

Association between the Risk of Preterm Birth and Low Birth Weight with Periodontal Disease in Pregnant Women: An Umbrella Review

 , ,
, ,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
- Population: pregnant women with PB and LBW;
- Intervention: pregnant women with PD;
- Comparison: pregnant woman without PD;
- Outcomes: association between PD and PB (<37 weeks) and LBW (<2500 gm) of the newborn.
2.2. Focused Question (PICO)
2.3. Search and Selection of Studies
2.4. Data Extraction
2.5. Risk of Bias (RoB) Assessment
2.6. Analysis of Results
3. Results
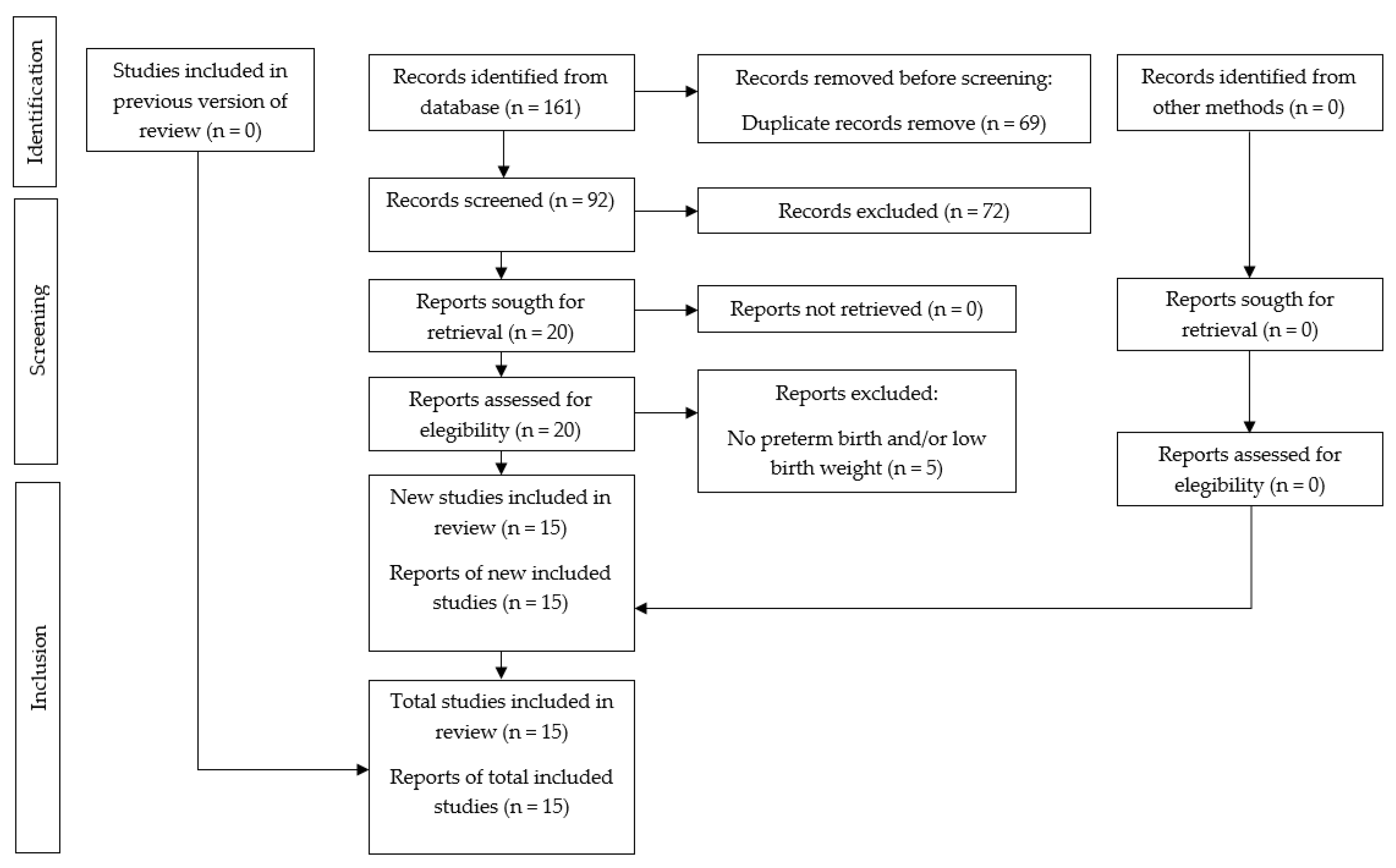
3.1. Selection of Studies
3.2. Characteristics of the Included Studies
3.3. Risk of Bias in the Analysis of the Studies
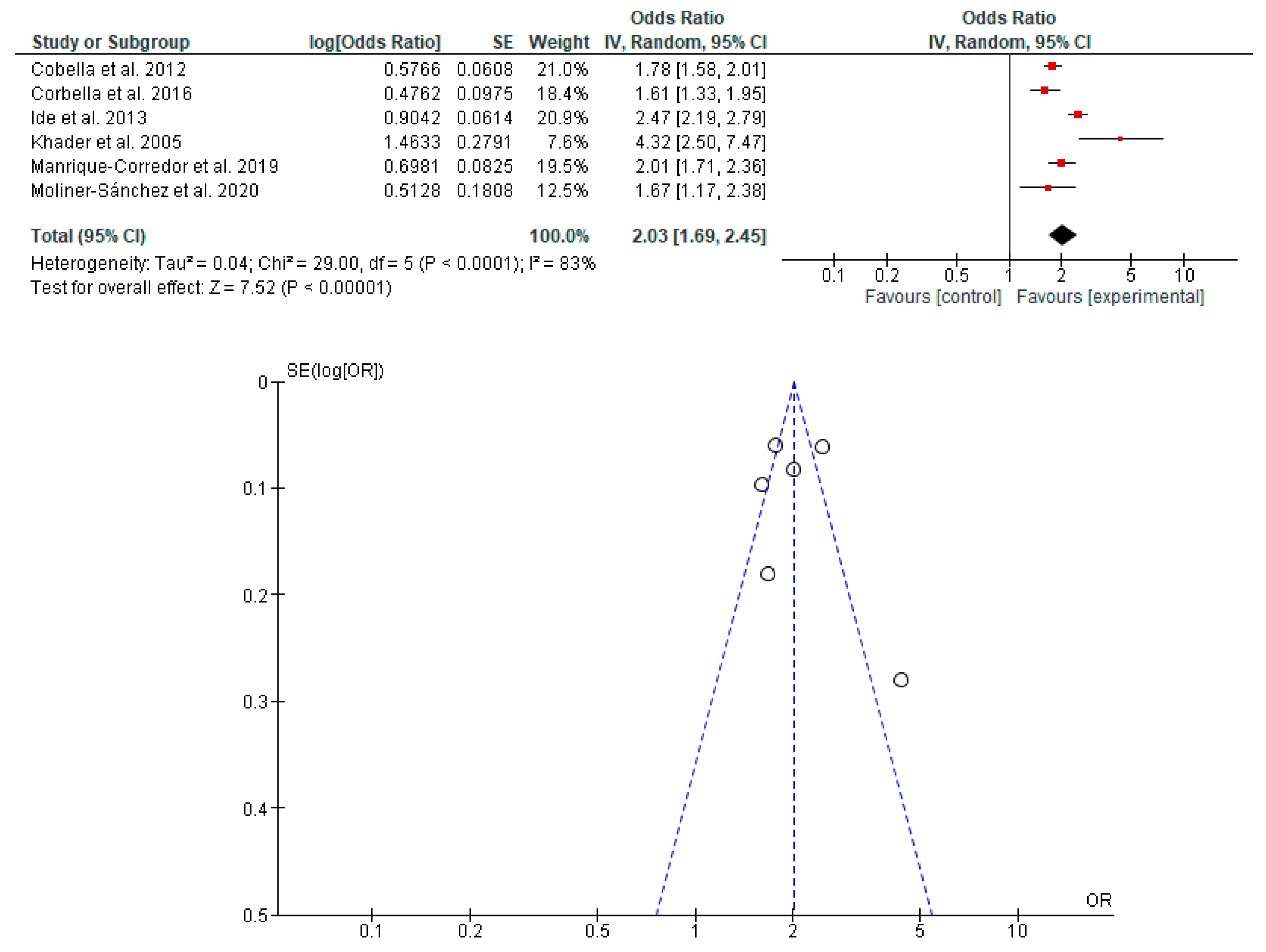
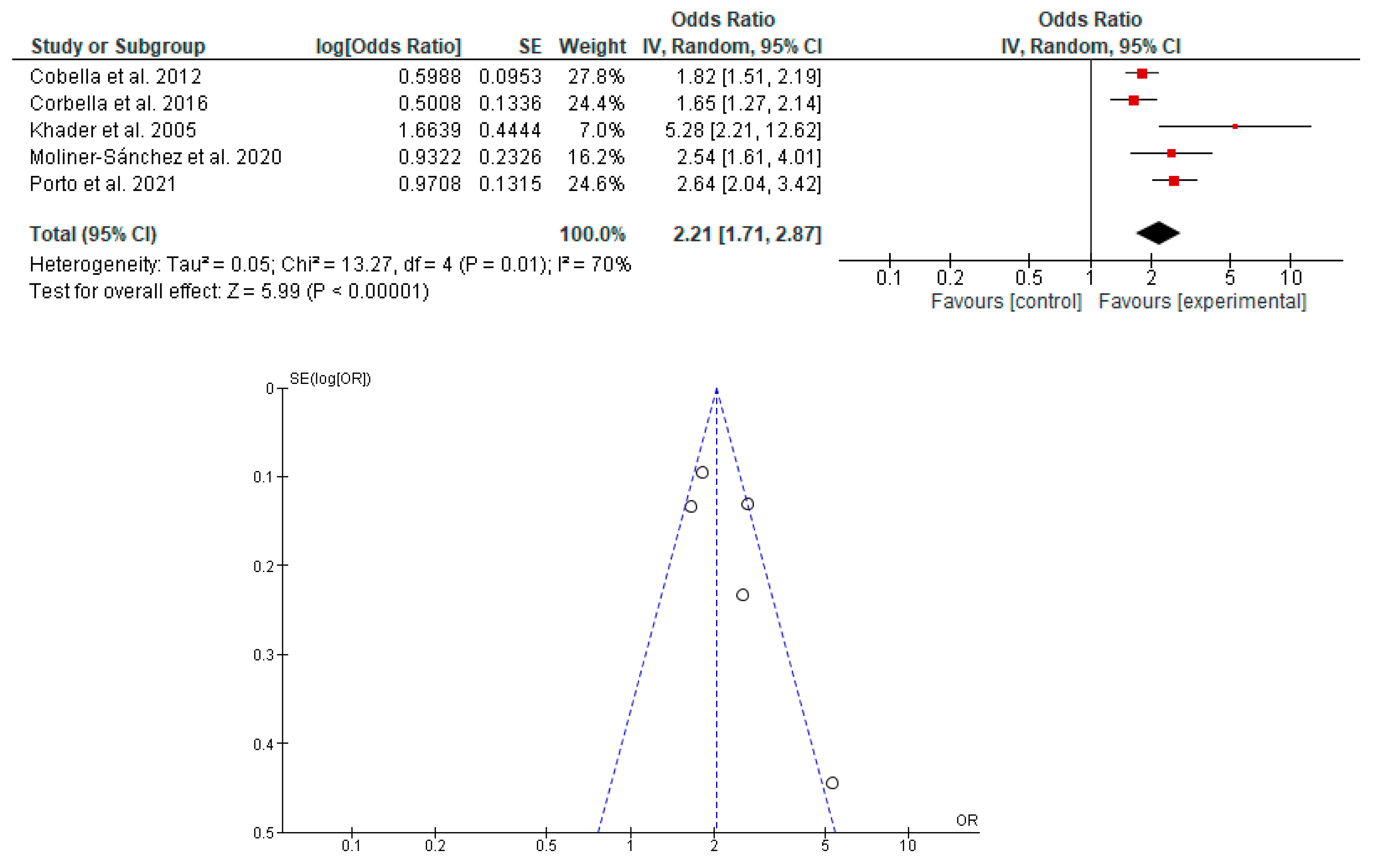
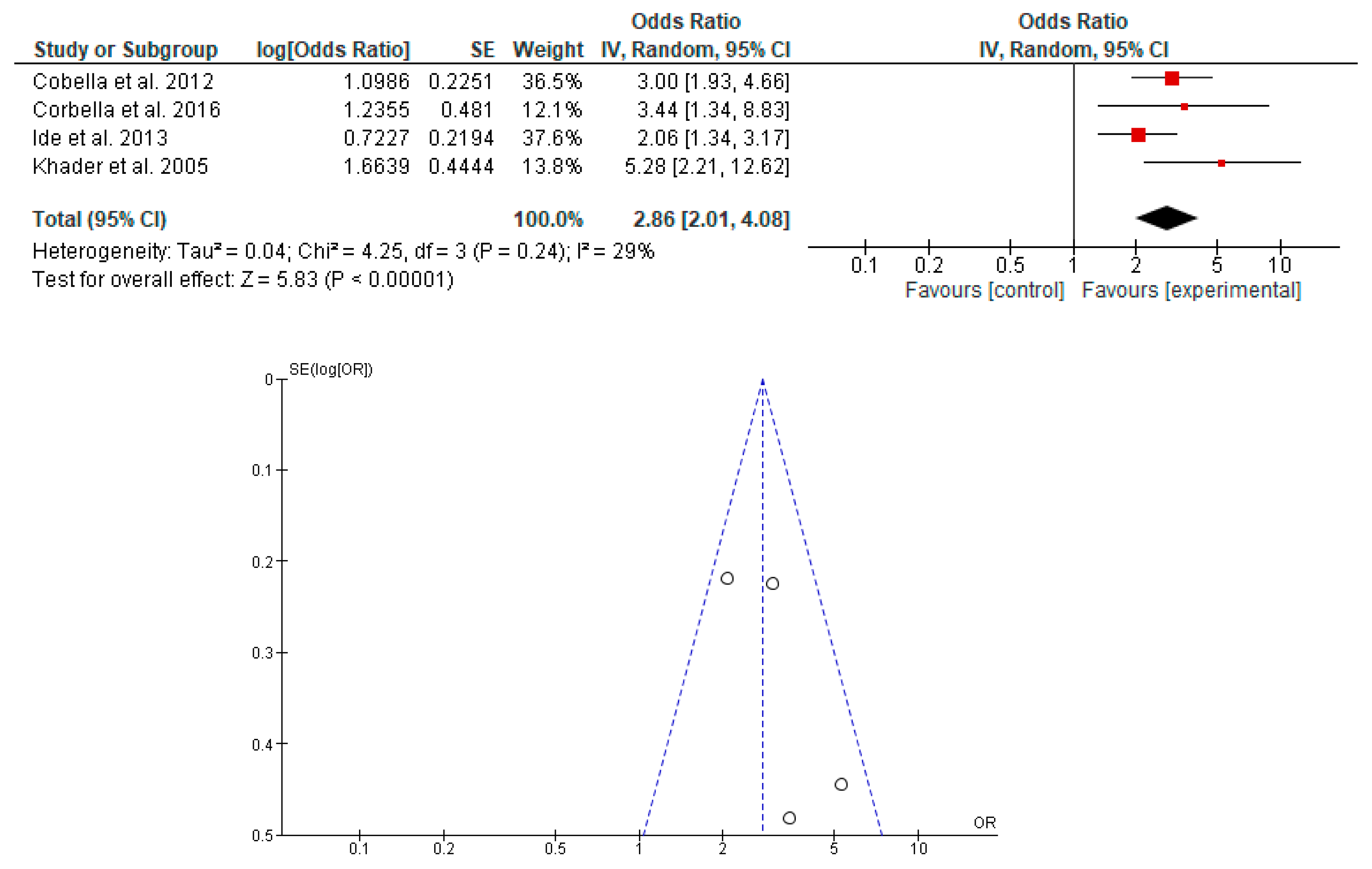
3.4. Synthesis of the Results
3.5. GRADE Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, J.G.; Nakaishi, L.A. Managing the Complexity of a Dynamic Biofilm. J. Am. Dent. Assoc. 2006, 137, S10–S15. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal Diseases. Nat. Rev. Dis. Prim. 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic Periodontitis, Inflammatory Cytokines, and Interrelationship with Other Chronic Diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, T.E.; Bartold, P.M.; Reynolds, E.C. The Nexus Between Periodontal Inflammation and Dysbiosis. Front. Immunol. 2020, 11, 511. [Google Scholar] [CrossRef]
- Kurgan, S.; Kantarci, A. Molecular Basis for Immunohistochemical and Inflammatory Changes during Progression of Gingivitis to Periodontitis. Periodontology 2000 2018, 76, 51–67. [Google Scholar] [CrossRef]
- Reynolds, I.; Duane, B. Periodontal Disease Has an Impact on Patients’ Quality of Life. Evid.-Based Dent. 2018, 19, 14–15. [Google Scholar] [CrossRef]
- Kane, S.F. The Effects of Oral Health on Systemic Health. Gen. Dent. 2017, 65, 30–34. [Google Scholar]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef]
- Nazir, M.A. Prevalence of Periodontal Disease, Its Association with Systemic Diseases and Prevention. Int. J. Health Sci. 2017, 1, 72–80. [Google Scholar] [CrossRef]
- Salih, Y.; Nasr, A.M.; Ahmed, A.B.A.; Sharif, M.E.; Adam, I. Prevalence of and Risk Factors for Periodontal Disease among Pregnant Women in an Antenatal Care Clinic in Khartoum, Sudan. BMC Res. Notes 2020, 13, 147. [Google Scholar] [CrossRef]
- Tettamanti, L.; Lauritano, D.; Nardone, M.; Gargari, M.; Silvestre-Rangil, J.; Gavoglio, P.; Tagliabue, A. Pregnancy and Periodontal Disease: Does Exist a Two-Way Relationship? ORAL Implantol. 2017, 10, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Andonova, I.; Iliev, V.; Živković, N.; Sušič, E.; Bego, I.; Kotevska, V. Can Oral Anaerobic Bacteria Cause Adverse Pregnancy Outcomes? Pril. (Makedon. Akad. Nauk. Umetnostite. Oddel. Med. Nauk.) 2015, 36, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Zi, M.Y.H.; Longo, P.L.; Bueno-Silva, B.; Mayer, M.P.A. Mechanisms Involved in the Association between Periodontitis and Complications in Pregnancy. Front. Public Health 2015, 2, 290. [Google Scholar] [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm Labor: One Syndrome, Many Causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Madianos, P.N.; Bobetsis, Y.A.; Offenbacher, S. Adverse Pregnancy Outcomes (APOs) and Periodontal Disease: Pathogenic Mechanisms. J. Clin. Periodontol. 2013, 40, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhou, J.; Ma, Y.; Liu, L.; Xia, Q.; Fan, D.; Ai, W. Mode of Delivery and Preterm Birth in Subsequent Births: A Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0213784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muchie, K.F.; Lakew, A.M.; Teshome, D.F.; Yenit, M.K.; Sisay, M.M.; Mekonnen, F.A.; Habitu, Y.A. Epidemiology of Preterm Birth in Ethiopia: Systematic Review and Meta-Analysis. BMC Pregnancy Childbirth 2020, 20, 574. [Google Scholar] [CrossRef]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, Regional, and National Estimates of Levels of Preterm Birth in 2014: A Systematic Review and Modelling Analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Moliner-Sánchez, C.A.; Iranzo-Cortés, J.E.; Almerich-Silla, J.M.; Bellot-Arcís, C.; Ortolá-Siscar, J.C.; Montiel-Company, J.M.; Almerich-Torres, T. Effect of per Capita Income on the Relationship between Periodontal Disease during Pregnancy and the Risk of Preterm Birth and Low Birth Weight Newborn. Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8015. [Google Scholar] [CrossRef]
- Manrique-Corredor, E.; Orozco-Beltran, D.; Lopez-Pineda, A.; Quesada, J.; Gil-Guillen, V.; Carratala-Munuera, C. Maternal Periodontitis and Preterm Birth: Systematic Review and Meta-Analysis. Community Dent. Oral Epidemiol. 2019, 47, 243–251. [Google Scholar] [CrossRef]
- Syafar, I.F.; Tahir, H.; Oktawati, S. The Correlations between Periodontal Disease in the Woman with Pregnancy and Low Birth Weight Infant: A Systematic Review. Makassar Dent. J. 2019, 8, 178–184. [Google Scholar] [CrossRef]
- Teshome, A.; Yitayeh, A. Relationship between Periodontal Disease and Preterm Low Birth Weight: Systematic Review. Pan Afr. Med. J. 2016, 24, 215. [Google Scholar] [CrossRef]
- Corbella, S.; Taschieri, S.; Francetti, L.; De Siena, F.; Del Fabbro, M. Periodontal Disease as a Risk Factor for Adverse Pregnancy Outcomes: A Systematic Review and Meta-Analysis of Case-Control Studies. Odontology 2012, 100, 232–240. [Google Scholar] [CrossRef]
- Xiong, X.; Buekens, P.; Fraser, W.D.; Beck, J.; Offenbacher, S. Periodontal Disease and Adverse Pregnancy Outcomes: A Systematic Review. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 135–143. [Google Scholar] [CrossRef]
- Vettore, M.V.; Lamarca, G.d.A.; Leão, A.T.T.; Thomaz, F.B.; Sheiham, A.; Leal, M.d.C. Periodontal Infection and Adverse Pregnancy Outcomes: A Systematic Review of Epidemiological Studies. Cad. Saude Publica 2006, 22, 2041–2053. [Google Scholar] [CrossRef] [Green Version]
- Komine-Aizawa, S.; Aizawa, S.; Hayakawa, S. Periodontal Diseases and Adverse Pregnancy Outcomes. J. Obstet. Gynaecol. Res. 2019, 45, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Falcao, A.; Bullón, P. A Review of the Influence of Periodontal Treatment in Systemic Diseases. Periodontology 2000 2019, 79, 117–128. [Google Scholar] [CrossRef]
- Offenbacher, S.; Katz, V.; Fertik, G.; Collins, J.; Boyd, D.; Maynor, G.; McKaig, R.; Beck, J. Periodontal Infection as a Possible Risk Factor for Preterm Low Birth Weight. J. Periodontol. 1996, 67, 1103–1113. [Google Scholar] [CrossRef] [PubMed]
- Daalderop, L.A.; Wieland, B.V.; Tomsin, K.; Reyes, L.; Kramer, B.W.; Vanterpool, S.F.; Been, J.V. Periodontal Disease and Pregnancy Outcomes: Overview of Systematic Reviews. JDR Clin. Transl. Res. 2018, 3, 10–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pockpa, Z.A.D.; Soueidan, A.; Koffi-Coulibaly, N.T.; Limam, A.; Badran, Z.; Struillou, X. Periodontal Diseases and Adverse Pregnancy Outcomes: Review of Two Decades of Clinical Research. Oral Health Prev. Dent. 2021, 19, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bashir, S.; Menon, I.; Gupta, R.; Sharma, A.; Arora, V.; Varshney, S. Dental Considerations in Pregnancy—A Systematic Review. J. Pharm. Res. Int. 2021, 33, 82–100. [Google Scholar] [CrossRef]
- Gharehghani, M.; Bayani, A.; Bayat, A.; Hemmat, M.; Karimy, M.; Ahounbar, E.; Armoon, B.; Fakhri, Y.; Schroth, R. Poor Oral Health-Related Quality of Life among Pregnant Women: A Systematic Review and Meta-Analysis. Int. J. Dent. Hyg. 2021, 19, 39–49. [Google Scholar] [CrossRef]
- Konopka, T.; Zakrzewska, A. Periodontitis and Risk for Preeclampsia—A Systematic Review. Ginekol. Pol. 2020, 91, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Abariga, S.; Whitcomb, B. Periodontitis and Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Observational Studies. BMC Pregnancy Childbirth 2016, 16, 344. [Google Scholar] [CrossRef] [Green Version]
- Kunnen, A.; van Doormaal, J.; Abbas, F.; Aarnoudse, J.; van Pampus, M.; Faas, M. Periodontal Disease and Pre-Eclampsia: A Systematic Review. J. Clin. Periodontol. 2010, 37, 1075–1087. [Google Scholar] [CrossRef]
- Porto, E.; Gomes, I.; Batista, J.; Lyrio, A.; Souza, E.; Figueiredo, A.; Pereira, M.; da Cruz, S. Maternal periodontitis and low birth weight: Systematic review and meta-analysis. Cienc. Saude Coletiva 2021, 26, 5383–5392. [Google Scholar] [CrossRef]
- Corbella, S.; Taschieri, S.; Del Fabbro, M.; Francetti, L.; Weinstein, R.; Ferrazzi, E. Adverse Pregnancy Outcomes and Periodontitis: A Systematic Review and Meta-Analysis Exploring Potential Association. Quintessence Int. 2016, 47, 193–204. [Google Scholar] [CrossRef]
- Ide, M.; Papapanou, P.N. Epidemiology of Association between Maternal Periodontal Disease and Adverse Pregnancy Outcomes-Systematic Review. J. Clin. Periodontol. 2013, 40, S181–S194. [Google Scholar] [CrossRef]
- Xiong, X.; Buekens, P.; Vastardis, S.; Yu, S.M. Periodontal Disease and Pregnancy Outcomes: State-of-the-Science. Obstet. Gynecol. Surv. 2007, 62, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Khader, Y.S.; Ta’ani, Q. Periodontal Diseases and the Risk of Preterm Birth and Low Birth Weight: A Meta-Analysis. J. Periodontol. 2005, 76, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Scannapieco, F.A.; Bush, R.B.; Paju, S. Periodontal Disease as a Risk Factor for Adverse Pregnancy Outcomes. A Systematic Review. Ann. Periodontol. 2003, 8, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Madianos, P.N.; Bobetsis, G.A.; Kinane, D.F. Is Periodontitis Associated with an Increased Risk of Coronary Heart Disease and Preterm and/or Low Birth Weight Births? J. Clin. Periodontol. 2002, 29, 22–36. [Google Scholar] [CrossRef]
- Corbella, S.; Del Fabbro, M.; Taschieri, S.; Francetti, L. Periodontal Disease and Adverse Pregnancy Outcomes: A Systematic Review. Ital. Oral Surg. 2012, 11, 132–146. [Google Scholar] [CrossRef]
- Natto, Z.S.; Hameedaldain, A. Methodological Quality Assessment of Meta-Analyses and Systematic Reviews of the Relationship Between Periodontal and Systemic Diseases. J. Evid. Based Dent. Pract. 2019, 19, 131–139. [Google Scholar] [CrossRef]
- Chugh, A.; Patnana, A.K.; Kumar, P.; Chugh, V.K.; Khera, D.; Singh, S. Critical Analysis of Methodological Quality of Systematic Reviews and Meta-Analysis of Antibiotics in Third Molar Surgeries Using AMSTAR 2. J. Oral Biol. Craniofacial Res. 2020, 10, 441–449. [Google Scholar] [CrossRef]
- Radochova, V.; Stepan, M.; Kacerovska Musilova, I.; Slezak, R.; Vescicik, P.; Menon, R.; Jacobsson, B.; Kacerovsky, M. Association between Periodontal Disease and Preterm Prelabour Rupture of Membranes. J. Clin. Periodontol. 2019, 46, 189–196. [Google Scholar] [CrossRef]
- Luna, M.C.; Cubides Munevar, A.M.; Ruiz Melo, C.F.; Alonso, S.V.; Pinzón, E.M.; Gullozo, L.; Luna, M.C.; Cubides Munevar, A.M.; Ruiz Melo, C.F.; Alonso, S.V.; et al. Asociación Entre Bajo Peso al Nacer y Parto Pretermino En Gestantes Con Signos de Enfermedad Periodontal Atendidas En Una Institución Del Nivel Primario de Salud Del Valle Del Cauca-Colombia. Rev. Chil. Obstet. Ginecol. 2019, 84, 103–111. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Nutrition Targets 2025: Low Birth Weight Policy Brief. Available online: https://www.who.int/publications-detail-redirect/WHO-NMH-NHD-14.5 (accessed on 3 January 2022).
- World Health Organization. Nacimientos Prematuros. Available online: https://www.who.int/es/news-room/fact-sheets/detail/preterm-birth (accessed on 3 January 2022).
- Maspero, C.; Fama, A.; Giannini, L.; Galbiati, G.; Batia, S.; Farronato, M. Preventive Hygiene Protocol of University of Milan for Women during Pregnancy: A Qualitative and Quantitative Bacterial Plaque Analysis Prospective Original Study. Saudi Dent. J. 2020, 32, 29–35. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Strategy |
|---|---|
| PubMed/Medline | (((“periodontal disease treatment”) OR periodontitis) OR gingivitis) AND (((((“preterm birth”) OR “low birth weight”) OR “perinatal outcomes”) OR “premature labor”) OR “adverse pregnancy outcomes”) |
| Cochrane Library | #1 MeSH descriptor: [Periodontal Diseases] explode all trees #2 MeSH descriptor: [Periodontitis] explode all trees #3 MeSH descriptor: [Gingivitis] explode all trees #4 (periodontal disease treatment) OR (periodontitis) OR (gingivitis) (Word variations have been searched) #5 #1 OR #2 OR #3 OR #4 #6 MeSH descriptor: [Premature Birth] explode all trees #7 MeSH descriptor: [Infant, Low Birth Weight] explode all trees #8 MeSH descriptor: [Obstetric Labor, Premature] explode all trees #9 (preterm birth) OR (low birth weight) OR (perinatal outcomes) OR (premature labor) OR (adverse pregnancy outcomes) (Word variations have been searched) #10 #6 OR #7 OR #8 OR #9 #11 #5 AND #10 |
| Scopus | TITLE-ABS-KEY (((“periodontal disease treatment”) OR periodontitis) OR gingivitis) AND TITLE-ABS-KEY (((((“preterm birth”) OR “low birth weight”) OR “perinatal outcomes”) OR “premature labor”) OR “adverse pregnancy outcomes”) AND TITLE-ABS-KEY (“systematic review”) AND (LIMIT-TO (SUBJAREA, “DENT”)) AND (LIMIT-TO (DOCTYPE, “re”)) |
| Scielo | ((((“periodontal disease”) OR (treatment) (periodontitis) OR (gingivitis))) AND (((“preterm birth”) OR (“low birth weight”) OR (“perinatal outcomes”) OR (“premature labor”) OR (“adverse pregnancy outcomes”)))) AND ((“systematic review”)) ((((“enfermedad periodontal”) OR (tratamiento) OR (periodontitis) OR (gingivitis))) AND (((“parto pretérmino”) OR (“bajo peso al nacer”) OR (“resultados perinatales”) OR (“resultados adversos al embarazo”)))) AND ((“revisión sistemática”)) |
| EMBASE | (‘periodontal disease treatment’:ti,ab,kw OR periodontitis:ti,ab,kw OR gingivitis:ti,ab,kw) AND (‘preterm birth’:ti,ab,kw OR ‘low birth weight’:ti,ab,kw OR ‘perinatal outcomes’:ti,ab,kw OR ‘premature labor’:ti,ab,kw OR ‘adverse pregnancy outcomes’:ti,ab,kw) AND ‘systematic review’:ti,ab,kw |
| Web of Science | ((TS = (((“periodontal disease treatment”) OR (periodontitis) OR (gingivitis)))) AND TS = (((“preterm birth”) OR (“low birth weight”) OR (“perinatal outcomes”) OR (“premature labor”) OR (“adverse pregnancy outcomes”)))) AND TS = ((“systematic review”)) |
| Google Scholar | allintitle: “periodontal disease treatment” “preterm birth” “systematic review” allintitle: “periodontitis” “preterm birth” “systematic review” allintitle: “periodontitis” “low birth weight” “systematic review” |
| Authors | Reason for Exclusion |
|---|---|
| Bashir et al. [33], Gharehghani et al. [34], Konopka et al. [35], Abariga et al. [36], Kunnen et al. [37] | Studies not referring to PB or LBW |
| Author | Year | Type of Study | Country | Type of Studies Included | Number of Studies Included in Qualitative Analysis | Number of Studies Included in Quantitative Analysis | Type of Periodontal Disease | Outcomes | OR/RR | Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|
| Porto et al. [38] | 2021 | SR with MA | Brazil | Cases and controls and cohorts | 21 | 21 | Periodontitis | LBW | 2.64 (2.04–3.42)/NR | Pregnant women with periodontitis may be more than twice as likely to have babies with PB. |
| Moliner-Sánchez et al. [19] | 2020 | SR with MA | Spain | Cohorts | 11 | 11 (11 PB and 6 LBW) | Periodontal disease | PB and LBW | NR/PB = 1.67 (1.17–2.38), LBW = 2.54 (1.61–3.98) | There is a relationship between PD and PB and LBW. |
| Manrique-Corredor et al. [20] | 2019 | SR with MA | Colombia | Cases and controls and cohorts | 31 | 20 | Periodontitis | PB | 2.01 (1.71–2.36)/NR | There is an association between periodontitis and PB. |
| Syafar et al. [21] | 2019 | SR | Indonesia | Cases and controls | 6 | 0 | Periodontal disease | LBW | NR/NR | There is an association between periodontitis and PB. |
| Teshome et al. [22] | 2016 | SR | Ethiopia | Cases and controls | 10 | 0 | Periodontal disease | LBW | NR/NR | There is an association between periodontitis and PB. |
| Corbella et al. [39] | 2016 | SR with MA | Italy | Cases and controls | 22 | 22 (14 PB and 10 LBW) | Periodontitis | PB, LBW and PB + LBW | NR/PB = 1.61 (1.33–1.95), LBW = 1.65 (1.27–2.14), PB + LBW = 3.44 (1.34–8.8) | There is an association between periodontitis and PB, LBW and PB + LBW. |
| Ide et al. [40] | 2013 | SR with MA | United Kingdom | Cases and controls, cohorts and cross-sectional | 18 | 16 (14 PB and 2 LBW) | Periodontitis | PB and PB + LBW | PB = 2.47 (2.19–2.77), PB + LBW = 2.06 (1.34–3.16)/PB = 1.15 (0.89–1.49) | There is an association between periodontitis and PB and PB + LBW. |
| Corbella et al. [23] | 2012 | SR with MA | Italy | Cases and controls | 17 | 17 (14 PB and 7 LBW) | Periodontal disease | PB, LBW and PB + LBW | PB = 1.78 (1.58–2.01), LBW = 1.82 (1.51–2.2), PB + LBW = 3.00 (1.93–4.68)/NR | There is an association between PD and PB, LBW and PB + LBW. |
| Corbella et al. [45] | 2012 | SR with MA | Italy | Cases and controls, cohorts and clinical trials | 37 | 5 (5 PB and 5 LBW) | Periodontal disease | PB and LBW | NR/NR | There was no clear evidence that PD is a major risk factor for adverse pregnancy outcomes, although it may have a minor effect. |
| Xiong et al. [41] | 2007 | SR with MA | United States | Cases and controls, cohorts and clinical trials | 26 (12 PB and 10 LBW) | 4 (3 PB and 2 LBW) | Periodontal disease | PB and LBW | NR/NR | There is an association between PD and PB and LBW. |
| Vettore et al. [25] | 2006 | SR | Brazil | Cases and controls, cohorts and clinical trials | 36 (30 PB and 28 LBW) | 0 | Periodontal disease | PB and LBW | NR/NR | It is not possible to determine the association between PD and PB and LBW. |
| Xiong et al. [24] | 2006 | SR | United States | Cases and controls, cohorts and clinical trials | 25 (8 PB and 6 LBW) | 0 | Periodontal disease | PB and LBW | NR/NR | There is an association between PD and PB and LBW. |
| Khader et al. [42] | 2005 | SR with MA | Jordan | Cases and controls and cohorts | 5 | 4 (3 PB and 2 LBW) | Periodontal disease | PB, LBW and PB + LBW | PB = 4.32 (2.5–7.44), LBW = 5.28 (2.21–12.62), PB + LBW = 5.28 (2.21–12.62)/NR | There is an association between PD and PB, LBW and PB + LBW. |
| Scannapieco et al. [43] | 2003 | SR | United States | Cases and controls, cohorts, cross-sectional and clinical trials | 12 | 0 | Periodontal disease | PB and LBW | NR/NR | There is an association between PD and PB and LBW. |
| Madianos et al. [44] | 2002 | SR | United States | Cases and controls, cohorts, cross-sectional and clinical trials | 25 (5 LBW) | 0 | Periodontitis | PB | NR/NR | The association between PD and PB cannot be determined. |
| Author | Year | AMSTAR-2 | Overall Confidence | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 * | 3 | 4 * | 5 | 6 | 7 * | 8 | 9 * | 10 | 11 * | 12 | 13 * | 14 | 15 * | 16 | |||
| Porto et al. [38] | 2021 | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Moliner-Sánchez et al. [19] | 2020 | Yes | Yes | Yes | Yes | Yes | No | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Manrique-Corredor et al. [20] | 2019 | Yes | Yes | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Syafar et al. [21] | 2019 | Yes | Yes | No | Yes | Yes | Yes | Yes partial | Yes | Yes | No | No meta-analysis | No meta-analysis | Yes | Yes | No meta-analysis | Yes | Moderate |
| Teshome et al. [22] | 2016 | Yes | Yes | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | No | No meta-analysis | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High |
| Corbella et al. [39] | 2016 | Yes | Yes | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Ide et al. [40] | 2013 | Yes | Yes | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Corbella et al. [23] | 2012 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Corbella et al. [45] | 2012 | Yes | Yes partial | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Xiong et al. [41] | 2007 | Yes | Yes | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Vettore et al. [25] | 2006 | Yes | Yes partial | Yes | Yes | No | No | Yes partial | Yes | Yes | Yes | No meta-analysis | No meta-analysis | Yes | Yes | No meta-analysis | Yes | Moderate |
| Xiong et al. [24] | 2006 | Yes | Yes | Yes | Yes | No | No | Yes partial | Yes | Yes | No | No meta-analysis | No meta-analysis | Yes | Yes | No meta-analysis | No | Moderate |
| Khader et al. [42] | 2005 | Yes | Yes partial | Yes | No | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Low |
| Scannapieco et al. [43] | 2003 | Yes | Yes | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | No | No meta-analysis | No meta-analysis | Yes | Yes | No meta-analysis | No | Moderate |
| Madianos et al. [44] | 2002 | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | No | No meta-analysis | No meta-analysis | Yes | Yes | No meta-analysis | No | Moderate |
| Certainty Assessment | Certainty | ||||||
|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | |
| Association between the risk of PB in newborns with PD in pregnant women | |||||||
| 6 | SR | not serious | very serious | not serious | not serious | none | ⨁⨁◯◯ Low |
| Association between the risk of LBW in newborns with PD in pregnant women | |||||||
| 5 | SR | not serious | very serious | not serious | not serious | none | ⨁⨁◯◯ Low |
| Association between the risk of PB with LBW in newborns with PD in pregnant women | |||||||
| 4 | SR | not serious | serious | not serious | not serious | none | ⨁⨁⨁◯ Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padilla-Cáceres, T.; Arbildo-Vega, H.I.; Caballero-Apaza, L.; Cruzado-Oliva, F.; Mamani-Cori, V.; Cervantes-Alagón, S.; Munayco-Pantoja, E.; Panda, S.; Vásquez-Rodrigo, H.; Castro-Mejía, P.; et al. Association between the Risk of Preterm Birth and Low Birth Weight with Periodontal Disease in Pregnant Women: An Umbrella Review. Dent. J. 2023, 11, 74. https://doi.org/10.3390/dj11030074
Padilla-Cáceres T, Arbildo-Vega HI, Caballero-Apaza L, Cruzado-Oliva F, Mamani-Cori V, Cervantes-Alagón S, Munayco-Pantoja E, Panda S, Vásquez-Rodrigo H, Castro-Mejía P, et al. Association between the Risk of Preterm Birth and Low Birth Weight with Periodontal Disease in Pregnant Women: An Umbrella Review. Dentistry Journal. 2023; 11(3):74. https://doi.org/10.3390/dj11030074
Chicago/Turabian StylePadilla-Cáceres, Tania, Heber Isac Arbildo-Vega, Luz Caballero-Apaza, Fredy Cruzado-Oliva, Vilma Mamani-Cori, Sheyla Cervantes-Alagón, Evelyn Munayco-Pantoja, Saurav Panda, Hernán Vásquez-Rodrigo, Percy Castro-Mejía, and et al. 2023. "Association between the Risk of Preterm Birth and Low Birth Weight with Periodontal Disease in Pregnant Women: An Umbrella Review" Dentistry Journal 11, no. 3: 74. https://doi.org/10.3390/dj11030074