
The Use of Computational Fluid Dynamics for Assessing Flow-Induced Acoustics to Diagnose Lung Conditions


Abstract
:1. Introduction
2. Materials and Methods
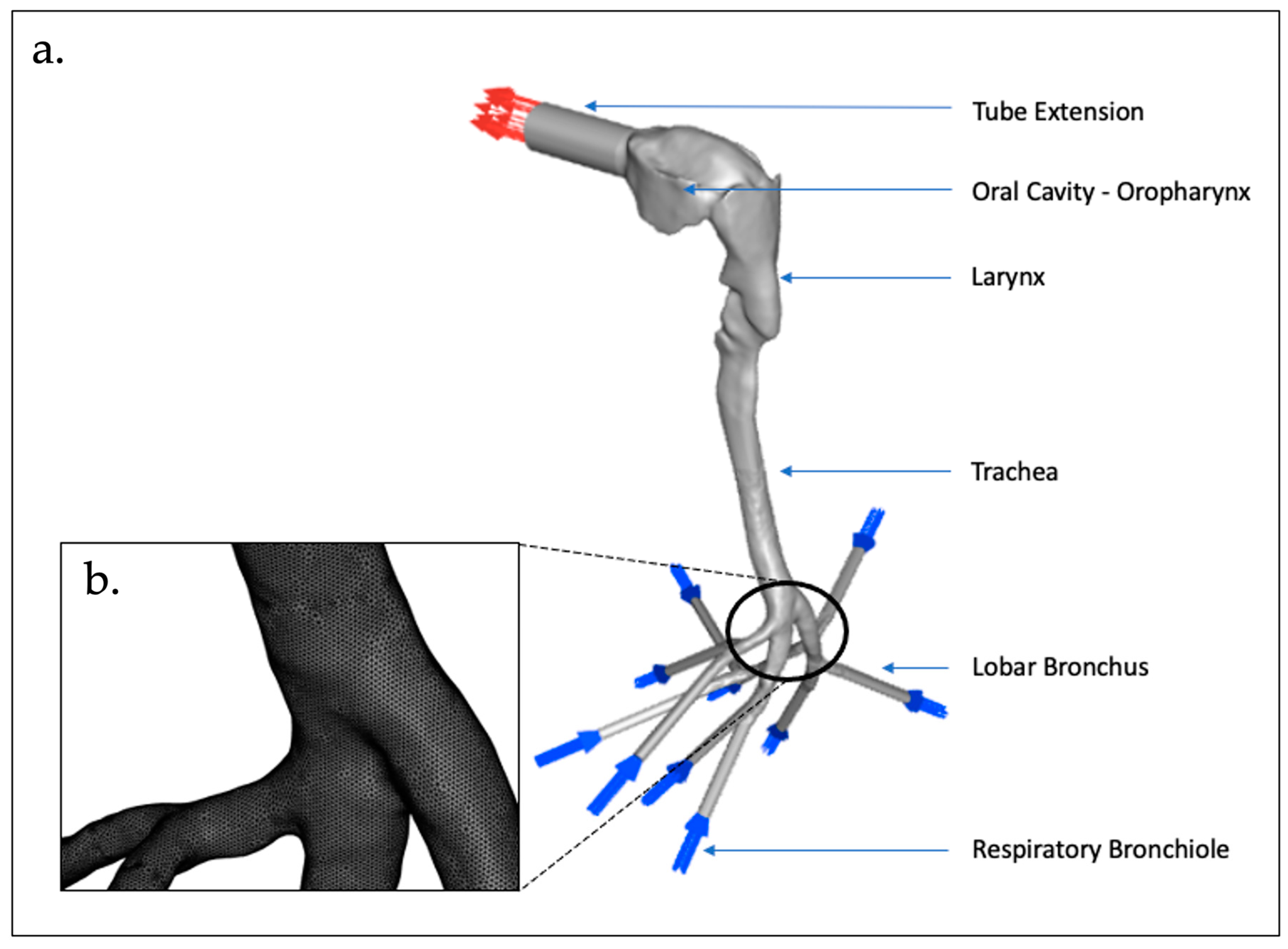
2.1. Model Geometry and Mesh
2.2. CFD Procedures and Boundary Conditions
2.3. Governing Equations
2.3.1. CFD Model—Broadband Noise Source Models
2.3.2. CFD Model—Transport Equations
2.4. Data Analysis and Comparison
3. Results and Discussion
3.1. Validation of Simulated Flow Velocity
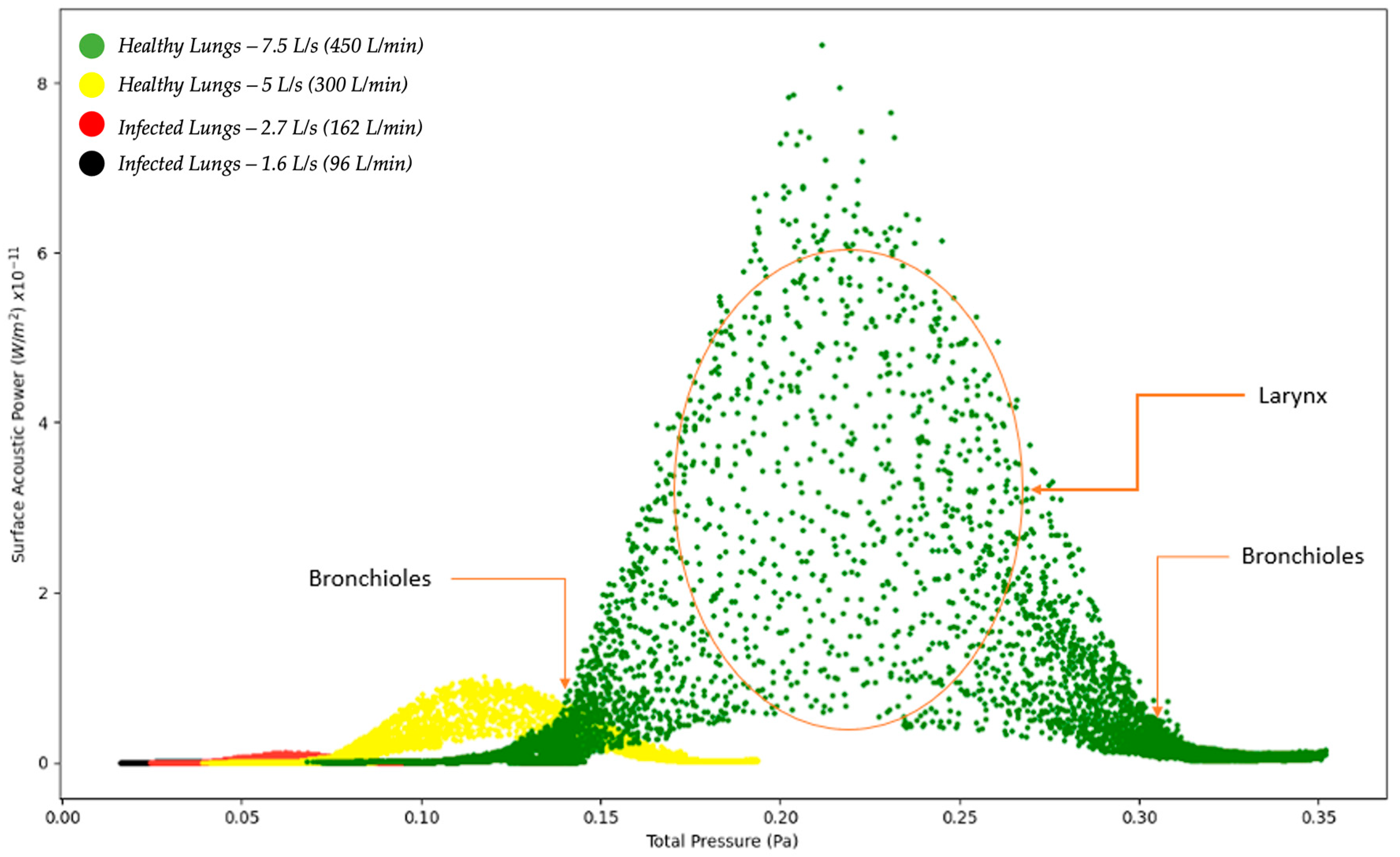
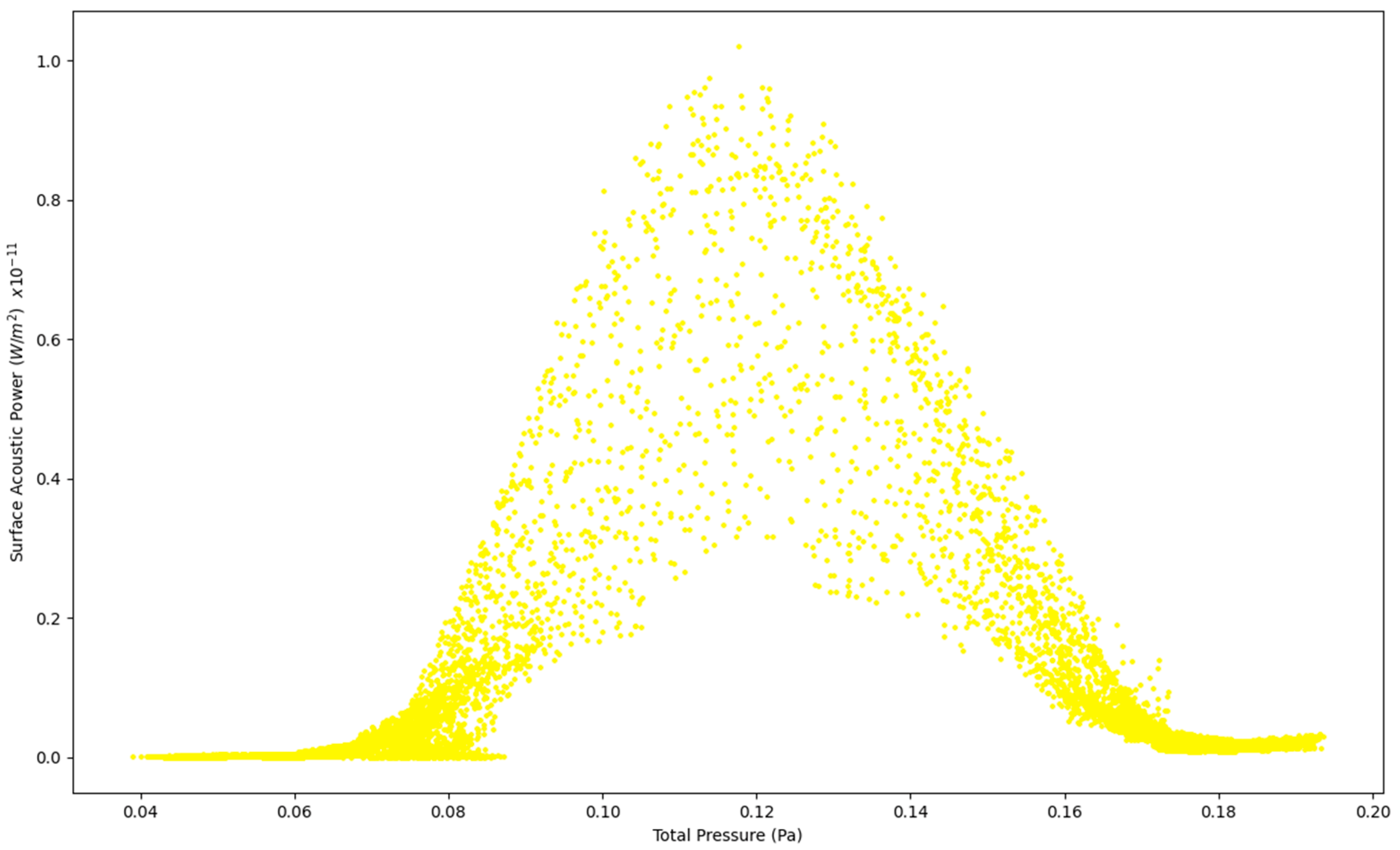
3.2. Surface Acoustic Power for Healthy Lungs and Infected Lungs at the Larynx





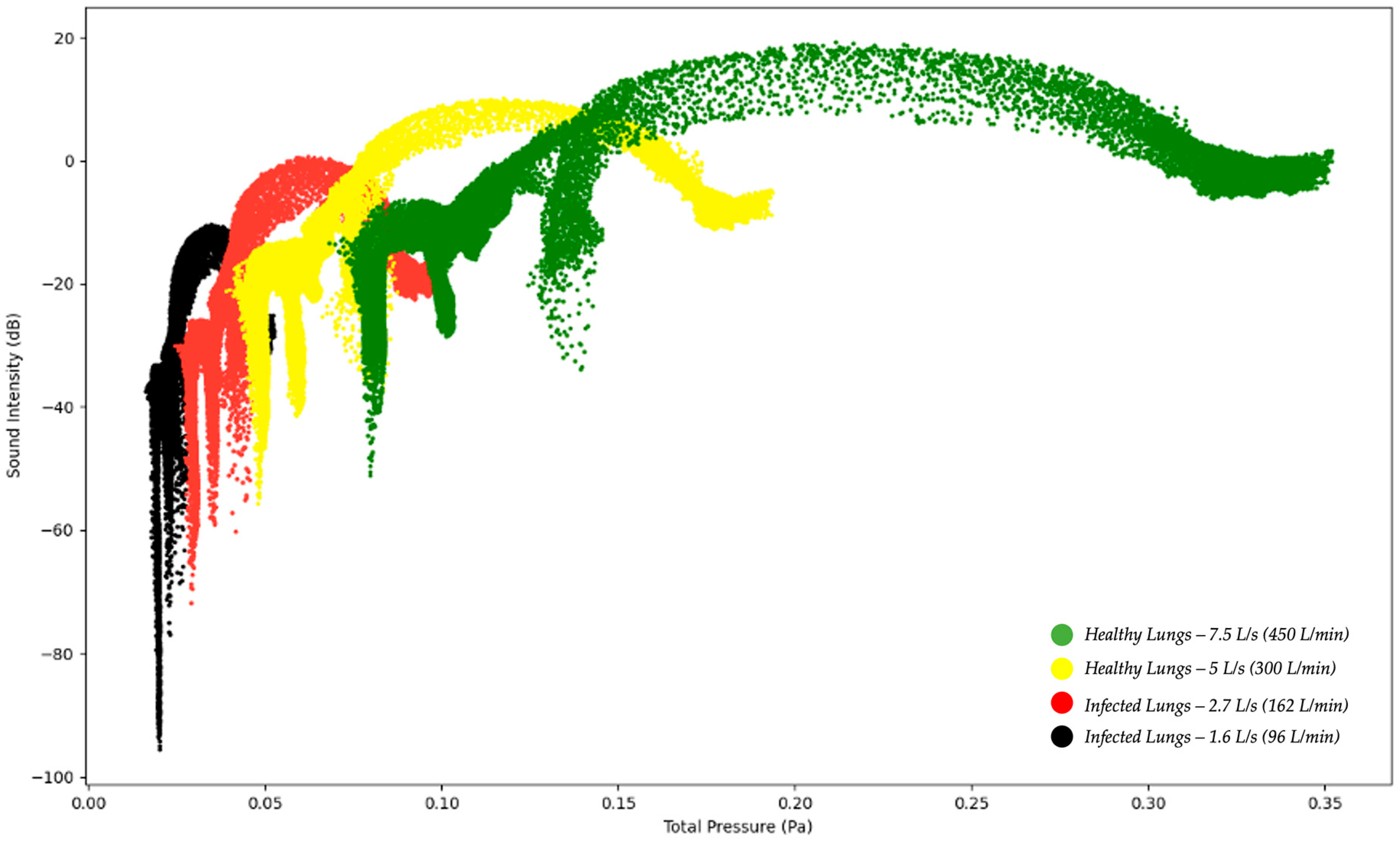
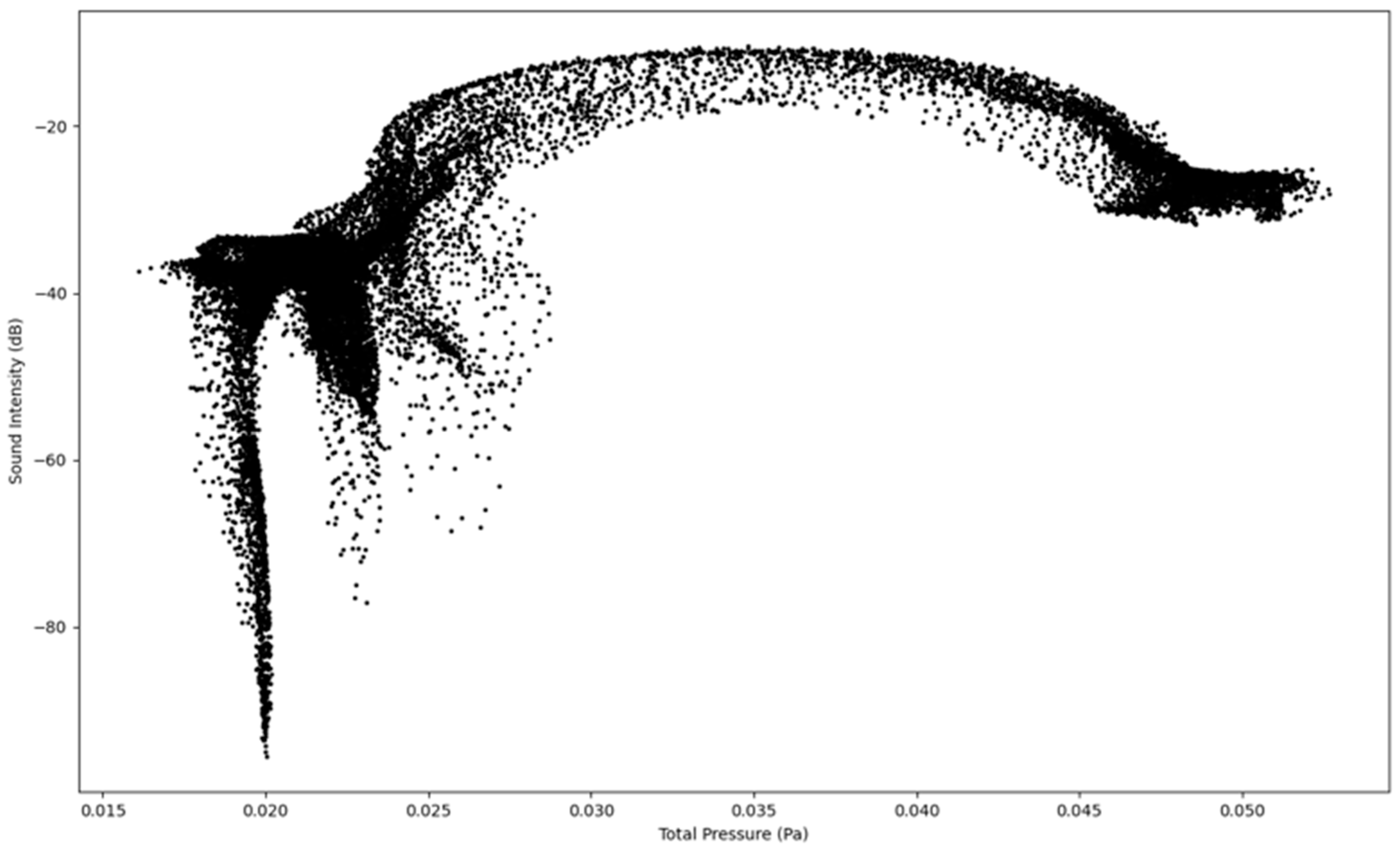
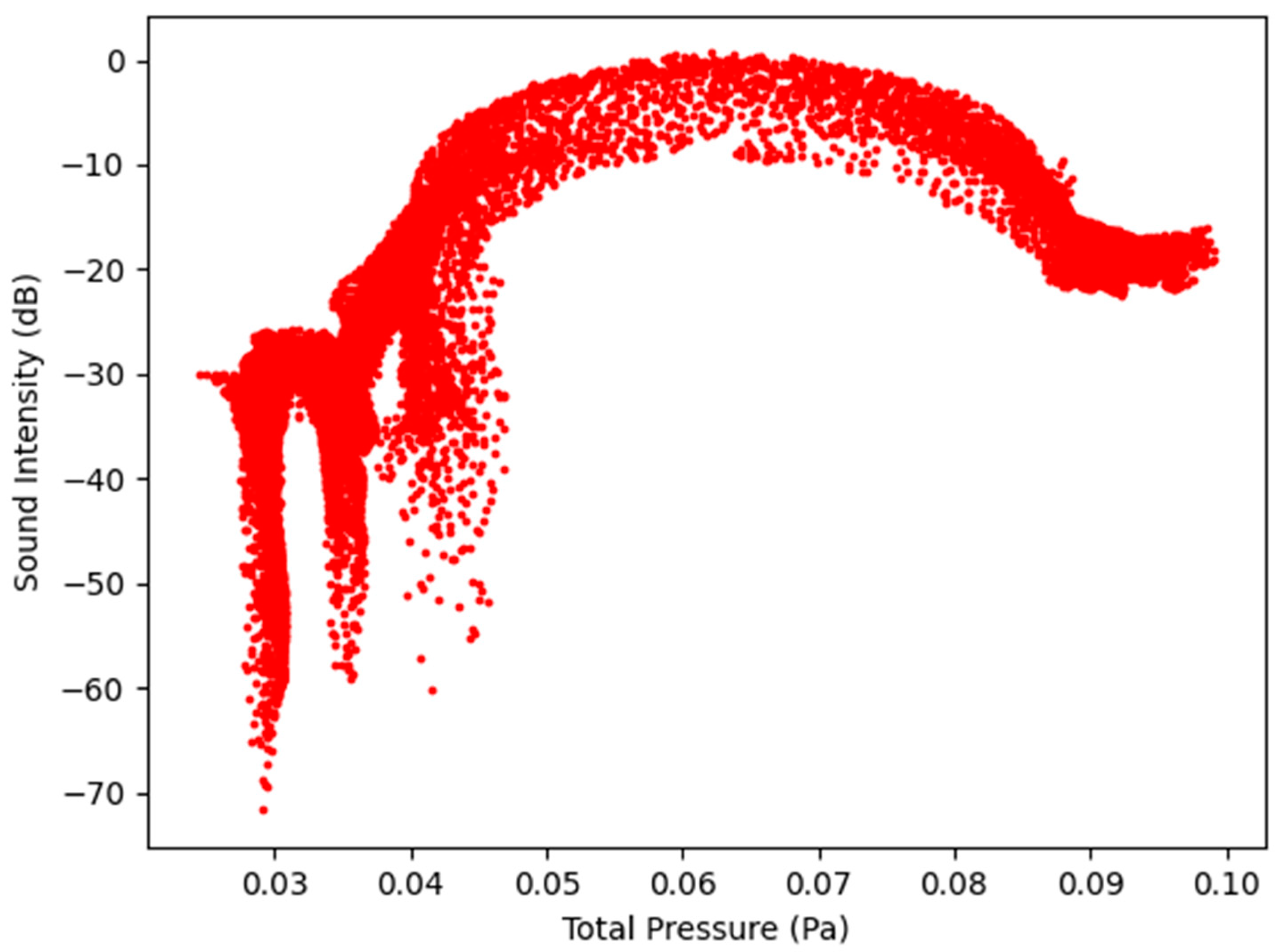
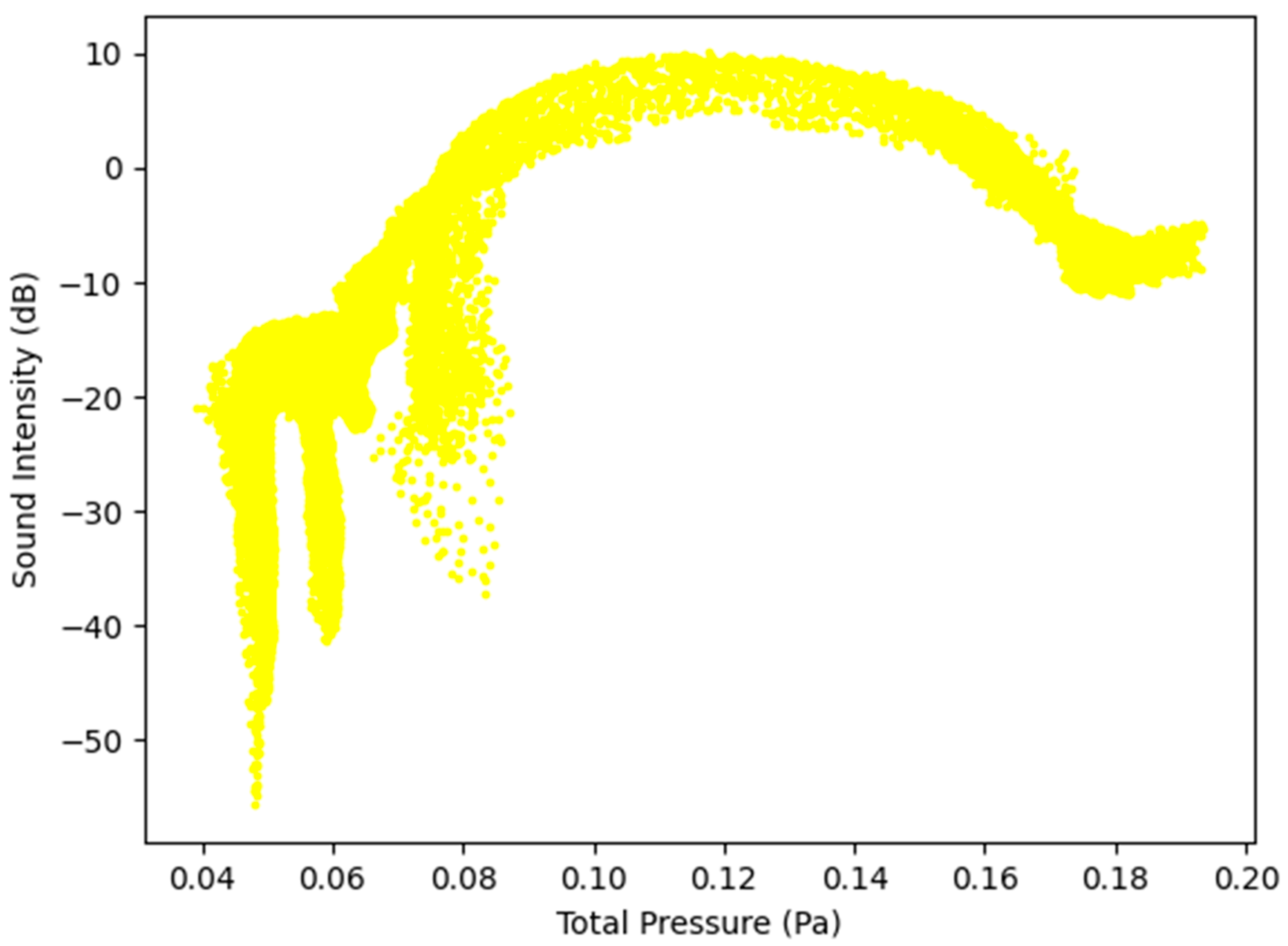
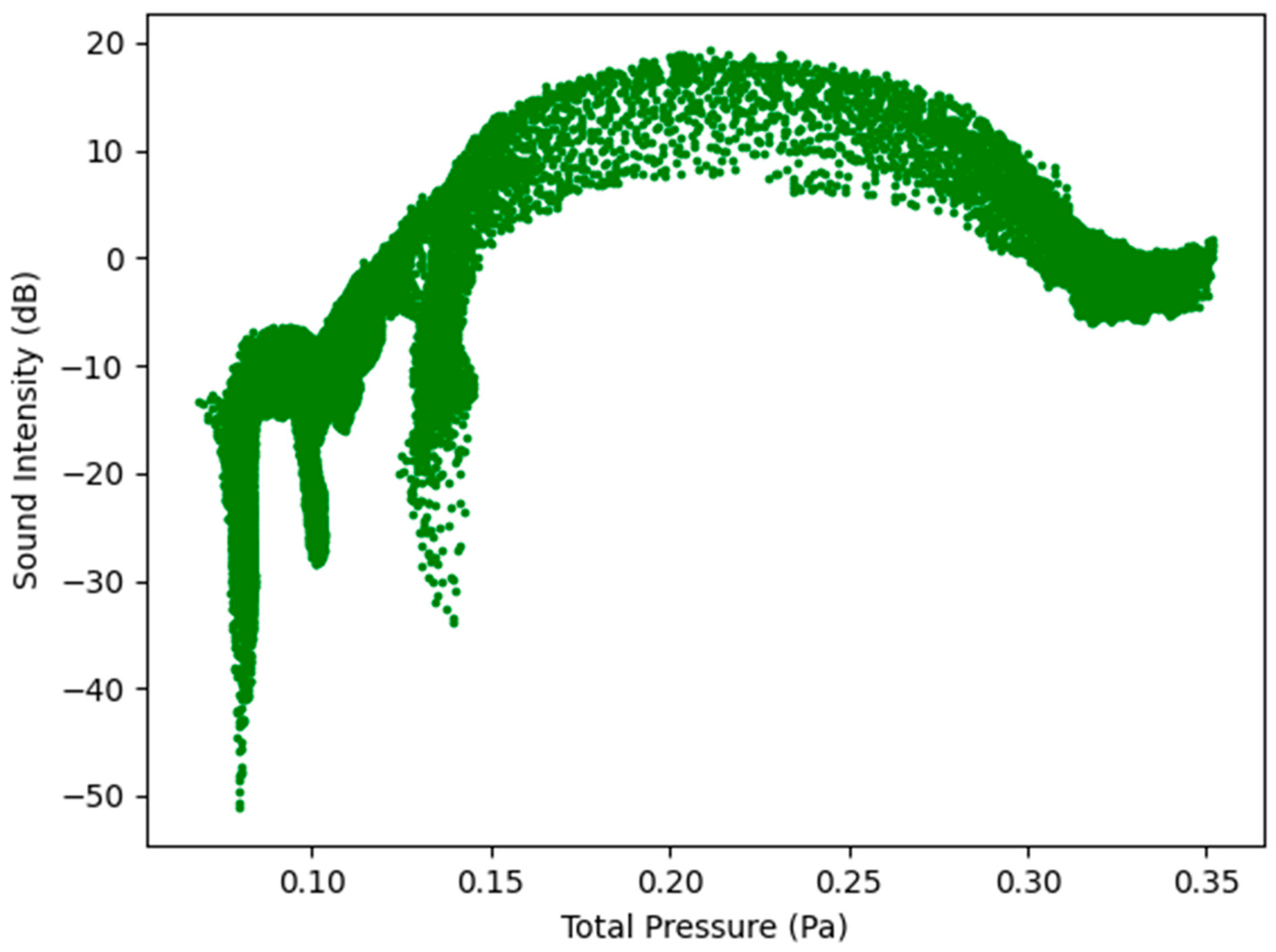
3.3. Sound Intensity Level for Healthy Lungs and Infected Lungs at the Larynx





4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations/Nomenclature
| CFD | Computational Fluid Dynamics | |
| CHPC | Centre for High Performance Computing | |
| dB | Decibel | |
| IBM | International Business Machines | |
| ICEM | Integrated Computer-aided Engineering and Manufacturing | |
| INC | Incorporated | |
| LES | Large Eddy Simulation | |
| NCSU | North Carolina State University | |
| PHRU | Perinatal HIV Research Unit | |
| PU | Polyurethane | |
| RANS | Reynolds Averaged Navier-Stokes | |
| TB | Tuberculosis | |
| USA | United States of America | |
| Acceleration (m/s2) | ||
| Local speed of sound (m/s) | ||
| CD | Drag coefficient, defined different ways (dimensionless) | |
| cp, cv | Heat capacity at constant pressure, volume (J/kg-K) | |
| Diameter; dp, Dp particle diameter (m) | ||
| Force vector (N) | ||
| FD | Drag force (N) | |
| Gravitational acceleration (m/s2); standard values = 9.80665 m/s2) | ||
| Gk | Generation of turbulence kinetic energy due to the mean velocity gradients | |
| Gb | Generation of turbulence kinetic energy due to the buoyancy | |
| I | Sound Intensity (W/m2) | |
| Iref | Reference Sound Intensity (W/m2) | |
| k | Kinetic energy per unit mass (J/kg) | |
| k | Reaction rate constant, e.g., k1, k−1, kf,r, kb,r (units vary) | |
| kB | Boltzmann constant (1.38 × 10−23 J/molecule-K) | |
| k, kc | Mass transfer coefficient (units vary); also K, Kc | |
| l, L | Length scale (m, cm) | |
| Lp | Sound Pressure (dB) | |
| m | Mass (g, kg) | |
| M | Mach number ratio of fluid velocity magnitude to local speed of sound (dimensionless) | |
| p | Pressure (Pa, atm, mm Hg) | |
| PA | Acoustic power due to the unit volume of isotropic turbulence (W/m3) | |
| Pref | Reference Acoustic Power (W/m3) | |
| r | Radius (m) | |
| Re | Reynolds number ratio of inertial forces to viscous forces (dimensionless) | |
| s | Species entropy; s0, standard state entropy (J/kgmol-K) | |
| Si,j | Mean rate-of-strain tensor (s−1) | |
| T | Temperature (K) | |
| t | Time (s) | |
| u | Turbulence Velocity | |
| V | Volume (m3) | |
| YM | Contribution of the fluctuating dilation in compressible turbulence to the overall dissipation | |
| Overall velocity vector (m/s) | ||
| Thermal diffusivity (m2/s) | ||
| Volume fraction (dimensionless) | ||
| Coefficient of thermal expansion (K−1) | ||
| Ratio of specific heats, cp, cv (dimensionless) | ||
| Change in variable, final—initial | ||
| Delta function (units vary) | ||
| Turbulent dissipation rate (m2/s3) | ||
| Void fraction (dimensionless) | ||
| Effectiveness factor (dimensionless) | ||
| Wavelength (m, nm) | ||
| Dynamic viscosity (cP, Pa-s) | ||
| v | Kinematic viscosity (m2/s) | |
| v′, v″ | Stoichiometric coefficients for reactants, products (dimensionless) | |
| Density (kg/m3) | ||
| Stefan-Boltzmann constant (5.67 × 108 W/m2-K4) | ||
| Surface tension (kg/m, dyn/cm) | ||
| 2 | Scattering coefficient (m−1) | |
| σk | Turbulent Prandtl number for k | |
| σε | Turbulent Prandtl number for | |
| Stress tensor (Pa) | ||
| Shear stress (Pa) | ||
| Time scale, (s) | ||
| Equivalence ratio (dimensionless) | ||
| w | Specific dissipation rate (s−1) | |
References
- Purwanto, B.; Sabrina, M.; Rusjadi, D. The difference between several methods of sound power level for determining the sound energy emitted by a sound source. In Journal of Physics: Conference Series; Institute of Physics Publishing: Bristol, UK, 2020. [Google Scholar] [CrossRef]
- Munson, B.; Okiishi, T.; Huebsch, W.; Rothmayer, A. Fundamentals of Fluid Mechanics; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013. [Google Scholar]
- Lee, B.K. Computational fluid dynamics in cardiovascular disease. Korean Circ. J. 2011, 41, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, B.; Santiago, J.L.; Martilli, A.; Palacios, M.; Kirchner, F. CFD modeling of reactive pollutant dispersion in simplified urban configurations with different chemical mechanisms. Atmos. Chem. Phys. 2016, 16, 12143–12157. [Google Scholar] [CrossRef]
- Lim, T.; Cho, J.; Kim, B.S. The influence of ward ventilation on hospital cross infection by varying the location of supply and exhaust air diffuser using CFD. J. Asian Archit. Build. Eng. 2010, 9, 259–266. [Google Scholar] [CrossRef]
- Powell, N.B.; Mihaescu, M.; Mylavarapu, G.; Weaver, E.M.; Guilleminault, C.; Gutmark, E. Patterns in pharyngeal airflow associated with sleep-disordered breathing. Sleep Med. 2011, 12, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Faizal, W.M.; Ghazali, N.N.N.; Khor, C.Y.; Badruddin, I.A.; Zainon, M.Z.; Yazid, A.A.; Razi, R.M. Computational fluid dynamics modelling of human upper airway: A review. Comput. Methods Programs Biomed. 2020, 196, 105627. [Google Scholar] [CrossRef] [PubMed]
- Bohadana, A.; Izbicki, G.; Kraman, S.S. Fundamentals of Lung Auscultation. N. Engl. J. Med. 2014, 370, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, M.; Madabhavi, I.; Niranjan, N.; Dogra, M. Auscultation of the respiratory system. In Annals of Thoracic Medicine; Wolters Kluwer Medknow Publications: Mumbai, India, 2015; Volume 10, pp. 158–168. [Google Scholar] [CrossRef]
- Shilpa, N.; Veena, H.C. Peak flow meter and digital spirometer: A comparative study of peak expiratory flow rate values. Natl. J. Physiol. Pharm. Pharmacol. 2020, 10, 208. [Google Scholar] [CrossRef]
- Sitalakshmi, R.; Poornima, K.N.; Karthick, N. The peak expiratory flow rate (PEFR): The effect of stress in a geriatric population of Chennai-a pilot study. J. Clin. Diagn. Res. 2013, 7, 409–410. [Google Scholar] [CrossRef]
- Gurumurthy, A.; Kleinstreuer, C. Improving Pulmonary Nano-Therapeutics Using Helical Aerosol Streams—An In-Silico Study. J. Biomech. Eng. 2021, 143, 111001. [Google Scholar] [CrossRef] [PubMed]
- Su, W.C.; Cheng, Y. Fiber deposition pattern in two human respiratory tract replicas. Inhal. Toxicol. 2006, 18, 749–760. [Google Scholar] [CrossRef] [PubMed]
- Roache, P.J. Perspective: A method for uniform reporting of grid refinement studies. J. Fluids Eng. 1994, 116, 405–413. [Google Scholar] [CrossRef]
- Zhou, B.; Zhang, X. Lung mass density analysis using deep neural network and lung ultrasound surface wave elastography. Ultrasonics 2018, 89, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Obando, L.M.G.; López, A.L.; Ávila, C.L. Normal values of the maximal respiratory pressures in healthy people older than 20 years old in the city of Manizales—Colombia. Colomb. Med. 2023, 43, 119–125. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4001942/pdf/1657-9534-cm-43-02-00119.pdf (accessed on 21 January 2023). [CrossRef]
- ANSYS Fluent Technical Staff. ANSYS Fluent 2021R2 Theory Guide; ANSYS Inc.: Canonsburg, PA, USA, 2021. [Google Scholar]
- Oliveira, A.; Marques, A. Respiratory sounds in healthy people: A systematic review. Respir. Med. 2014, 108, 550–570. [Google Scholar] [CrossRef] [PubMed]
- Gavriely, N.; Cugell, D.W. Airflow effects on amplitude and spectral content of normal breath sounds. J. Appl. Physiol. 1996, 80, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Pasterkamp, H.; Sanchez, I. Effect of gas density on respiratory sounds. Am. J. Respir. Crit. Care Med. 1996, 153, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Wang, C. (Ed.) Chapter 3 Airflow in the respiratory system. In Interface Science and Technology; Inhaled Particles; Elsevier: Amsterdam, The Netherlands, 2005; Volume 5, pp. 31–54. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Position | f1 | f2 | f3 | GCI12 | GCI23 | Asymptotic Range |
|---|---|---|---|---|---|---|
| Position 1 | 6.5 × 10−28 | 6.4 × 10−28 | 5.8 × 10−28 | 0.003841615 | 0.0234375 | 1.016 |
| Position 2 | 6.6 × 10−28 | 6.38 × 10−28 | 5.6 × 10−28 | 0.01636905 | 0.06003695 | 1.034 |
| Position 3 | 6.4 × 10−28 | 6.3 × 10−28 | 5.7 × 10−28 | 0.00390625 | 0.02380952 | 1.016 |
| Position | f1 | f2 | f3 | GCI12 | GCI23 | Asymptotic Range |
|---|---|---|---|---|---|---|
| Position 1 | 2.36 × 10−27 | 2.40 × 10−27 | 2.40 × 10−27 | 0.025207785 | 0.001032223 | 0.981 |
| Position 2 | 7.39 × 10−28 | 7.81 × 10−28 | 7.86 × 10−28 | 0.081109195 | 0.00851182 | 0.945 |
| Time Step (s) | ∆x (m) | Velocity Magnitude | CFL | Surface Acoustic Power (W/m2) | Convergence Achieved |
|---|---|---|---|---|---|
| 1 | 0.003 | 0.0016 | 0.5333 | 2.00 × 10−27 | No |
| 0.1 | 0.0533 | 2.36 × 10−27 | Yes | ||
| 0.01 | 0.0053 | 2.40 × 10−27 | Yes | ||
| 0.001 | 0.0005 | 2.40 × 10−27 | Yes |
| Material Properties | ||
| Fluid Material | Air | Density—1.225 kg/m3 |
| Solid Material—Adventitia (Outer Membrane) | Representative Material | Density—949.79 kg/m3 |
| Boundary Conditions | ||
| Boundary | Type | Condition |
| Oral Cavity | Pressure Outlet | Atmospheric Pressure |
| Respiratory Bronchiole | Velocity Inlet | Case Dependent |
| Wall (Oropharynx, Larynx, Trachea, Lobar Bronchus) | Wall Boundary | No Slip |
| Solver Settings | ||
| Number of Time Steps | 100 | |
| Time Step Size (s) | 0.1 | |
| Max Iterations/Time Step | 20 | |
| Pressure Velocity Coupling—Type | Simple | |
| Discretization Scheme—Pressure | 2nd Order | |
| Discretization Scheme—Momentum | 2nd Order Upwind | |
| Discretization Scheme—Turbulent Kinetic Energy | 1st Order Upwind | |
| Discretization Scheme—Turbulent Dissipation Rate | 1st Order Upwind | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makhanya, K.M.; Connell, S.; Bhamjee, M.; Martinson, N. The Use of Computational Fluid Dynamics for Assessing Flow-Induced Acoustics to Diagnose Lung Conditions. Math. Comput. Appl. 2023, 28, 64. https://doi.org/10.3390/mca28030064
Makhanya KM, Connell S, Bhamjee M, Martinson N. The Use of Computational Fluid Dynamics for Assessing Flow-Induced Acoustics to Diagnose Lung Conditions. Mathematical and Computational Applications. 2023; 28(3):64. https://doi.org/10.3390/mca28030064
Chicago/Turabian StyleMakhanya, Khanyisani Mhlangano, Simon Connell, Muaaz Bhamjee, and Neil Martinson. 2023. "The Use of Computational Fluid Dynamics for Assessing Flow-Induced Acoustics to Diagnose Lung Conditions" Mathematical and Computational Applications 28, no. 3: 64. https://doi.org/10.3390/mca28030064