
Do Metacognitions of Children and Adolescents with Anxiety Disorders Change after Intensified Exposure Therapy?


Abstract
:1. Introduction
1.1. Treatment of Anxiety Disorders in Children and Adolescents
1.2. Negative Repetitive Thoughts in the Context of Anxiety
1.3. Metacognitions and Their Role in Psychotherapy
1.4. Research Questions and Hypothesis
- Do repetitive negative thoughts, worry, and metacognitive beliefs of children with anxiety disorders change across treatment with exposure-focused therapy?
- 2.
- Are changes in repetitive negative thinking, worry, and anxiety associated with changes in metacognitive beliefs in children with anxiety disorders?
- 3.
- Do patients with specific phobia, separation anxiety disorder, and social phobia differ in metacognitive beliefs and in how their metacognitive beliefs change?
2. Materials and Methods
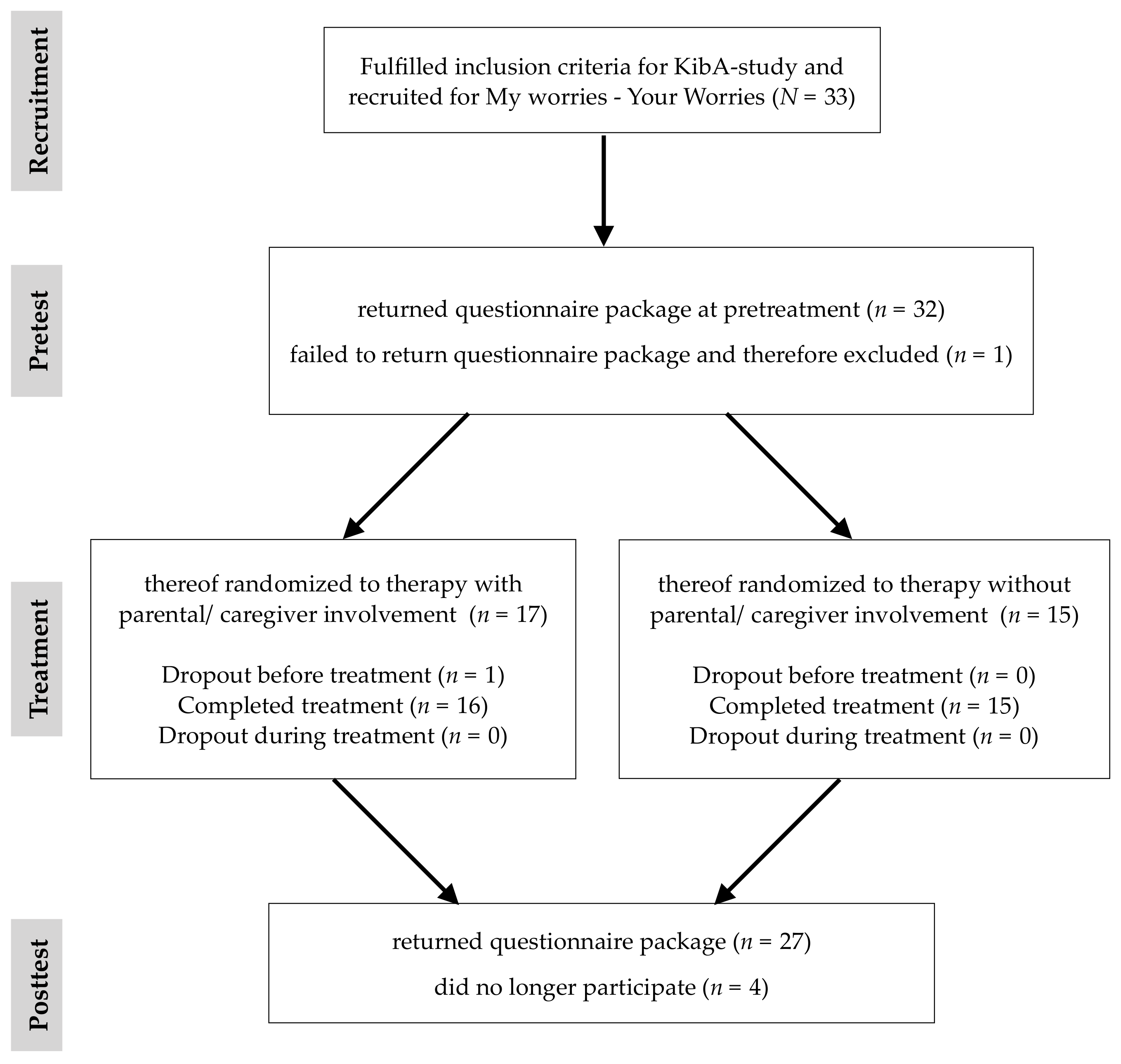
2.1. Participants and Procedure
2.2. Measures
2.2.1. Structured Diagnostic Interview for Mental Disorders in Children (Kinder-DIPS)
2.2.2. Demographic and Socioeconomic Variables
2.2.3. Questionnaires for Anxiety- and Obsessive-Compulsive-Disorders (ANZ) of the Diagnostiksystem für Psychische Störungen nach ICD-10 und DSM-IV für Kinder und Jugendliche 2. Version (DISYPS-II)
2.2.4. Measure of Excessive Worry Content (EWC)
2.2.5. Perseverative Thinking Questionnaire (PTQ)
2.2.6. German Metacognitions Questionnaire for Children (MKF-K)
2.3. Statistical Analysis
3. Results
3.1. Changes across Time
3.2. Relationships between Changes in Anxiety, Worry and Metacognitions
3.3. Regression Analysis
3.4. Exploratory Comparison of the Diagnostic Groups
3.5. Post-Hoc Power Analysis
4. Discussion
4.1. Change in Anxiety, Worry and Repetitive Negative Thoughts
4.2. Change in Metacognitive Beliefs
4.3. Comparisons of Diagnostic Subsamples
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wagner, G.; Zeiler, M.; Waldherr, K.; Philipp, J.; Truttmann, S.; Dür, W.; Treasure, J.L.; Karwautz, A.F.K. Mental health problems in Austrian adolescents: A nationwide, two-stage epidemiological study applying DSM-5 criteria. Eur. Child Adolesc. Psychiatry 2017, 26, 1483–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Petresco, S.; Anselmi, L.; Santos, I.S.; Barros, A.; Fleitlich-Bilyk, B.; Barros, F.C.; Matijasevich, A. Prevalence and comorbidity of psychiatric disorders among 6-year-old children: 2004 Pelotas Birth Cohort. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 975–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franz, L.; Angold, A.; Copeland, W.; Costello, E.J.; Towe-Goodman, N.; Egger, H. Preschool Anxiety Disorders in Pediatric Primary Care: Prevalence and Comorbidity. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 1294–1303.e1. [Google Scholar] [CrossRef] [Green Version]
- Kim-Cohen, J.; Caspi, A.; Moffitt, T.E.; Harrington, H.; Milne, B.J.; Poulton, R. Prior Juvenile Diagnoses in Adults With Mental Disorder: Developmental follow-back of a prospective-longitudinal cohort. Arch. Gen. Psychiatry 2003, 60, 709–717. [Google Scholar] [CrossRef]
- Bittner, A.; Egger, H.L.; Erkanli, A.; Costello, E.J.; Foley, D.L.; Angold, A. What do childhood anxiety disorders predict? J. Child Psychol. Psychiatry 2007, 12, 1174–1183. [Google Scholar] [CrossRef]
- Essau, C.A.; Lewinsohn, P.M.; Olaya, B.; Seeley, J.R. Anxiety disorders in adolescents and psychosocial outcomes at age 30. J. Affect. Disord. 2014, 163, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Heiervang, E.; Stormark, K.M.; Lundervold, A.J.; Heimann, M.; Goodman, R.; Posserud, M.-B.; Ullebø, A.K.; Plessen, K.J.; Bjelland, I.; Lie, S.A.; et al. Psychiatric Disorders in Norwegian 8- to 10-Year-Olds. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 438–447. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Social Anxiety Disorder: Recognition, Assessment and Treatment—Clinical Guideline; NICE: London, UK, 2013. [Google Scholar]
- In-Albon, T.; Schneider, S. Psychotherapy of Childhood Anxiety Disorders: A Meta-Analysis. Psychother. Psychosom. 2007, 76, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Whiteside, S.P.H.; Sim, L.; Farah, W.; Morrow, A.S.; Alsawas, M.; Barrionuevo, P.; Tello, M.; Asi, N.; Beuschel, B.; et al. Comparative Effectiveness and Safety of Cognitive Behavioral Therapy and Pharmacotherapy for Childhood Anxiety Disorders. JAMA Pediatr. 2017, 171, 1049–1056. [Google Scholar] [CrossRef]
- James, A.C.; Reardon, T.; Soler, A.; James, G.; Creswell, C. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst. Rev. 2020, 11, CD013162. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.; Clark, D.M.; Leigh, E. Are young people with primary social anxiety disorder less likely to recover following generic CBT compared to young people with other primary anxiety disorders? A systematic review and meta-analysis. Behav. Cogn. Psychother. 2021, 49, 352–369. [Google Scholar] [CrossRef]
- McEvoy, P.M.; Salmon, K.; Hyett, M.P.; Jose, P.E.; Gutenbrunner, C.; Bryson, K.; Dewhirst, M. Repetitive Negative Thinking as a Transdiagnostic Predictor of Depression and Anxiety Symptoms in Adolescents. Assessment 2019, 26, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T.; Watkins, E. Repetitive Negative Thinking as a Transdiagnostic Process. Int. J. Cogn. Ther. 2008, 1, 192–205. [Google Scholar] [CrossRef]
- Ehring, T.; Zetsche, U.; Weidacker, K.; Wahl, K.; Schönfeld, S.; Ehlers, A. The Perseverative Thinking Questionnaire (PTQ): Validation of a content-independent measure of repetitive negative thinking. J. Behav. Ther. Exp. Psychiatry 2011, 42, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Bijttebier, P.; Raes, F.; Vasey, M.; Bastin, M.; Ehring, T. Assessment of Repetitive Negative Thinking in Children: The Perseverative Thinking Questionnaire—Child Version (PTQ-C). J. Psychopathol. Behav. Assess. 2015, 37, 164–170. [Google Scholar] [CrossRef]
- Hitchcock, C.; Brown, R.L.; Cobham, V.E. Validation of the Child version of the Perseverative Thinking Questionnaire of repetitive negative thinking in young people with diagnosed depressive and anxiety disorders. Br. J. Clin. Psychol. 2021, 1–13. [Google Scholar] [CrossRef]
- Wilson, C. Pathological Worry in Children: What is Currently Known? J. Exp. Psychopathol. 2010, 1, 6–33. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlingon, VA, USA, 2013. [Google Scholar]
- World Health Organisation (WHO). Internationale statistische Klassifikation der Krankheiten und Verwandter Gesundheitsprobleme, German Modification. ICD-10-GM; Deutsches Institut für Medizinische Dokumentation und Information (DIMDI): Köln, Germany, 2019. [Google Scholar]
- Watkins, E.R. Constructive and unconstructive repetitive thought. Psychol. Bull. 2008, 134, 163–206. [Google Scholar] [CrossRef] [Green Version]
- Muris, P.; Merckelbach, H.; Meesters, C.; Van Brand, K.V.D. Cognitive Development and Worry in Normal Children. Cogn. Ther. Res. 2002, 26, 775–787. [Google Scholar] [CrossRef]
- Bacow, T.L.; Pincus, D.B.; Ehrenreich, J.T.; Brody, L.R. The metacognitions questionnaire for children: Development and validation in a clinical sample of children and adolescents with anxiety disorders. J. Anxiety Disord. 2009, 23, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Ellis, D.M.; Hudson, J.L. Test of the Metacognitive Model of Generalized Anxiety Disorder in Anxiety-Disordered Adolescents. J. Exp. Psychopathol. 2011, 2, 28–43. [Google Scholar] [CrossRef]
- Bacow, T.L.; May, J.E.; Brody, L.R.; Pincus, D.B. Are there specific metacognitive processes associated with anxiety disorders in youth? Psychol. Res. Behav. Manag. 2010, 3, 81–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hearn, C.S.; Donovan, C.L.; Spence, S.H.; March, S.; Holmes, M.C. What’s the Worry with Social Anxiety? Comparing Cognitive Processes in Children with Generalized Anxiety Disorder and Social Anxiety Disorder. Child Psychiatry Hum. Dev. 2017, 48, 786–795. [Google Scholar] [CrossRef]
- Vassilopoulos, S.P.; Brouzos, A.; Moberly, N.J. The Relationships Between Metacognition, Anticipatory Processing, and Social Anxiety. Behav. Chang. 2015, 32, 114–126. [Google Scholar] [CrossRef]
- Hodson, K.J.; McManus, F.V.; Clark, D.M.; Doll, H. Can Clark and Wells’ (1995) Cognitive Model of Social Phobia be Applied to Young People? Behav. Cogn. Psychother. 2008, 36, 449–461. [Google Scholar] [CrossRef]
- Gavric, D.; Moscovitch, D.A.; Rowa, K.; McCabe, R. Post-event processing in social anxiety disorder: Examining the mediating roles of positive metacognitive beliefs and perceptions of performance. Behav. Res. Ther. 2017, 91, 1–12. [Google Scholar] [CrossRef]
- Asbrand, J.; Schmitz, J.; Krämer, M.; Nitschke, K.; Heinrichs, N.; Tuschen-Caffier, B. Effects of Group-Based CBT on Post-Event Processing in Children with Social Anxiety Disorder Following an Experimental Social Stressor. J. Abnorm. Child Psychol. 2019, 47, 1945–1956. [Google Scholar] [CrossRef]
- Hearn, C.S.; Donovan, C.L.; Spence, S.H.; March, S. Do worry and its associated cognitive variables alter following CBT treatment in a youth population with Social Anxiety Disorder? Results from a randomized controlled trial. J. Anxiety Disord. 2018, 53, 46–57. [Google Scholar] [CrossRef]
- Flavell, J.H. Metacognition and cognitive monitoring: A new area of cognitive-developmental inquiry. Am. Psychol. 1979, 34, 906–911. [Google Scholar] [CrossRef]
- Wells, A.; Matthews, G. Modelling cognition in emotional disorder: The S-REF model. Behav. Res. Ther. 1996, 34, 881–888. [Google Scholar] [CrossRef]
- Wells, A. A Cognitive Model of Generalized Anxiety Disorder. Behav. Modif. 1999, 23, 526–555. [Google Scholar] [CrossRef] [Green Version]
- Wells, A. The Metacognitive Model of GAD: Assessment of Meta-Worry and Relationship With DSM-IV Generalized Anxiety Disorder. Cogn. Ther. Res. 2005, 29, 107–121. [Google Scholar] [CrossRef]
- Köcher, L.M.; Schneider, K.; Christiansen, H. Thinking about worry: A systematic review and meta-analysis on the assessment of metacognitions in children and adolescents. World J. Psychiatry 2021, 11, 635–658. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, L.; La Fauci, E.; Ingrassia, M. Exploring meta-worry and perceived parenting behaviors in adolescents’ anxiety. Life Span Disabil. 2018, 2, 117–141. [Google Scholar]
- Donovan, C.L.; Holmes, M.C.; Farrell, L.J. Investigation of the cognitive variables associated with worry in children with Generalised Anxiety Disorder and their parents. J. Affect. Disord. 2016, 192, 1–7. [Google Scholar] [CrossRef]
- Smith, K.E.; Hudson, J.L. Metacognitive Beliefs and Processes in Clinical Anxiety in Children. J. Clin. Child Adolesc. Psychol. 2013, 42, 590–602. [Google Scholar] [CrossRef] [PubMed]
- Reinholdt-Dunne, M.L.; Blicher, A.; Nordahl, H.; Normann, N.; Esbjørn, B.H.; Wells, A. Modeling the Relationships Between Metacognitive Beliefs, Attention Control and Symptoms in Children with and Without Anxiety Disorders: A Test of the S-REF Model. Front. Psychol. 2019, 10, 1205. [Google Scholar] [CrossRef]
- Esbjørn, B.H.; Lønfeldt, N.; Nielsen, S.K.K.; Reinholdt-Dunne, M.L.; Sømhovd, M.J.; Cartwright-Hatton, S. Meta-Worry, Worry, and Anxiety in Children and Adolescents: Relationships and Interactions. J. Clin. Child Adolesc. Psychol. 2015, 44, 145–156. [Google Scholar] [CrossRef]
- Wells, A. Metacognitive Therapy for Anxiety and Depression; Guilford: New York, NY, USA, 2009. [Google Scholar]
- McEvoy, P.M. Metacognitive Therapy for Anxiety Disorders: A Review of Recent Advances and Future Research Directions. Curr. Psychiatry Rep. 2019, 21, 29. [Google Scholar] [CrossRef]
- Haseth, S.; Solem, S.; Sørø, G.B.; Bjørnstad, E.; Grøtte, T.; Fisher, P. Group Metacognitive Therapy for Generalized Anxiety Disorder: A Pilot Feasibility Trial. Front. Psychol. 2019, 10, 290. [Google Scholar] [CrossRef] [PubMed]
- Nordahl, H.; Wells, A. Metacognitive Therapy for Social Anxiety Disorder: An A–B Replication Series Across Social Anxiety Subtypes. Front. Psychol. 2018, 9, 540. [Google Scholar] [CrossRef] [PubMed]
- Normann, N.; Morina, N. The Efficacy of Metacognitive Therapy: A Systematic Review and Meta-Analysis. Front. Psychol. 2018, 9, 2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffart, A.; Johnson, S.U.; Nordahl, H.M.; Wells, A. Mechanisms of change in metacognitive and cognitive behavioral therapy for treatment-resistant anxiety. J. Exp. Psychopathol. 2018, 9, 2043808718787414. [Google Scholar] [CrossRef] [Green Version]
- McEvoy, P.M.; Perini, S.J. Cognitive behavioral group therapy for social phobia with or without attention training: A controlled trial. J. Anxiety Disord. 2009, 23, 519–528. [Google Scholar] [CrossRef]
- McEvoy, P.M.; Mahoney, A.; Perini, S.J.; Kingsep, P. Changes in post-event processing and metacognitions during cognitive behavioral group therapy for social phobia. J. Anxiety Disord. 2009, 23, 617–623. [Google Scholar] [CrossRef]
- Simons, M. Metakognitive Therapie mit Kindern und Jugendlichen; Beltz: Weinheim, Germany; Basel, Switzerland, 2018. [Google Scholar]
- Esbjørn, B.H.; Normann, N.; Christiansen, B.M.; Reinholdt-Dunne, M.L. The efficacy of group metacognitive therapy for children (MCT-c) with generalized anxiety disorder: An open trial. J. Anxiety Disord. 2018, 53, 16–21. [Google Scholar] [CrossRef]
- Walczak, M.; Breinholst, S.; Ollendick, T.; Esbjørn, B.H. Cognitive Behavior Therapy and Metacognitive Therapy: Moderators of Treatment Outcomes for Children with Generalized Anxiety Disorder. Child Psychiatry Hum. Dev. 2019, 50, 449–458. [Google Scholar] [CrossRef]
- Normann, N.; Lønfeldt, N.; Reinholdt-Dunne, M.L.; Esbjørn, B.H. Negative Thoughts and Metacognitions in Anxious Children Following CBT. Cogn. Ther. Res. 2016, 40, 188–197. [Google Scholar] [CrossRef]
- Holmes, M.C.; Donovan, C.L.; Farrell, L.J.; March, S. The efficacy of a group-based, disorder-specific treatment program for childhood GAD—A randomized controlled trial. Behav. Res. Ther. 2014, 61, 122–135. [Google Scholar] [CrossRef] [Green Version]
- Schneider, S.; Pflug, V.I.; Albon, T.-N.; Margraf, J. Kinder-DIPS Open Access: Diagnostisches Interview bei Psychischen Storungen im Kindes- und Jugendalter; Ruhr-Universität Bochum Forschungs- und Behandlungszentrum für psychische Gesundheit: Bochum, Germany, 2017. [Google Scholar]
- Margraf, J.; Cwik, J.; Pflug, V.; Schneider, S. Strukturierte klinische Interviews zur Erfassung psychischer Störungen über die Lebensspanne. Z Klin. Psychol. Psychother. 2017, 46, 176–186. [Google Scholar] [CrossRef]
- Weber, L.; Christiansen, H.; Chavanon, M.L. Diagnoseerhebung mit strukturiertem Interview: Übereinstimmung von klinischem Urteil und Kinder-DIPS. Verhaltenstherapie 2020, 30, 281–292. [Google Scholar] [CrossRef]
- Neuschwander, M.; In-Albon, T.; Meyer, A.H.; Schneider, S. Acceptance of a structured diagnostic interview in children, parents, and interviewers. Int. J. Methods Psychiatr. Res. 2017, 26, e1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Currie, C.; Roberts, C.; Morgan, A.; Smith, R.; Settertobulte, W.; Samdal, O.; Rasmussen, V.B. Young People’s Health in Context. Health Behaviour in School-Aged Children Study: International Report from The 2001/2002 Survey; WHO Regional Office for Europe: Copenhagen, Denmark, 2004. [Google Scholar]
- Döpfner, M.; Görtz-Dorten, A.; Lehmkuhl, G. Diagnostik-System für Psychische Störungen nach ICD-10 und DSM-IV für Kinder und Jugendliche-II: DISYPS-II; Hogrefe: Bern, Switzerland, 2008. [Google Scholar]
- Goletz, H.; Yang, Y.-I.; Suhr-Dachs, L.; Walter, D.; Döpfner, M. Alltagswirksamkeit kognitiver Verhaltenstherapie bei Kindern und Jugendlichen mit Angststörungen in einer Ausbildungsambulanz. Z Kinder Jugendpsychiatr. Psychother. 2013, 41, 247–260. [Google Scholar] [CrossRef]
- Piepenbreier, S. Metakognitive Prozesse im Kindes-und Jugendalter: Eine explorative Studie zur Bedeutung von Metakognitionen für Angst-und Zwangssymptome im Kindes-und Jugendalter. Unpublished Thesis, Philipps-Universität Marburg, Marburg, Germany, 2015. [Google Scholar]
- Silverman, W.K.; Albano, A.M. The Anxiety Disorders Interview Schedule for Children for DSM-IV: (Child and Parent Versions); Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Chorpita, B.F.; Tracey, S.A.; Brown, T.A.; Collica, T.J.; Barlow, D.H. Assessment of worry in children and adolescents: An adaptation of the Penn State Worry Questionnaire. Behav. Res. Ther. 1997, 35, 569–581. [Google Scholar] [CrossRef]
- Ehring, T.; Raes, F.; Weidacker, K.; Emmelkamp, P. Validation of the Dutch Version of the Perseverative Thinking Questionnaire (PTQ-NL). Eur. J. Psychol. Assess. 2012, 28, 102–108. [Google Scholar] [CrossRef]
- De Voogd, E.L.; Wiers, R.W.; Salemink, E. Online visual search attentional bias modification for adolescents with heightened anxiety and depressive symptoms: A randomized controlled trial. Behav. Res. Ther. 2017, 92, 57–67. [Google Scholar] [CrossRef]
- Naumann, L. Understanding and Assessing Worrying—Analyzing Relevant Psychopathological Mechanisms Relevant for Generalized Anxiety Disorder Across the Lifespan. Unpublished Dissertation, Universität zu Köln, Köln, Germany, 2014. [Google Scholar]
- Arndt, A.; Patzelt, J.; Andor, T.; Hoyer, J.; Gerlach, A.L. Psychometrische Gütekriterien des Metakognitionsfragebogens (Kurzversion, MKF-30). Z. Klin. Psychol. Psychother. 2011, 40, 107–114. [Google Scholar] [CrossRef]
- Wells, A.; Cartwright-Hatton, S. A short form of the metacognitions questionnaire: Properties of the MCQ-30. Behav. Res. Ther. 2004, 42, 385–396. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Davidson, R.; MacKinnon, J.G. The Power of Bootstrap Tests; Queens University: Kingston, ON, Canada, 1996. [Google Scholar]
- Meyer, J.P.; Seaman, M.A. A Comparison of the Exact Kruskal-Wallis Distribution to Asymptotic Approximations for All Sample Sizes up to 105. J. Exp. Educ. 2013, 81, 139–156. [Google Scholar] [CrossRef]
- Mahoney, M.; Magel, R. Estimation of the Power of the Kruskal-Wallis Test. Biom. J. 1996, 38, 613–630. [Google Scholar] [CrossRef]
- Fan, C.; Zhang, D. A Note on Power and Sample Size Calculations for the Kruskal–Wallis Test for Ordered Categorical Data. J. Biopharm. Stat. 2012, 22, 1162–1173. [Google Scholar] [CrossRef]
- Lantz, B. The impact of sample non-normality on ANOVA and alternative methods. Br. J. Math. Stat. Psychol. 2013, 66, 224–244. [Google Scholar] [CrossRef]
- Van Hecke, T. Power study of anova versus Kruskal-Wallis test. J. Stat. Manag. Syst. 2010, 15, 241–247. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Wolenski, R.; Vaclavik, D.; Rey, Y.; Pettit, J.W. Metacognitive Beliefs Predict Cognitive Behavioral Therapy Outcome in Children with Anxiety Disorders. Int. J. Cogn. Ther. 2021, 14, 687–703. [Google Scholar] [CrossRef]
- Simons, M.; Vloet, T.D. Emetophobia—A Metacognitive Therapeutic Approach for an Overlooked Disorder. Z Kinder Jugend-psychiatr. Psychother. 2018, 46, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Thorslund, J.; McEvoy, P.M.; Anderson, R.A. Group metacognitive therapy for adolescents with anxiety and depressive disorders: A pilot study. J. Clin. Psychol. 2020, 76, 625–645. [Google Scholar] [CrossRef] [PubMed]
- Lønfeldt, N.N.; Marin, C.E.; Silverman, W.K.; Reinholdt-Dunne, M.L.; Esbjørn, B.H. The Role of Metacognitions in the Association between Children’s Perceptions of Maternal Control and Anxiety. J. Child Fam. Stud. 2017, 26, 1398–1408. [Google Scholar] [CrossRef]
- Matthews, L.; Reynolds, S.; Derisley, J. Examining Cognitive Models of Obsessive Compulsive Disorder in Adolescents. Behav. Cogn. Psychother. 2006, 35, 149–163. [Google Scholar] [CrossRef]
- Merikangas, K.R.; He, J.-P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Voogd, E.L.; Wiers, R.; Zwitser, R.J.; Salemink, E. Emotional working memory training as an online intervention for adolescent anxiety and depression: A randomised controlled trial. Aust. J. Psychol. 2016, 68, 228–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Total | SAD | SepAD | SP |
|---|---|---|---|---|
| n = 31 | n = 7 | n = 12 | n = 12 | |
| Age, M (SD) | 10.36 (2.17) | 10.05 (1.99) | 9.84 (1.41) | 10.25 (2.49) |
| Gender, n (%) female | 16 (51.6) | 5 (71.4) | 5 (41.7) | 6 (50.0) |
| School type, n (%) | ||||
| elementary school | 15 (48.4) | 3 (42.9) | 6 (50.0) | 6 (50.0) |
| grammar school | 8 (25.8) | 1 (14.3) | 4 (33.3) | 3 (25.0) |
| comprehensive secondary school | 4 (12.9) | 1 (14.3) | 1 (8.3) | 2 (16.7) |
| secondary school | 3 (9.7) | 2 (28.6) | - | 1 (8.3) |
| school for special needs | 1 (3.2) | - | 1 (8.3) | - |
| FAS-II, n (%) a | ||||
| High family wealth | 20 (64.5) | 5 (71.4) | 7 (58.3) | 8 (66.7) |
| Moderate family wealth | 6 (19.4) | 1 (14.3) | 3 (25.0) | 2 (16.7) |
| Low family wealth | 4 (12.9) | 1 (14.3) | 1 (8.3) | 2 (16.7) |
| Comorbid disorder, n (%) | ||||
| None | 10 (32.3) | - | 4 (33.3) | 6 (50.0) |
| One | 10 (32.3) | 5 (71.4) | 4 (33.3) | 1 (8.3) |
| Two or more | 11 (35.4) | 2 (28.6) | 4 (33.3) | 5 (41.7) |
| Comorbid GAD | 1 (3.2) | - | - | 1 (8.3) |
| Randomization, n (%) | ||||
| With caregiver/parent | 16 (51.6) | 5 (71.4) | 6 (50.0) | 5 (41.7) |
| Without caregiver/parent | 15 (48.4) | 2 (28.6) | 6 (50.0) | 7 (58.3) |
| Measure | Pretest | Posttest | Test Statistic | d | ||
|---|---|---|---|---|---|---|
| Range | M (SD) | Range | M (SD) | |||
| ANZchild | 3.0–50.0 | 23.64 (14.62) a | 0.0–32.0 | 9.89 (10.59) a | 95%-CI [9.37; 18.16] *,b | 1.077 |
| ANZparent | 3.0–40.0 | 19.69 (10.26) a | 0.0–23.0 | 8.43 (6.32) a | t(24) = 6.295, p < 0.001 * | 1.321 |
| EWC | 0.0–23.0 | 8.86 (6.27) | 0.0–13.0 | 5.31 (4.14) | t(25) = 4.027, p < 0.001 * | 0.668 |
| PTQ | 0.0–49.3 | 14.65 (11.55) | 0.0–38.0 | 10.35 (10.79) | t(25) = 2.256, p = 0.017 | 0.385 |
| MKF-POS | 0.0–8.0 | 1.35 (2.28) | 0.0–5.0 | 0.92 (1.60) | 95%-CI [−0.44; 1.40] b | 0.218 |
| MKF-NEG | 0.0–9.8 | 2.88 (2.24) | 0.0–8.0 | 2.31 (1.78) | 95%-CI [−0.33; 1.59] b | 0.282 |
| MKF-total | 1.0–38.0 | 14.90 (9.08) | 1.0–33.0 | 13.49 (9.15) | t(25) = 0.791, p = 0.219 | 0.155 |
| Measure | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|
| 1. Δ ANZchild a | 0.304 | 0.759 *** | 0.635 *** | 0.182 | 0.364 * | 0.483 ** |
| 2. Δ ANZparent a | 0.269 | 0.433 * | 0.209 | 0.347 * | 0.455 * | |
| 3. Δ EWC | 0.657 *** | 0.118 | 0.219 | 0.404 * | ||
| 4. Δ PTQ | 0.123 | 0.485 ** | 0.602 ** | |||
| 5. Δ MKF-POS | 0.163 | 0.515 ** | ||||
| 6. Δ MKF-NEG | 0.680 *** | |||||
| 7. Δ MKF-total |
| Measure | B | SE B | β | R2 |
|---|---|---|---|---|
| Δ ANZchild | 0.623 ** | |||
| Δ EWC | 1.593 | 0.457 | 0.646 * | |
| Δ PTQ | 0.136 | 0.249 | 0.115 | |
| Δ MKF-NEG | 0.706 | 0.692 | 0.163 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köcher, L.M.; Pflug, V.; Schneider, S.; Christiansen, H. Do Metacognitions of Children and Adolescents with Anxiety Disorders Change after Intensified Exposure Therapy? Children 2022, 9, 168. https://doi.org/10.3390/children9020168
Köcher LM, Pflug V, Schneider S, Christiansen H. Do Metacognitions of Children and Adolescents with Anxiety Disorders Change after Intensified Exposure Therapy? Children. 2022; 9(2):168. https://doi.org/10.3390/children9020168
Chicago/Turabian StyleKöcher, Laura Marie, Verena Pflug, Silvia Schneider, and Hanna Christiansen. 2022. "Do Metacognitions of Children and Adolescents with Anxiety Disorders Change after Intensified Exposure Therapy?" Children 9, no. 2: 168. https://doi.org/10.3390/children9020168