
Systematic Review and Meta-Analysis of the Efficacy and Safety of Metformin and GLP-1 Analogues in Children and Adolescents with Diabetes Mellitus Type 2


 ,
,  and
and 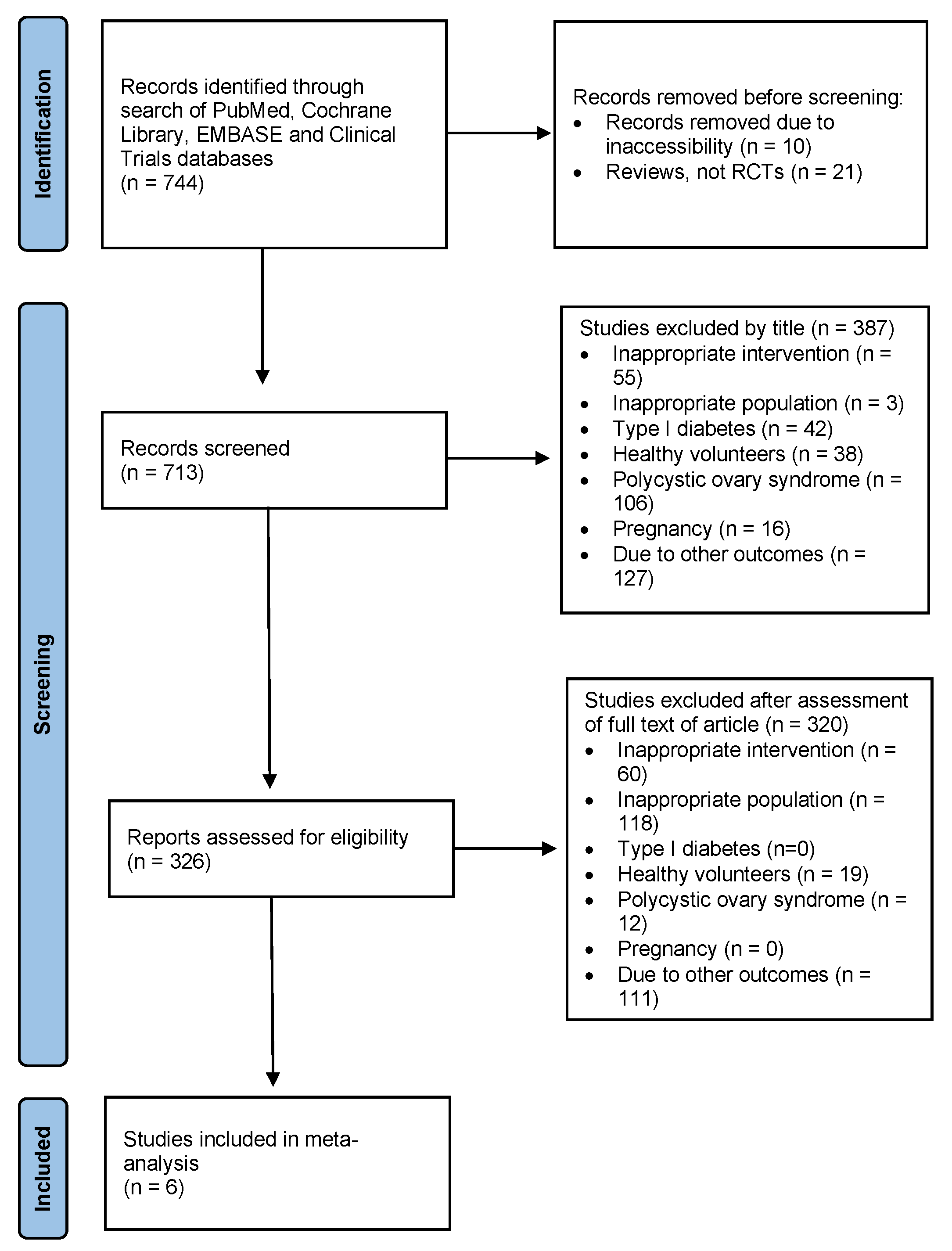{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy, Selection Process, Data Collection Process
2.4. Data Items, Outcome Assessment
2.5. Study Risk of Bias Assessment
2.6. Synthesis Methods
2.7. Certainty Assessment
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Results of Syntheses
3.3.1. Metformin
3.3.2. GLP-1 Analogues
3.4. Reporting Biases
3.5. Assessment of Level of Certainty of Results (GRADE)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of type 2 diabetes—Global burden of disease and forecasted trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Stefanaki, C.; Michos, A.; Mastorakos, G.; Mantzou, A.; Landis, G.; Zosi, P.; Bacopoulou, F. Probiotics in adolescent prediabetes: A pilot RCT on glycemic control and intestinal bacteriome. J. Clin. Med. 2019, 8, 1743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martin, C. Pathophysiology of type 2 diabetes mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef] [PubMed]
- Bacopoulou, F.; Landis, G.N.; Palasz, A.; Tsitsika, A.; Vlachakis, D.; Tsarouhas, K.; Tsitsimpikou, C.; Stefanaki, C.; Kouretas, D.; Efthymiou, V. Identifying early abdominal obesity risk in adolescents by telemedicine: A cross-sectional study in Greece. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2020, 144, 111532. [Google Scholar] [CrossRef] [PubMed]
- Pulungan, A.B.; Afifa, I.T.; Annisa, D. Type 2 diabetes mellitus in children and adolescent: An Indonesian perspective. Ann. Pediatric Endocrinol. Metab. 2018, 23, 119–125. [Google Scholar] [CrossRef]
- Stefanaki, C.; Michos, A.; Latsios, G.; Tousoulis, D.; Peppa, M.; Zosi, P.; Boschiero, D.; Bacopoulou, F. Sexual dimorphism of heart rate variability in adolescence: A case-control study on depression, anxiety, stress levels, body composition, and heart rate variability in adolescents with impaired fasting glucose. Int. J. Environ. Res. Public Health 2020, 17, 2688. [Google Scholar] [CrossRef]
- Stefanaki, C.; Bacopoulou, F.; Peppa, M. Prediabetes and adolescence—Trends, causes, effects, and screening. US Endocrinol. 2016, 12, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Stefanaki, C.; Peppa, M.; Boschiero, D.; Chrousos, G.P. Healthy overweight/obese youth: Early osteosarcopenic obesity features. Eur. J. Clin. Investig. 2016, 46, 767–778. [Google Scholar] [CrossRef]
- Stefanaki, C.; Paltoglou, G.; Mastorakos, G.; Chrousos, G.P. Chronic stress and steatosis of muscles, bones, liver, and pancreas—A review. Horm. Res. Paediatr. 2022. [Google Scholar] [CrossRef]
- Bacopoulou, F.; Foskolos, E.; Stefanaki, C.; Tsitsami, E.; Vousoura, E. Disordered eating attitudes and emotional/behavioral adjustment in Greek adolescents. Eat. Weight. Disord. 2018, 23, 621–628. [Google Scholar] [CrossRef]
- Wu, H.; Patterson, C.C.; Zhang, X.; Ghani, R.B.A.; Magliano, D.J.; Boyko, E.J.; Ogle, G.D.; Luk, A.O.Y. Worldwide estimates of incidence of type 2 diabetes in children and adolescents in 2021. Diabetes Res. Clin. Pract. 2022, 185, 109785. [Google Scholar] [CrossRef] [PubMed]
- Bacha, F. FDA approval of GLP-1 receptor agonist (liraglutide) for use in children. Lancet Child Adolesc. Health 2019, 3, 595–597. [Google Scholar] [CrossRef]
- Soliman, A.; De Sanctis, V.; Alaaraj, N.; Hamed, N. The clinical application of metformin in children and adolescents: A short update. Acta Bio-Med. Atenei Parm. 2020, 91, e2020086. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schunemann, H.J.; Group, G.W. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group, T.S. Effects of metformin, metformin plus rosiglitazone, and metformin plus lifestyle on insulin sensitivity and beta-cell function in TODAY. Diabetes Care 2013, 36, 1749–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuura, N.; Amemiya, S.; Sugihara, S.; Urakami, T.; Kikuchi, N.; Kato, H.; Yodo, Y.; Study Group of the Pediatric Clinical Trial of Metformin in Japan. Metformin monotherapy in children and adolescents with type 2 diabetes mellitus in Japan. Diabetol Int. 2019, 10, 51–57. [Google Scholar] [CrossRef]
- Gottschalk, M.; Danne, T.; Vlajnic, A.; Cara, J.F. Glimepiride versus metformin as monotherapy in pediatric patients with type 2 diabetes: A randomized, single-blind comparative study. Diabetes Care 2007, 30, 790–794. [Google Scholar] [CrossRef] [Green Version]
- Klein, D.J.; Battelino, T.; Chatterjee, D.J.; Jacobsen, L.V.; Hale, P.M.; Arslanian, S.; Group, N.N.S. Liraglutide’s safety, tolerability, pharmacokinetics, and pharmacodynamics in pediatric type 2 diabetes: A randomized, double-blind, placebo-controlled trial. Diabetes Technol. Ther. 2014, 16, 679–687. [Google Scholar] [CrossRef] [Green Version]
- Tamborlane, W.V.; Barrientos-Perez, M.; Fainberg, U.; Frimer-Larsen, H.; Hafez, M.; Hale, P.M.; Jalaludin, M.Y.; Kovarenko, M.; Libman, I.; Lynch, J.L.; et al. Liraglutide in children and adolescents with type 2 diabetes. N. Engl. J. Med. 2019, 381, 637–646. [Google Scholar] [CrossRef]
- U.S. National Library of Medicine. Safety and Efficacy of Exenatide as Monotherapy and Adjunctive Therapy to Oral Antidiabetic Agents in Adolescents with Type 2 Diabetes. Available online: https://clinicaltrials.gov/ct2/show/NCT00658021 (accessed on 30 March 2022).
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence—Study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE guidelines: 8. Rating the quality of evidence—Indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence—Publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef]
- Al-Shareef, M.A.; Sanneh, A.F.; Aljoudi, A.S. Clinical effect of Metformin in children and adolescents with type 2 diabetes mellitus: A systematic review and meta-analysis. J. Fam. Community Med. 2012, 19, 68–73. [Google Scholar] [CrossRef]
- Jones, K.L.; Arslanian, S.; Peterokova, V.A.; Park, J.S.; Tomlinson, M.J. Effect of metformin in pediatric patients with type 2 diabetes: A randomized controlled trial. Diabetes Care 2002, 25, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Kuzik, N.; Myette-Cote, E.; Carson, V.; Slater, L.; Boule, N.G. Evaluating the effects of metformin use on height in children and adolescents: A meta-analysis of randomized clinical trials. JAMA Pediatr. 2015, 169, 1032–1039. [Google Scholar] [CrossRef] [Green Version]
- Chadda, K.R.; Cheng, T.S.; Ong, K.K. GLP-1 agonists for obesity and type 2 diabetes in children: Systematic review and meta-analysis. Obes. Rev. 2021, 22, e13177. [Google Scholar] [CrossRef]
- Vilsboll, T.; Christensen, M.; Junker, A.E.; Knop, F.K.; Gluud, L.L. Effects of glucagon-like peptide-1 receptor agonists on weight loss: Systematic review and meta-analyses of randomised controlled trials. BMJ 2012, 344, d7771. [Google Scholar] [CrossRef]
- Sun, F.; Chai, S.; Yu, K.; Quan, X.; Yang, Z.; Wu, S.; Zhang, Y.; Ji, L.; Wang, J.; Shi, L. Gastrointestinal adverse events of glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes: A systematic review and network meta-analysis. Diabetes Technol. Ther. 2015, 17, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippatos, T.D.; Panagiotopoulou, T.V.; Elisaf, M.S. Adverse Effects of GLP-1 Receptor Agonists. Rev. Diabet. Stud. 2014, 11, 202–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monami, M.; Marchionni, N.; Mannucci, E. Glucagon-like peptide-1 receptor agonists in type 2 diabetes: A meta-analysis of randomized clinical trials. Eur. J. Endocrinol. 2009, 160, 909–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temneanu, O.R.; Trandafir, L.M.; Purcarea, M.R. Type 2 diabetes mellitus in children and adolescents: A relatively new clinical problem within pediatric practice. J. Med. Life 2016, 9, 235–239. [Google Scholar] [PubMed]
- Tronieri, J.S.; Wadden, T.A.; Walsh, O.; Berkowitz, R.I.; Alamuddin, N.; Chao, A.M. Measures of adherence as predictors of early and total weight loss with intensive behavioral therapy for obesity combined with liraglutide 3.0mg. Behav. Res. Ther. 2020, 131, 103639. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carydias, E.; Tasho, A.; Kani, C.; Bacopoulou, F.; Stefanaki, C.; Markantonis, S.L. Systematic Review and Meta-Analysis of the Efficacy and Safety of Metformin and GLP-1 Analogues in Children and Adolescents with Diabetes Mellitus Type 2. Children 2022, 9, 1572. https://doi.org/10.3390/children9101572
Carydias E, Tasho A, Kani C, Bacopoulou F, Stefanaki C, Markantonis SL. Systematic Review and Meta-Analysis of the Efficacy and Safety of Metformin and GLP-1 Analogues in Children and Adolescents with Diabetes Mellitus Type 2. Children. 2022; 9(10):1572. https://doi.org/10.3390/children9101572
Chicago/Turabian StyleCarydias, Elisabeth, Andoneta Tasho, Chara Kani, Flora Bacopoulou, Charikleia Stefanaki, and Sophia L. Markantonis. 2022. "Systematic Review and Meta-Analysis of the Efficacy and Safety of Metformin and GLP-1 Analogues in Children and Adolescents with Diabetes Mellitus Type 2" Children 9, no. 10: 1572. https://doi.org/10.3390/children9101572