
Individual Circadian Preference, Eating Disorders and Obesity in Children and Adolescents: A Dangerous Liaison? A Systematic Review and a Meta-Analysis

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
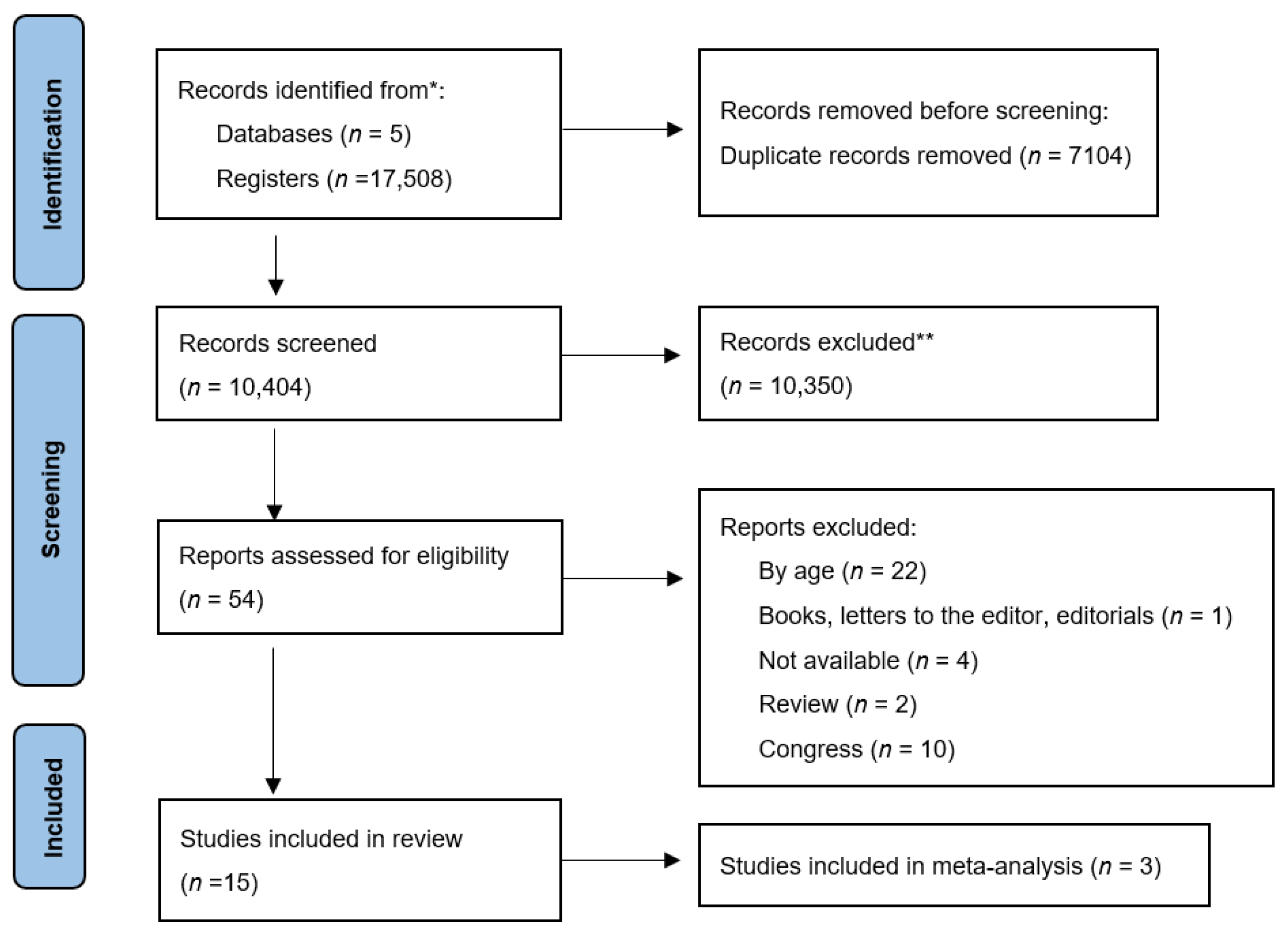
2.1. Design, Search Methods and Inclusion/Exclusion Criteria
2.2. Study Selection, Strategy for Data Synthesis and Quality Assessment
3. Results
3.1. General Characteristics of the Studies
3.1.1. Chronotype
3.1.2. Association with Sex
3.1.3. Eating Disorders
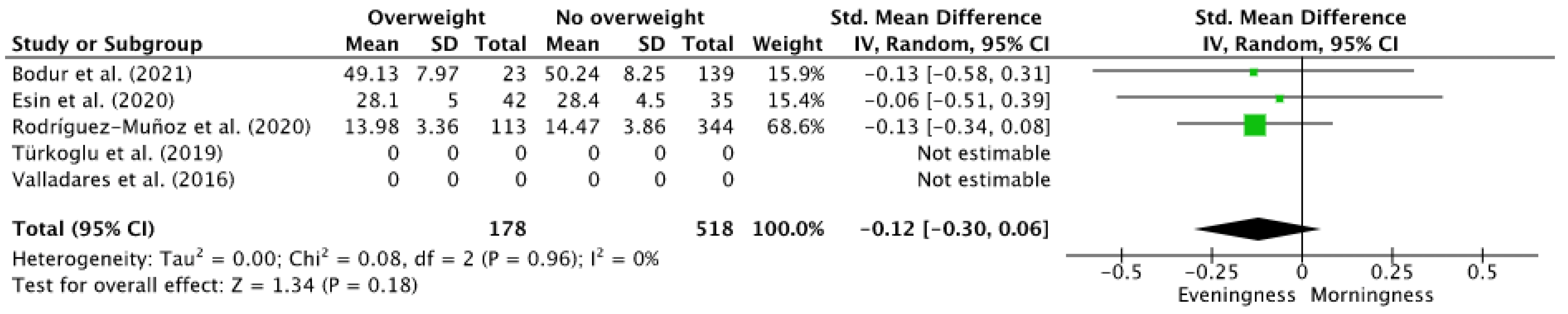
3.1.4. Quantitative Analysis: Overweight and Chronotype
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muscogiuri, G.; Barrea, L.; Aprano, S.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Pugliese, G.; Savastano, S.; Colao, A.; on behalf of the Opera Prevention Project. Chronotype and adherence to the Mediterranean diet in obesity: Results from the Opera Prevention Project. Nutrients 2020, 12, 1354. [Google Scholar] [CrossRef]
- Linke, M.; Jankowski, K.S. Chronotype in individuals with schizophrenia: A meta-analysis. Schizophr. Res. 2021, 235, 74–79. [Google Scholar] [CrossRef]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythm. Chronobiol. Int. 1976, 4, 97–110. [Google Scholar]
- Kandeger, A.; Selvi, Y.; Tanyer, D.K. The effects of individual circadian rhythm differences on insomnia, impulsivity, and food addiction. Eat. Weight. Disord. 2019, 24, 47–55. [Google Scholar] [CrossRef]
- Makarem, N.; Paul, J.; Giardina, E.V.; Liao, M.; Aggarwal, B. Evening chronotype is associated with poor cardiovascular health and adverse health behaviors in a diverse population of women. Chronobiol. Int. 2020, 37, 673–685. [Google Scholar] [CrossRef]
- Ashkenazi, I.E.; Reinberg, A.E.; Motohashi, Y. Interindividual differences in the flexibility of human temporal organization: Pertinence to jetlag and shiftwork. Chronobiol. Int. 1997, 14, 99–113. [Google Scholar] [CrossRef]
- Fishcer, D.; Lombardi, D.A.; Marucci-Wellman, H.; Roenneberg, T. Chronotypes in the US—Influence of age and sex. PLoS ONE 2017, 12, e0178782. [Google Scholar]
- Fabbian, F.; Zucchi, B.; De Giorgi, A.; Tiseo, R.; Boari, B.; Salmi, R.; Cappadona, R.; Gianesini, G.; Bassi, E.; Signani, F.; et al. Chronotype, gender and general health. Chronobiol. Int. 2016, 33, 863–882. [Google Scholar] [CrossRef]
- López-Soto, P.J.; Fabbian, F.; Cappadona, R.; Zucchi, B.; Manfredini, F.; García-Arcos, A.; Carmona-Torres, J.M.; Manfredini, R.; Rodríguez-Borrego, M.A. Chronotype, nursing activity, and gender: A systematic review. J. Adv. Nurs. 2019, 75, 734–748. [Google Scholar] [CrossRef]
- Najem, J.; Saber, M.; Aoun, C.; El Osta, N.; Papazian, T.; Khabbaz, L.R. Prevalence of food addiction and association with stress, sleep quality and chronotype: A cross-sectional survey among university students. Clin. Nutr. 2020, 39, 533–539. [Google Scholar] [CrossRef]
- Kurnaz, S.; Kandeger, A. Do chronotype differences and night eating syndrome affect dental health? Int. J. Dent. Hyg. 2020, 18, 378–383. [Google Scholar] [CrossRef]
- Riccobono, G.; Pompili, A.; Iannitelli, A.; Pacitti, F. The relationship between Night Eating Syndrome, depression and chronotype in a non-clinical adolescent population. Riv. Psichiatr. 2019, 54, 115–119. [Google Scholar]
- Romo-Nava, F.; Blom, T.J.; Cuellar-Barboza, A.B.; Winham, S.J.; Colby, C.L.; Nunez, N.A.; Biernacka, J.M.; Frye, M.A.; McElroy, S.L. Evening chronotype as a discrete clinical subhenotype in bipolar disorder. J. Affect. Disord. 2020, 266, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.C.; Story, M.; Larson, N.I.; Neumark-Sztainer, D.; Lytle, L.A. Emerging adulthood and college-aged youth: An overlooked age for weight-related behavior change. Obesity 2008, 16, 2205–2211. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated September 2020); Cochrane: London, UK, 2020. [Google Scholar]
- Centre for Reviews and Dissemination. Systematic Reviews. 2008 CRD’s Guidance for Undertaking Reviews in Health Care; University of York: York, UK, 2008. [Google Scholar]
- Bodur, M.; Bidar, S.N.; Yardimci, H. Effect of chronotype on diet and sleep quality in healthy female students: Night lark versus early bird. Nutr. Food Sci. 2021, 51, 1138–1149. [Google Scholar] [CrossRef]
- Esin, I.S.; Dsun, O.B.; Demirdogen, E.Y.; Asikhasanoglu, E.O.; Aslan, S.C.; Ozturk, K.; Cayir, A. Effects of chronotype and sleep duration on life quality and psychopathology in childhood obesity. Pediatric Endocrinol. Diabetes Metab. 2020, 26, 192–197. [Google Scholar] [CrossRef]
- Türkoglu, S.; Çetin, F.H. The relationship between chronotype and obesity in children and adolescent with attention deficit hyperactivity disorder. Chronobiol. Int. 2019, 36, 1138–1147. [Google Scholar] [CrossRef]
- Valladares, M.; Campos, B.; Zapata, C.; Durán Agüero, S.; Obregón, A.M. Association between chronotype and obesity in yough people. Nutr. Hosp. 2016, 33, 1336–1339. [Google Scholar]
- Rodríguez-Muñoz, P.M.; Carmona-Torres, J.M.; Rivera-Picón, C.; Fabbian, F.; Manfredini, R.; Rodríguez-Borrego, M.A.; López-Soto, P.J. Associations between chronotype, adherence to the Mediterranean diet and sexual opinion among university students. Nutrients 2020, 12, 1990. [Google Scholar] [CrossRef]
- Saidi, O.; Rochette, E.; Bovet, M.; Merlin, E.; Duché, P. Acute intense exercise improves sleep and decreases next morning consumption of energy-dense food in adolescent girls with obesity and evening chronotype. Pediatric Obes. 2019, 15, e12613. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Taheri, S. Associations among late chronotype, body mass index and dietary behaviors in young adolescents. Int. J. Obes. 2015, 39, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Karadag, M.; Yilmaz, G.C. What is the relationship between obesity and new circadian rhythm parameters in Turkish children and adolescents? A case-control study. J. Pediatric Endocrinol. Metab. 2021, 34, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Wu, M.; Yuan, F.; Zhang, H. Sugary beverage consumption mediates the relationship between late chronotype, sleep duration, and weight increase among undergraduates: A cross-sectional study. Environ. Health Prev. Med. 2018, 23, 63. [Google Scholar] [CrossRef] [PubMed]
- Roßbach, S.; Diederichs, T.; Nöthlings, U.; Buyken, A.E.; Alexy, U. Relevance of chronotype for eating patterns in adolescents. Chronobiol. Int. 2017, 35, 336–347. [Google Scholar] [CrossRef]
- Yu, B.Y.M.; Yeung, W.F.; Ho, Y.S.; Yee Ho, F.Y.; Chung, K.F.; Tong Lee, R.L.; Lam, M.Y.; Chen, S. Associations between the chronotypes and eating habits of Hong Kong school-aged children. Int. J. Environ. Res. Public Health 2020, 17, 2583. [Google Scholar] [CrossRef] [Green Version]
- Kandeger, A.; Egilmez, U.; Sayin, A.A.; Selvi, Y. The relationship between night eating symptoms and disordered eating attitudes via insomnia and chronotype differences. Psychiatry Res. 2018, 268, 354–357. [Google Scholar] [CrossRef]
- Agagündüz, D.; Acar-Tek, N.; Bozbulut, R. Chronotype is associated with REEs in obese children and adolescents. Prog. Nutr. 2020, 22, e2020009. [Google Scholar]
- Study Quality Assessment Tools. NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 September 2021).
- Roenneberg, T.; Daan, S.; Merrow, M. The art of entrainment. J. Biol. Rhythm. 2003, 18, 183–194. [Google Scholar] [CrossRef]
- Vollmer, C.; Michel, U.; Randler, C. Outdoor light at night (LAN) is correlated with eveningness in adolescents. Chronobiol. Int. 2012, 29, 502–508. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Milesi, C. Artificial Outdoor Nightime Lights associate with altered sleep behavior in the American general population. Sleep 2016, 39, 1311–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garaulet, M.; Ordovas, J.M.; Madrid, J.A. The chronobiology, etiology and pathophysiology of obesity. Int. J. Obes. 2010, 34, 1667–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, R. Sleep: Late to bed, late to rise, could be cardiometabolically unwise. Nat. Rev. Endocrinol. 2016, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Vera, B.; Dashti, H.S.; Gómez-Abellán, P.; Hernández-Martínez, A.M.; Esteban, A.; Scheer, F.A.J.L.; Saxena, R.; Garaulet, M. Modifiable lifestyle behaviors, but not a genetic risk score, associate with metabolic syndrome in evening chronotype. Sci. Rep. 2018, 8, 945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Anderson, S.E. Body mass index in children and adolescents: Considerations for population-based applications. Int. J. Obes. 2006, 30, 590–594. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; Technical Report Series: 894; WHO: Geneva, Switzerland, 2000; Available online: https://apps.who.int/iris/handle/10665/42330 (accessed on 27 November 2021).
- Galindo Muñoz, J.S.; Gómez Gallego, M.; Soler, I.D.; Barberá Ortega, M.C.; Martínez Cáceres, C.M.; Hernández Morante, J.J. Effect of a chronotype-adjusted diet on weight loss effectiveness: A randomized clinical trial. Clin. Nutr. 2020, 39, 1041–1048. [Google Scholar] [CrossRef]
- Ricotti, R.; Caputo, M.; Monzani, A.; Pigni, S.; Antoniotti, V.; Bellone, S.; Prodam, F. Breakfast skipping, weight, cardiometabolic risk, and nutrition quality in children and adolescents: A systematic review of randomized controlled and intervention longitudinal trials. Nutrients 2021, 13, 3331. [Google Scholar] [CrossRef]
- Xiao, Q.; Garaulet, M.; Scheer, F.A.J.L. Meal timing and obesity: Interactions with macronutrient intake and chronotype. Int. J. Obes. 2019, 43, 1701–1711. [Google Scholar] [CrossRef]
- Ramón-Arbués, E.; Granada-López, J.-M.; Martínez-Abadía, B.; Echániz-Serrano, E.; Antón-Solanas, I.; Jerue, B.A. Factors Related to Diet Quality: A Cross-Sectional Study of 1055 University Students. Nutrients 2021, 13, 3512. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, P.M.; Cappadona, R.; Fabbian, F.; Di Simone, E.; Di Muzio, M.; Rodríguez-Borrego, M.A.; López-Soto, P.J. Lifestyles and habits in young people: Analysis of Italian National Institute of Statistics database. Prog. Nutr. 2021, 23, e2021202. [Google Scholar]
- Rodríguez-Muñoz, R.M.; Carmona-Torres, J.M.; Rivera-Picón, C.; Morales-Cané, I.; Fabbian, F.; Manfredini, R.; Rodríguez-Borrego, M.A.; López-Soto, P.J. Risky behaviours of Spanish university students: Associations with Mediterranean diet, sexual attitude and chronotype. Nutrients 2021, 13, 4042. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors, Year | Design (Country) | Disorder (n) | Control (n) | Gender M/F | Age (SD) [Disorder/Control] | Chronotype (SD) [Disorder/Control] | Tool | Main Results |
|---|---|---|---|---|---|---|---|---|
| Bodur et al. (2021) [18] | Cross sectional study (Turkey) | BMI > 25 23 | 139 | 0/23 0/139 | [20.13 (1.55) years 20.39 (1.53) years] | [49,13 (7.97) 50,24 (8.25)] | MEQ | E-type individuals have a lower intake of fruit and a higher intake of refined grains. Healthy individuals may be vulnerable to chronic diseases. In the long-term, chronotype effect in dietary (high energy, carbohydrate and fat intake of E-type individuals) |
| Esin et al. (2020) [19] | Case-control study (Turkey) | BMI > 25 42 | 35 | 20/22 20/15 | [11.5 (2.9) years 10.4 (2.9) years] | [28.1 (5) 28.4 (4.5)] | CCTQ | No risk factors (chronotype or having at least one psychiatric disorder) were statistically associated to become obese. |
| Türkoğlu et al. (2019) [20] | Cross sectional study (Turkey) | BMI > 25 22 | 56 | 22/0 56/0 | 10.02 (2.24) years | NR | CCTQ | E-type was directly related to obesity and M-type related to normal weight in children and adolescents with attention deficit hyperactivity disorder |
| Valladares et al. (2016) [21] | Cross sectional study (Spain) | BMI > 25 | 65 | 30/35 | 20 years | [48.5 49.1] | MEQ | E-type is strongly associated with altered body composition measures. E-type may be a risk factor for the development of metabolic diseases. |
| Rodriguez-Munoz. et al. (2020) [22] | Cross sectional study (Spain) | BMI > 25 113 | 344 | 152/305 | 22 (4) years | [13.98 (3.36) 14.47 (3.86)] | rMEQ | Having an E-type during university was associated with poor adherence to the Mediterranean diet. Chronotype is an important variable that interferes with diet and sexual opinion. |
| Saidi et al. (2020) [23] | Cross sectional study (France) | BMI > 25 and E-type 16 | NA | 0/16 | 13.18 (0.98) years | NA | MEQ | E-type adolescent women with obesity, after practicing intense exercise, show a decrease in the intake of foods with high energy content. |
| Arora et al. (2015) [24] | Cross sectional study (United Kingdon) | BMI z-score (NR) | NA | 212/299 | 12.0 (0.7) years | NR | MEQ | E-type are associated with a high BMI and poorer eating behaviors. There is also a negative relationship between sleep duration and BMI |
| Karadag et al. (2021) [25] | Case-control study (Turkey) | BMI ≥ 95th percentile 79 | 82 | 41/38 45/37 | [12.1 (2.3) years 12.4 (2.2) years] | 31.9 (6.3) 27.2 (5.7) | CCTQ | Obese children and adolescents had greater evening preference, longer sleep debt duration, SJL duration and SJLsc duration, higher MEQ scores, and shorter mean sleep duration |
| Li et al. (2018) [26] | Cross sectional study (China) | Sugary beverage intake (NR) | NA | 271/517 | 19.8 (1.1) years | M-type: 21.8% I-type: 62.8% E-type: 15.4% | MEQ | Chronotype and sleep duration were associated with BMI, and this relationship was mediated by sugary beverage intake. |
| Roßbach et al. (2018) [27] | Cross sectional study (Germany) | BMI (According to IOTF) | NA | 184/162 | 12.2 (1.4) years | Median (Q1; Q3) | MCTQ | E-Type adolescents are more likely to perform regular breakfast skipping and higher evening energy intake. |
| Yu et al. (2020) [28] | Retrospec. cohort study (Hong Kong) | Fast Food intake 398 | 98 | 261/235 | 9.25 (1.58) years | Boys: - M-type: 74.2% - E-type: 91.2% Girls - M-type: 43.5% - E-type: 86.2% | CCTQ | E-type boys were more likely to eat fast food than M-type boys [OR = 3.62 (1.07–12.26), p = 0.03]. When adjusted for the screen time of the children no statistically significant differences were found [aOR = 3.18, (0.91–11.16), p = 0.07] |
| Najem et al. (2020) [10] | Cross sectional study (Lebanon) | Food addiction 65 | 579 | 190/453 | 20.22 (1.8) years | 47.89 (8.03) - M-type: 8.7% - E-type: 20.5% | MEQ | Poor sleep quality, high stress and an E-type could lead to the development of food addiction, as their effect can be cumulative. |
| Kandeger et al. (2018) [29] | Cross sectional study. (Turkey) | NES 20 | 363 | 9/11 153/230 | [20.55 (2.46) years 21.12 (2.31) years] | [45.25 (10.67) 51.24 (8.56)] | MEQ | Presence of NES affects chronotype differences and insomnia severity. NES might represent a misalignment of food intake and might shift the chronotype to the late sleep phase as a peripheral oscillator in humans. |
| Riccobono et al. (2019) [12] | Cross sectional study. (Italy) | NES 12 | 289 | 114/175 | [17.25 (1.54) years 17.65 (1.29) years] | [42.92 (11.1) 47.56 (8.39)] | MEQ | A high prevalence of NES was observed in subjects with an E-type and depression. |
| Ağagündüz et al. (2020) [30] | Cross sectional study (Turkey) | REE 103 | NA | 57/46 | 10.6 (2.19) years | 31.5 (7.39) | CCTQ | Compared with M-type and I-type, participants with E-type had lower energy expenditure for physical activity, lower REE and total energy expenditure. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Cortés, F.J.; Morales-Cané, I.; Rodríguez-Muñoz, P.M.; Cappadona, R.; De Giorgi, A.; Manfredini, R.; Rodríguez-Borrego, M.A.; Fabbian, F.; López-Soto, P.J. Individual Circadian Preference, Eating Disorders and Obesity in Children and Adolescents: A Dangerous Liaison? A Systematic Review and a Meta-Analysis. Children 2022, 9, 167. https://doi.org/10.3390/children9020167
Rodríguez-Cortés FJ, Morales-Cané I, Rodríguez-Muñoz PM, Cappadona R, De Giorgi A, Manfredini R, Rodríguez-Borrego MA, Fabbian F, López-Soto PJ. Individual Circadian Preference, Eating Disorders and Obesity in Children and Adolescents: A Dangerous Liaison? A Systematic Review and a Meta-Analysis. Children. 2022; 9(2):167. https://doi.org/10.3390/children9020167
Chicago/Turabian StyleRodríguez-Cortés, Francisco José, Ignacio Morales-Cané, Pedro Manuel Rodríguez-Muñoz, Rosaria Cappadona, Alfredo De Giorgi, Roberto Manfredini, María Aurora Rodríguez-Borrego, Fabio Fabbian, and Pablo Jesús López-Soto. 2022. "Individual Circadian Preference, Eating Disorders and Obesity in Children and Adolescents: A Dangerous Liaison? A Systematic Review and a Meta-Analysis" Children 9, no. 2: 167. https://doi.org/10.3390/children9020167