
Dupilumab-Associated Mycosis Fungoides with a CD8+ Immunophenotype
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
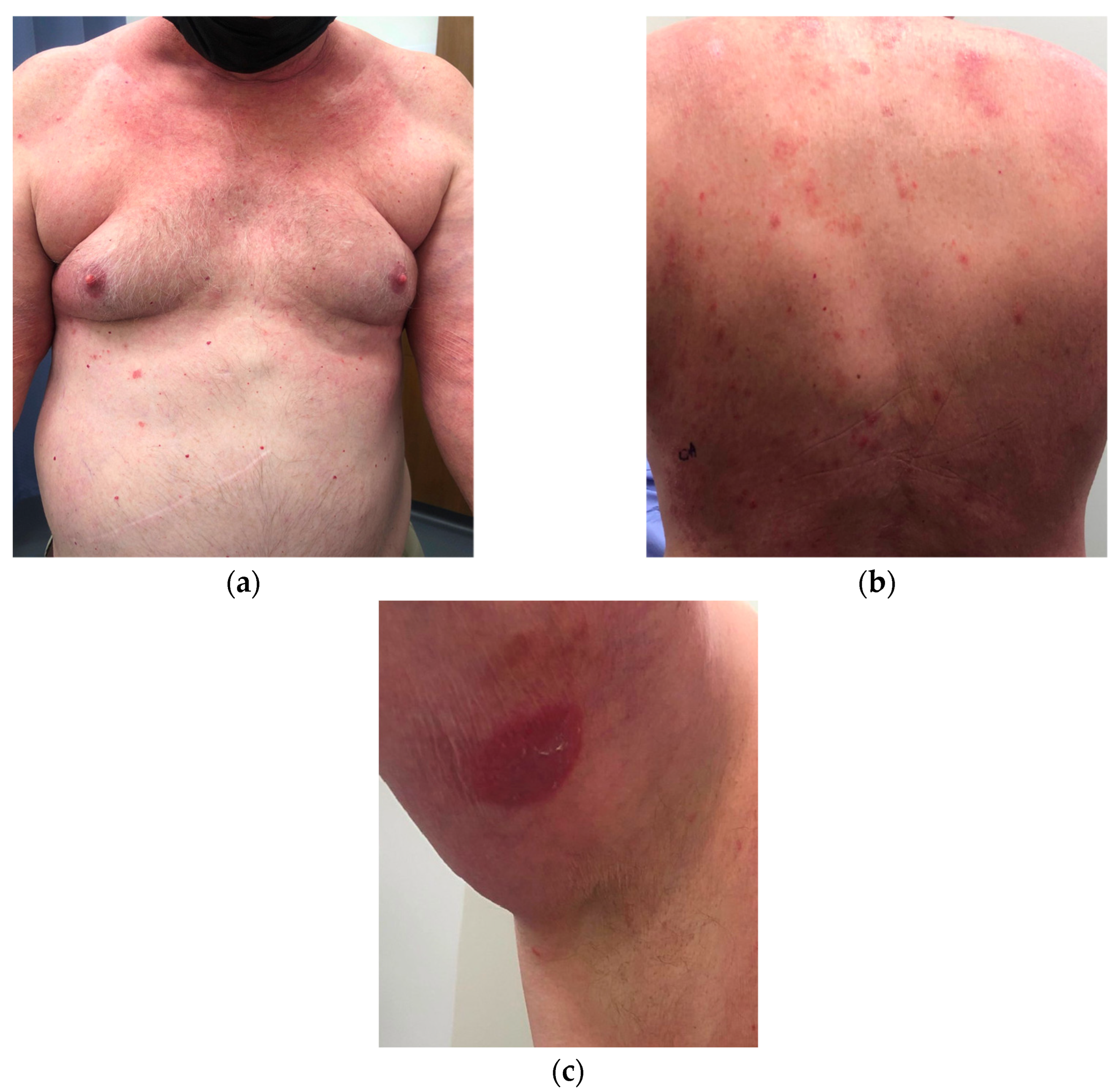
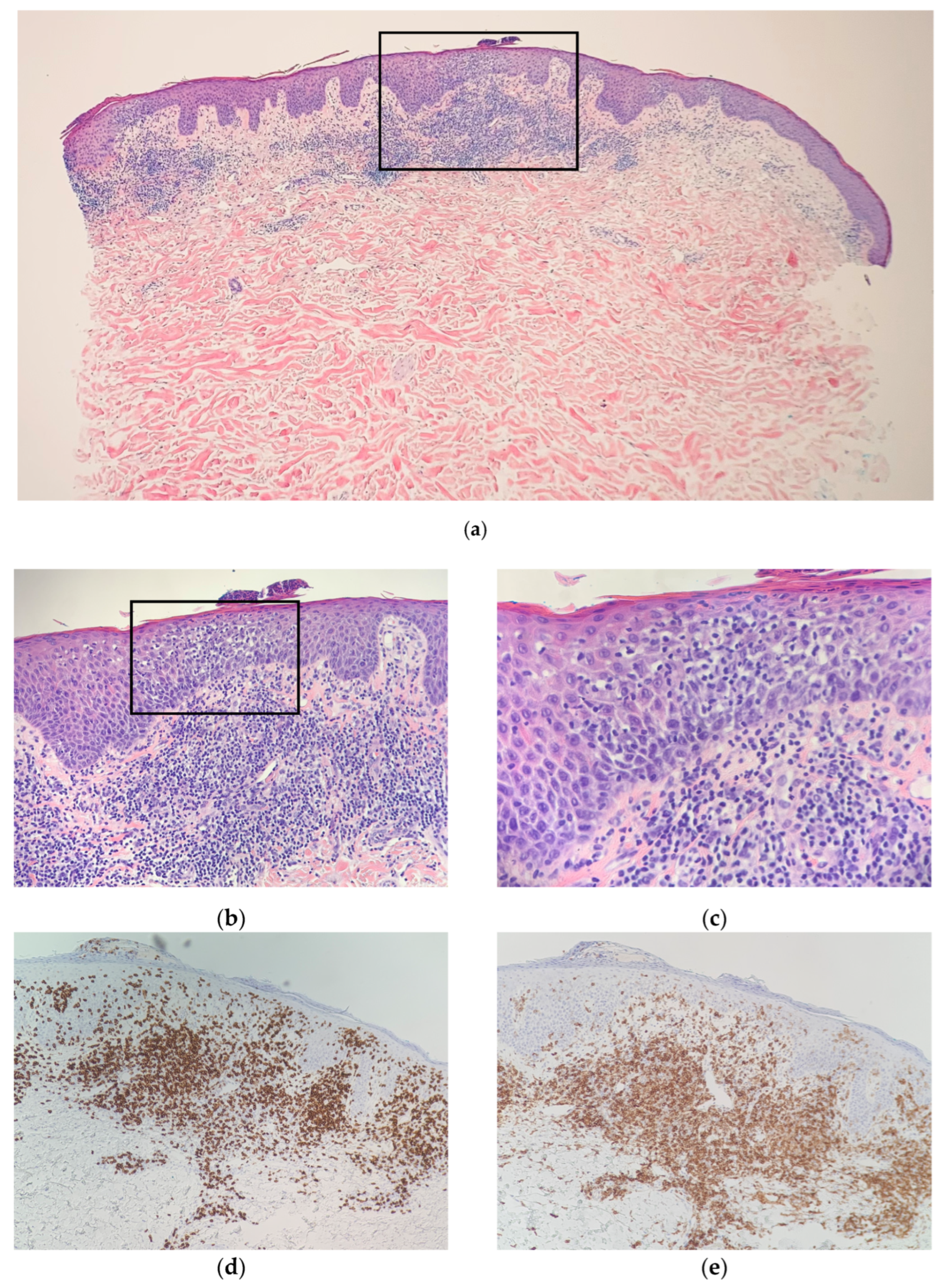
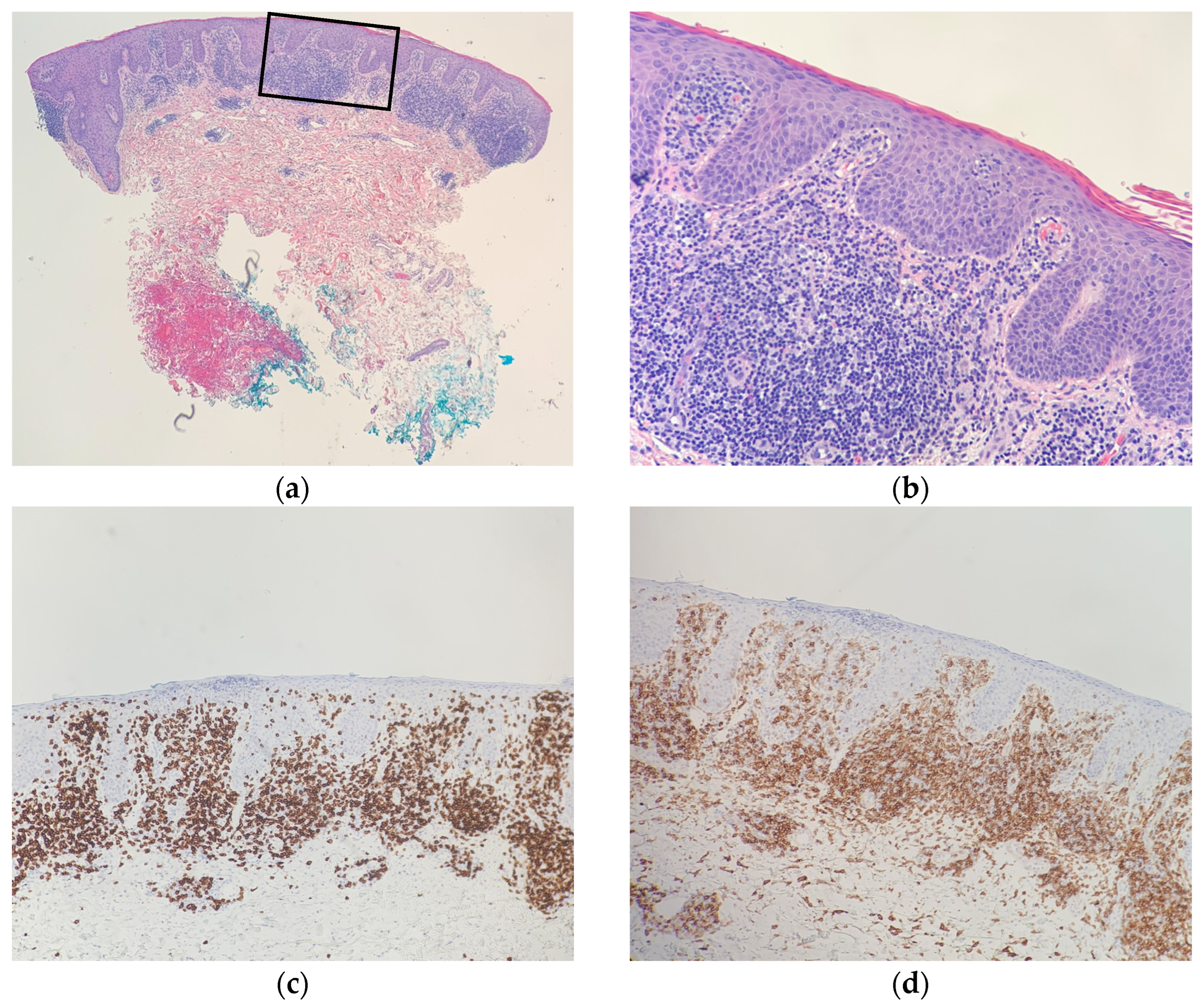
2. Case Synopsis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Thibodeaux, Q.; Smith, M.P.; Ly, K.; Beck, K.; Liao, W.; Bhutani, T. A review of dupilumab in the treatment of atopic diseases. Hum. Vaccines Immunother. 2019, 15, 2129–2139. [Google Scholar] [CrossRef] [PubMed]
- Ayasse, M.; Nelson, K.; Glass, F.; Silverberg, J.I. Mycosis Fungoides Unmasked by Dupilumab Treatment in a Patient with a History of Atopic Dermatitis. Dermatitis 2020, 32, e88–e89. [Google Scholar] [CrossRef] [PubMed]
- Chiba, T.; Nagai, T.; Osada, S.I.; Manabe, M. Diagnosis of Mycosis Fungoides Following Administration of Dupilumab for Misdiagnosed Atopic Dermatitis. Acta Derm. Venereol. 2019, 99, 818–819. [Google Scholar] [CrossRef] [Green Version]
- Espinosa, M.L.; Nguyen, M.T.; Aguirre, A.S.; Martinez-Escala, M.E.; Kim, J.; Walker, C.J.; Pontes, D.S.; Silverberg, J.I.; Choi, J.; Pro, B.; et al. Progression of cutaneous T-cell lymphoma after dupilumab: Case review of 7 patients. J. Am. Acad. Dermatol. 2020, 83, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Hollins, L.C.; Wirth, P.; Fulchiero, G.J., Jr.; Foulke, G.T. Long-standing dermatitis treated with dupilumab with subsequent progression to cutaneous T-cell lymphoma. Cutis 2020, 106, E8–E11. [Google Scholar] [CrossRef] [PubMed]
- Lazaridou, I.; Ram-Wolff, C.; Bouaziz, J.D.; Bégon, E.; Battistella, M.; Rivet, J.; Jachiet, M.; Bagot, M.; de Masson, A. Dupilumab Treatment in Two Patients with Cutaneous T-cell Lymphomas. Acta Derm. Venereol. 2020, 100, adv00271. [Google Scholar] [CrossRef] [PubMed]
- Miyashiro, D.; Vivarelli, A.G.; Gonçalves, F.; Cury-Martins, J.; Sanches, J.A. Progression of mycosis fungoides after treatment with dupilumab: A case report. Dermatol. Ther. 2020, 33, e13880. [Google Scholar] [CrossRef]
- Newsom, M.; Hrin, M.L.; Hamid, R.N.; Strowd, L.C.; Ahn, C.; Jorizzo, J.L.; Feldman, S.R. Two cases of mycosis fungoides diagnosed after treatment non-response to dupilumab. Dermatol. Online J. 2021, 27, 1–4. [Google Scholar] [CrossRef]
- Poyner, E.; Bacon, C.; Meggitt, S.; Weatherhead, S. A case of mycosis fungoides with large cell transformation following dupilumab treatment. Eur. J. Cancer 2019, 119, S42–S43. [Google Scholar] [CrossRef]
- Russomanno, K.; Carver De Klotz, C.M. Acceleration of cutaneous T-cell lymphoma following dupilumab administration. JAAD Case Rep. 2020, 8, 83–85. [Google Scholar] [CrossRef]
- Sokumbi, O.; Shamim, H.; Davis, M.D.P.; Wetter, D.A.; Newman, C.C.; Comfere, N. Evolution of Dupilumab-Associated Cutaneous Atypical Lymphoid Infiltrates. Am. J. Dermatopathol. 2021, 43, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Morris, L.; Vu, A.; Duvic, M. Development of Sézary syndrome following the administration of dupilumab. Dermatol. Online J. 2020, 26, 17. [Google Scholar] [CrossRef]
- Umemoto, N.; Demitsu, T.; Otaki, K.; Matsumoto, T.; Takazawa, M.; Yamada, A.; Kimura, S.I.; Kakurai, M. Dupilumab therapy in Sézary syndrome misdiagnosed as atopic dermatitis: A case report. J. Dermatol. 2020, 47, e356–e357. [Google Scholar] [CrossRef] [PubMed]
- Park, A.; Wong, L.; Lang, A.; Kraus, C.; Anderson, N.; Elsensohn, A. Cutaneous T-cell lymphoma following dupilumab use: A systematic review. Int. J. Dermatol. 2022, 1–15. [Google Scholar] [CrossRef]
- Lázaro-Sastre, M.; García-Sánchez, A.; Gómez-Cardeñosa, A.; Dávila, I. Dupilumab in atopic dermatitis. Curr. Treat. Options Allergy 2019, 6, 211–225. [Google Scholar] [CrossRef]
- Elston, D.M. Dupilumab and cutaneous T-cell lymphoma. J. Am. Acad. Dermatol. 2020, 83, 33–34. [Google Scholar] [CrossRef]
- Furue, M.; Ulzii, D.; Nakahara, T.; Tsuji, G.; Furue, K.; Hashimoto-Hachiya, A.; Kido-Nakahara, M. Implications of IL-13Rα2 in atopic skin inflammation. Allergol. Int. 2020, 69, 412–416. [Google Scholar] [CrossRef]
- Kwon, H.J.; Choi, J.E.; Bae, Y.K. Interleukin-13 receptor alpha 2 expression in tumor cells is associated with reduced disease-free survival in patients with luminal subtype invasive breast cancer. Tumour. Biol. 2018, 40, 1010428318783657. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Song, X.; Traub, B.; Luxenhofer, M.; Kornmann, M. Involvement of IL-4, IL-13 and Their Receptors in Pancreatic Cancer. Int. J. Mol. Sci. 2021, 22, 2998. [Google Scholar] [CrossRef]
- Fichtner-Feigl, S.; Terabe, M.; Kitani, A.; Young, C.A.; Fuss, I.; Geissler, E.K.; Schlitt, H.J.; Berzofsky, J.A.; Strober, W. Restoration of tumor immunosurveillance via targeting of interleukin-13 receptor-alpha 2. Cancer Res. 2008, 68, 3467–3475. [Google Scholar] [CrossRef]
- Zhao, T.; Su, Z.; Li, Y.; Zhang, X.; You, Q. Chitinase-3 like-protein-1 function and its role in diseases. Signal Transduct. Target. Ther. 2020, 5, 201. [Google Scholar] [CrossRef] [PubMed]
- Jawed, S.I.; Myskowski, P.L.; Horwitz, S.; Moskowitz, A.; Querfeld, C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): Part I. Diagnosis: Clinical and histopathologic features and new molecular and biologic markers. J. Am. Acad. Dermatol. 2014, 70, 205.e1–222. [Google Scholar] [CrossRef] [PubMed]
- Whittam, L.R.; Calonje, E.; Orchard, G.; Fraser-Andrews, E.A.; Woolford, A.; Russell-Jones, R. CD8-positive juvenile onset mycosis fungoides: An immunohistochemical and genotypic analysis of six cases. Br. J. Dermatol. 2000, 143, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Massone, C.; Crisman, G.; Kerl, H.; Cerroni, L. The prognosis of early mycosis fungoides is not influenced by phenotype and T-cell clonality. Br. J. Dermatol. 2008, 159, 881–886. [Google Scholar] [CrossRef]
- Diwan, H.; Ivan, D. CD8-positive mycosis fungoides and primary cutaneous aggressive epidermotropic CD8-positive cytotoxic T-cell lymphoma. J. Cutan. Pathol. 2009, 36, 390–392. [Google Scholar] [CrossRef]
- Kalay Yildizhan, I.; Sanli, H.; Akay, B.N.; Sürgün, E.; Heper, A. CD8+ cytotoxic mycosis fungoides: A retrospective analysis of clinical features and follow-up results of 29 patients. Int. J. Dermatol. 2020, 59, 127–133. [Google Scholar] [CrossRef]
- Martinez-Escala, M.E.; Kantor, R.W.; Cices, A.; Zhou, X.A.; Kaplan, J.B.; Pro, B.; Choi, J.; Guitart, J. CD8+ mycosis fungoides: A low-grade lymphoproliferative disorder. J. Am. Acad. Dermatol. 2017, 77, 489–496. [Google Scholar] [CrossRef]
- Mollanazar, N.K.; Savage, K.T.; Pousti, B.T.; Jariwala, N.; Del Guzzo, C.; Haun, P.; Vittorio, C.; Rook, A.H.; Kim, E.J. Cutaneous T-cell lymphoma and concomitant atopic dermatitis responding to dupilumab. Cutis 2020, 106, 131–132. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, A.; Wong, L.; Lang, A.; Kraus, C.; Anderson, N.; Elsensohn, A. Dupilumab-Associated Mycosis Fungoides with a CD8+ Immunophenotype. Dermatopathology 2022, 9, 385-391. https://doi.org/10.3390/dermatopathology9040045
Park A, Wong L, Lang A, Kraus C, Anderson N, Elsensohn A. Dupilumab-Associated Mycosis Fungoides with a CD8+ Immunophenotype. Dermatopathology. 2022; 9(4):385-391. https://doi.org/10.3390/dermatopathology9040045
Chicago/Turabian StylePark, Ariel, Lulu Wong, Annalise Lang, Christina Kraus, Nancy Anderson, and Ashley Elsensohn. 2022. "Dupilumab-Associated Mycosis Fungoides with a CD8+ Immunophenotype" Dermatopathology 9, no. 4: 385-391. https://doi.org/10.3390/dermatopathology9040045