
Risk Factors, Clinical Consequences, Prevention, and Treatment of Childhood Obesity

 , ,
, ,
Abstract
:1. Introduction
2. Risk Factors
2.1. Nutrition and Diet
2.2. Socioeconomic Factors
2.3. Comorbidities and Healthcare System-Related Factors
2.4. Maternal-Related Factors
2.5. Physical Activity
2.6. Sleep Duration and Quality
3. Clinical Consequences
3.1. Cardiovascular Disease
3.2. Respiratory Disease
3.3. Endocrine Disease
3.4. Mental Health and Psychosocial
3.5. Gastrointestinal and Hepatic Diseases
3.6. Infectious Diseases
3.7. Overall Increase in the Demand for Healthcare Services
3.8. Overall Increase in the Healthcare Costs
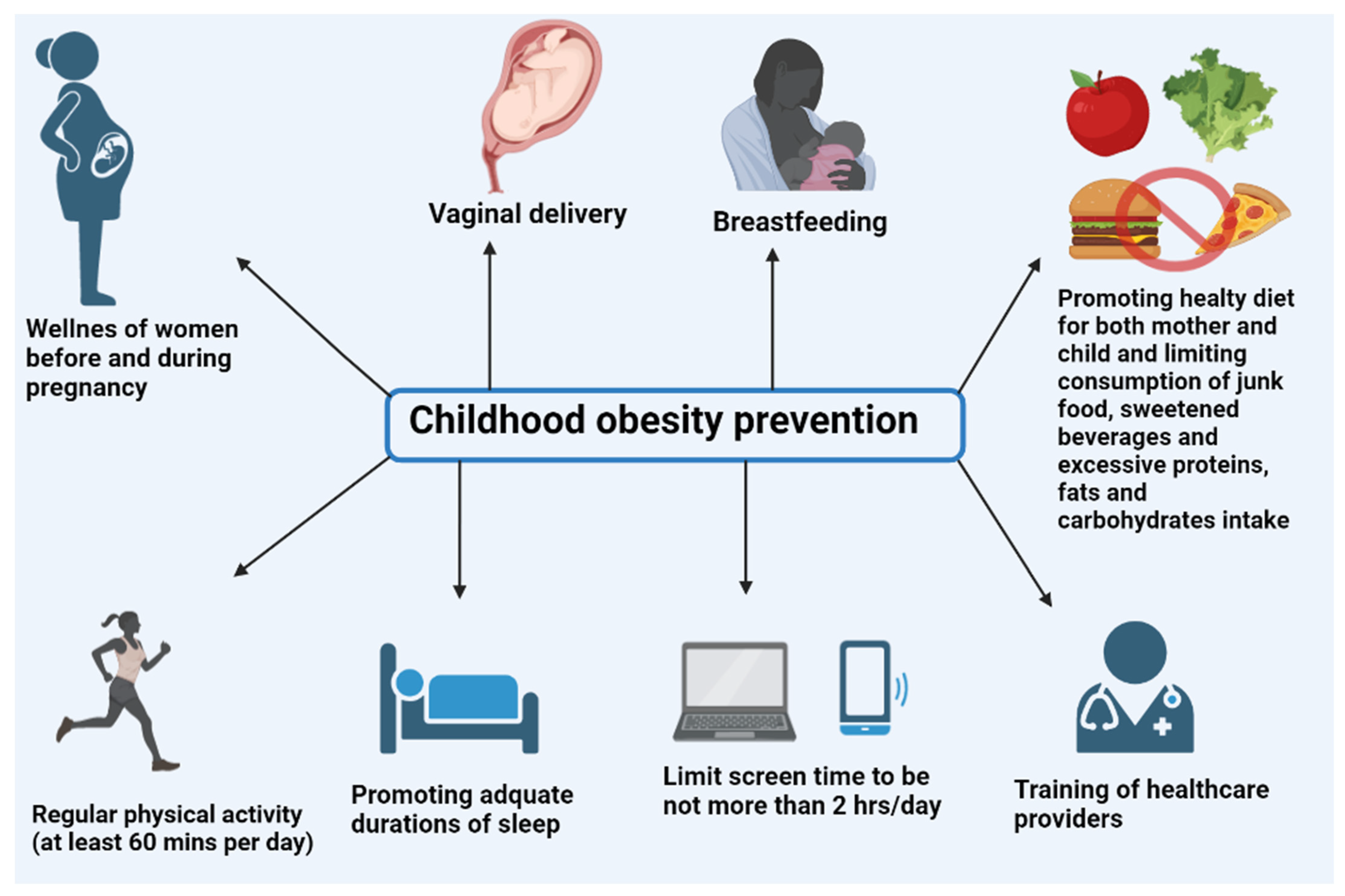
4. Prevention
4.1. Obesogenic Environment-Oriented Approaches
4.1.1. Healthy Diet
4.1.2. Physical Activity
4.1.3. Screen Time
4.1.4. Sleeping Duration and Quality
4.2. Maternal Health before and during Pregnancy
4.2.1. Vaginal Delivery
4.2.2. Breastfeeding
4.3. Strategies for Combating Weight Stigma and Enhancing Obesity Care
Training of Healthcare Providers
5. Treatment
5.1. FDA-Approved Medications
5.1.1. Orlistat
5.1.2. Liraglutide
5.1.3. Phentermine and Topiramate Combination
5.1.4. Setmelanotide (FDA-Approved for Syndromic Obesity)
5.2. Off-Label Medications
5.2.1. Metformin
5.2.2. Lisdexamfetamine
5.2.3. Zonisamide
5.2.4. Naltrexone S.R. with Bupropion S.R.
5.2.5. Fluoxetine
5.2.6. Metabolic and Bariatric Surgery
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Syed, N.K.; Syed, M.H.; Meraya, A.M.; Albarraq, A.A.; Al-Kasim, M.A.; Alqahtani, S.; Makeen, H.A.; Yasmeen, A.; Banji, O.J.F.; Elnaem, M.H. The association of dietary behaviors and practices with overweight and obesity parameters among Saudi university students. PLoS ONE 2020, 15, e0238458. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P. Sleep patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 86–91. [Google Scholar] [CrossRef]
- Albuquerque, D.; Nóbrega, C.; Manco, L.; Padez, C. The contribution of genetics and environment to obesity. Br. Med. Bull. 2017, 123, 159–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef] [PubMed]
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Riley, L.M.; Taddei, C.; Hajifathalian, K.; Lu, Y.; et al. Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128.9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.P.; Bentham, J. The epidemiological burden of obesity in childhood: A worldwide epidemic requiring urgent action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.T.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Steinbeck, K. Childhood Obesity: Consequences and Complications. Clin. Obes. Adults Child. 2010, 392–407. [Google Scholar] [CrossRef]
- Lakshman, R.; Elks, C.E.; Ong, K.K. Childhood Obesity. Circulation 2012, 126, 1770–1779. [Google Scholar] [CrossRef]
- Alam Mahumud, R.; Sahle, B.W.; Owusu-Addo, E.; Chen, W.; Morton, R.L.; Renzaho, A.M.N. Association of dietary intake, physical activity, and sedentary behaviours with overweight and obesity among 282,213 adolescents in 89 low and middle income to high-income countries. Int. J. Obes. 2021, 45, 2404–2418. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.; Zulaily, N.; Shahril, M.R.; Wafa, S.W.; Amin, R.M.; Piernas, C.; Ahmed, A. Obesity determinants among Malaysian 12-year old school adolescents: Findings from the HAT study. BMC Pediatr. 2021, 21, 418. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Katzmarzyk, P.; Boyce, W.F.; King, M.A.; Pickett, W. Overweight and obesity in Canadian adolescents and their associations with dietary habits and physical activity patterns. J. Adolesc. Health 2004, 35, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, L.; Haghighatdoost, F.; Feizi, A.; Esmaillzadeh, A. Breakfast eating pattern and its association with dietary quality indices and anthropometric measurements in young women in Isfahan. Nutrition 2013, 29, 420–425. [Google Scholar] [CrossRef]
- Verduci, E.; Di Profio, E.; Fiore, G.; Zuccotti, G. Integrated Approaches to Combatting Childhood Obesity. Ann. Nutr. Metab. 2022, 78, 8–19. [Google Scholar] [CrossRef]
- Edwin Thanarajah, S.; Tittgemeyer, M. Food reward and gut-brain signalling. Neuroforum 2020, 26, 1–9. [Google Scholar] [CrossRef]
- Ledikwe, J.H.; Ello-Martin, J.A.; Rolls, B.J. Portion Sizes and the Obesity Epidemic. J. Nutr. 2005, 135, 905–909. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.-T.; Ju, Y.-S.; Park, K.-H.; Kwon, Y.-J.; Im, H.-J.; Paek, D.-M.; Lee, H.-J. Study on the relationship between childhood obesity and various determinants, including socioeconomic factors, in an urban area. J. Prev. Med. Public Health 2006, 39, 371–378. [Google Scholar]
- Gardner, R.; Feely, A.; Layte, R.; Williams, J.; McGavock, J. Adverse childhood experiences are associated with an increased risk of obesity in early adolescence: A population-based prospective cohort study. Pediatr. Res. 2019, 86, 522–528. [Google Scholar] [CrossRef]
- Parekh, N.; Deierlein, A.L. Health behaviours during the coronavirus disease 2019 pandemic: Implications for obesity. Public Health Nutr. 2020, 23, 3121–3125. [Google Scholar] [CrossRef]
- Hill, A.P.; Zuckerman, K.E.; Fombonne, E. Obesity and Autism. Pediatrics 2015, 136, 1051–1061. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Neumark-Sztainer, D.; Austin, S.B.; Luedicke, J.; King, K.M. Setting policy priorities to address eating disorders and weight stigma: Views from the field of eating disorders and the US general public. BMC Public Health 2014, 14, 524. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Liu, S. A national survey of public views about the classification of obesity as a disease. Obesity 2015, 23, 1288–1295. [Google Scholar] [CrossRef] [PubMed]
- Baidal, J.A.W.; Locks, L.M.; Cheng, E.R.; Blake-Lamb, T.L.; Perkins, M.E.; Taveras, E.M. Risk Factors for Childhood Obesity in the First 1000 Days: A Systematic Review. Am. J. Prev. Med. 2016, 50, 761–779. [Google Scholar] [CrossRef]
- Druet, C.; Ong, K.K. Early childhood predictors of adult body composition. Best Pr. Res. Clin. Endocrinol. Metab. 2008, 22, 489–502. [Google Scholar] [CrossRef]
- Dantas, R.R.; da Silva, G.A.P. The role of the obesogenic environment and parental lifestyles in infant feeding behavior. Rev. Paul. Pediatr. 2019, 37, 363. [Google Scholar] [CrossRef]
- Ritchie, S.; Connell, J. The link between abdominal obesity, metabolic syndrome and cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 319–326. [Google Scholar] [CrossRef]
- Yang, Z.; Li, Y.; Dong, B.; Gao, D.; Wen, B.; Ma, J. Relationship between parental overweight and obesity and childhood metabolic syndrome in their offspring: Result from a cross-sectional analysis of parent–offspring trios in China. BMJ Open 2020, 10, e036332. [Google Scholar] [CrossRef]
- Zhou, J.; Zeng, L.; Wang, D.; Li, C.; Liu, Y.; Yan, H.; Xiao, Y. Effects of birth weight on body composition and overweight/obesity at early school age. Clin. Nutr. 2019, 39, 1778–1784. [Google Scholar] [CrossRef]
- Adair, L.S. Child and adolescent obesity: Epidemiology and developmental perspectives. Physiol. Behav. 2008, 94, 8–16. [Google Scholar] [CrossRef]
- Mittal, M.; Jain, V. Management of Obesity and Its Complications in Children and Adolescents. Indian J. Pediatr. 2021, 88, 1222–1234. [Google Scholar] [CrossRef] [PubMed]
- Mathialagan, A.; Nallasamy, N.; Razali, S.N. Physical activity and media environment as antecedents of childhood obesity in malaysia. Asian J. Pharm. Clin. Res. 2018, 11, 287–292. [Google Scholar] [CrossRef]
- Han, S.-H.; Yee, J.-Y.; Pyo, J.-S. Impact of Short Sleep Duration on the Incidence of Obesity and Overweight among Children and Adolescents. Medicina 2022, 58, 1037. [Google Scholar] [CrossRef] [PubMed]
- Noorwali, E.; Potter, G.; Ford, H.; Mulla, U.; Murphy, D.; Wark, P.; Frost, G.; Hardie, L.; Cade, J. Sleep timing and vegetable intakes in UK adults: A cross-sectional study. Proc. Nutr. Soc. 2018, 77, E132. [Google Scholar] [CrossRef]
- Sidik, S.M.; Ahmad, R. Childhood obesity: Contributing factors, consequences and intervention. Malays. J. Nutr. 2004, 10, 13–22. [Google Scholar] [PubMed]
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-Related Consequences of Childhood Obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef]
- Sorof, J.; Daniels, S. Obesity Hypertension in Children: A problem of epidemic proportions. Hypertension 2002, 40, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Tauman, R.; Gozal, D. Obesity and obstructive sleep apnea in children. Paediatr. Respir. Rev. 2006, 7, 247–259. [Google Scholar] [CrossRef]
- Sideleva, O.; Black, K.; Dixon, A.E. Effects of obesity and weight loss on airway physiology and inflammation in asthma. Pulm. Pharmacol. Ther. 2013, 26, 455–458. [Google Scholar] [CrossRef] [Green Version]
- Gilliland, F.D.; Berhane, K.; Islam, T.; McConnell, R.; Gauderman, W.J.; Gilliland, S.S.; Avol, E.; Peters, J.M.; Gilliland, F.D.; Berhane, K.; et al. Obesity and the Risk of Newly Diagnosed Asthma in School-age Children. Am. J. Epidemiol. 2003, 158, 406–415. [Google Scholar] [CrossRef] [Green Version]
- Babakr, A.T.; Elsheikh, O.; Almarzoqi, A.; Assiri, A.; Abdalla, B.E.; Zaki, H.; Fatani, S.; Eldin, E.E.N. Relationship between oxidized low-density lipoprotein antibodies and obesity in different glycemic situations. Diabetes Metab. Syndr. Obes. 2014, 7, 513–520. [Google Scholar] [CrossRef]
- Bradley, S.H.; Lawrence, N.; Steele, C.; Mohamed, Z. Precocious puberty. BMJ 2020, 368, l6597. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Guo, J.; Zhang, X.; Lu, Y.; Miao, J.; Xue, H. Obesity is a risk factor for central precocious puberty: A case-control study. BMC Pediatr. 2021, 21, 509. [Google Scholar] [CrossRef]
- Uçar, A.; Saka, N.; Baş, F.; Hatipoğlu, N.; Bundak, R.; Darendeliler, F. Reduced atherogenic indices in prepubertal girls with precocious adrenarche born appropriate for gestational age in relation to the conundrum of DHEAS. Endocr. Connect. 2013, 2, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, A.D.; Solorzano, C.M.B.; McCartney, C.R. Childhood Obesity and Its Impact on the Development of Adolescent PCOS. Semin. Reprod. Med. 2014, 32, 202–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinlen, D.; Cody, D.; O’Shea, D. Complications of obesity. Qjm Int. J. Med. 2017, 111, 437–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindberg, L.; Hagman, E.; Danielsson, P.; Marcus, C.; Persson, M. Anxiety and depression in children and adolescents with obesity: A nationwide study in Sweden. BMC Med. 2020, 18, 30. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.J.; Feldman, I.; Schiöth, H.B.; Titova, O.E. Important gender differences in psychosomatic and school-related complaints in relation to adolescent weight status. Sci. Rep. 2021, 11, 14147. [Google Scholar] [CrossRef]
- Lerret, S.M.; Garcia-Rodriguez, L.; Skelton, J.; Biank, V.; Kilway, D.; Telega, G. Predictors of Nonalcoholic Steatohepatitis in Obese Children. Gastroenterol. Nurs. 2011, 34, 434–437. [Google Scholar] [CrossRef] [Green Version]
- Peng, L.; Wu, S.; Zhou, N.; Zhu, S.; Liu, Q.; Li, X. Clinical characteristics and risk factors of nonalcoholic fatty liver disease in children with obesity. BMC Pediatr. 2021, 21, 122. [Google Scholar] [CrossRef]
- Koebnick, C.; Getahun, D.; Smith, N.; Porter, A.; Der-Sarkissian, J.K.; Jacobsen, S. Extreme childhood obesity is associated with increased risk for gastroesophageal reflux disease in a large population-based study. Int. J. Pediatr. Obes. 2011, 6, e257–e263. [Google Scholar] [CrossRef] [PubMed]
- Fradin, K.; Racine, A.D.; Belamarich, P.F. Obesity and Symptomatic Cholelithiasis in Childhood: Epidemiologic and case-control evidence for a strong relation. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Nasif, W.A.; Mukhtar, M.H.; Ali, A.S.E.-M.; Eldein, M.M.N.; Almaimani, R.A.; Ashgar, S.S. Body mass index is associated with Helicobacter pylori infection and increased oxidative DNA damage in an obese population. J. Int. Med. Res. 2022, 50, 3000605221076975. [Google Scholar] [CrossRef] [PubMed]
- Dobner, J.; Kaser, S. Body mass index and the risk of infection—From underweight to obesity. Clin. Microbiol. Infect. 2017, 24, 24–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, C.J.; Murphy, K.E.; Fernandez, M.L. Impact of Obesity and Metabolic Syndrome on Immunity. Adv. Nutr. Int. Rev. J. 2016, 7, 66–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Pinto, M.A.; Ortiz-Marrón, H.; Esteban-Vasallo, M.D.; Quadrado-Mercadal, A.; Casanova-Pardomo, D.; González-Alcón, M.; Ordobás-Gavin, M.; Galán, I. Demand for health services and drug prescriptions among overweight or obese preschool children. Arch. Dis. Child. 2019, 105, 292–297. [Google Scholar] [CrossRef]
- Nielsen, J.D.J.; Laverty, A.A.; Millett, C.; Iii, A.G.M.; Majeed, A.; Saxena, S. Rising Obesity-Related Hospital Admissions among Children and Young People in England: National Time Trends Study. PLoS ONE 2013, 8, e65764. [Google Scholar] [CrossRef] [Green Version]
- Shanley, L.A.; Lin, H.; Flores, G. Factors associated with length of stay for pediatric asthma hospitalizations. J. Asthma 2014, 52, 471–477. [Google Scholar] [CrossRef]
- Carroll, C.L.; Stoltz, P.; Raykov, N.; Smith, S.R.; Zucker, A.R. Childhood Overweight Increases Hospital Admission Rates for Asthma. Pediatrics 2007, 120, 734–740. [Google Scholar] [CrossRef]
- Hamilton, D.; Dee, A.; Perry, I.J. The lifetime costs of overweight and obesity in childhood and adolescence: A systematic review. Obes. Rev. 2018, 19, 452–463. [Google Scholar] [CrossRef]
- Biener, A.; Cawley, J.; Meyerhoefer, C. The Impact of Obesity on Medical Care Costs and Labor Market Outcomes in the US. Clin. Chem. 2018, 64, 108–117. [Google Scholar] [CrossRef] [PubMed]
- d’Errico, M.; Pavlova, M.; Spandonaro, F. The economic burden of obesity in Italy: A cost-of-illness study. Eur. J. Health Econ. 2022, 23, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Azzeh, F.S.; Bukhari, H.M.; Header, E.A.; Ghabashi, M.A.; Al-Mashi, S.S.; Noorwali, N.M. Trends in overweight or obesity and other anthropometric indices in adults aged 18–60 years in western Saudi Arabia. Ann. Saudi Med. 2017, 37, 106–113. [Google Scholar] [CrossRef] [Green Version]
- MyPlate Food Guide (for Parents)—Nemours KidsHealth. Available online: https://kidshealth.org/en/parents/myplate.html (accessed on 3 December 2022).
- Nader, P.R.; Bradley, R.H.; Houts, R.; McRitchie, S.L.; O’Brien, M. Moderate-to-Vigorous Physical Activity From Ages 9 to 15 Years. JAMA 2008, 300, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Laurson, K.R.; Lee, J.A.; Gentile, D.A.; Walsh, D.A.; Eisenmann, J.C. Concurrent Associations between Physical Activity, Screen Time, and Sleep Duration with Childhood Obesity. ISRN Obes. 2014, 2014, 204540. [Google Scholar] [CrossRef] [PubMed]
- Falbe, J.; Rosner, B.; Willett, W.C.; Sonneville, K.R.; Hu, F.B.; Field, A.E. Adiposity and Different Types of Screen Time. Pediatrics 2013, 132, e1497–e1505. [Google Scholar] [CrossRef] [Green Version]
- Alwafi, H.; Alwafi, R.; Naser, A.Y.; Samannodi, M.; Aboraya, D.; Salawati, E.; Alqurashi, A.; Ekram, R.; Alzahrani, A.R.; Aldhahir, A.M.; et al. The Impact of Social Media Influencers on Food Consumption in Saudi Arabia, a Cross-Sectional Web-Based Survey. J. Multidiscip. Health 2022, 15, 2129–2139. [Google Scholar] [CrossRef]
- Golley, R.K.; Maher, C.; Matricciani, L.; Olds, T. Sleep duration or bedtime? Exploring the association between sleep timing behaviour, diet and BMI in children and adolescents. Int. J. Obes. 2013, 37, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Noorwali, E.; Hardie, L.; Cade, J. Bridging the Reciprocal Gap between Sleep and Fruit and Vegetable Consumption: A Review of the Evidence, Potential Mechanisms, Implications, and Directions for Future Work. Nutrients 2019, 11, 1382. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, J.M.; Murphy, K.; Stanton, C.; Ross, R.P.; Kober, O.I.; Juge, N.; Avershina, E.; Rudi, K.; Narbad, A.; Jenmalm, M.C.; et al. The composition of the gut microbiota throughout life, with an emphasis on early life. Microbes Ecol. Health Dis. 2015, 26, 26050. [Google Scholar] [CrossRef]
- Munyaka, P.M.; Khafipour, E.; Ghia, J.-E. External Influence of Early Childhood Establishment of Gut Microbiota and Subsequent Health Implications. Front. Pediatr. 2014, 2, 109. [Google Scholar] [CrossRef] [PubMed]
- Quecke, B.; Graf, Y.; Epure, A.; Santschi, V.; Chiolero, A.; Carmeli, C.; Cullati, S. Caesarean section and obesity in young adult offspring: Update of a systematic review with meta-analysis. Obes. Rev. 2021, 23, e13368. [Google Scholar] [CrossRef] [PubMed]
- Martin, F.-P.J.; Moco, S.; Montoliu, I.; Collino, S.; Da Silva, L.; Rezzi, S.; Prieto, R.; Kussmann, M.; Inostroza, J.; Steenhout, P. Impact of breast-feeding and high- and low-protein formula on the metabolism and growth of infants from overweight and obese mothers. Pediatr. Res. 2013, 75, 535–543. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; Liu, L.; Zhu, Y.; Huang, G.; Wang, P.P. The association between breastfeeding and childhood obesity: A meta-analysis. BMC Public Health 2014, 14, 1267. [Google Scholar] [CrossRef] [Green Version]
- Mischke, M.; Plösch, T. More than just a gut instinct-the potential interplay between a baby’s nutrition, its gut microbiome, and the epigenome. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 304, 1065–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray, D.; Sniehotta, F.; McColl, E.; Ells, L. Barriers and facilitators to implementing practices for prevention of childhood obesity in primary care: A mixed methods systematic review. Obes. Rev. 2022, 23, e13417. [Google Scholar] [CrossRef] [PubMed]
- Mattiazzi, E.; Bolgeo, T.; Prosperi, A.; Dagna, C.; Polverelli, M.; Di Matteo, R.; Maconi, A. The role of the physiotherapist in pediatric obesity prevention: Comparing experiences. Work. Pap. Public Health 2022, 10. [Google Scholar] [CrossRef]
- Bagnes, M.F.G.; González, C.; Hirschler, V.; Di Girolamo, G. Pharmacotherapeutic options in pediatric obesity: An urgent call for further research. Expert Opin. Pharmacother. 2022, 23, 869–872. [Google Scholar] [CrossRef]
- New AAP Guidelines for Pediatric Obesity a “Sea Change”. Available online: https://www.medscape.com/viewarticle/983837 (accessed on 3 December 2022).
- Xia, Y.; Kelton, C.M.; Guo, J.J.; Bian, B.; Heaton, P.C. Treatment of obesity: Pharmacotherapy trends in the United States from 1999 to 2010. Obesity 2015, 23, 1721–1728. [Google Scholar] [CrossRef] [Green Version]
- Boland, C.L.; Harris, J.B.; Harris, K.B. Pharmacological Management of Obesity in Pediatric Patients. Ann. Pharmacother. 2014, 49, 220–232. [Google Scholar] [CrossRef]
- Chanoine, J.; Hampl, S.; Jensen, C.; Boldrin, M.; Hauptman, J. Effect of Orlistat on Weight and Body Composition in Obese Adolescents. A Randomized Controlled Trial. JAMA 2005, 293, 2873–2891. [Google Scholar] [CrossRef] [PubMed]
- McGovern, L.; Johnson, J.N.; Paulo, R.; Hettinger, A.; Singhal, V.; Kamath, C.; Erwin, P.J.; Montori, V. Treatment of Pediatric Obesity: A Systematic Review and Meta-Analysis of Randomized Trials. J. Clin. Endocrinol. Metab. 2008, 93, 4600–4605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDuffie, J.R.; Calis, K.A.; Booth, S.L.; Uwaifo, G.I.; Yanovski, J.A. Effects of Orlistat on Fat-Soluble Vitamins in Obese Adolescents. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2002, 22, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Alruwaili, H.; Dehestani, B.; le Roux, C.W. Clinical Impact of Liraglutide as a Treatment of Obesity. Clin. Pharmacol. 2021, 13, 53–60. [Google Scholar] [CrossRef]
- Kelly, A.S.; Auerbach, P.; Barrientos-Perez, M.; Gies, I.; Hale, P.M.; Marcus, C.; Mastrandrea, L.D.; Prabhu, N.; Arslanian, S. A Randomized, Controlled Trial of Liraglutide for Adolescents with Obesity. N. Engl. J. Med. 2020, 382, 2117–2128. [Google Scholar] [CrossRef]
- Bensignor, M.O.; Bomberg, E.M.; Bramante, C.T.; Divyalasya, T.V.S.; Hale, P.M.; Ramesh, C.K.; Rudser, K.D.; Kelly, A.S. Effect of liraglutide treatment on body mass index and weight parameters in children and adolescents with type 2 diabetes: Post hoc analysis of the ellipse trial. Pediatr. Obes. 2021, 16, e12778. [Google Scholar] [CrossRef]
- Dhillon, S. Phentermine/Topiramate: Pediatric First Approval. Pediatr. Drugs 2022, 24, 715–720. [Google Scholar] [CrossRef]
- Hsia, D.S.; Gosselin, N.H.; Williams, J.; Farhat, N.; Marier, J.F.; Shih, W.; Peterson, C.; Siegel, R. A randomized, double-blind, placebo-controlled, pharmacokinetic and pharmacodynamic study of a fixed-dose combination of phentermine/topiramate in adolescents with obesity. Diabetes Obes. Metab. 2019, 22, 480–491. [Google Scholar] [CrossRef]
- Forsythe, E.; Beales, P.L. Bardet–Biedl syndrome. Eur. J. Hum. Genet. 2012, 21, 8–13. [Google Scholar] [CrossRef]
- Clément, K.; Akker, E.V.D.; Argente, J.; Bahm, A.; Chung, W.K.; Connors, H.; De Waele, K.; Farooqi, I.S.; Gonneau-Lejeune, J.; Gordon, G.; et al. Efficacy and safety of setmelanotide, an MC4R agonist, in individuals with severe obesity due to LEPR or POMC deficiency: Single-arm, open-label, multicentre, phase 3 trials. Lancet Diabetes Endocrinol. 2020, 8, 960–970. [Google Scholar] [CrossRef]
- Haws, R.; Brady, S.; Davis, E.; Fletty, K.; Yuan, G.; Gordon, G.; Stewart, M.; Yanovski, J. Effect of setmelanotide, a melanocortin-4 receptor agonist, on obesity inBardet-Biedlsyndrome. Diabetes Obes. Metab. 2020, 22, 2133–2140. [Google Scholar] [CrossRef] [PubMed]
- Apperley, L.J.; Blackburn, J.; Erlandson-Parry, K.; Gait, L.; Laing, P.; Senniappan, S. Childhood obesity: A review of current and future management options. Clin. Endocrinol. 2021, 96, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Temneanu, O.; Trandafir, L.; Purcarea, M.R. Type 2 diabetes mellitus in children and adolescents: A relatively new clinical problem within pediatric practice. J. Med. Life 2016, 9, 235–239. [Google Scholar] [PubMed]
- Brufani, C.; Crinò, A.; Fintini, D.; Patera, P.I.; Cappa, M.; Manco, M. Systematic Review of Metformin Use in Obese Nondiabetic Children and Adolescents. Horm. Res. Paediatr. 2013, 80, 78–85. [Google Scholar] [CrossRef]
- Ejtahed, H.-S.; Tito, R.Y.; Siadat, S.D.; Hasani-Ranjbar, S.; Hoseini-Tavassol, Z.; Rymenans, L.; Verbeke, K.; Soroush, A.-R.; Raes, J.; Larijani, B. Metformin induces weight loss associated with gut microbiota alteration in non-diabetic obese women: A randomized double-blind clinical trial. Eur. J. Endocrinol. 2019, 180, 165–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wigal, S.B.; Raja, P.; Shukla, A. An update on lisdexamfetamine dimesylate for the treatment of attention deficit hyperactivity disorder. Expert Opin. Pharmacother. 2012, 14, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Guerdjikova, A.I.; Blom, T.J.; Mori, N.; Matthews, A.; Cummings, T.; Casuto, L.L.; McElroy, S.L. Lisdexamfetamine in Pediatric Binge Eating Disorder: A Retrospective Chart Review. Clin. Neuropharmacol. 2019, 42, 214–216. [Google Scholar] [CrossRef]
- French, J.A.; Kanner, A.M.; Bautista, J.; Abou-Khalil, B.; Browne, T.; Harden, C.L.; Theodore, W.H.; Bazil, C.; Stern, J.; Schachter, S.C.; et al. Efficacy and tolerability of the new antiepileptic drugs II: Treatment of refractory epilepsy [RETIRED]. Neurology 2004, 62, 1261–1273. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M.L.; Pirzada, M.H.; Shapiro, M.A. Case Report Zonisamide for Weight Loss in Adolescents. 2013. Available online: http://meridian.allenpress.com/jppt/article-pdf/18/4/311/1784142/1551-6776-18_4_311.pdf (accessed on 9 October 2022).
- Lagae, L.; Meshram, C.; Giorgi, L.; Patten, A. Effects of adjunctive zonisamide treatment on weight and body mass index in children with partial epilepsy. Acta Neurol. Scand. 2015, 131, 341–346. [Google Scholar] [CrossRef]
- Lobmaier, P.P.; Kunøe, N.; Gossop, M.; Waal, H. Naltrexone Depot Formulations for Opioid and Alcohol Dependence: A Systematic Review. CNS Neurosci. Ther. 2010, 17, 629–636. [Google Scholar] [CrossRef]
- Stahl, S.M.; Pradko, J.F.; Haight, B.R.; Modell, J.G.; Rockett, C.B. A Review of the Neuropharmacology of Bupropion, a Dual Norepinephrine and Dopamine Reuptake Inhibitor. Prim. Care Companion J. Clin. Psychiatry 2004, 6, 159–166. [Google Scholar] [CrossRef] [PubMed]
- McElroy, S.L.; Guerdjikova, A.I.; Kim, D.D.; Burns, C.; Harris-Collazo, R.; Landbloom, R.; Dunayevich, E. Naltrexone/Bupropion Combination Therapy in Overweight or Obese Patients With Major Depressive Disorder: Results of a pilot study. Prim. Care Companion CNS Disord. 2013, 15, PCC.12m01494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billes, S.K.; Sinnayah, P.; Cowley, M.A. Naltrexone/bupropion for obesity: An investigational combination pharmacotherapy for weight loss. Pharmacol. Res. 2014, 84, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dörks, M.; Langner, I.; Dittmann, U.; Timmer, A.; Garbe, E. Antidepressant drug use and off-label prescribing in children and adolescents in Germany: Results from a large population-based cohort study. Eur. Child Adolesc. Psychiatry 2013, 22, 511–518. [Google Scholar] [CrossRef]
- Faith, M.S.; Butryn, M.; Wadden, T.A.; Fabricatore, A.; Nguyen, A.M.; Heymsfield, S.B. Evidence for prospective associations among depression and obesity in population-based studies. Obes. Rev. 2011, 12, e438–e453. [Google Scholar] [CrossRef]
- Serralde-Zuñiga, A.E.; González-Garay, A.G.; Rodríguez-Carmona, Y.; Meléndez-Mier, G. Use of Fluoxetine to Reduce Weight in Adults with Overweight or Obesity: Abridged Republication of the Cochrane Systematic Review. Obes. Facts 2022, 15, 473–486. [Google Scholar] [CrossRef]
- Polfuss, M.L.; Duderstadt, K.G.; Kilanowski, J.F.; Thompson, M.E.; Davis, R.L.; Quinn, M. Childhood Obesity: Evidence-Based Guidelines for Clinical Practice—Part One. J. Pediatr. Health Care 2020, 34, 283–290. [Google Scholar] [CrossRef]
- Halloun, R.; Weiss, R. Bariatric Surgery in Adolescents with Obesity: Long-Term Perspectives and Potential Alternatives. Horm. Res. Paediatr. 2021, 95, 193–203. [Google Scholar] [CrossRef]
- Goldenshluger, A.; Maor, T.; Via-Kagan, R.; Zelekha, O.; Gepner, Y. Short-Term Changes in Mental, Physical, and Social Factors After Metabolic Bariatric Surgery in Adolescents: A Nationwide Prospective Cohort Study. Front. Nutr. 2022, 9, 878202. [Google Scholar] [CrossRef]
- Paulus, G.F.; de Vaan, L.E.G.; Verdam, F.J.; Bouvy, N.D.; Ambergen, T.A.W.; van Heurn, L.W.E. Bariatric Surgery in Morbidly Obese Adolescents: A Systematic Review and Meta-analysis. Obes. Surg. 2015, 25, 860–878. [Google Scholar] [CrossRef] [Green Version]
- Frías, J.P.; Davies, M.J.; Rosenstock, J.; Pérez Manghi, F.C.; Fernández Landó, L.; Bergman, B.K.; Liu, B.; Cui, X.; Brown, K. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 503–515. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Drug Name | Orlistat | Phentermine and Topiramate Combination | Liraglutide |
|---|---|---|---|
| Pharmacological class | Lipase inhibitor | Combination of sympathomimetic and GABAA receptor agonist | Glucagon-like peptide 1 (GLP-1) receptor agonists |
| Dose | 120 mg | NA | 3 mg |
| Frequency | Three times daily | Once daily | Once daily |
| Route of administration | Orally | Orally | Subcutaneous (S.C.) |
| Most common adverse effects | steatorrhea, flatulence, constipation, and occasionally deficit of fat-soluble vitamins. | Paresthesia, dry mouth, constipation, dysgeusia, insomnia. | Gastrointestinal (nausea, vomiting and diarrhea) |
| Efficacy (expressed as reduction in BMI and/or weight) | BMI reduction by 0.7 kg/m2 | Average weight loss by 6.2 kg. | 5–10% BMI reduction |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaban Mohamed, M.A.; AbouKhatwa, M.M.; Saifullah, A.A.; Hareez Syahmi, M.; Mosaad, M.; Elrggal, M.E.; Dehele, I.S.; Elnaem, M.H. Risk Factors, Clinical Consequences, Prevention, and Treatment of Childhood Obesity. Children 2022, 9, 1975. https://doi.org/10.3390/children9121975
Shaban Mohamed MA, AbouKhatwa MM, Saifullah AA, Hareez Syahmi M, Mosaad M, Elrggal ME, Dehele IS, Elnaem MH. Risk Factors, Clinical Consequences, Prevention, and Treatment of Childhood Obesity. Children. 2022; 9(12):1975. https://doi.org/10.3390/children9121975
Chicago/Turabian StyleShaban Mohamed, Mossad Abdelhak, Merna Mahmoud AbouKhatwa, Abdul Aziz Saifullah, Muhammad Hareez Syahmi, Mohamed Mosaad, Mahmoud E. Elrggal, Inderpal Singh Dehele, and Mohamed Hassan Elnaem. 2022. "Risk Factors, Clinical Consequences, Prevention, and Treatment of Childhood Obesity" Children 9, no. 12: 1975. https://doi.org/10.3390/children9121975