
Clinical and Histopathologic Profile of Patients with Cutaneous Metastasis in a Tertiary Hospital in the Philippines
Abstract
:1. Introduction
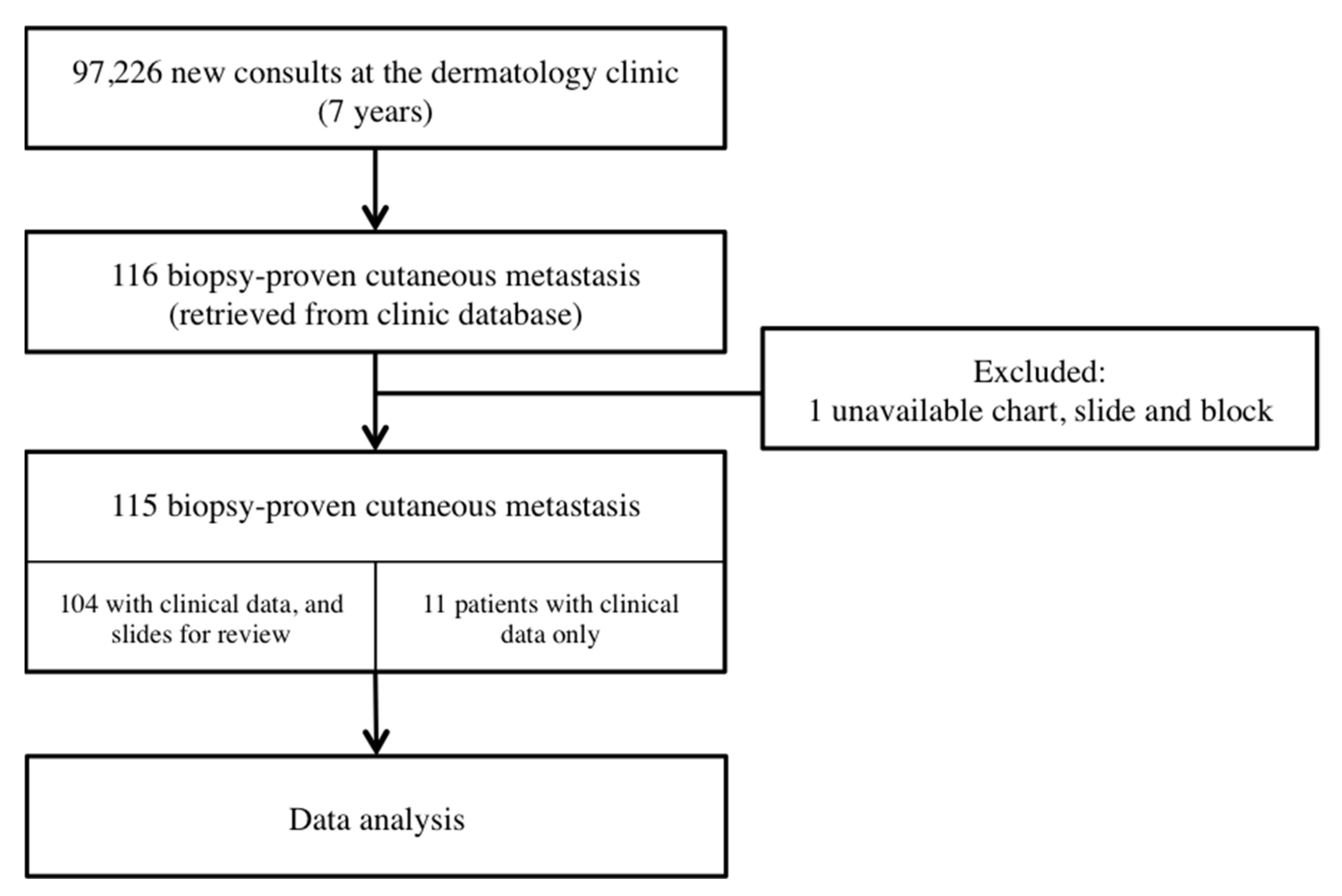
2. Methodology
2.1. Data Collection
2.2. Plan for Analysis
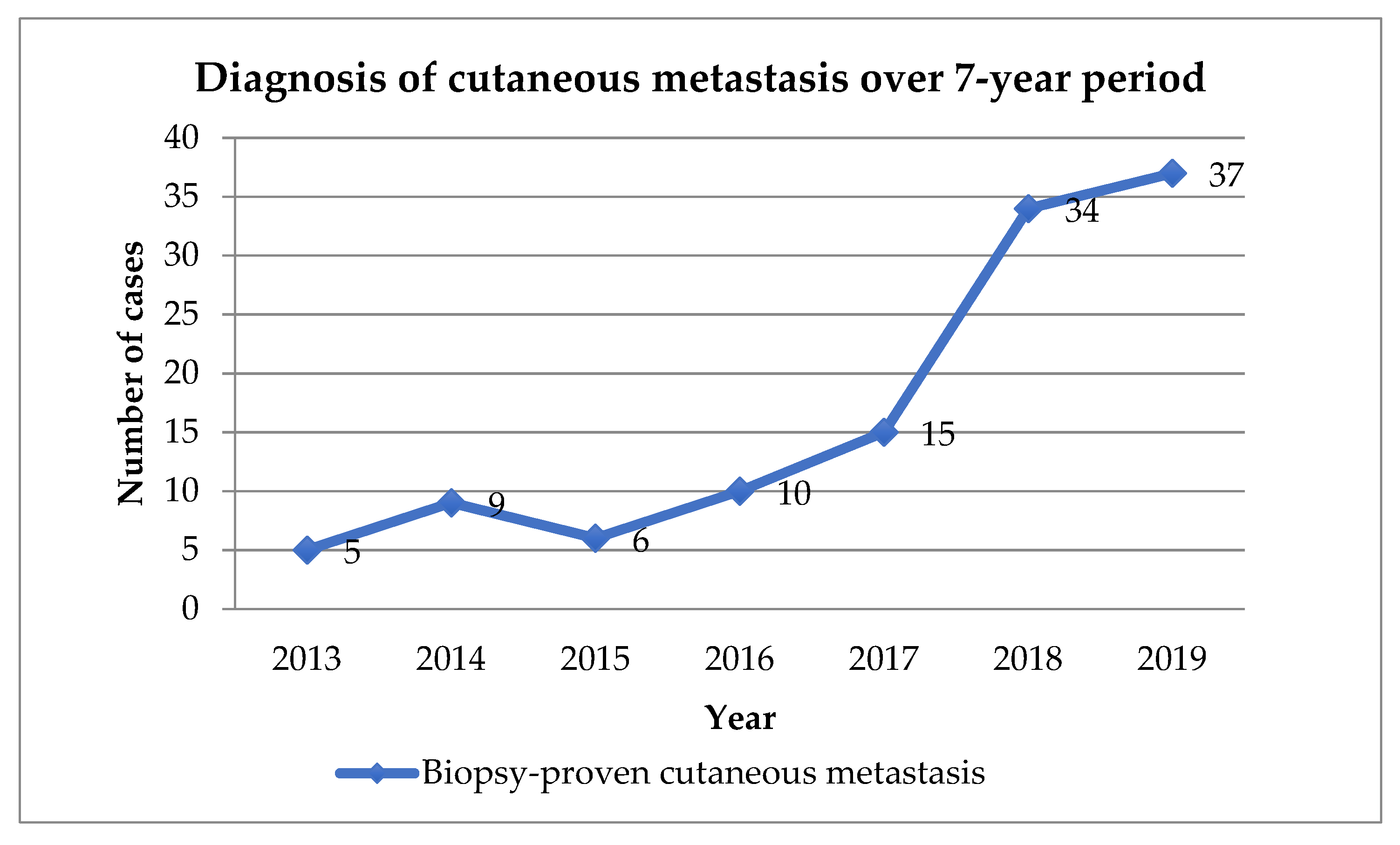
3. Results
3.1. Clinical Features
3.1.1. Patient Characteristics and Location of Primary Malignancy
3.1.2. Clinical Presentation of Skin Lesions
3.1.3. Sequence of Diagnosis between Primary Cancer and Cutaneous Metastases
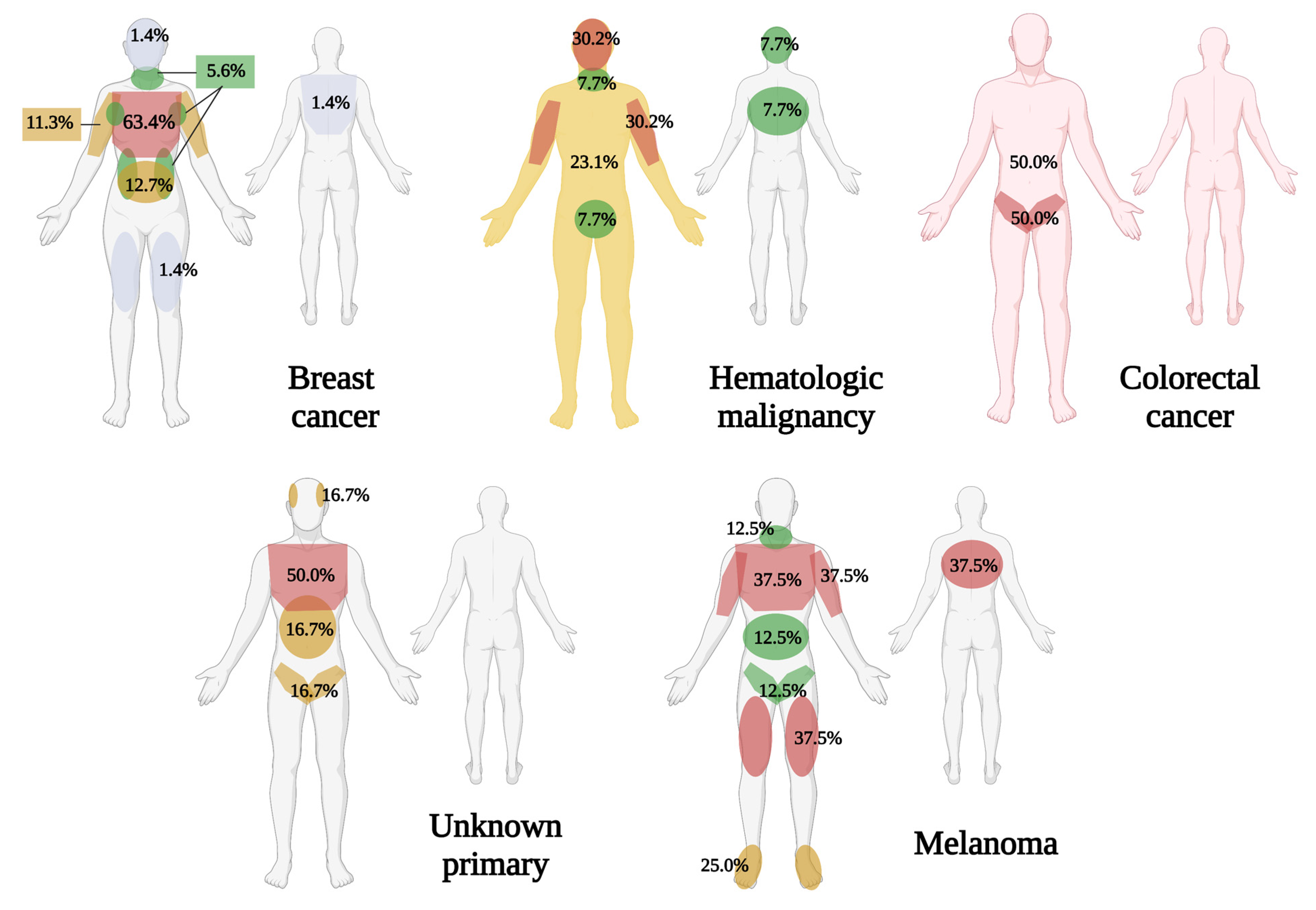
3.2. Location
3.3. Treatment
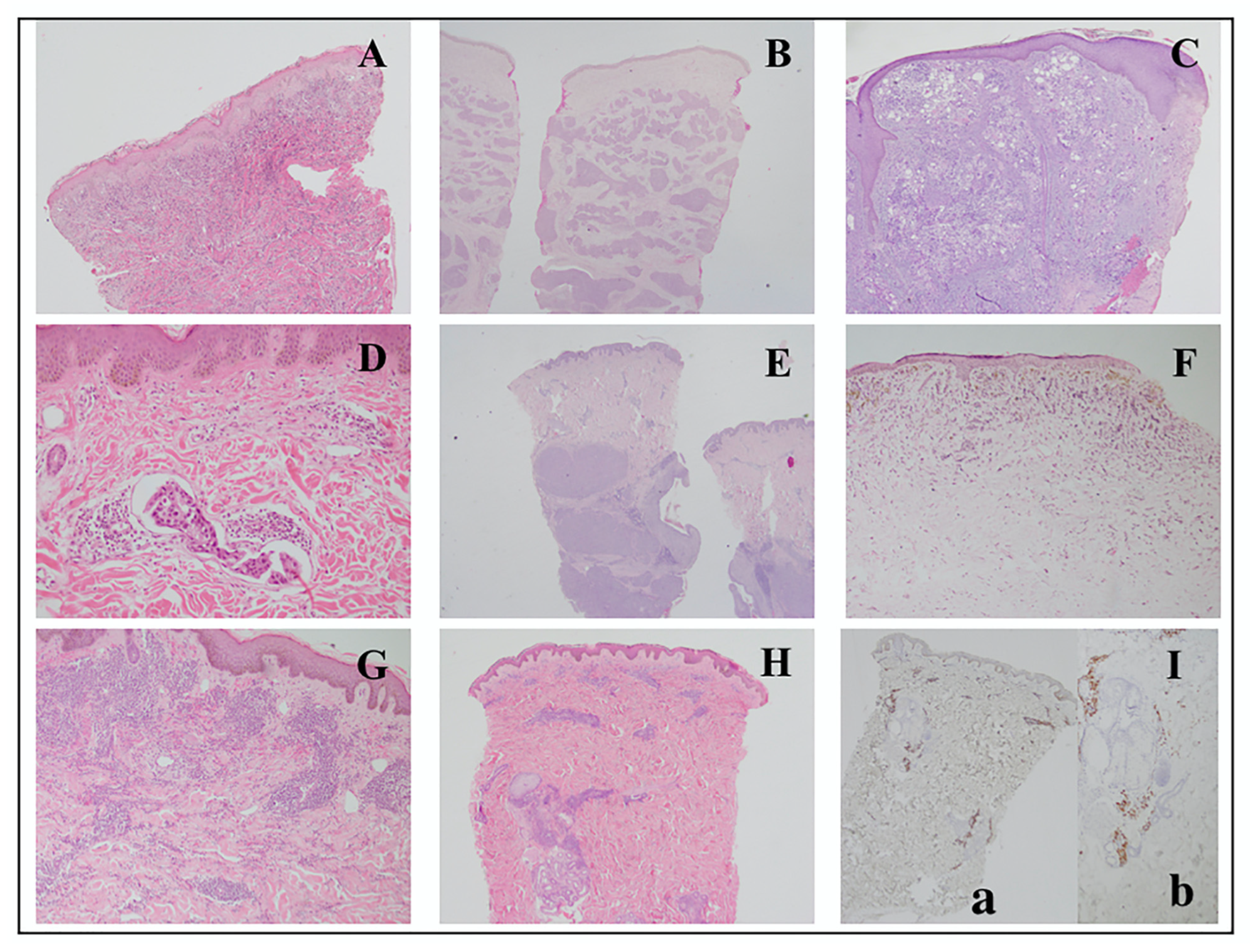
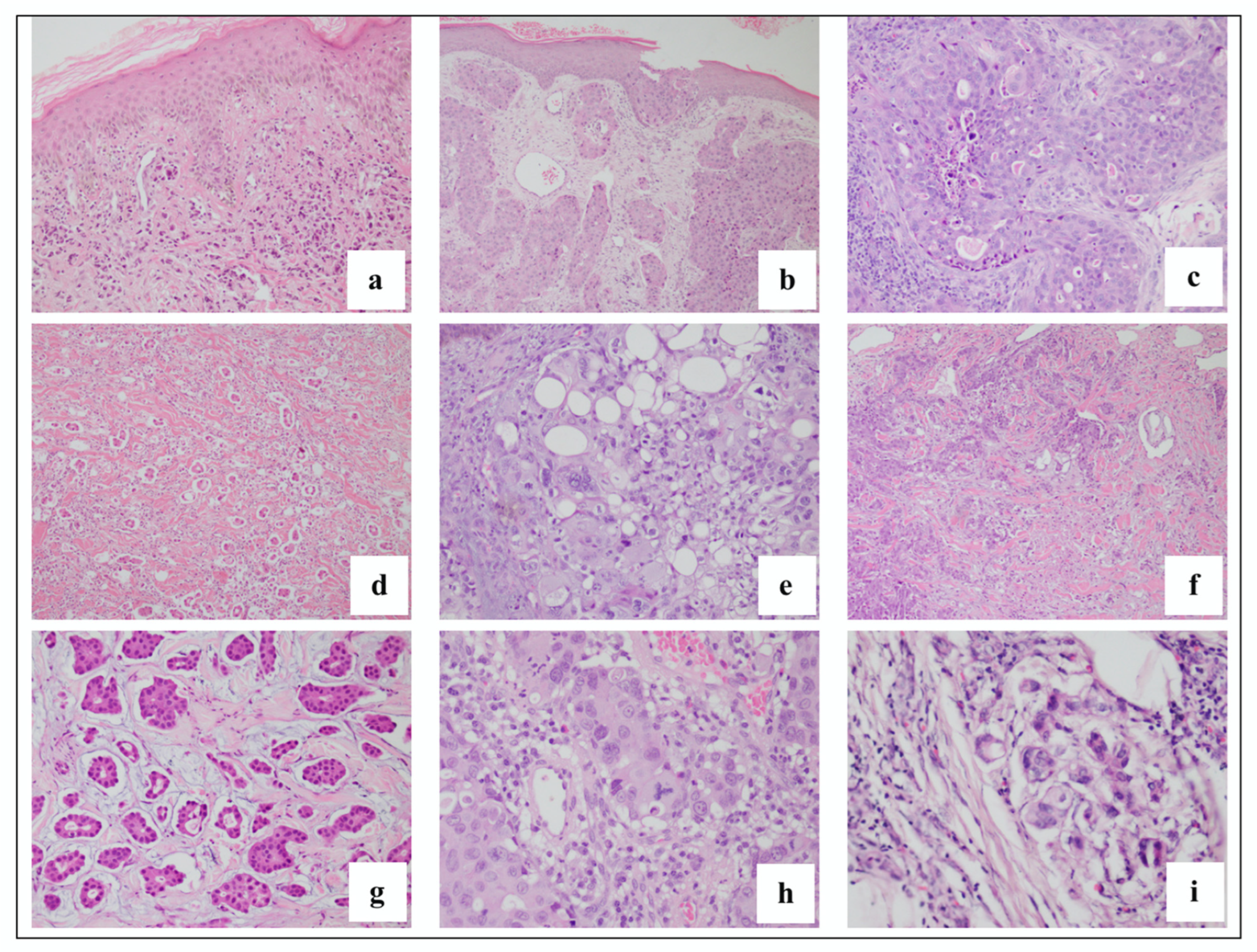
3.4. Histologic Features
3.5. Concurrence of Diagnosis
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saeed, S.; Keehn, C.A.; Morgan, M.B. Cutaneous metastasis: A clinical, pathological, and immunohistochemical appraisal. J. Cutan. Pathol. 2004, 31, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Alcaraz, I.; Cerroni, L.; Rutten, A.; Kutzner, H.; Requena, L. Cutaneous metastases from internal malignancies: A clinicopathologic and immunohistochemical review. Am. J. Dermatopathol. 2012, 34, 347–393. [Google Scholar] [CrossRef] [PubMed]
- Nibhoria, S.; Tiwana, K.K.; Kaur, M.; Kumar, S. A Clinicopathological and Immunohistochemical Correlation in Cutaneous Metastases from Internal Malignancies: A Five-Year Study. J. Skin Cancer 2014, 2014, 793937. [Google Scholar] [CrossRef] [PubMed]
- Krathen, R.A.; Orengo, I.F.; Rosen, T. Cutaneous metastasis: A meta-analysis of data. South Med. J. 2003, 96, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Sariya, D.; Ruth, K.; Adams-McDonnell, R.; Cusack, C.; Xu, X.; Elenitsas, R.; Seykora, J.; Pasha, T.; Zhang, P.; Baldassano, M.; et al. Clinicopathologic Correlation of Cutaneous Metastases. Arch. Dermatol. 2007, 143, 613–620. [Google Scholar] [CrossRef]
- Brownstein, M.H.; Helwig, E.B. Patterns of Cutaneous Metastasis. Arch. Dermatol. 1972, 105, 862–868. [Google Scholar] [CrossRef]
- Hussein, M.R.A. Skin metastasis: A pathologist’s perspective. J. Cutan. Pathol. 2010, 37, e1–e20. [Google Scholar] [CrossRef]
- Fernandez-Flores, A. Cutaneous metastases: A study of 78 biopsies from 69 patients. Am. J. Dermatopathol. 2010, 32, 222–239. [Google Scholar] [CrossRef]
- El Khoury, J.; Khalifeh, I.; Kibbi, A.G.; Abbas, O. Cutaneous metastasis: Clinicopathological study of 72 patients from a tertiary care center in Lebanon. Int. J. Dermatol. 2014, 53, 147–158. [Google Scholar] [CrossRef]
- Kaplan, V.; Morales, C.; Bobadilla, F.; Fernández, J.; Segovia, L.; Vera, V.; Sanhueza, I. Epidemiologic and Histopathologic Characterization of Cutaneous Metastases in Patients Who Visited 2 Hospitals in Santiago de Chile between 2005 and 2017. Actas Dermosifiliogr. 2019, 110, 220–226. [Google Scholar] [CrossRef]
- Perez, K.B.A. Skin Metastasis from Laryngeal Carcinoma: A Case Report. Philipp. Sci. J. 2003, 36, 50–54. [Google Scholar]
- Cañal, J.P.A. Dermal Metastasis from Nasopharyngeal Carcinoma: A Rare Form of Metastasis. Philipp. J. Otolaryngol. Neck Surg. 2011, 26, 42–45. [Google Scholar] [CrossRef]
- Hu, S.C.S.; Chen, G.S.; Lu, Y.W.; Wu, C.S.; Lan, C.C.E. Cutaneous metastases from different internal malignancies: A clinical and prognostic appraisal. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Benmously, R.; Souissi, A.; Badri, T.; Ben Jannet, S.; Marrak, H.; Mokhtar, I.; Fenniche, S. Cutaneous metastases from internal cancers. Acta Derm. Venereol. 2008, 17, 167–170. [Google Scholar]
- Gan, E.Y.; Chio, M.T.W.; Tan, W.P. A retrospective review of cutaneous metastases at the National Skin Centre Singapore. Australas. J. Dermatol. 2015, 56, 1–6. [Google Scholar] [CrossRef]
- Wong, C.Y.B.; Helm, M.A.; Helm, T.N.; Zeitouni, N. Patterns of skin metastases: A review of 25years’ experience at a single cancer center. Int. J. Dermatol. 2014, 53, 56–60. [Google Scholar] [CrossRef]
- Chopra, R.; Chhabra, S.; Samra, S.G.; Thami, G.P.; Punia, R.P.S.; Mohan, H. Cutaneous metastases of internal malignancies: A clinicopathologic study. Indian J. Dermatol. Venereol. Leprol. 2010, 76, 125–131. [Google Scholar] [CrossRef]
- Schulman, J.M.; Pauli, M.L.; Neuhaus, I.M.; Rodriguez, R.S.; Taravati, K.; Shin, U.S.; McCalmont, T.H.; Rosenblum, M.D. The distribution of cutaneous metastases correlates with local immunologic milieu. J. Am. Dermatol. 2016, 74, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Panjwani, P.K.; Rajalakshmi, T.; Incham, K.Y.; Anuradha, A. Interstitial pattern of cutaneous metastasis and its diagnosic pitfalls: A report of three cases. Indian J. Dermatopathol. Diagn. Dermatol. 2018, 5, 120–123. [Google Scholar] [CrossRef]
- Varricchi, G.; Rosaria, M.; Loffredo, S.; Lucarini, V.; Marone, G. Eosinophils: The unsung heroes in cancer ? Oncoimmunology 2018, 7, e1393134. [Google Scholar] [CrossRef] [Green Version]
- Habermehl, G.; Ko, J. Cutaneous Metastasis: A Review and Diagnostic Approach to Tumors of Unknown Origin. Arch. Pathol. Lab. Med. 2018, 143, 943–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spratt, D.E.; Spratt, E.A.G.; Wu, S.; DeRosa, A.; Lee, N.Y.; Lacouture, M.E.; Barker, C.A. Efficacy of skin-directed therapy for cutaneous metastases from advanced cancer: A meta-analysis. J. Clin. Oncol. 2014, 32, 3144–3155. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Total (N = 115) | Male (n = 26) | Female (n = 89) |
|---|---|---|---|
| N (%) | n (%) | n (%) | |
| Breast | 71 (61.7) | 0 | 71 (79.8) |
| Hematologic | 13 (11.3) | 7 (26.9) | 6 (6.7) |
| Skin (melanoma) | 8 (7.0) | 4 (15.4) | 4 (4.5) |
| Unknown | 6 (5.2) | 4 (15.4) | 2 (2.2) |
| Colorectal | 4 (3.5) | 2 (7.7) | 2 (2.2) |
| Thyroid | 2 (1.7) | 1 (3.8) | 1 (1.1) |
| Bladder | 1 (0.9) | 1 (3.8) | 0 |
| Breast and Lung | 1 (0.9) | 1 (3.8) | 0 |
| Breast and Parotid | 1 (0.9) | 0 | 1 (1.1) |
| Cervix | 1 (0.9) | 0 | 1 (1.1) |
| Esophagus | 1 (0.9) | 1 (3.8) | 0 |
| Lung | 1 (0.9) | 1 (3.8) | 0 |
| Nasopharyngeal | 1 (0.9) | 1 (3.8) | 0 |
| Pancreas | 1 (0.9) | 1 (3.8) | 0 |
| Renal | 1 (0.9) | 1 (3.8) | 0 |
| Soft tissue | 1 (0.9) | 1 (3.8) | 0 |
| Vulva | 1 (0.9) | 0 | 1 (1.1) |
| N (%) | |
|---|---|
| Symptoms associated with skin lesions at presentation | |
| None | 65 (56.5) |
| Pruritus | 16 (13.9) |
| Infection (yellowish crusts, draining abscess) | 14 (12.2) |
| Pain, tenderness | 12 (10.4) |
| Lymphedema | 5 (4.3) |
| Not known | 2 (1.7) |
| Hydrocele | 1 (0.9) |
| Clinical presentation of lesions | |
| Number of lesions | |
| Multiple | 106 (92.2) |
| Solitary | 9 (7.8) |
| Primary lesions | 106 |
| Nodules | 58 (50.4) |
| Papules and plaques | 47 (40.9) |
| Macules/patches | 7 (6.1) |
| Mass/tumor | 3 (2.6) |
| Secondary changes | |
| None | 91 (79.1) |
| Serous and sero-purulent crusts | 12 (10.4) |
| Erosion and ulceration | 6 (5.2) |
| Hemorrhagic crusts and eschar | 3 (2.6) |
| Not indicated | 3 (2.6) |
| General Pattern | N (%) N = 122 |
|---|---|
| Infiltrative | 32 (26.2) |
| Intravascular | 24 (19.7) |
| Infiltrative | 6 (25.0) |
| Nodular | 2 (8.3) |
| Top-heavy | 1 (4.2) |
| Nodular | 23 (18.9) |
| Diffuse | 17 (13.9) |
| Infiltrative | 4 (23.5) |
| Nodular | 1 (5.9) |
| Top-heavy | 1 (5.9) |
| Nodular and infiltrative | 12 (9.8) |
| Top heavy | 7 (5.7) |
| Nodular | 2 (28.6) |
| Infiltrative | 1 (14.3) |
| Bottom Heavy | 6 (4.9) |
| Nodular | 2 (33.3) |
| Infiltrative | 1 (16.7) |
| Intravascular | 1 (16.7) |
| Superficial and deep perivascular | 1 (0.8) |
| Patient Code | Primary Site | Immunohistochemistry Studies Performed |
|---|---|---|
| 18 | Nasopharyngeal | AE1/AE3—diffuse, strong, cytoplasmic; CEA—negative |
| 25 | Breast | CK7—focal, strong, membranous |
| 39 | Melanoma | S100—diffuse, moderate stain, cytoplasmic |
| 61 | Breast | CK7—diffuse, strong, cytoplasmic; CK20—negative; CEA—negative |
| 62 | Breast | CK7—diffuse, strong, cytoplasmic; CEA—focal scattered staining of cells, cytoplasmic |
| 64 | Unknown | CK7—diffuse, strong, cytoplasmic |
| 69 | Breast | CK7 strong, cytoplasmic, focal |
| 71 | Hematologic | CD20—negative; CD3—negative; MPO—diffuse, strong, cytoplasmic |
| 81 | Breast and Lung | CD34—negative, but highlights vascularization; CK7—negative; CEA-negative; CD10—scattered staining; ER—diffuse, strong, nuclear |
| 89 | Hematologic | MPO—scattered staining, cytoplasmic; CD3—diffuse, strong, cytoplasmic; CD20—negative; CD10—strong, diffuse, cytoplasmic; CD1a—negative |
| 91 | Melanoma | HMB45—diffuse, strong, cytoplasmic |
| 93 | Melanoma | HMB45—diffuse, strong, cytoplasmic |
| 96 | Hematologic | CD7—scattered staining, weak, cytoplasmic; CD5, diffuse, strong, cytoplasmic margins; CD2—scattered, strong, dot-like pattern; CD3—diffuse strong cytoplasmic |
| 101 | Hematologic | Tdt—negative; MPO—strong, scattered, cytoplasmic |
| 105 | Breast | CK7—diffuse, strong, cytoplasmic margin; CEA—scattered, strong, cytoplasmic margin |
| 106 | Renal | AE1/AE3—strong, cytoplasmic; EMA—strong, cytoplasmic margins; CD10—strong, cytoplasmic |
| Clinical Differential Diagnosis Given along with Cutaneous Metastases | |
|---|---|
| Benign | Malignant |
| Infection Hansen’s disease, erythema nodosum Erysipelas Septic vasculitis Herpes zoster Bullous impetigo Inflammatory Morphea Radiation dermatitis Lymphedema Tumor Seborrheic keratosis Pyogenic granuloma Lymphangioma | Tumor Angiosarcoma Merkel cell carcinoma Basal cell carcinoma Squamous cell carcinoma Paget’s disease |
| Saeed et al., 2004 + [1] | Nibhoria et al., 2014 * [3] | Sariya et al., 2007 [5] | Fernandez-Flores, 2010 * [8] | El Khoury, 2014 [9] | Kaplan, 2019 + [10] | Hu et al., 2008 [13] | Benmously et al., 2008 [14] | Gan et al., 2015 [15] | Wong et al., 2014 [16] | Chopra et al., 2010 [17] | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Region | North America | Asia | North America | Europe | Middle East | South America | Asia | Africa | Asia | North America | Asia |
| Number of years reviewed | 10 | 9 | 15 | 13 | 18 | 12 | 20 | 14 | 10 | 25 | 14 |
| Patient (N) | 77 | 9 | 51 | 69 | 72 | 96 | 141 | 14 | 35 | 401 | 14 |
| Sex | |||||||||||
| Males | 75 | 4 | 21 | 32 | 22 | 38 | 61 | 8 | 14 | Not specified | 3 |
| Females | 2 | 5 | 30 | 37 | 50 | 58 | 80 | 6 | 21 | 11 | |
| Mean age (range) | 62 (38–83 y.o.) | 60 (30–72 y.o) | 62 (37–86 y.o.) | (45–90 y.o.) | 55.2 (19–81y.o.) | 67.95 (28–96 y.o.) | 60.8 (22–88 y.o) | 63.5 (53–96 y.o) | 65 (41–88 y.o) | Not specified | Not mentioned |
| Top 3 sites | Abdomen/groin | Chest Chest and abdomen Face, scalp and trunk | Upper trunk and abdomen Head and neck (Scalp) | abdomen | Chest Head and neck Back | Abdomen Extremities Thorax | Chest Abdomen Scalp | Thorax Abdomen Head and neck | Chest Pelvis scalp | Not specified | Sternum abdomen |
| Most common cancer | |||||||||||
| Male | Lung, melanoma | Non-Hodgkin’s lymphoma, Renal Cell CA | Lung | Lymphoma | Laryngeal CA | Melanoma | Breast, lung | Lung | Unknown primary | Breast (Sex unspecified) | Gastric, colon, lung |
| Female | GI, GU Breast | Breast | Breast | Breast | Breast | Breast | Breast, lung, colorectal | Breast | Breast | Breast | |
| Most common morphology | nodules | Plaques, nodules | Solitary nodules | nodules | Solitary nodule | Multiple nodules | Multiple nodules | nodules | Dermal nodules | Not specified | Solitary nodule |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumlao, J.K.G.; Cubillan, E.L.A.; Villena, J.P.D.S. Clinical and Histopathologic Profile of Patients with Cutaneous Metastasis in a Tertiary Hospital in the Philippines. Dermatopathology 2022, 9, 392-407. https://doi.org/10.3390/dermatopathology9040046
Dumlao JKG, Cubillan ELA, Villena JPDS. Clinical and Histopathologic Profile of Patients with Cutaneous Metastasis in a Tertiary Hospital in the Philippines. Dermatopathology. 2022; 9(4):392-407. https://doi.org/10.3390/dermatopathology9040046
Chicago/Turabian StyleDumlao, Jolene Kristine Gatmaitan, Eileen Liesl A. Cubillan, and Juan Paolo David S. Villena. 2022. "Clinical and Histopathologic Profile of Patients with Cutaneous Metastasis in a Tertiary Hospital in the Philippines" Dermatopathology 9, no. 4: 392-407. https://doi.org/10.3390/dermatopathology9040046