
Recreational Soccer Training Effects on Pediatric Populations Physical Fitness and Health: A Systematic Review
 ,
,  ,
,  , ,
, ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Extraction Process
2.6. Data Items
2.7. Study Risk of Bias Assessment
3. Results
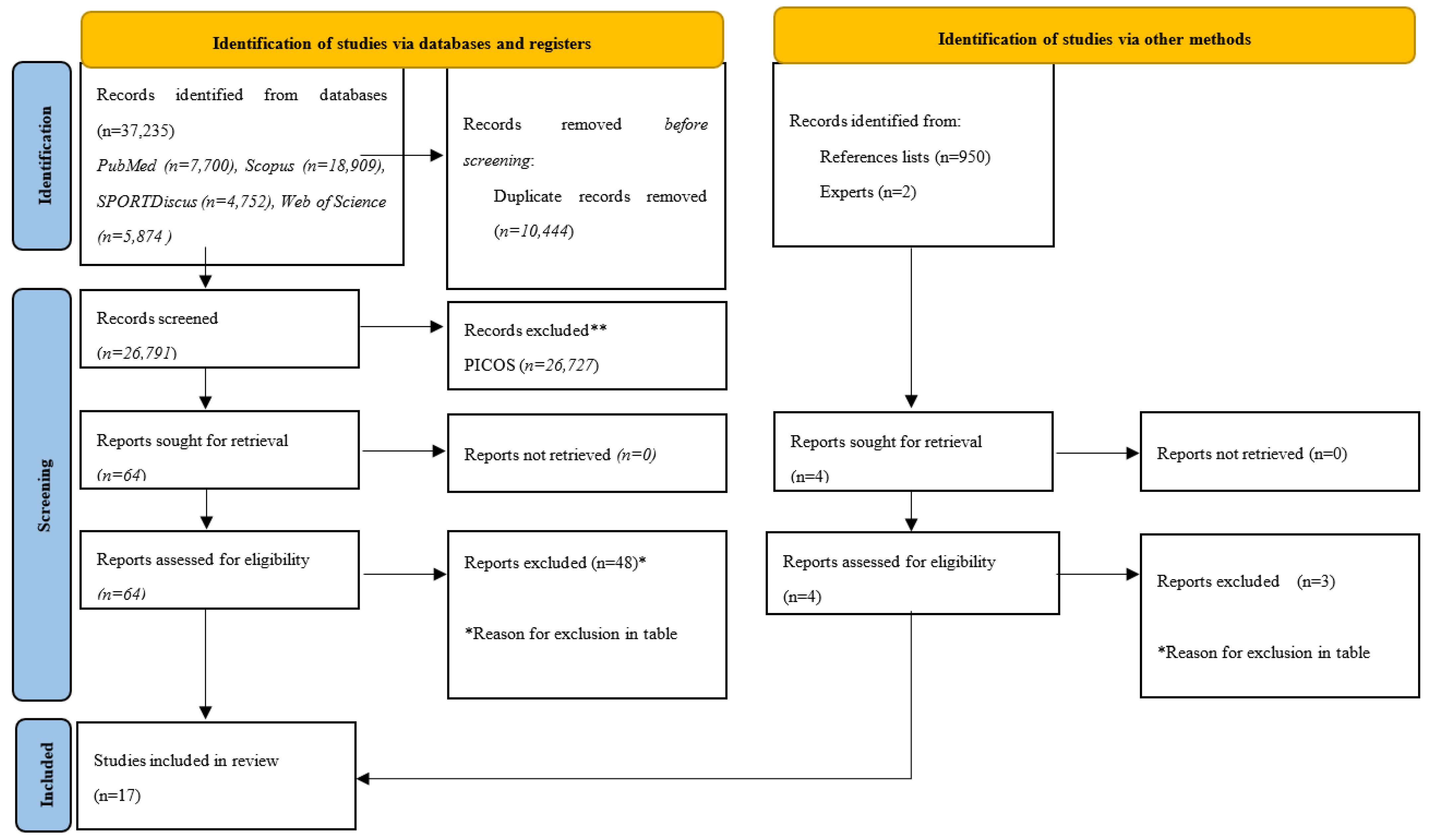
3.1. Study Identification and Selection
3.2. Study Characteristics
3.3. Risk of Bias in Studies
3.4. Results of Individual Studies
4. Discussion
4.1. Main Findings Regarding Physical Fitness
4.2. Main Findings in Relation to Body Composition
4.3. Main Findings Regarding Health-Related Outcomes
4.4. Behavioral Area
4.5. Cardiovascular Adaptations
4.6. Blood Pressure
4.7. Biochemical Parameters
4.8. Limitations
4.9. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biddle, S.J.H.; García Bengoechea, E.; Wiesner, G. Sedentary Behaviour and Adiposity in Youth: A Systematic Review of Reviews and Analysis of Causality. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, T.J.; Chaput, J.P.; Tremblay, M.S. Sedentary Behaviour as an Emerging Risk Factor for Cardiometabolic Diseases in Children and Youth. Can. J. Diabetes 2014, 38, 53–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- le Roux, E.; de Jong, N.P.; Blanc, S.; Simon, C.; Bessesen, D.H.; Bergouignan, A. Physiology of Physical Inactivity, Sedentary Behaviours and Non-exercise Activity: Insights from the Space Bedrest Model. J. Physiol. 2022, 600, 1037–1051. [Google Scholar] [CrossRef]
- Duvivier, B.M.F.M.; Schaper, N.C.; Bremers, M.A.; van Crombrugge, G.; Menheere, P.P.C.A.; Kars, M.; Savelberg, H.H.C.M. Minimal Intensity Physical Activity (Standing and Walking) of Longer Duration Improves Insulin Action and Plasma Lipids More than Shorter Periods of Moderate to Vigorous Exercise (Cycling) in Sedentary Subjects When Energy Expenditure Is Comparable. PLoS ONE 2013, 8, e55542. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Gorely, T.; Marshall, S.J.; Murdey, I.; Cameron, N. Physical Activity and Sedentary Behaviours in Youth: Issues and Controversies. J. R. Soc. Promot. Health 2004, 124, 29–33. [Google Scholar] [CrossRef]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S.; et al. Systematic Review of Sedentary Behaviour and Health Indicators in School-Aged Children and Youth: An Update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaput, J.-P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO Guidelines on Physical Activity and Sedentary Behaviour for Children and Adolescents Aged 5–17 Years: Summary of the Evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- Hallal, P.C.; Victora, C.G.; Azevedo, M.R.; Wells, J.C.K. Adolescent Physical Activity and Health: A Systematic Review. Sports Med. 2006, 36, 1019–1030. [Google Scholar] [CrossRef]
- Castagna, C.; de Sousa, M.; Krustrup, P.; Kirkendall, D.T. Recreational Team Sports: The Motivational Medicine. J. Sport Health Sci. 2018, 7, 129. [Google Scholar] [CrossRef]
- Milanović, Z.; Pantelić, S.; Čović, N.; Sporiš, G.; Mohr, M.; Krustrup, P. Broad-Spectrum Physical Fitness Benefits of Recreational Football: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2019, 53, 926–939. [Google Scholar] [CrossRef]
- Andersen, L.J.; Hansen, P.R.; Søgaard, P.; Madsen, J.K.; Bech, J.; Krustrup, P. Improvement of Systolic and Diastolic Heart Function after Physical Training in Sedentary Women. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. S1), 50–57. [Google Scholar] [CrossRef] [PubMed]
- Milanović, Z.; Pantelić, S.; Kostić, R.; Trajković, N.; Sporiš, G. Soccer vs. Running Training Effects in Young Adult Men: Which Programme Is More Effective in Improvement of Body Composition? Randomized Controlled Trial. Biol. Sport 2015, 32, 301–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montealegre Suárez, D.; Lerma Castaño, P.; Rojas Calderón, M.; Perdomo Trujillo, J.; Torres Méndez, M. Condición Física de Niños Futbolistas En Función de La Posición de Juego (Physical Condition of Children Footballers Depending on the Playing Position). Rev. Iberoam. De Cienc. De La Act. Física Y El Deporte 2020, 9, 23. [Google Scholar] [CrossRef] [Green Version]
- Ayala Hernández, H.; Rivera Girón, A.; Castineyra Mendoza, S.; Gómez Figueroa, J. Influencia de La Educación Física en Jugadores de Fútbol Asociación Sub-13 y Sub-15 (INFLUENCE OF PHYSICAL EDUCATION IN U-13 AND U-15 ASSOCIATION SOCCER PLAYERS). Rev. Iberoam. De Cienc. De La Act. Física Y El Deporte 2021, 10, 37–46. [Google Scholar] [CrossRef]
- Sarmento, H.; Manuel Clemente, F.; Marques, A.; Milanovic, Z.; David Harper, L.; Figueiredo, A. Recreational Football Is Medicine against Non-Communicable Diseases: A Systematic Review. Scand. J. Med. Sci. Sports 2020, 30, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Helge, E.W.; Aagaard, P.; Jakobsen, M.D.; Sundstrup, E.; Randers, M.B.; Karlsson, M.K.; Krustrup, P. Recreational Football Training Decreases Risk Factors for Bone Fractures in Untrained Premenopausal Women. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. S1), 31–39. [Google Scholar] [CrossRef]
- Mielke, G.I.; Bailey, T.G.; Burton, N.W.; Brown, W.J. Participation in sports/recreational activities and incidence of hypertension, diabetes, and obesity in adults. Scand. J. Med. Sci. Sports 2020, 30, 2390–2398. [Google Scholar] [CrossRef] [PubMed]
- Pinho, C.D.F.; Farinha, J.B.; Lisboa, S.D.C.; Bagatini, N.C.; Leites, G.T.; Voser, R.D.C.; Gaya, A.R.; Reischak-Oliveira, A.; Cunha, G.D.S. Effects of a small-sided soccer program on health parameters in obese children. Rev. Brasileira Med. Esporte 2022, 29. [Google Scholar] [CrossRef]
- Tsorbatzoudis, H.; Alexandris, K.; Zahariadis, P.; Grouios, G. Examining the Relationship between Recreational Sport Participation and Intrinsic and Extrinsic Motivation and Amotivation. Percept. Mot. Ski. 2006, 103, 363–374. [Google Scholar] [CrossRef]
- Milanović, Z.; Pantelić, S.; Čović, N.; Sporiš, G.; Krustrup, P.; Milanovic, Z.; Pantelic, S.; Covic, N.; Sporis, G.; Krustrup, P. Is Recreational Soccer Effective for Improving VO2max ? A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1339–1353. [Google Scholar] [CrossRef]
- Luo, H.; Newton, R.U.; Ma’ayah, F.; Galvão, D.A.; Taaffe, D.R. Recreational Soccer as Sport Medicine for Middle-Aged and Older Adults: A Systematic Review. BMJ Open Sport Exerc. Med. 2018, 4, e000336. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.; González-Fernández, F.; Ceylan, H.; Silva, R.; Ramirez-Campillo, R. Effects of Recreational Soccer on Fat Mass in Untrained Sedentary Adults: A Systematic Review with Meta-Analysis. Hum. Mov. 2022, 23, 15–32. [Google Scholar] [CrossRef]
- Krustrup, P.; Aagaard, P.; Nybo, L.; Petersen, J.; Mohr, M.; Bangsbo, J. Recreational football as a health promoting activity: A topical review. Scand. J. Med. Sci. Sports 2010, 20, 1–13. [Google Scholar] [CrossRef]
- Castillo-Bellot, I.; Mora-Gonzalez, J.; Fradua, L.; Ortega, F.B.; Gracia-Marco, L. Effects of Recreational Soccer on Health Outcomes: A Narrative Review. J Sci Sport and Exercise 2019, 1, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Hammami, A.; Chamari, K.; Slimani, M.; Shephard, R.; Yousfi, N.; Tabka, Z.; Bouhlel, E. Effects of Recreational Soccer on Physical Fitness and Health Indices in Sedentary Healthy and Unhealthy Subjects. Biol. Sport 2016, 33, 127–137. [Google Scholar] [CrossRef]
- Clemente, F.M.; Ramirez-Campillo, R.; Sarmento, H.; Castillo, D.; Raya-González, J.; Rosemann, T.; Knechtle, B. Effects of Recreational Small-Sided Soccer Games on Bone Mineral Density in Untrained Adults: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 457. [Google Scholar] [CrossRef]
- Milanović, Z.; Čović, N.; Helge, E.W.; Krustrup, P.; Mohr, M. Recreational Football and Bone Health: A Systematic Review and Meta-Analysis. Sports Med. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Rechenchosky, L.; Menegassi, V.M.; Jaime, M.D.O.; Borges, P.H.; Sarmento, H.; Mancha-Triguero, D.; Serra-Olivares, J.; Rinaldi, W. Scoping Review of Tests to Assess Tactical Knowledge and Tactical Performance of Young Soccer Players. J. Sports Sci. 2021, 39, 2051–2067. [Google Scholar] [CrossRef]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2021. [Google Scholar]
- Wong, S.S.-L.; Wilczynski, N.L.; Haynes, R.B. Developing Optimal Search Strategies for Detecting Clinically Sound Treatment Studies in EMBASE. J. Med. Libr. Assoc. 2006, 94, 41–47. [Google Scholar] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, M.N.; Nielsen, C.M.; Ørntoft, C.; Randers, M.B.; Helge, E.W.; Madsen, M.; Manniche, V.; Hansen, L.; Hansen, P.R.; Bangsbo, J.; et al. Fitness Effects of 10-Month Frequent Low-Volume Ball Game Training or Interval Running for 8-10-Year-Old School Children. Biomed Res. Int. 2017, 2017, 2719752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, M.N.; Nielsen, C.M.; Helge, E.W.; Madsen, M.; Manniche, V.; Hansen, L.; Hansen, P.R.; Bangsbo, J.; Krustrup, P. Positive Effects on Bone Mineralisation and Muscular Fitness after 10 Months of Intense School-Based Physical Training for Children Aged 8–10 Years: The FIT FIRST Randomised Controlled Trial. Br. J. Sports Med. 2018, 52, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.N.; Nielsen, C.M.; Madsen, M.; Manniche, V.; Hansen, L.; Bangsbo, J.; Krustrup, P.; Hansen, P.R. Cardiovascular Adaptations after 10 Months of Intense School-Based Physical Training for 8- to 10-Year-Old Children. Scand. J. Med. Sci. Sports 2018, 28 (Suppl. S1), 33–41. [Google Scholar] [CrossRef]
- Larsen, M.N.; Madsen, M.; Nielsen, C.M.; Manniche, V.; Hansen, L.; Bangsbo, J.; Krustrup, P.; Hansen, P.R. Cardiovascular Adaptations after 10 months of Daily 12-Min Bouts of Intense School-Based Physical Training for 8-10-Year-Old Children. Prog. Cardiovasc. Dis. 2020, 63, 813–817. [Google Scholar] [CrossRef]
- Krustrup, P.; Hansen, P.R.; Nielsen, C.M.; Larsen, M.N.; Randers, M.B.; Manniche, V.; Hansen, L.; Dvorak, J.; Bangsbo, J. Structural and Functional Cardiac Adaptations to a 10-Week School-Based Football Intervention for 9-10-Year-Old Children. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. S1), 4–9. [Google Scholar] [CrossRef]
- Hammami, A.; Kasmi, S.; Razgallah, M.; Tabka, Z.; Shephard, R.J.; Bouhlel, E. Recreational Soccer Training Improves Heart-Rate Variability Indices and Physical Performance in Untrained Healthy Adolescent. Sport Sci. Health 2017, 13, 507–514. [Google Scholar] [CrossRef]
- Cvetković, N.; Stojanović, E.; Stojiljković, N.; Nikolić, D.; Milanović, Z. Effects of a 12 Week Recreational Football and High-intensity Interval Training on Physical Fitness in Overweight Children./Efekti Rekreativnog Fudbala od 12 Nedelja i Intervalnog Treninga Visokog Intenziteta (Hiit) Na Fizičku Spremnost Kod dece Sa Prek. Facta Univ. Ser. Phys. Educ. Sport 2018, 16, 435–450. [Google Scholar]
- Cvetković, N.; Stojanović, E.; Stojiljković, N.; Nikolić, D.; Scanlan, A.T.; Milanović, Z. Exercise Training in Overweight and Obese Children: Recreational Football and High-Intensity Interval Training Provide Similar Benefits to Physical Fitness. Scand. J. Med. Sci. Sports 2018, 28 (Suppl. S1), 18–32. [Google Scholar] [CrossRef]
- Hammami, A.; Randers, M.B.; Kasmi, S.; Razgallah, M.; Tabka, Z.; Chamari, K.; Bouhlel, E. Effects of Soccer Training on Health-Related Physical Fitness Measures in Male Adolescents. J. Sport Health Sci. 2018, 7, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Lind, R.R.; Geertsen, S.S.; Ørntoft, C.; Madsen, M.; Larsen, M.N.; Dvorak, J.; Ritz, C.; Krustrup, P. Improved Cognitive Performance in Preadolescent Danish Children after the School-Based Physical Activity Programme “FIFA 11 for Health” for Europe-A Cluster-Randomised Controlled Trial. Eur. J. Sport Sci. 2018, 18, 130–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skoradal, M.B.; Purkhús, E.; Steinholm, H.; Olsen, M.H.; Ørntoft, C.; Larsen, M.N.; Dvorak, J.; Mohr, M.; Krustrup, P. “FIFA 11 for Health” for Europe in the Faroe Islands: Effects on Health Markers and Physical Fitness in 10- to 12-Year-Old Schoolchildren. Scand. J. Med. Sci. Sports 2018, 28 (Suppl. S1), 8–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Cao, L.; Xie, P.; Wang, J. Recreational Football Training Improved Health-Related Physical Fitness in 9- to 10-Year-Old Boys. J. Sports Med. Phys. Fitness 2018, 58, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Trajkovi, N.; Madic, D.M.; Milanovic, Z.; MacAk, D.; Padulo, J.; Krustrup, P.; Chamari, K. Eight Months of School-Based Soccer Improves Physical Fitness and Reduces Aggression in High-School Children. Biol. Sport 2020, 37, 185–193. [Google Scholar] [CrossRef]
- Vasconcellos, F.; Cunha, F.A.; Gonet, D.T.; Farinatti, P.T.V. Does Recreational Soccer Change Metabolic Syndrome Status in Obese Adolescents? A Pilot Study. Res. Q. Exerc. Sport 2021, 92, 91–99. [Google Scholar] [CrossRef]
- Mohammed, M.H.H.; Al-Qahtani, M.H.H.; Takken, T. Effects of 12 Weeks of Recreational Football (Soccer) with Caloric Control on Glycemia and Cardiovascular Health of Adolescent Boys with Type 1 Diabetes. Pediatr. Diabetes 2021, 22, 625–637. [Google Scholar] [CrossRef]
- Hadjicharalambous, M.; Zaras, N.; Apostolidis, A.; Tsofliou, F. Recreational Soccer, Body Composition and Cardiometabolic Health: A Training-Intervention Study in Healthy Adolescents. Int. J. Hum. Mov. Sports Sci. 2022, 10, 524–533. [Google Scholar] [CrossRef]
- Ryom, K.; Christiansen, S.R.; Elbe, A.M.; Aggestrup, C.S.; Madsen, E.E.; Madsen, M.; Larsen, M.N.; Krustrup, P. The Danish “11 for Health” Program Raises Health Knowledge, Well-Being, and Fitness in Ethnic Minority 10- to 12-Year-Olds. Scand. J. Med. Sci. Sports 2022, 32, 138–151. [Google Scholar] [CrossRef]
- Vasconcellos, F.; Seabra, A.; Cunha, F.; Montenegro, R.; Penha, J.; Bouskela, E.; Nogueira Neto, J.F.; Collett-Solberg, P.; Farinatti, P. Health Markers in Obese Adolescents Improved by a 12-Week Recreational Soccer Program: A Randomised Controlled Trial. J. Sports Sci. 2016, 34, 564–575. [Google Scholar] [CrossRef]
- Abrignani, M.G.; Lucà, F.; Favilli, S.; Benvenuto, M.; Rao, C.M.; di Fusco, S.A.; Gabrielli, D.; Gulizia, M.M. Lifestyles and Cardiovascular Prevention in Childhood and Adolescence. Pediatr. Cardiol. 2019, 40, 1113–1125. [Google Scholar] [CrossRef] [PubMed]
- Drozdz, D.; Alvarez-Pitti, J.; Wójcik, M.; Borghi, C.; Gabbianelli, R.; Mazur, A.; Herceg-čavrak, V.; Lopez-Valcarcel, B.G.; Brzeziński, M.; Lurbe, E.; et al. Obesity and Cardiometabolic Risk Factors: From Childhood to Adulthood. Nutrients 2021, 13, 4176. [Google Scholar] [CrossRef] [PubMed]
- de Jesus, J.M. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics 2011, 128, S213–S256. [Google Scholar]
- Lang, J.J.; Belanger, K.; Poitras, V.; Janssen, I.; Tomkinson, G.R.; Tremblay, M.S. Systematic Review of the Relationship between 20 m Shuttle Run Performance and Health Indicators among Children and Youth. J. Sci. Med. Sport 2018, 21, 383–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Högström, G.; Nordström, A.; Nordström, P. High Aerobic Fitness in Late Adolescence Is Associated with a Reduced Risk of Myocardial Infarction Later in Life: A Nationwide Cohort Study in Men. Eur. Heart J. 2014, 35, 3133–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical Fitness in Childhood and Adolescence: A Powerful Marker of Health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Labayen, I.; Martínez-Gómez, D.; Vicente-Rodriguez, G.; Cuenca- García, M.; Gracia-Marco, L.; Manios, Y.; Beghin, L.; Molnar, D.; et al. Health Inequalities in Urban Adolescents: Role of Physical Activity, Diet, and Genetics. Pediatrics 2014, 133, e884–e895. [Google Scholar] [CrossRef]
- Soares, I.F.; Cunha, F.A.; Vasconcellos, F. Effects of a 12-Week Recreational Soccer Program on Resting Metabolic Rate Among Adolescents with Obesity. J. Sci. Sport Exerc. 2022. [CrossRef]
- Faude, O.; Kerper, O.; Multhaupt, M.; Winter, C.; Beziel, K.; Junge, A.; Meyer, T. Football to Tackle Overweight in Children. Scand. J. Med. Sci. Sports 2010, 20, 103–110. [Google Scholar] [CrossRef]
- Zouhal, H.; Hammami, A.; Tijani, J.M.; Jayavel, A.; de Sousa, M.; Krustrup, P.; Sghaeir, Z.; Granacher, U.; ben Abderrahman, A. Effects of Small-Sided Soccer Games on Physical Fitness, Physiological Responses, and Health Indices in Untrained Individuals and Clinical Populations: A Systematic Review. Sports Med. 2020, 50, 987–1007. [Google Scholar] [CrossRef]
- Castagna, C.; Krustrup, P.; Póvoas, S. Cardiovascular fitness and health effects of various types of team sports for adult and elderly inactive individuals-a brief narrative review. Progress in Cardiovascular Diseases 2020, 63, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Koyuncuoğlu Güngör, N. Overweight and Obesity in Children and Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, D.L.; Tirumalai, E.C.; Farish Haydel, K.; Fujimoto, M.; Fulton, J.E.; Robinson, T.N. Team Sports for Overweight Children the Stanford Sports to Prevent Obesity Randomized Trial (SPORT). Arch. Pediatr. Adolesc. Med. 2008, 162, 232–237. [Google Scholar] [CrossRef] [Green Version]
- Seabra, A.; Brito, J.; Figueiredo, P.; Beirão, L.; Seabra, A.; Carvalho, M.J.; Abreu, S.; Vale, S.; Pedretti, A.; Nascimento, H.; et al. School-Based Soccer Practice Is an Effective Strategy to Improve Cardiovascular and Metabolic Risk Factors in Overweight Children. Prog. Cardiovasc. Dis. 2020, 63, 807–812. [Google Scholar] [CrossRef]
- de Sousa, M.V.; Fukui, R.; Krustrup, P.; Pereira, R.M.R.; Silva, P.R.S.; Rodrigues, A.C.; de Andrade, J.L.; Hernandez, A.J.; da Silva, M.E.R. Positive Effects of Football on Fitness, Lipid Profile, and Insulin Resistance in Brazilian Patients with Type 2 Diabetes. Scand. J. Med. Sci. Sports 2014, 24, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Ørntoft, C.; Larsen, M.N.; Elbe, A.M.; Ottesen, L.; Junge, A.; Dvorak, J.; Krustrup, P. “FIFA 11 for Health” for Europe. 1: Effect on Health Knowledge and Well-Being of 10- to 12-Year-Old Danish School Children. Br. J. Sports Med. 2017, 51, 1483–1488. [Google Scholar] [CrossRef] [Green Version]
- Jovanović, R.; Nikolovski, D.; Radulović, O.; Novak, S. Physical Activity Influence on Nutritional Status of Preschool Children. Acta Med. Median. 2010, 49, 17–21. [Google Scholar]
- Atlantis, E.; Barnes, E.H.; Singh, M.A.F. Efficacy of Exercise for Treating Overweight in Children and Adolescents: A Systematic Review. Int. J. Obes. 2006, 30, 1027–1040. [Google Scholar] [CrossRef] [Green Version]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical Activity and Public Health. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Bauman, A. Physical Activity and Public Health: Updated Recommendation for Adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar] [CrossRef] [Green Version]
- Shaw, K.; Gennat, H.; O’Rourke, P.; del Mar, C. Exercise for Overweight or Obesity. Cochrane Database Syst. Rev. 2006, 2006, CD003817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ørntoft, C.; Fuller, C.W.; Larsen, M.N.; Bangsbo, J.; Dvorak, J.; Krustrup, P. “FIFA 11 for Health” for Europe. II: Effect on Health Markers and Physical Fitness in Danish Schoolchildren Aged 10-12 Years. Br. J. Sports Med. 2016, 50, 1394–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laskowski, E.R. The Role of Exercise in the Treatment of Obesity. PM&R 2012, 4, 840–844. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Ciaccioni, S.; Thomas, G.; Vergeer, I. Physical Activity and Mental Health in Children and Adolescents: An Updated Review of Reviews and an Analysis of Causality. Psychol. Sport Exerc. 2019, 42, 146–155. [Google Scholar] [CrossRef]
- Zolotarjova, J.; ten Velde, G.; Vreugdenhil, A.C.E. Effects of Multidisciplinary Interventions on Weight Loss and Health Outcomes in Children and Adolescents with Morbid Obesity. Obes. Rev. 2018, 19, 931–946. [Google Scholar] [CrossRef] [Green Version]
- Okoniewski, W.; Lu, K.D.; Forno, E. Weight Loss for Children and Adults with Obesity and Asthma a Systematic Review of Randomized Controlled Trials. Ann. Am. Thorac. Soc. 2019, 16, 613–625. [Google Scholar] [CrossRef]
- Herman, K.M.; Craig, C.L.; Gauvin, L.; Katzmarzyk, P.T. Tracking of Obesity and Physical Activity from Childhood to Adulthood: The Physical Activity Longitudinal Study. Int. J. Pediatric Obes. 2009, 4, 281–288. [Google Scholar] [CrossRef]
- Scharfen, H.E.; Memmert, D. The Relationship between Cognitive Functions and Sport-Specific Motor Skills in Elite Youth Soccer Players. Front. Psychol. 2019, 10, 817. [Google Scholar] [CrossRef]
- Sabarit, A.; Reigal, R.E.; Morillo-Baro, J.P.; de Mier, R.J.R.; Franquelo, A.; Hernández-Mendo, A.; Falcó, C.; Morales-Sánchez, V. Cognitive Functioning, Physical Fitness, and Game Performance in a Sample of Adolescent Soccer Players. Sustainability 2020, 12, 5245. [Google Scholar] [CrossRef]
- Erikstad, M.K.; Martin, L.J.; Haugen, T.; Høigaard, R. Group Cohesion, Needs Satisfaction, and Self-Regulated Learning: A One-Year Prospective Study of Elite Youth Soccer Players’ Perceptions of Their Club Team. Psychol. Sport Exerc. 2018, 39, 171–178. [Google Scholar] [CrossRef]
- Price, M.S.; Weiss, M.R. Relationships among Coach Leadership, Peer Leadership, and Adolescent Athletes’ Psychosocial and Team Outcomes: A Test of Transformational Leadership Theory. J. Appl. Sport Psychol. 2013, 25, 265–279. [Google Scholar] [CrossRef]
- Li, J.; Shao, W. Influence of Sports Activities on Prosocial Behavior of Children and Adolescents: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 6484. [Google Scholar] [CrossRef] [PubMed]
- Barczuk-Falęcka, M.; Małek, Ł.A.; Krysztofiak, H.; Roik, D.; Brzewski, M. Cardiac Magnetic Resonance Assessment of the Structural and Functional Cardiac Adaptations to Soccer Training in School-Aged Male Children. Pediatr. Cardiol. 2018, 39, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Zdravkovic, M.; Perunicic, J.; Krotin, M.; Ristic, M.; Vukomanovic, V.; Soldatovic, I.; Zdravkovic, D. Echocardiographic Study of Early Left Ventricular Remodeling in Highly Trained Preadolescent Footballers. J. Sci. Med. Sport 2010, 13, 602–606. [Google Scholar] [CrossRef]
- Scharhag, J.; Schneider, G.; Urhausen, A.; Rochette, V.; Kramann, B.; Kindermann, W. Athlete’s Heart Right and Left Ventricular Mass and Function in Male Endurance Athletes and Untrained Individuals Determined by Magnetic Resonance Imaging. J. Am. Coll. Cardiol. 2002, 40, 1856–1863. [Google Scholar] [CrossRef] [Green Version]
- Galderisi, M.; Cardim, N.; D’Andrea, A.; Bruder, O.; Cosyns, B.; Davin, L.; Donal, E.; Edvardsen, T.; Freitas, A.; Habib, G.; et al. Themulti-Modality Cardiac Imaging Approach to the Athletés Heart: An Expert Consensus of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 353–353r. [Google Scholar] [CrossRef]
- Unnithan, V.B.; Rowland, T.; George, K.; Bakhshi, A.; Beaumont, A.; Sculthorpe, N.; Lord, R.N.; Oxborough, D.L. Effect of Long-Term Soccer Training on Changes in Cardiac Function during Exercise in Elite Youth Soccer Players. Scand. J. Med. Sci. Sports 2022, 32, 892–902. [Google Scholar] [CrossRef]
- Weberruß, H.; Engl, T.; Baumgartner, L.; Mühlbauer, F.; Shehu, N.; Oberhoffer-Fritz, R. Cardiac Structure and Function in Junior Athletes: A Systematic Review of Echocardiographic Studies. Rev. Cardiovasc. Med. 2022, 23, 129. [Google Scholar] [CrossRef]
- Bellenger, C.R.; Fuller, J.T.; Thomson, R.L.; Davison, K.; Robertson, E.Y.; Buckley, J.D. Monitoring Athletic Training Status Through Autonomic Heart Rate Regulation: A Systematic Review and Meta-Analysis. Sports Med. 2016, 46, 1461–1486. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Saavedra, J.M.; Escalante, Y. Effects of Exercise on Resting Blood Pressure in Obese Children: A Meta-Analysis of Randomized Controlled Trials. Obes. Rev. 2013, 14, 919–928. [Google Scholar] [CrossRef]
- Knowles, G.; Pallan, M.; Thomas, G.N.; Ekelund, U.; Cheng, K.K.; Barrett, T.; Adab, P. Physical Activity and Blood Pressure in Primary School Children: A Longitudinal Study. Hypertension 2013, 61, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauer, R.M.; Clarke, W.R.; Mahoney, L.T.; Witt, J. Childhood Predictors for High Adult Blood Pressure: The Muscatine Study. Pediatr. Clin. North Am. 1993, 40, 23–40. [Google Scholar] [CrossRef]
- Cook, N.R.; Cohen, J.; Hebert, P.R.; Taylor, J.O.; Hennekens, C.H. Implications of Small Reductions in Diastolic Pressure for Primary Prevention. Arch. Intern. Med. 1995, 155, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Rowland, T.W. The Role of Physical Activity and Fitness in Children in the Prevention of Adult Cardiovascular Disease. Prog. Pediatric Cardiol. 2001, 12, 199–203. [Google Scholar] [CrossRef]
- Juonala, M.; Magnussen, C.G.; Venn, A.; Dwyer, T.; Burns, T.L.; Davis, P.H.; Chen, W.; Srinivasan, S.R.; Daniels, S.R.; Kähönen, M.; et al. Influence of Age on Associations between Childhood Risk Factors and Carotid Intima-Media Thickness in Adulthood: The Cardiovascular Risk in Young Finns Study, the Childhood Determinants of Adult Health Study, the Bogalusa Heart Study, and the Muscatine Study for the International Childhood Cardiovascular Cohort (I3C) Consortium. Circulation 2010, 122, 2514–2520. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Youth populations (under 18) with no restriction on sex or clinical conditions. Populations were included in Tier 0, indicating sedentary behavior, or Tier 1, indicating recreationally active, of the participant classification framework [30]; this means that: (Tier 0) they do not meet minimum activity guidelines, and, thus, can be considered inactive; or (Tier 1) they meet the World Health Organization minimum activity target and/or may participate in multiple sports/forms of activity. | Adults (>18 years old) or youths enrolled in Tiers 2 to 5 of the participant classification framework [30]. |
| Intervention | Players were exposed to a structured recreational soccer training program for a minimum of four weeks, with no restrictions on the maximum length. Similarly, there were no restrictions on training volume, intensity, or weekly training frequency. | Exposed to less than four weeks of training intervention. Exposed to training programs for other sports than soccer. |
| Comparator | Passive control groups (not exposed to other training interventions, while retaining their regular physical activity levels and lifestyle) or active control groups (exposed to other exercise programs, not including recreational soccer training) | Exposed to training programs, which included recreational soccer. |
| Outcomes | Physical fitness outcomes (e.g., cardiorespiratory measures, speed or change-of-direction measures, muscular strength and power measures, and balance measures) and/or body characteristics or composition (e.g., body mass index, fat mass, and lean mass) and/or health-related markers (e.g., biochemical markers and inflammatory markers) | Acute physiological and/or physical responses (i.e., responses to a single training session or those experienced during exercise). Socio/psychological factors. Technical/tactical factors. |
| Study design | Randomized parallel group design. | No randomized designs. No controlled designs. |
| Database | Specificities of the Databases | Search Strategy | Number of Articles in Automatic Search |
|---|---|---|---|
| PubMed | None to report | (recreation * OR untrain * OR health) AND (Soccer [Title/Abstract] OR Football [Title/Abstract]) | 7700 |
| Scopus | Search for title and abstract also includes keywords | (TITLE-ABS-KEY (soccer OR football) AND ALL (recreation * OR untrain * OR health)) | 18,909 |
| SPORTDiscus | None to report | TI (soccer or Football) AND TX (recreation * OR untrain * OR health) | 4752 |
| Web of Science | Search for title and abstract also includes keywords and its designated “topic” | Soccer OR Football (Title) and recreation * OR untrain * OR health (Topic) | 5874 |
| Study | Clinical Registration | Country | N | Age (Years) | Sex | Assessments (Number) | Tests Applied | Outcomes Presented in the Study |
|---|---|---|---|---|---|---|---|---|
| [39] | Not reported | Germany | 22 | 10.8 ± 1.2 | Both | 3 (pre, mid, post) | Anthropometry; cycling ergometry; CMJ; sit-and-reach; OLS; agility run; 20-m shuttle run test | BMI; POmax; VO2max; lactate max; HRmax; CMJ height; change-of-direction time; 20-m shutle run time; HRmax at 20-m shutle run test; OLS time; sit-and-reach distance; |
| [34] | NCT01711892 | Denmark | 97 | 9.4 ± 0.4 | Both | 2 (pre, post) | Echocardiography; Anthropometry | BMI; systolic and diastolic BP; resting HR; LVDD; LVSD; LV; LA; LVEF; IVT; LVPWD; CO; DT; IVRT; RVDD; TAPSE |
| [40] | Not reported | Denmark | 526 | 11.1 ± 0.4 and 11.0 ± 0.5 | Both | 2 (pre, post) | Anthropometry; X-ray absorptiometry; arterial blood pressure; 20-m sprint test; horizontal jump length; YYIRT; flamingo balance test | BMI; body fat; lean mass; systolic and diastolic BP; mean arterial pressure; resting HR; YYIRT distance; 20-m sprint time; flaming balance; horizontal jump length. |
| [41] | TCTR20150512001 | Brazil | 30 | 14.1 ± 1.3 and 14.8 ± 1.4 | Both | 2 (pre, post) | Anthropometry; X-ray absorptiometry; arterial blood pressure; cardiopulmonary exercise testing; heart rate variability; biochemical markers; endothelial function assessment; inflammatory biomarkers | BMI; body fat; fat-free mass; systolic and diastolic BP; mean blood pressure; maximal oxygen uptake; HRmax; total cholesterol; HDL; LDL; triglycerides; C-reactive protein; fasting glucose; glucose tolerance; insulin; HOMA-IR; leptin; IL-6; resistin; TNF-α; adiponectin; ET-1; NEFA. |
| [42] | Not reported | NA | 22 | 15.9 ± 0.6 | Boys | 2 (pre, post) | Anthropometry; arterial blood pressure; heart rate variability; resting heart rate; YYIRT; 20-m sprint test; bilateral standing long jump; stork balance test. | Sum of skinfolds; systolic and diastolic BP; HR rest; Ln SDNN; Ln rMSSD; Ln HF; HF; Ln LF; LF; LF/HF; SD1; YYIRT distance; balance time; sprint time; jump distance. |
| [35] | Not reported | NA | 35 | 11 to 13 | Boys | 2 (pre, post) | CMJ test; 10- and 30-m sprints; leg spreading, lying on the back; flexibility of the body when bending; flexibility of the body when stretching; biochemical markers. | CMJ; Sprint time at 10 and 30 m; leg spreading lying on the back; flexibility of the body when bending; flexibility of the body when stretching; leukocytes; erythrocytes; hemoglobin; glucose; cholesterol; triglycerides. |
| [36] | Not reported | NA | 35 | 11 to 13 | Boys | 2 (pre, post) | Bioimpedance; CMJ test; agility t-test; sit-and-reach test; YYIRT; blood pressure. | BMI; body fat; lean body mass; muscle mass; CMJ; agility test; sit-and-reach test; YYIRT; resting and maximal HR; systolic and diastolic BP. |
| [43] | Not reported | NA | 20 | 15.9 ± 0.6 | Boys | 2 (pre, post) | Anthropometry; YYIRT; 10- and 20-m sprint; sit-and-reach test; CMJ; standing long jump; stork balance test. | BMI; body fat; lean mass; sprint time; CMJ height; standing long-jump; sit-and-reach distance; balance; YYIRT distance. |
| [38] | NCT02000492 | Denmark | 295 | 9.3 ± 0.4 | Both | 2 (pre, post) | Anthropometry; X-ray absorptiometry; flamingo balance test; horizontal jump test; 20-m sprint test; coordination wall with three stages of increased difficulty. | Bone mineral content; lean mass; areal bone mineral density; the number of falls in the balance test; sprint time; coordination ability. |
| [44] | H-16026885 | Denmark | 931 | 11.9 ± 0.4 11.8 ± 0.2 | Both | 2 (pre, post) | Cognitive test battery, including detection, identification, and one-back and one-card learning tasks. | Psychomotor function; attention; working memory; visual memory. |
| [45] | Not reported | Faroe Islands | 491 | 11.1 ± 0.3 | Both | 2 (pre, post) | Anthropometry; X-ray absorptiometry; blood pressure; stork balance test; horizontal jump test; YYIRT. | Systolic and diastolic BP; mean arterial pressure; resting HR; BMI; body fat; lean body mass; horizontal jump; postural balance; YYIRT distance. |
| [37] | Not reported | China | 38 | 9 to 10 | Boys | 2 (pre, post) | Anthropometry; X-ray absorptiometry; 20-m shuttle run test; 50-m sprint; standing long jump; handgrip; 1-min sit up; sit-and-reach; single-leg standing, | BMI; body fat; fat mass and fat-free mass; maximal oxygen uptake; sprint time; standing long jump distance; 1-min sit-up; core muscle function; body balance; heart rate index. |
| [46] | No reported | NA | 105 | 15.7 ± 0.6 | Both | 2 (pre, post) | Anthropometry; backward overhead medicine ball (3 kg) throw test; vertical jump test; YYIRT. | BMI; backward overhead medicine ball throw distance; vertical jump; YYIRT distance |
| [47] | TCTR20150512001 | Brazil | 13 | 13.9 ± 1.6 14.7 ± 2.3 | Both | 2 (pre, post) | Anthropometry; blood pressure; biochemical markers. | BMI; systolic and diastolic BP; body fat; HDL: triglycerides; fasting blood glucose level. |
| [48] | Not reported | Saudi Arabia | 30 | 14.4 ± 2.0 15.6 ± 1.8 17.8 ± 0.4 | Boys | 2 (pre, post) | Blood pressure; blood glucose monitoring; biochemical markers. | LDL; HDL; triglyceride; systolic and diastolic blood pressure; total day insulin; fasting blood glucose; HbA1c. |
| [49] | REC-010712 | NA | 53 | 17.0 ± 0.6 16.7 ± 0.4 16.7 ± 0.4 | Boys | 2 (pre, post) | Anthropometry; multistage fitness test; push-up test; abdominal curl conditioning test; blood pressure. | BMI; body fat; systolic and diastolic BP; resting HR; VO2max; sit-ups; push-ups. |
| [50] | H-16026885 | Denmark | 1122 | 11.6 ± 0.5 11.4 ± 0.5 | Both | 2 (pre, post) | Anthropometry; bioimpedance; blood pressure; YYIRT; stork balance stand test; standing long jump. | YYIRT distance; VO2max; BMI; standing forward jump; balance; body fat; muscle mass; systolic and diastolic BP; resting HR. |
| Study | Training Attendance | Duration | Days Per Week | Total Sessions | Training Duration (min) | Sets (n) | Recovery (min) | Work Duration (min) | Work Intensity | Training Drills |
|---|---|---|---|---|---|---|---|---|---|---|
| [39] | 60 to 69% | 6 months | 3 | 54 | 60 | NA | NA | NA | 80 ± 8% HRmax | Warm-up; SSGs (50%); technique (20%); fitness courses with a ball (20%) |
| [34] | 77 ± 18% | 10 weeks | 3 | 21 ± 5 | 49 | NA | NA | NA | 71 ± 6% HRmax | Warm-up; SSGs. |
| [40] | NA | 11 weeks | 2 | 22 | 45 | NA | NA | NA | NA | Technique; SSGs |
| [41] | NA | 12 weeks | 3 | 36 | 52.1 ± 5.6 | NA | NA | NA | 84.5 ± 4.1% HRmax | Warm-up (10 min); SSGs (40 min; cool-down (10 min) |
| [42] | NA | 8 weeks | 2 | 16 | NA | NA | NA | NA | NA | Warm-up; SSGs (30–45 min) |
| [35] | >50% | 12 weeks | NA | NA | 60 | 4 | 2 min | 8 min per set | 75.1 ± 2.3% HRmax | Warm-up (10 min); SSGs (32 min); cool-down (10 min) |
| [36] | >50% | 12 weeks | NA | NA | 60 | 4 | 2 min | 8 min per set | 75.1 ± 2.3% HRmax | Warm-up (10 min); SSGs (32 min); cool-down (10 min) |
| [43] | NA | 8 weeks | 2 | 16 | 30–45 | NA | NA | NA | 84.6 ± 6.3% HRpeak | Warm-up; SSGs (30–45 min) |
| [38] | NA | 10 months | 3 | NA | NA | NA | NA | NA | 0.48 ± 0.15 arbitrary units player load | Warm-up (3 to 5 min); SSGs |
| [44] | NA | 11 weeks | 2 | 22 | 45 | NA | NA | NA | NA | NA |
| [45] | NA | 11 weeks | 2 | 22 | 45 | NA | NA | NA | NA | SSGs. |
| [37] | NA | 10 weeks | 3 | 30 | 60 | NA | NA | NA | NA | Warm-up (10 min); dribbling (10 min); dribbling and shooting (10 min); passing (10 min); running (10 min); cool-down (10 min). |
| [46] | >85% | 32 weeks | 2 | 64 | 45 | 4 | 3 | 5 | NA | Warm-up (10 min); stretching (4 min); acceleration running (2 min); soccer (30 min); cool-down (5 min) |
| [47] | NA | 12 weeks | 3 | 36 | 60 | NA | NA | NA | 84.5 ± 4.1% HRmax | Warm-up (10 min); SSGs (40 min); cool-down (10 min) |
| [48] | 21–24 n | 12 weeks | 2 | 24 | 90 | NA | NA | NA | ~80% HRmax | Warm-up (5–10 min); game |
| [49] | NA | 8 weeks | NA | 28 | 60 | NA | NA | NA | NA | NA |
| [50] | NA | 11 weeks | 2 | 22 | 45 | NA | NA | NA | NA | NA |
| Study | Characteristic | Duration/Frequency | Attendance | Training Intensity | |
|---|---|---|---|---|---|
| [39] | One group performing standard classes | 6 months/thrice a week | 72% | 77 ± 6% | Warm-up; aerobic endurance activities (40%); coordination and flexibility (20%); strength (15%); speed (15%). |
| [34] | One group performing standard classes | 10 weeks/twice a week | NA | NA | 40 min of physical education classes. |
| [40] | One group performing standard classes | 11 weeks/twice a week | NA | NA | 45 min of physical education classes. |
| [41] | NA | NA | NA | NA | NA |
| [42] | Inactive group | NA | NA | NA | Kept their regular physical activity level. |
| [35] | One high-intensity interval training group and one control group | 12 weeks/NA | NA | High-intensity interval training (80.0 ± 3.0% HRmax) Control (68.3 ± 2.2% HRmax) | Warm-up (10 min); 3 sets of high-intensity interval runs (100% maximal aerobic speed) interspaced by 3 min of passive rest; cool down (10 min) The control group performed the regular physical education classes. |
| [36] | One high-intensity interval training group and one control group | 12 weeks/NA | NA | High-intensity interval training (80.0 ± 3.0% HRmax) Control (68.3 ± 2.2% HRmax) | Warm-up (10 min); 3 sets of high-intensity interval runs (100% maximal aerobic speed) interspaced by 3 min of passive rest; cool down (10 min) The control group performed the regular physical education classes. |
| [43] | Control group enrolled in regular physical education classes. | 8 weeks/2 sessions a week | NA | NA | One hour of physical education classes per session. |
| [38] | One group performed circuit strength training and one acted as the control. | 10 months/3 sessions | NA | 0.34 ± 0.09 arbitrary units player load | Circuit strength training consisted of 30 s of all-out exercise with 45 s rest in between. Six to ten stations were used focusing on plyometric and dynamic or static strength (upper and lower body). |
| [44] | Control group enrolled in regular physical education classes. | 11 weeks/2 session | NA | NA | Regular physical education classes of 45 min each. |
| [45] | Control group enrolled in regular physical education classes. | 11 weeks/2 session | NA | NA | Regular physical education classes of 45 min each. |
| [37] | Inactive group | NA | NA | NA | Kept their regular physical activity level. |
| [46] | Control group enrolled in regular physical education classes. | 32 weeks/2 sessions week | NA | NA | Regular physical education classes. |
| [47] | Inactive group | 32 weeks | NA | NA | Kept their regular physical activity level. |
| [48] | Diet-only group and control group | 12 weeks | NA | NA | One group had a nutritional program without exercise and the other acted as a control not receiving the program. |
| [49] | Control (inactive) | NA | NA | NA | Kept their regular physical activity level. |
| [50] | Control group enrolled in regular physical education classes. | 11 weeks/2 sessions week | NA | NA | Regular physical education classes. |
| Study | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 | C11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [39] | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| [34] | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| [40] | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| [41] | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| [42] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| [35] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| [36] | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| [43] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| [38] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| [44] | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| [45] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| [37] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| [46] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| [47] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| [48] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| [49] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| [50] | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Study | Physical Fitness—Evidence of the Main Findings (Differences or Not after Training Programs in Terms of the Main Physical Fitness Outcomes) | General Effects of Soccer Training |
|---|---|---|
| [39] | 6-month soccer training improved maximal power output, balance, flexibility, jump ability, agility, and cardiorespiratory fitness in overweight children. | Favorable |
| [40] | 11-week soccer training improved the ability of a 20-m sprint and cardiorespiratory fitness performance in children. | Favorable |
| [41] | 12-week soccer training increased the VO2peak in obese adolescents. | Favorable |
| [42] | 8-week soccer training increased cardiorespiratory fitness and 20-m sprint performance in untrained adolescents. | Favorable |
| [35] | 12-week soccer training increased explosive power and flexibility of lower extremities in overweight children. | Favorable |
| [36] | 12-week soccer training increased agility and cardiorespiratory fitness in overweight and obese children. | Favorable |
| [43] | 8-week soccer training decreased time in sprint performance (10 and 20 m), and increased jump ability, balance, and cardiorespiratory fitness in adolescents. | Favorable |
| [38] | 10-month soccer training improved cardiorespiratory fitness, although without significant differences in children. | Favorable |
| [45] | 11 weeks of “FIFA 11 for Health” improved balance and cardiorespiratory fitness in both genders. Specifically, when only girls were analyzed, cardiorespiratory fitness and jump ability were improved, while boys only improved cardiorespiratory fitness in children. | Favorable |
| [37] | 10-week soccer training improved cardiorespiratory fitness, VO2peak, 50-m sprinting ability, jump ability, core muscle strength, and balance in children. | Favorable |
| [46] | 8-month soccer training improved resistance in the upper body and cardiorespiratory fitness in adolescents. | Favorable |
| [49] | 8-week soccer training improved abdominal strength and cardiorespiratory fitness in adolescents. | Favorable |
| [50] | An 11-week study of “11 for Health in Denmark” showed positive cardiorespiratory fitness and VO2max levels in children. | Favorable |
| Study | Health-Related Outcomes—Evidence of the Main Findings (Differences or Not after Training Programs in Terms of Health-Related Outcomes) | General Effects of Soccer Training |
|---|---|---|
| [39] | 6-month soccer training did not improve any biochemical or inflammatory marker in overweight children. | No significant effect |
| [34] | 10-week soccer training improved the posterior wall diameter, interventricular septum thickness, and global isovolumetric relaxation in pre-adolescent children. | Favorable |
| [40] | 11-week soccer training decreased systolic blood pressure and mean arterial blood pressure in children. | Favorable |
| [41] | 12-week soccer training decreased systolic blood pressure, total cholesterol, triglycerides, C-reactive protein, insulin resistance, sympathetic activity, and vascular resistance. At the same time, parasympathetic activity, high-density lipoprotein cholesterol, and vascular conductance increased in obese adolescents. | Favorable |
| [42] | 8-week soccer training increased high-frequency power, the root mean squared value of the standard deviation (rMSSD), and decreased sympathetic activity in untrained adolescents. | Favorable |
| [35] | 12-week soccer training led to a positive effect on biochemical parameters, such as the increased number of erythrocytes in overweight children. | Favorable |
| [36] | 12-week soccer training decreased the resting and maximal heart rate in overweight and obese children. | Favorable |
| [38] | 10-month soccer training decreased the diastolic blood pressure and elicited discrete cardiac adaptations, such as interventricular septum thickness, cuspid annular plane systolic excursion, and left-atrial volume index in children. | Favorable |
| [44] | 11 weeks of “FIFA 11 for Health” improved cognitive performance by reducing reaction time in terms of psychomotor function, attention, and working memory in children. | Favorable |
| [45] | 11 weeks of “FIFA 11 for Health” decreased the systolic blood pressure in children. | Favorable |
| [37] | 10-week soccer training improved heart function in children. | Favorable |
| [51] | 10-month soccer training improved interventricular septum thickness and peak transmitral flow velocity in early diastole, while no other changes were observed in children. | |
| [47] | 12-week soccer training was effective in reducing metabolic syndrome in obese adolescents. | Favorable |
| [46] | 8-month soccer training improved the physical aggression subscale (physical aggression, verbal aggression, hostility, and anger) in adolescents. | Favorable |
| [48] | 12-week soccer training with diet restriction decreased the glycated hemoglobin, while no other changes were shown for this group or soccer training without diet restriction, which means that diet was important to improving glycemia in adolescents with type 1 diabetes. | Favorable |
| [49] | 8-week soccer training did not cause any significant changes in blood pressure or heart rate health in adolescents. | No significant effect |
| Study | Body Composition—Evidence of the Main Findings (Differences or Not after Training Programs in Terms of Body Composition) | General Effects of Soccer Training |
|---|---|---|
| [39] | During the 6-month soccer training, height and weight increased in overweight children. | No significant effect |
| [34] | During the 10-week soccer training, body composition variables did not change in children. | No significant effect |
| [40] | During the 11-week soccer training, body mass index and body fat percentage decreased in children. | Favorable |
| [41] | During the 12-week soccer training, body mass index, waist circumference, and percentage of body fat decreased in obese adolescents. | Favorable |
| [42] | During the 8-week soccer training, body composition variables did not change in untrained adolescents. | No significant effect |
| [36] | During the 12-week soccer training, body composition variables did not change in overweight and obese children. | No significant effect |
| [38] | During the 10-month soccer training, body composition variables did not change in any children. | No significant effect |
| [45] | During the 11-week period of “FIFA 11 for Health”, height, weight, body mass index, and lean body mass increased, while body fat decreased in children of both genders. | Favorable |
| [37] | During the 10-week soccer training, body fat, fat mass, and abdominal fat decreased in children. | Favorable |
| [46] | During the 8-month soccer training, body composition variables did not change in adolescents. | No significant effect |
| [47] | The 12 weeks of soccer training were not enough to significantly decrease the fat percentage. | No significant effect |
| [49] | During 8-week soccer training, body composition variables did not change in adolescents. | No significant effect |
| [50] | The 11 weeks of “11 for Health in Denmark” showed a positive effect on body mass index in children. | Favorable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clemente, F.M.; Moran, J.; Ramirez-Campillo, R.; Oliveira, R.; Brito, J.; Silva, A.F.; Badicu, G.; Praça, G.; Sarmento, H. Recreational Soccer Training Effects on Pediatric Populations Physical Fitness and Health: A Systematic Review. Children 2022, 9, 1776. https://doi.org/10.3390/children9111776
Clemente FM, Moran J, Ramirez-Campillo R, Oliveira R, Brito J, Silva AF, Badicu G, Praça G, Sarmento H. Recreational Soccer Training Effects on Pediatric Populations Physical Fitness and Health: A Systematic Review. Children. 2022; 9(11):1776. https://doi.org/10.3390/children9111776
Chicago/Turabian StyleClemente, Filipe Manuel, Jason Moran, Rodrigo Ramirez-Campillo, Rafael Oliveira, João Brito, Ana Filipa Silva, Georgian Badicu, Gibson Praça, and Hugo Sarmento. 2022. "Recreational Soccer Training Effects on Pediatric Populations Physical Fitness and Health: A Systematic Review" Children 9, no. 11: 1776. https://doi.org/10.3390/children9111776