

The Impact of Dental Care Programs on Individuals and Their Families: A Scoping Review

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Conceptual Framework
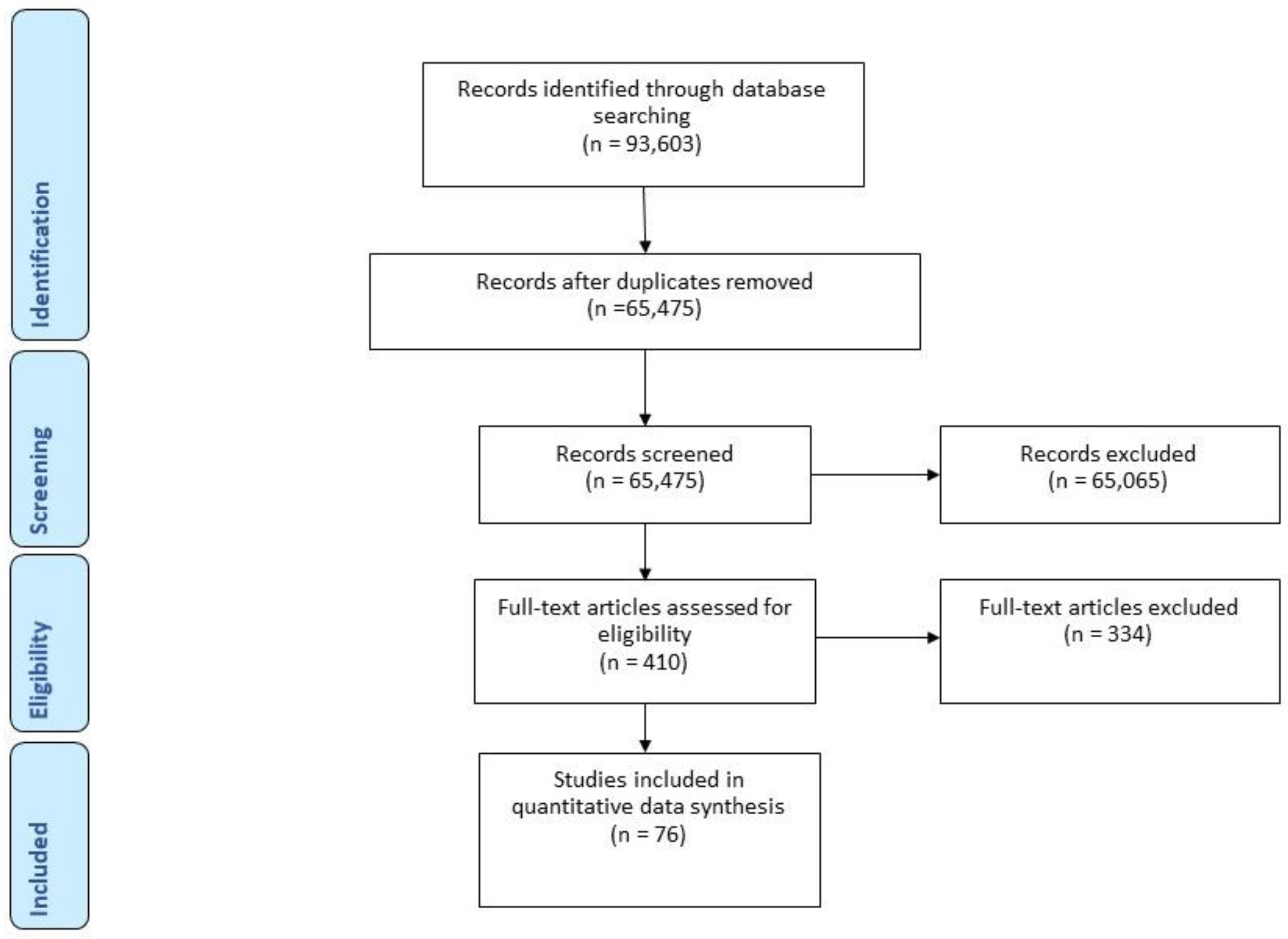
2.2. Design and Study Search
2.3. Inclusion Criteria and Screening Process
2.4. Selection and Data Extraction
3. Results
Data Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Lagerweij, M.; Van Loveren, C. Declining caries trends: Are we satisfied? Curr. Oral Health Rep. 2015, 2, 212–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelton, H. Overview of the impact of changing global patterns of dental caries experience on caries clinical trials. J. Dent. Res. 2004, 83, 29–34. [Google Scholar] [CrossRef]
- Saintrain, M.V.D.L.; Correa, C.R.S.; Saintrain, S.V.; Nuto, S.D.A.S.; Vieira-Meyer, A.P.G.F. Brazilian adolescents’ oral health trends since 1986: An epidemiological observational study. BMC Res. Notes 2015, 8, 554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, D.J.; O’Hayre, M.; Kusiak, J.W.; Somerman, M.J.; Hill, C.V. Oral health disparities: A perspective from the national institute of dental and craniofacial research. Am. J. Public Health 2017, 107, S36–S38. [Google Scholar] [CrossRef] [PubMed]
- Ravaghi, V.; Quiñonez, C.; Allison, P.J. The magnitude of oral health inequalities in C anada: Findings of the C anadian health measures survey. Community Dent. Oral Epidemiol. 2013, 41, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Listl, S.; Galloway, J.; Mossey, P.A.; Marcenes, W. Global Economic Impact of Dental Diseases. J. Dent. Res. 2015, 94, 1355–1361. [Google Scholar] [CrossRef]
- Gift, H.C.; Reisine, S.T.; Larach, D.C. The social impact of dental problems and visits. Am. J. Public Health 1992, 82, 1663–1668. [Google Scholar] [CrossRef] [Green Version]
- Reisine, S.T. Dental health and public policy: The social impact of dental disease. Am. J. Public Health 1985, 75, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Seirawan, H.; Faust, S.; Mulligan, R. The impact of oral health on the academic performance of disadvantaged children. Am. J. Public Health 2012, 102, 1729–1734. [Google Scholar] [CrossRef]
- Jackson, S.L.; Vann, W.F., Jr.; Kotch, J.B.; Pahel, B.T.; Lee, J.Y. Impact of poor oral health on children’s school attendance and performance. Am. J. Public Health 2011, 101, 1900–1906. [Google Scholar] [CrossRef] [PubMed]
- Zaitsu, T.; Saito, T.; Oshiro, A.; Fujiwara, T.; Kawaguchi, Y. The Impact of Oral Health on Work Performance of Japanese Workers. J. Occup. Environ. Med. 2020, 62, e59–e64. [Google Scholar] [CrossRef] [PubMed]
- Halasa-Rappel, Y.A.; Tschampl, C.A.; Foley, M.; Dellapenna, M.; Shepard, D.S. Broken smiles: The impact of untreated dental caries and missing anterior teeth on employment. J. Public Health Dent. 2019, 79, 231–237. [Google Scholar] [CrossRef]
- Quadri, M.F.A.; Jaafari, F.R.M.; Mathmi, N.A.A.; Huraysi, N.H.F.; Nayeem, M.; Jessani, A.; Tadakamadla, S.K.; Tadakamadla, J. Impact of the Poor Oral Health Status of Children on Their Families: An Analytical Cross-Sectional Study. Children 2021, 8, 586. [Google Scholar] [CrossRef] [PubMed]
- Badewy, R.; Singh, H.; Quiñonez, C.; Singhal, S. Impact of poor oral health on community-dwelling seniors: A scoping review. Health Serv. Insights 2021, 14, 1178632921989734. [Google Scholar] [CrossRef] [PubMed]
- Allin, S.; Farmer, J.; Quiñonez, C.; Peckham, A.; Marchildon, G.; Panteli, D.; Henschke, C.; Fattore, G.; Lamloum, D.; Holden, A.C. Do health systems cover the mouth? Comparing dental care coverage for older adults in eight jurisdictions. Health Policy 2020, 124, 998–1007. [Google Scholar] [CrossRef]
- Chari, M.; Ravaghi, V.; Sabbah, W.; Gomaa, N.; Singhal, S.; Quiñonez, C. Oral health inequality in Canada, the United States and United Kingdom. PLoS ONE 2022, 17, e0268006. [Google Scholar] [CrossRef]
- Ravaghi, V.; Farmer, J.; Quiñonez, C. Persistent but narrowing oral health care inequalities in Canada from 2001 through 2016. J. Am. Dent. Assoc. 2020, 151, 349–357. [Google Scholar] [CrossRef]
- Zivkovic, N.; Aldossri, M.; Gomaa, N.; Farmer, J.W.; Singhal, S.; Quiñonez, C.; Ravaghi, V. Providing dental insurance can positively impact oral health outcomes in Ontario. BMC Health Serv. Res. 2020, 20, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Manning, W.G.; Bailit, H.L.; Benjamin, B.; Newhouse, J.P. The demand for dental care: Evidence from a randomized trial in health insurance. J. Am. Dent. Assoc. (1939) 1985, 110, 895–902. [Google Scholar] [CrossRef]
- Bailit, H.L.; Newhouse, J.P.; Brook, R.H.; Duan, N.; Goldberg, G.A.; Hanley, J.M.; Kamberg, C.; Spolsky, V.W.; Black, A.; Lohr, K.N. Does More Generous Dental Insurance Coverage Improve Oral Health? Available online: https://www.rand.org/pubs/notes/N2591.html (accessed on 27 October 2020).
- Goes, P.; Watt, R.; Hardy, R.; Sheiham, A. The prevalence and severity of dental pain in 14-15 year old Brazilian schoolchildren. Community Dent. Health 2007, 24, 217–224. [Google Scholar] [PubMed]
- Gherunpong, S.; Tsakos, G.; Sheiham, A. The prevalence and severity of oral impacts on daily performances in Thai primary school children. Health Qual. Life Outcomes 2004, 2, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- After Medicaid Expansion In Kentucky, Use Of Hospital Emergency Departments For Dental Conditions Increased|Health Affairs. Available online: https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2016.0976 (accessed on 27 October 2020).
- Wallace, B.B.; MacEntee, M.I.; Pauly, B. Community dental clinics in British Columbia, Canada: Examining the potential as health equity interventions. Health Soc. Care Community 2015, 23, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Graham, H. Tackling inequalities in health in England: Remedying health disadvantages, narrowing health gaps or reducing health gradients? J. Soc. Policy 2004, 33, 115–131. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 1–7. [Google Scholar] [CrossRef]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Trico, A.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Prisma Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- The World Bank High income|Data. Available online: https://data.worldbank.org/country/XD (accessed on 16 August 2022).
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. JMLA 2016, 104, 240. [Google Scholar] [CrossRef]
- Sfeatcu, R.; Dumitrache, M.A.; Cărămidă, M.; Johannsen, A.; Perlea, P. A pilot study on the effectiveness of a 2-year school-based oral health educational programme using experiential learning among adolescents. Int. J. Dent. Hyg. 2019, 17, 221–228. [Google Scholar] [CrossRef]
- Samson, H.; Berven, L.; Strand, G.V. Long-term effect of an oral healthcare programme on oral hygiene in a nursing home. Eur. J. Oral Sci. 2009, 117, 575–579. [Google Scholar] [CrossRef]
- Sakayori, T.; Maki, Y.; Ohkubo, M.; Ishida, R.; Hirata, S.; Ishii, T. Longitudinal Evaluation of Community Support Project to Improve Oral Function in Japanese Elderly. Bull. Tokyo Dent. Coll. 2016, 57, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plutzer, K.; Spencer, A.J. Efficacy of an oral health promotion intervention in the prevention of early childhood caries. Community Dent. Oral Epidemiol. 2008, 36, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Phlypo, I.; De Tobel, J.; Marks, L.; De Visschere, L.; Koole, S. Integrating community service learning in undergraduate dental education: A controlled trial in a residential facility for people with intellectual disabilities. Spec. Care Dentist. 2018, 38, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Van den Branden, S.; Van den Broucke, S.; Leroy, R.; Declerck, D.; Bogaerts, K.; Hoppenbrouwers, K. Effect evaluation of an oral health promotion intervention in preschool children. Eur. J. Public Health 2014, 24, 893–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, Y.; Heinrich-Weltzien, R. Evaluation of an interdisciplinary preventive programme for early childhood caries: Findings of a regional German birth cohort study. Clin. Oral Investig. 2016, 20, 1943–1952. [Google Scholar] [CrossRef]
- Ueno, M.; Shinada, K.; Zaitsu, T.; Yokoyama, S.; Kawaguchi, Y. Effects of an oral health education program targeting oral malodor prevention in Japanese senior high school students. Acta Odontol. Scand. 2012, 70, 426–431. [Google Scholar] [CrossRef]
- Tubert-Jeannin, S.; Leger, S.; Manevy, R. Addressing children’s oral health inequalities: Caries experience before and after the implementation of an oral health promotion program. Acta Odontol. Scand. 2012, 70, 255–264. [Google Scholar] [CrossRef]
- Bizarra, M.D.F.; Ribeiro Graça, S. Short-term impact of an oral health program for adults with cerebral palsy. Spec. Care Dentist. 2020, 40, 26–34. [Google Scholar] [CrossRef]
- Freeman, R.; Gibson, B.; Humphris, G.; Leonard, H.; Yuan, S.; Whelton, H. School-based health education programmes, health-learning capacity and child oral health–related quality of life. Health Educ. J. 2016, 75, 698–711. [Google Scholar] [CrossRef] [Green Version]
- Ganss, C.; Heins, M.; Schlueter, N. An oral care programme for adults—Evaluation after 15 years; Carvalho, T.S., Ed. PLoS ONE 2019, 14, e0223960. [Google Scholar] [CrossRef]
- Lambert, M.J.; De Visschere, L.M.; Martens, L.C.; Deschepper, E.; Vanobbergen, J. The impact of a prospective 4-year longitudinal school intervention for improving oral health and oral health inequalities in primary schoolchildren in Flanders-Belgium. Int. J. Paediatr. Dent. 2019, 29, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Mariño, R.; Calache, H.; Morgan, M. A community-based culturally competent oral health promotion for migrant older adults living in Melbourne, Australia. J. Am. Geriatr. Soc. 2013, 61, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Mariño, R.J.; Marwaha, P.; Barrow, S. Web-based oral health promotion program for older adults: Development and preliminary evaluation. Int. J. Med. Inf. 2016, 91, e9–e15. [Google Scholar] [CrossRef] [PubMed]
- Nihtilä, A.; Tuuliainen, E.; Komulainen, K.; Autonen-Honkonen, K.; Nykänen, I.; Hartikainen, S.; Ahonen, R.; Tiihonen, M.; Suominen, A.L. Preventive oral health intervention among old home care clients. Age Ageing 2017, 46, 846–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faulks, D.; Hennequin, M. Evaluation of a long-term oral health program by carers of children and adults with intellectual disabilities. Spec. Care Dentist. 2000, 20, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.; Bartsch, B.; Schütz, C.; Jablonski-Momeni, A.; Pieper, K. Implementation and evaluation of an interdisciplinary preventive program to prevent early childhood caries. Clin. Oral Investig. 2019, 23, 187–197. [Google Scholar] [CrossRef]
- Lopez Cazaux, S.; Lefer, G.; Rouches, A.; Bourdon, P. Toothbrushing training programme using an iPad® for children and adolescents with autism. Eur. Arch. Paediatr. Dent. 2019, 20, 277–284. [Google Scholar] [CrossRef]
- Livny, A.; Sgan-Cohen, H.D. A review of a community program aimed at preventing early childhood caries among Jerusalem infants–a brief communication. J. Public Health Dent. 2007, 67, 78–82. [Google Scholar] [CrossRef]
- Livny, A.; Vered, Y.; Slouk, L.; Sgan-Cohen, H.D. Oral health promotion for schoolchildren—Evaluation of a pragmatic approach with emphasis on improving brushing skills. BMC Oral Health 2008, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.; Blinkhorn, F.; Moir, R.; Blinkhorn, A. Results of a two year dental health education program to reduce dental caries in young Aboriginal children in New South Wales, Australia. Community Dent. Health 2018, 35, 211–216. [Google Scholar]
- Hoeft, K.S.; Barker, J.C.; Shiboski, S.; Pantoja-Guzman, E.; Hiatt, R.A. Effectiveness evaluation of Contra Caries Oral Health Education Program for improving Spanish-speaking parents’ preventive oral health knowledge and behaviors for their young children. Community Dent. Oral Epidemiol. 2016, 44, 564–576. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Weidner, N.; Logeswaran, T.; Jux, C.; Schlenz, M.A.; Krämer, N.; Bulski, J.C. Evaluation of the Effectiveness of an Interdisciplinary Preventive Oral Hygiene Program for Children with Congenital Heart Disease. Int. J. Environ. Res. Public. Health 2021, 18, 3497. [Google Scholar] [CrossRef] [PubMed]
- Seo, K.; Kim, H. Effects of oral health programmes on xerostomia in community-dwelling elderly: A systematic review and meta-analysis. Int. J. Dent. Hyg. 2020, 18, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.; Santos, N.M.L.; Hilgert, J.B.; Hugo, F.N. Effectiveness of oral health education on oral hygiene and dental caries in schoolchildren: Systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2018, 46, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.-F.; Huang, C.-M.; Chou, C.; Yu, S. Effect of oral health education programs for caregivers on oral hygiene of the elderly: A systemic review and meta-analysis. Int. J. Nurs. Stud. 2015, 52, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Nakre, P.D.; Harikiran, A. Effectiveness of oral health education programs: A systematic review. J. Int. Soc. Prev. Community Dent. 2013, 3, 103. [Google Scholar] [CrossRef] [Green Version]
- Henry, J.A.; Muthu, M.S.; Swaminathan, K.; Kirubakaran, R. Do oral health educational programmes for expectant mothers prevent early childhood caries? Systematic review. Oral Health Prev Dent 2017, 15, 215–221. [Google Scholar]
- Anderson, L.W.; Bloom, B.S. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives; Pearson: London, UK, 2001. [Google Scholar]
- Slade, G.D.; Bailie, R.S.; Roberts-Thomson, K.; Leach, A.J.; Raye, I.; Endean, C.; Simmons, B.; Morris, P. Effect of health promotion and fluoride varnish on dental caries among Australian Aboriginal children: Results from a community-randomized controlled trial: Cluster RCT of health promotion and fluoride varnish. Community Dent. Oral Epidemiol. 2011, 39, 29–43. [Google Scholar] [CrossRef] [Green Version]
- Sköld, U.M. Approximal caries increment in relation to baseline approxi- mal caries prevalence among adolescents in Sweden with and without a school-based fluoride varnish programme. Community Dent Health 2016, 33, 281–285. [Google Scholar]
- Wagner, Y.; Heinrich-Weltzien, R. Evaluation of a regional German interdisciplinary oral health programme for children from birth to 5 years of age. Clin. Oral Investig. 2017, 21, 225–235. [Google Scholar] [CrossRef]
- Achembong, L.N.; Kranz, A.M.; Rozier, R.G. Office-Based Preventive Dental Program and Statewide Trends in Dental Caries. Pediatrics 2014, 133, e827–e834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dohnke-Hohrmann, S.; Zimmer, S. Change in Caries Prevalence after Implementation of a Fluoride Varnish Program. J. Public Health Dent. 2004, 64, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Milsom, K.; Rice, A.; Kearney-Mitchell, P.; Kellett, L. A review of a child population dental preventive programme in Halton and St Helens. Br. Dent. J. 2014, 216, E18. [Google Scholar] [CrossRef]
- Källestål, C. The effect of five years’ implementation of caries-preventive methods in Swedish high-risk adolescents. Caries Res. 2005, 39, 20–26. [Google Scholar] [CrossRef]
- Sundell, A.L.; Ullbro, C.; Koch, G. Evaluation of preventive programs in high caries active preschool children. Swed. Dent. J. 2013, 37, 8. [Google Scholar]
- Pieper, K.; Weber, K.; Margraf-Stiksrud, J.; Heinzel-Gutenbrunner, M.; Stein, S.; Jablonski-Momeni, A. Evaluation of a preventive program aiming at children with increased caries risk using ICDAS II criteria. Clin. Oral Investig. 2013, 17, 2049–2055. [Google Scholar] [CrossRef]
- Zimmer, S.; Bizhang, M.; Seemann, R.; Witzke, S.; Roulet, J.-F. The effect of a preventive program, including the application of low-concentration fluoride varnish, on caries control in high-risk children. Clin. Oral Investig. 2001, 5, 40–44. [Google Scholar] [CrossRef]
- Wennhall, I.; Matsson, L.; Schröder, U.; Twetman, S. Outcome of an oral health outreach programme for preschool children in a low socioeconomic multicultural area. Int. J. Paediatr. Dent. 2008, 18, 84–90. [Google Scholar] [CrossRef]
- Winter, J.; Jablonski-Momeni, A.; Ladda, A.; Pieper, K. Long-term effect of intensive prevention on dental health of primary school children by socioeconomic status. Clin. Oral Investig. 2018, 22, 2241–2249. [Google Scholar] [CrossRef]
- Winter, J.; Weber, K.; Martin, K.; Heinzel-Gutenbrunner, M.; Pieper, K. Evaluation of an intensified prevention program for 4th graders with increased caries risk using ICDAS. Int. J. Paediatr. Dent. 2016, 26, 250–258. [Google Scholar] [CrossRef]
- Macnab, A.; Rozmus, J.; Benton, D.; Gagnon, F. 3-year results of a collaborative school-based oral health program in a remote First Nations community. Rural. Remote Health 2008, 8, 1–7. [Google Scholar] [CrossRef]
- Bergström, E.; Lingström, P.; Hakeberg, M.; Gahnberg, L.; Sköld, U. Caries and costs: An evaluation of a school-based fluoride varnish programme for adolescents in a Swedish region. Community Dent Health 2016, 33, 138–144. [Google Scholar] [PubMed]
- Andruškevičienė, V.; Milčiuvienė, S.; Bendoraitienė, E.; Saldūnaitė, K.; Vasiliauskienė, I.; Slabšinskienė, E.; Narbutaitė, J. Oral health status and effectiveness of caries prevention programme in kindergartens in Kaunas city (Lithuania). Oral Health Prev. Dent. 2008, 6, 343–348. [Google Scholar] [PubMed]
- Meyer, K.; Khorshidi-Böhm, M.; Geurtsen, W.; Günay, H. An early oral health care program starting during pregnancy—A long-term study—Phase V. Clin. Oral Investig. 2014, 18, 863–872. [Google Scholar] [CrossRef]
- Sloane, P.D.; Zimmerman, S.; Chen, X.; Barrick, A.L.; Poole, P.; Reed, D.; Mitchell, M.; Cohen, L.W. Effect of a person-centered mouth care intervention on care processes and outcomes in three nursing homes. J. Am. Geriatr. Soc. 2013, 61, 1158–1163. [Google Scholar] [CrossRef]
- Wennhall, I.; Mårtensson, E.-M.; Sjunnesson, I.; Matsson, L.; Schröder, U.; Twetman, S. Caries-preventive effect of an oral health program for preschool children in a low socio-economic, multicultural area in Sweden: Results after one year. Acta Odontol. Scand. 2005, 63, 163–167. [Google Scholar] [CrossRef]
- Nakamura, A.; Sakuma, S.; Yoshihara, A.; Deguchi, T.; Yagi, M.; Miyazaki, H. Long-term follow-up of the effects of a school-based caries preventive programme involving fluoride mouth rinse and targeted fissure sealant: Evaluation at 20 years old. Int. Dent. J. 2009, 59, 215–221. [Google Scholar]
- Lee, M.-Y.; Kim, N.-H.; Chung, W.-G.; Choi, E.-M.; Kim, C.-B.; Choi, E.-H.; Chang, S.-J. Effect of an oral healthcare program on gingival health status in rural areas of South Korea. Rural Remote Health 2017, 17. [Google Scholar] [CrossRef] [Green Version]
- Sköld, U.M.; Birkhed, D.; Borg, E.; Petersson, L.G. Approximal caries development in adolescents with low to moderate caries risk after different 3-year school-based supervised fluoride mouth rinsing programmes. Caries Res. 2005, 39, 529–535. [Google Scholar] [CrossRef]
- Ruff, R.R.; Niederman, R. Comparative effectiveness of school-based caries prevention: A prospective cohort study. BMC Oral Health 2018, 18, 53. [Google Scholar] [CrossRef] [Green Version]
- Simmer-Beck, M.; Walker, M.; Gadbury-Amyot, C.; Liu, Y.; Kelly, P.; Branson, B. Effectiveness of an alternative dental workforce model on the oral health of low-income children in a school-based setting. Am. J. Public Health 2015, 105, 1763–1769. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.; Edwards, J.M.; Brothwell, D.J.; Yakiwchuk, C.A.; Bertone, M.F.; Mellon, B.; Ward, J.; Ellis, M.; Hai-Santiago, K.; Lawrence, H. Evaluating the impact of a community developed collaborative project for the prevention of early childhood caries: The Healthy Smile Happy Child project. Rural. Remote Health 2015, 15, 155–170. [Google Scholar] [CrossRef]
- Muller-Bolla, M.; Pierre, A.; Lupi-Pégurier, L.; Velly, A.M. Effectiveness of school-based dental sealant programs among children from low-income backgrounds: A pragmatic randomized clinical trial with a follow-up of 3 years. Community Dent. Oral Epidemiol. 2016, 44, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Dudovitz, R.N.; Valiente, J.E.; Espinosa, G.; Yepes, C.; Padilla, C.; Puffer, M.; Slavkin, H.C.; Chung, P.J. A school-based public health model to reduce oral health disparities: A school-based public health model. J. Public Health Dent. 2018, 78, 9–16. [Google Scholar] [CrossRef]
- Lai, B.; Tan, W.K.; Lu, Q.S. Clinical efficacy of a two-year oral health programme for infants and toddlers in Singapore. Singapore Med. J. 2018, 59, 87. [Google Scholar] [CrossRef]
- Lin, D.L.; Harrison, R.; Aleksejuniene, J. Can a prenatal dental public health program make a difference. J. Can. Dent. Assoc. 2011, 77, 7. [Google Scholar]
- Burgette, J.M.; Preisser, J.S.; Weinberger, M.; King, R.S.; Lee, J.Y.; Rozier, R.G. Enrollment in early head start and oral health-related quality of life. Qual. Life Res. 2017, 26, 2607–2618. [Google Scholar] [CrossRef]
- Kim, E.-K.; Park, E.Y.; Sa Gong, J.-W.; Jang, S.-H.; Choi, Y.-H.; Lee, H.-K. Lasting effect of an oral hygiene care program for patients with stroke during in-hospital rehabilitation: A randomized single-center clinical trial. Disabil. Rehabil. 2017, 39, 2324–2329. [Google Scholar] [CrossRef]
- García-Pola, M.; González-Díaz, A.; García-Martín, J.M.M. Effect of a Preventive Oral Health Program Starting during Pregnancy: A Case-Control Study Comparing Immigrant and Native Women and Their Children. Int. J. Environ. Res. Public. Health 2021, 18, 4096. [Google Scholar] [CrossRef]
- Lee, H.-J.; Han, D.-H.; Kim, J.-H.; Wu, H.-G. The effect of comprehensive oral care program on oral health and quality of life in patients undergoing radiotherapy for head and neck cancer: A quasi-experimental case-control study. Medicine 2021, 100. [Google Scholar] [CrossRef]
- Starr, J.R.; Ruff, R.R.; Palmisano, J.; Goodson, J.M.; Bukhari, O.M.; Niederman, R. Longitudinal caries prevalence in a comprehensive, multicomponent, school-based prevention program. J. Am. Dent. Assoc. 2021, 152, 224–233. [Google Scholar] [CrossRef]
- Eckersten, C.; Pylvänen, L.; Schröder, U.; Twetman, S.; Wennhall, I.; Matsson, L. Prevalence of dental fluorosis in children taking part in an oral health programme including fluoride tablet supplements from the age of 2 years. Int. J. Paediatr. Dent. 2010, 20, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Alsumait, A.; ElSalhy, M.; Amin, M. Long-term effects of school-based oral health program on oral health knowledge and practices and oral health-related quality of life. Med. Princ. Pract. 2015, 24, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Alsumait, A.; ElSalhy, M.; Behzadi, S.; Raine, K.D.; Gokiert, R.; Cor, K.; Almutawa, S.; Amin, M. Impact evaluation of a school-based oral health program: Kuwait National Program. BMC Oral Health 2019, 19, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyatt, C.C.L. A 5-year follow-up of older adults residing in long-term care facilities: Utilisation of a comprehensive dental programme. Gerodontology 2009, 26, 282–290. [Google Scholar] [CrossRef]
- Walker, R.J.; Kiyak, H.A. The impact of providing dental services to frail older adults: Perceptions of elders in adult day health centers. Spec. Care Dentist. 2007, 27, 139–143. [Google Scholar] [CrossRef]
- Janssens, B.; Vanobbergen, J.; Petrovic, M.; Jacquet, W.; Schols, J.M.; De Visschere, L. The impact of a preventive and curative oral healthcare program on the prevalence and incidence of oral health problems in nursing home residents. PLoS ONE 2018, 13, e0198910. [Google Scholar] [CrossRef] [Green Version]
- Hyde, S.; Weintraub, J.A.; Satariano, W.A. An evaluation of the San Francisco department of human services welfare dental program. J. Public Health Dent. 2005, 65, 104–109. [Google Scholar] [CrossRef]
- Hyde, S.; Satariano, W.A.; Weintraub, J.A. Welfare dental intervention improves employment and quality of life. J. Dent. Res. 2006, 85, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Gomez, S.; Weber, A. Effectiveness of a caries preventive program in pregnant women and new mothers on their offspring. Int. J. Paediatr. Dent. 2001, 11, 117–122. [Google Scholar] [CrossRef]
- George, A.; Dahlen, H.G.; Blinkhorn, A.; Ajwani, S.; Bhole, S.; Ellis, S.; Yeo, A.; Elcombe, E.; Johnson, M. Evaluation of a midwifery initiated oral health-dental service program to improve oral health and birth outcomes for pregnant women: A multi-centre randomised controlled trial. Int. J. Nurs. Stud. 2018, 82, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.D.; Larsen, M.D.; Ambrose, T.; Degano, R.; Gallo, L.; Cardo, V.A., Jr. Efficacy of a Prenatal Oral Health Program Follow-up with Mothers and their Children. N. Y. State Dent. J. 2016, 82, 15–20. [Google Scholar] [PubMed]
- Rong, W.S.; Lo, E.C.M. Effect of providing outreach oral health care to institutionalised elders in Hong Kong. Oral Health Prev. Dent. 2009, 7, 261. [Google Scholar]
- Borroto, D.O.; Salinas, A.A.; Buratovic, J.V.; Mococain, C.C.; Ferrer, A.M.; Vera, S.P. Impact of the national program More Smiles for Chile on women’s quality of life. Community Dent. Health 2021, 38, 39–43. [Google Scholar]
- Sheiham, A.; Alexander, D.; Cohen, L.; Marinho, V.; Moysés, S.; Petersen, P.; Spencer, J.; Watt, R.; Weyant, R. Global oral health inequalities: Task group—Implementation and delivery of oral health strategies. Adv. Dent. Res. 2011, 23, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Kay, E.; Locker, D. Is dental health education effective? A systematic review of current evidence. Community Dent. Oral Epidemiol. 1996, 24, 231–235. [Google Scholar] [CrossRef]
- Habbu, S.G.; Krishnappa, P. Effectiveness of oral health education in children–a systematic review of current evidence (2005–2011). Int. Dent. J. 2015, 65, 57–64. [Google Scholar] [CrossRef]
- World Health Organization. Ottawa Charter for Health Promotion, 1986; World Health Organization: Geneva, Switzerland, 1986. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics of the Studies | n | % |
|---|---|---|
| Year of publication | ||
| 2000–2005 | 8 | 11 |
| 2006–2010 | 12 | 16 |
| 2011–2015 | 18 | 24 |
| 2016–2021 | 38 | 50 |
| Region of study | ||
| North America | 16 | 21 |
| South America | 2 | 2 |
| Europe | 35 | 46 |
| Middle East | 4 | 5 |
| Asia | 8 | 11 |
| Australia and Oceania | 6 | 8 |
| Not applicable | 5 | 7 |
| Type of intervention | ||
| Oral health education (OHE) | 29 | 38 |
| Diagnostic and preventive | 35 | 46 |
| Interventional | 12 | 16 |
| Program setting * | ||
| School-based setting | 28 | 37 |
| Long-term care and institutional settings | 8 | 11 |
| Community setting/public health setting | 20 | 26 |
| Medical setting | 11 | 14 |
| Dental setting | 7 | 9 |
| Reviews | 5 | 6 |
| Target population * | ||
| Children | 42 | 55 |
| Adolescents | 11 | 14 |
| Adults | 13 | 17 |
| Elders | 14 | 18 |
| Not specified/unclear | 4 | 5 |
| Personnel delivering the program * | ||
| Non-healthcare personnel | 10 | 13 |
| Healthcare personnel | 13 | 17 |
| Dental personnel | 47 | 62 |
| Not specified/unclear | 11 | 14 |
| Type of outcome assessed | ||
| Clinical outcome(s) only | 46 | 61 |
| Behavioral/self-reported outcome(s) only | 14 | 18 |
| Both clinical and behavioral/self-reported outcomes | 16 | 21 |
| Study design | ||
| Experimental study | 47 | 62 |
| Cross-sectional study | 6 | 8 |
| Longitudinal/prospective cohort | 9 | 12 |
| Retrospective cohort | 5 | 7 |
| Secondary analysis of data | 1 | 1 |
| Ecological study | 1 | 1 |
| Systematic review | 5 | 7 |
| Not specified | 2 | 2 |
| Outcomes measures * | ||
| Individual level outcomes | ||
| Caries | 45 | 59 |
| Gingival health | 16 | 21 |
| Oral hygiene | 17 | 22 |
| Oral health related quality of life (OHRQoL) | 9 | 12 |
| Oral health knowledge and attitude | 15 | 20 |
| Oral health behaviors | 19 | 25 |
| Miscellaneous | 7 | 9 |
| Family level outcomes | ||
| Parental oral health knowledge and attitude | 4 | 5 |
| Parental oral health behaviors | 4 | 5 |
| Parental stress and family function | 1 | 1 |
| Parental OHRQoL | 1 | 1 |
| |
| School-based programs | Organized by schools and implemented either within schools or other educational premises, which include pre-school and public daycare centers. |
| Long-term care and institutional programs | Implemented in nursing homes, long-term care facilities, or residential homes for elders or adults with physical or mental challenges (e.g., cerebral palsy, neurodevelopmental disabilities, etc.). |
| Community-based programs | Implemented in public health/community centers. These include, but are not limited to, mother and child health centers, child health centers, and public health units. |
| Medical setting programs | Delivered in a medical context outside conventional dental settings, such as programs provided in hospitals, medical clinics, well-baby clinics, or other non-dental healthcare settings. |
| Dental setting programs | Programs implemented in conventional dental settings (i.e., private dental clinics) or dental schools. |
| |
| OHE programs | Programs that provide oral health education about preventing and managing various oral health diseases. It also includes oral hygiene instructions on the proper brushing techniques, the use of fluoridated toothpaste, and flossing. These were delivered in the form of lectures, motivational interviews, pamphlets, amongst other methods of oral health promotion. The programs utilize one or more of the three learning domains (cognitive, psychomotor, and affective) introduced by Bloom in 1956 [33]. |
| Diagnostic and preventive programs | Includes those programs providing primary and secondary prevention services that aim to prevent or limit the development of oral diseases such as oral screenings and referrals, fluoride applications, pit and fissure sealants, and non-invasive therapies (e.g., atraumatic restorative treatment and interim stabilization therapy). |
| Interventional programs | Includes those programs that provide curative dental services such as restorations, extractions, root canal treatments, and prosthodontic care. |
| |
| Children | Less than 12 years old. |
| Adolescents | Between 12 and 19 years old. |
| Adults | Between 20 and 64 years old. |
| Elders | Sixty-five years old and above. |
| |
| Non-healthcare personnel | Individuals outside the healthcare sector such as teachers, caregivers, social workers, and trained peers. |
| Healthcare personnel | Individuals who work in the healthcare sector but do not have formal training in dentistry, such as nurses, physicians, and midwives. |
| Dental personnel | Individuals who have completed formal training in dentistry or dentistry-related fields such as dentists, dental hygienists, dental assistants, dental therapists, and dental nurses. |
| |
| E.1 Individual outcomes | Outcomes that are specific to the individual receiving the intervention. Examples include changes in the oral health status, knowledge, and attitudes towards dental care behaviors. |
| E.1.1 Clinical outcomes | Assessed by calibrated examiners via clinical measures such as caries indices, periodontal measures, etc. |
| e.g., dmft/DMFT/, caries increment, percent increase in caries, demineralization, etc. |
| e.g., gingival and periodontal indices such as community periodontal index for treatment needs (CPITN), gingival index (GI), periodontal index (PI), bleeding on probing (BoP), clinical attachment loss (CAL), etc. |
| Assessed using indices for measuring plaque, calculus, debris, denture plaque, mucosal plaque score (MPS), etc. |
| Other less commonly used clinical outcomes that are captured in the review include:
|
| E.1.2 Self-reported outcomes | Collected through chairside interviews or questionnaires without a clinical assessment. |
| Indices or measures that assess the impact of dental problems on the quality of life, such as the oral health impact profile (OHIP), oral impact on daily performances (OIDP), and geriatric oral health assessment index (GOHAI). |
| All aspects of knowledge around the process of dental decay, periodontal disease, the importance of dental visits, fluoride agents, etc. |
| Oral hygiene measures (frequency of brushing, flossing etc.), dietary habits including the consumption of sugary food and beverages, and the consumption frequency reported by the individuals. |
| E.2 Family level outcomes | Outcomes that are specific to the parents and the family of the recipients of the intervention. |
| Measures of changes in the knowledge and perceptions about different dental disease processes. |
| Measures change in parental oral health behaviors (e.g., brushing, flossing, etc.) |
| Assesses change in parental distress levels attributed to changes in their dependents’ oral health status and wellbeing. |
| Measures change in parental quality of life influenced by their dependents’ oral health status and wellbeing. |
| The Domain Addressed | n | % |
|---|---|---|
| Cognitive only | 9 | 31 |
| Psychomotor only | 1 | 3 |
| Cognitive, psychomotor | 7 | 24 |
| Cognitive, affective | 4 | 14 |
| Psychomotor, affective | 2 | 7 |
| Cognitive, psychomotor, affective | 1 | 3 |
| N/A | 5 | 17 |
| Author, Year | Services Provided |
|---|---|
| Alsumiat et al., 2015 | Not specified |
| Alsumiat et al., 2019 | Not specified |
| George et al., 2018 |
|
| Gomez et al., 2001 |
|
| Hyde et al., 2005 |
|
| Hyde et al., 2006 | |
| Janssens et al., 2018 | Not specified |
| Larsen et al., 2016 | Not specified |
| Ortuno Borroto et al., 2021 | Prevention, conventional periodontal treatments, dental fillings, root canal treatments, dental extractions, and removable dentures |
| Rong et al., 2009 |
|
| Walker et al., 2007 |
|
| Wyatt et al., 2009 | Not specified |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghoneim, A.; D’Souza, V.; Ebnahmady, A.; Kaura Parbhakar, K.; He, H.; Gerbig, M.; Laporte, A.; Hancock Howard, R.; Gomaa, N.; Quiñonez, C.; et al. The Impact of Dental Care Programs on Individuals and Their Families: A Scoping Review. Dent. J. 2023, 11, 33. https://doi.org/10.3390/dj11020033
Ghoneim A, D’Souza V, Ebnahmady A, Kaura Parbhakar K, He H, Gerbig M, Laporte A, Hancock Howard R, Gomaa N, Quiñonez C, et al. The Impact of Dental Care Programs on Individuals and Their Families: A Scoping Review. Dentistry Journal. 2023; 11(2):33. https://doi.org/10.3390/dj11020033
Chicago/Turabian StyleGhoneim, Abdulrahman, Violet D’Souza, Arezoo Ebnahmady, Kamini Kaura Parbhakar, Helen He, Madeline Gerbig, Audrey Laporte, Rebecca Hancock Howard, Noha Gomaa, Carlos Quiñonez, and et al. 2023. "The Impact of Dental Care Programs on Individuals and Their Families: A Scoping Review" Dentistry Journal 11, no. 2: 33. https://doi.org/10.3390/dj11020033