodontal treatment in a periodontal practice in Norway. J. Clin. Periodontol. 2004, 31, 550–555. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Trombelli, L.; Heitz, F.; Needleman, I.; Moles, D. A systematic review of the effect of surgical debridement vs non-surgical debridement for the treatment of chronic periodontitis. J. Clin. Periodontol. 2002, 29 (Suppl. 3), 92–162. [Google Scholar] [CrossRef]
- Stambaugh, R.V. A clinician’s 3-year experience with perioscopy. Compend. Contin. Educ. Dent. 2002, 23, 1061–1070. [Google Scholar] [PubMed]
- Avradopoulos, V.; Wilder, R.S.; Chichester, S.; Offenbacher, S. Clinical and inflammatory evaluation of Perioscopy on patients with chronic periodontitis. J. Dent. Hyg. JDH 2004, 78, 30–38. [Google Scholar] [PubMed]
- Liao, Y.T.; Liu, Y.; Jiang, Y.; Ouyang, X.Y.; He, L.; An, N. A clinical evaluation of periodontal treatment effect using periodontal endoscope for patients with periodontitis: A split-mouth controlled study. Chin. J. Stomatol. 2016, 51, 722–727. [Google Scholar]
- Kwan, J.; Workman, P. Micro ultrasonic endoscopic periodontal debridement: Retrospective analysis of treatment with at least 1 year follow-up. J. Periodontol. 2009, 80, 1901–1904. [Google Scholar]
- Povšič, K.; Čuk, K.; Milavec, S.; Erčulj, V.; Seme, K.; Gašperšič, R. Systemic azithromycin as an adjunct to scaling and root planing in patients with stage III/IV periodontitis: 12-month results of a randomized controlled clinical trial. Clin. Oral Investig. 2021, 25, 5997–6006. [Google Scholar] [CrossRef]
- Preus, H.R.; Gjermo, P.; Baelum, V. A double-masked Randomized Clinical Trial (RCT) comparing four periodontitis treatment strategies: 5-year clinical results. J. Clin. Periodontol. 2017, 44, 1029–1038. [Google Scholar] [CrossRef]
- Checchi, L.; Montevecchi, M.; Checchi, V.; Zappulla, F. The relationship between bleeding on probing and subgingival deposits. An endoscopical evaluation. Open Dent. J. 2009, 3, 154–160. [Google Scholar] [PubMed]
- Nibali, L.; Pometti, D.; Tu, Y.K.; Donos, N. Clinical and radiographic outcomes following non-surgical therapy of periodontal infrabony defects: A retrospective study. J. Clin. Periodontol. 2011, 38, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y. Comparison of the effects of periodontal scaling under the periodontal endoscope and traditional periodontal scaling on periodontitis. Chin. J. Pract. Med. 2016, 43, 68–70. [Google Scholar]
- Ardila, C.M.; Vivares-Builes, A.M. Antibiotic Resistance in Patients with Peri-Implantitis: A Systematic Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 15609. [Google Scholar] [CrossRef] [PubMed]
- Ardila, C.M.; Bedoya-García, J.A.; González-Arroyave, D. Antimicrobial resistance in patients with endodontic infections: A systematic scoping review of observational studies. Aust. Endod. J. 2022. [CrossRef] [PubMed]


{kind=link}
| Authors Publication Date | Periodontal Diagnoses | Patients | Mean AGE | Female Male | Intervention Control | Main and Secondary Outcomes | Follow-Up |
|---|---|---|---|---|---|---|---|
| Naicker et al. 2022 [6] | Moderate to Severe Chronic Periodontitis | 38 | 52 years | 24/14 | Root surface debridement with perioscope (Test group) or root surface debridement only (Control group). | At 12 months, the test group had a significantly more reduced probing depth (Test group: 2.70 + 0.2 mm; Control group: 2.98 ± 0.4 mm). The test group presented a significantly lower % of probing depth 7 to 9 mm at three (0.72 ± 1.2%) and 12 months (0.5 ± 1.0%) as compared with the control group (2.25 ± 2.9%; 1.84 ± 2.3%) (p = 0.03). No differences were detected in the clinical attachment level. At 12 months, the test group had a significantly inferior mean bleeding on probing (Test group: 4.3 ± 3.2%; Control group: 11.95 ± 7.1%). | 12 months |
| Wu et al. 2022 [20] | Moderate to Severe Chronic Periodontitis | 37 | 37 years | 22/15 | Scaling and root planing plus periodontal endoscopy (Test group) or scaling and root planing alone (control group). | More significant reduction in probing depth were presented in the test group at the 6-month follow-up (3.12 ± 0.63 vs. 4.0 ± 0.68 mm; p = 0.001). No significant differences in clinical attachment level or bleeding on probing were perceived. | 6 months |
| Zhang et al. 2020 [21] | Chronic periodontitis | 38 | 36 years | 24/14 | Scaling and root planing plus periodontal endoscopy (Test group) or scaling and root planing alone (control group). | Compared with those in the scaling and root planing group, probing depth at 3 and 6 months after therapy, and clinical attachment level and bleeding on probing at 6 months after treatment were reduced in the endoscope group (p < 0.05). | 6 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardila, C.M.; Vivares-Builes, A.M. Efficacy of Periodontal Endoscopy during Subgingival Debridement to Treat Periodontitis: A Systematic Review of Randomized Clinical Trials. Dent. J. 2023, 11, 112. https://doi.org/10.3390/dj11050112
Ardila CM, Vivares-Builes AM. Efficacy of Periodontal Endoscopy during Subgingival Debridement to Treat Periodontitis: A Systematic Review of Randomized Clinical Trials. Dentistry Journal. 2023; 11(5):112. https://doi.org/10.3390/dj11050112
Chicago/Turabian StyleArdila, Carlos M., and Annie Marcela Vivares-Builes. 2023. "Efficacy of Periodontal Endoscopy during Subgingival Debridement to Treat Periodontitis: A Systematic Review of Randomized Clinical Trials" Dentistry Journal 11, no. 5: 112. https://doi.org/10.3390/dj11050112