
Ovarian Teratomas in Children and Adolescents: Our Own Experience and Review of Literature
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Łuczak, J.; Bagłaj, M. Ovarian teratoma in children: A plea for collaborative clinical study. J. Ovarian Res. 2018, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Lindfors, O. Primary ovarian neoplasms in infants and children. A study of 81 cases diagnosed in Finland and Sweden. Ann. Chir. Gynaecol. Fenn. Suppl. 1971, 177, 1–66. [Google Scholar] [PubMed]
- Martelli, H.; Patte, C. [Gonadal tumours in children]. Arch. Pediatr. 2003, 10, 246–250. [Google Scholar] [CrossRef]
- Anton-Păduraru, D.-T.; Miron, I.C.; Lupu, V.V.; Lupu, A.; Hanganu, E. Ovarian teratoma in a teenager causing ureterohydronephrosis: Case report and literature review. Medicine 2021, 100, e26472. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.H.; Kim, J.W.; Shin, S.S.; Jeong, S.I.; Lim, H.S.; Choi, Y.D.; Lee, K.H.; Kang, W.D.; Jeong, Y.Y.; Kang, H.K. Review of ovarian tumors in children and adolescents: Radiologic-pathologic correlation. Radiogr. Rev. Publ. Radiol. Soc. N. Am. Inc 2014, 34, 2039–2055. [Google Scholar] [CrossRef]
- Harms, D.; Zahn, S.; Göbel, U.; Schneider, D.T. Pathology and molecular biology of teratomas in childhood and adolescence. Klin. Padiatr. 2006, 218, 296–302. [Google Scholar] [CrossRef]
- Outwater, E.K.; Siegelman, E.S.; Hunt, J.L. Ovarian teratomas: Tumor types and imaging characteristics. Radiogr. Rev. Publ. Radiol. Soc. N. Am. Inc 2001, 21, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Oosterhuis, J.W.; Looijenga, L.H.; van Echten, J.; de Jong, B. Chromosomal constitution and developmental potential of human germ cell tumors and teratomas. Cancer Genet. Cytogenet. 1997, 95, 96–102. [Google Scholar] [CrossRef]
- Heifetz, S.A.; Cushing, B.; Giller, R.; Shuster, J.J.; Stolar, C.J.; Vinocur, C.D.; Hawkins, E.P. Immature teratomas in children: Pathologic considerations: A report from the combined Pediatric Oncology Group/Children’s Cancer Group. Am. J. Surg. Pathol. 1998, 22, 1115–1124. [Google Scholar] [CrossRef]
- Saida, T.; Mori, K.; Masumoto, T.; Hoshiai, S.; Ishiguro, T.; Sakai, M.; Hara, T.; Ochi, H.; Satoh, T.; Minami, M. Ovarian and non-ovarian teratomas: A wide spectrum of features. Jpn. J. Radiol. 2021, 39, 143–158. [Google Scholar] [CrossRef]
- Al Jama, F.E.; Al Ghamdi, A.A.; Gasim, T.; Al Dakhiel, S.A.; Rahman, J.; Rahman, M.S. Ovarian tumors in children and adolescents--a clinical study of 52 patients in a university hospital. J. Pediatr. Adolesc. Gynecol. 2011, 24, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Sarnacki, S.; Brisse, H. Surgery of ovarian tumors in children. Horm. Res. Paediatr. 2011, 75, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, C.; Pucci, V.; Strambi, S.; Piccolo, R.L.; Martin, A.; Messineo, A. Treatment of Ovarian Lesions in Children and Adolescents: A Retrospective Study of 130 Cases. Pediatr. Hematol. Oncol. 2015, 32, 199–206. [Google Scholar] [CrossRef]
- Elgendy, A.; Lakshminarayanan, B.; Elrouby, A.; Mostafa, M.; Salem, M.A.; Turner, K.; Khairi, A.; Squire, R.; Shehata, S.M.K.; Shehata, S.; et al. Management of pediatric benign ovarian tumors in England and Egypt: A comparative study. Afr. J. Paediatr. Surg. 2020, 17, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Michelotti, B.; Segura, B.J.; Sau, I.; Perez-Bertolez, S.; Prince, J.M.; Kane, T.D. Surgical Management of Ovarian Disease in Infants, Children, and Adolescents: A 15-Year Review. J. Laparoendosc. Adv. Surg. Tech. 2010, 20, 261–264. [Google Scholar] [CrossRef]
- Özcan, R.; Kuruoğlu, S.; Dervişoğlu, S.; Eliçevik, M.; Emir, H.; Büyükünal, C. Ovary-sparing surgery for teratomas in children. Pediatr. Surg. Int. 2013, 29, 233–237. [Google Scholar] [CrossRef]
- Park, J.-Y.; Kim, D.-Y.; Suh, D.-S.; Kim, J.-H.; Kim, Y.-M.; Kim, Y.-T.; Nam, J.N. Outcomes of pediatric and adolescent girls with malignant ovarian germ cell tumors. Gynecol. Oncol. 2015, 137, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Braungart, S.; Craigie, R.J.; Farrelly, P.; Losty, P.D. Ovarian tumors in children: How common are lesion recurrence and metachronous disease? A UK CCLG Surgeons Cancer Group nationwide study. J. Pediatr. Surg. 2020, 55, 2026–2029. [Google Scholar] [CrossRef]
- Terenziani, M.; D’Angelo, P.; Inserra, A.; Boldrini, R.; Bisogno, G.; Babbo, G.L.; Conte, M.; Indna, P.D.; De Pasquale, M.D.; Indolfit, P.; et al. Mature and immature teratoma: A report from the second Italian pediatric study. Pediatr. Blood Cancer 2015, 62, 1202–1208. [Google Scholar] [CrossRef]
- Zhang, M.; Jiang, W.; Li, G.; Xu, C. Ovarian Masses in Children and Adolescents—An Analysis of 521 Clinical Cases. J. Pediatr. Adolesc. Gynecol. 2014, 27, e73–e77. [Google Scholar] [CrossRef]
- Oue, T.; Uehara, S.; Sasaki, T.; Nose, S.; Saka, R.; Yamanaka, H.; Ueno, T.; Tazuke, Y.; Okuyama, H. Treatment and ovarian preservation in children with ovarian tumors. J. Pediatr. Surg. 2015, 50, 2116–2118. [Google Scholar] [CrossRef] [PubMed]
- Andrés, M.M.; Costa, E.; Cañete, A.; Moreno, L.; Castel, V. Solid ovarian tumours in childhood: A 35-year review in a single institution. Clin. Transl. Oncol. 2010, 12, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Chabaud-Williamson, M.; Netchine, I.; Fasola, S.; Larroquet, M.; Lenoir, M.; Patte, C.; Bénifla, J.; Coulomb-L’Herminé, A.; Grapin, C.; Audry, G.; et al. Ovarian-sparing surgery for ovarian teratoma in children. Pediatr. Blood Cancer 2011, 57, 429–434. [Google Scholar] [CrossRef]
- Pashankar, F.; Hale, J.P.; Dang, H.; Krailo, M.; Brady, W.E.; Rodriguez-Galindo, C.; Nicholson, J.C.; Murray, M.J.; Bilmire, D.F.; Stoneham, S.; et al. Is adjuvant chemotherapy indicated in ovarian immature teratomas? A combined data analysis from the Malignant Germ Cell Tumor International Collaborative. Cancer 2016, 122, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Takayasu, H.; Masumoto, K.; Tanaka, N.; Aiyoshi, T.; Sasaki, T.; Ono, K.; Chiba, F.; Urita, Y.; Shinkai, T. A clinical review of ovarian tumors in children and adolescents. Pediatr. Surg. Int. 2020, 36, 701–709. [Google Scholar] [CrossRef]
- Oltmann, S.C.; Garcia, N.; Barber, R.; Huang, R.; Hicks, B.; Fischer, A. Can we preoperatively risk stratify ovarian masses for malignancy? J. Pediatr. Surg. 2010, 45, 130–134. [Google Scholar] [CrossRef]
- Terzic, M.; Rapisarda, A.M.C.; Corte, D.L.; Manchanda, R.; Aimagambetova, G.; Norton, M.; Garzon, S.; Riemma, G.; King, C.R.; Chiofalo, B.; et al. Diagnostic work-up in paediatric and adolescent patients with adnexal masses: An evidence-based approach. J. Obstet. Gynaecol. 2021, 41, 503–515. [Google Scholar] [CrossRef]
- Ghosh, A.; Ghartimagar, D.; Thapa, S.; Sathian, B.; Narasimhan, R.; Talwar, O.P. Ovarian Tumors: Pattern of Histomorphological Types-A 10 Years Study in a Tertiary Referral Center and Review of Literature. Kathmandu Univ. Med. J. 2016, 14, 153–158. [Google Scholar]
- Renaud, E.J.; Sømme, S.; Islam, S.; Cameron, D.B.; Gates, R.L.; Williams, R.F.; Jancelewicz, T.; Oyetunji, T.A.; Grabowski, J.; Diefenbach, K.A.; et al. Ovarian masses in the child and adolescent: An American Pediatric Surgical Association Outcomes and Evidence-Based Practice Committee systematic review. J. Pediatr. Surg. 2019, 54, 369–377. [Google Scholar] [CrossRef]
- Spinelli, C.; Piscioneri, J.; Strambi, S. Adnexal torsion in adolescents: Update and review of the literature. Curr. Opin. Obstet. Gynecol. 2015, 27, 320–325. [Google Scholar] [CrossRef]
- Spinelli, C.; Strambi, S.; Masoni, B.; Ghionzoli, M.; Bertocchini, A.; Sanna, B.; Morganti, R.; Messina, M.; Molinaro, F.; Tursini, S.; et al. Surgical management of ovarian teratomas in childhood: A multicentric study on 110 cases and a literature review. Gynecol. Endocrinol. 2021, 37, 950–954. [Google Scholar] [CrossRef]
- Spinelli, C.; Pucci, V.; Buti, I.; Liserre, J.; Messineo, A.; Bianco, F.; Ugolini, C. The Role of Tumor Markers in the Surgical Approach of Ovarian Masses in Pediatric Age: A 10-Year Study and a Literature Review. Ann. Surg. Oncol. 2012, 19, 1766–1773. [Google Scholar] [CrossRef] [PubMed]
- Loh, A.H.P.; Gee, K.W.C.; Chua, J.H.Y. Diagnostic accuracy of preoperative alpha-fetoprotein as an ovarian tumor marker in children and adolescents: Not as good as we thought? Pediatr. Surg. Int. 2013, 29, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Kaijser, J.; Bourne, T.; Valentin, L.; Sayasneh, A.; Van Holsbeke, C.; Vergote, I.; Testa, A.C.; Franchi, D.; Van Calster, B.; Timmerman, D. Improving strategies for diagnosing ovarian cancer: A summary of the International Ovarian Tumor Analysis (IOTA) studies. Ultrasound Obstet. Gynecol. 2013, 41, 9–20. [Google Scholar] [CrossRef]
- Spinelli, C.; Strambi, S.; Liloia, C.; Bertocchini, A.; Messineo, A. Update on the surgical management of ovarian neoplasms in children and adolescents: Analysis on 32 cases. Gynecol. Endocrinol. 2016, 32, 787–791. [Google Scholar] [CrossRef]
- Braungart, S.; Craigie, R.J.; Losty, P.D. Controversies in the management of ovarian tumours in prepubertal children — A BAPS and UK CCLG Surgeons Cancer Group National Survey. J. Pediatr. Surg. 2018, 53, 2231–2234. [Google Scholar] [CrossRef]
- Hayes-Jordan, A. Surgical management of the incidentally identified ovarian mass. Semin. Pediatr. Surg. 2005, 14, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Malkan, A.D.; Loh, A.H.; Sandoval, J.A. Minimally invasive surgery in the management of abdominal tumors in children. J. Pediatr. Surg. 2014, 49, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, D.O.; Cooper, J.N.; Aldrink, J.H.; Hewitt, G.D.; Fallat, M.E.; Minneci, P.C.; Deans, K.J. Variability in surgical management of benign ovarian neoplasms in children. J. Pediatr. Surg. 2017, 52, 944–950. [Google Scholar] [CrossRef]
- Rousseau, V.; Massicot, R.; Darwish, A.A.; Sauvat, F.; Emond, S.; Thibaud, E.; Nihoul-Fékété, C. Emergency Management and Conservative Surgery of Ovarian Torsion in Children: A Report of 40 Cases. J. Pediatr. Adolesc. Gynecol. 2008, 21, 201–206. [Google Scholar] [CrossRef]


{kind=link}
| Item | Our Series (n = 40) | Literature (n = 1418) |
|---|---|---|
| Mean age at diagnosis | 11.8 | 10.4 |
| Adnexal torsion | 12 | 481 |
| Biochemical markers elevated | 8 | 57 |
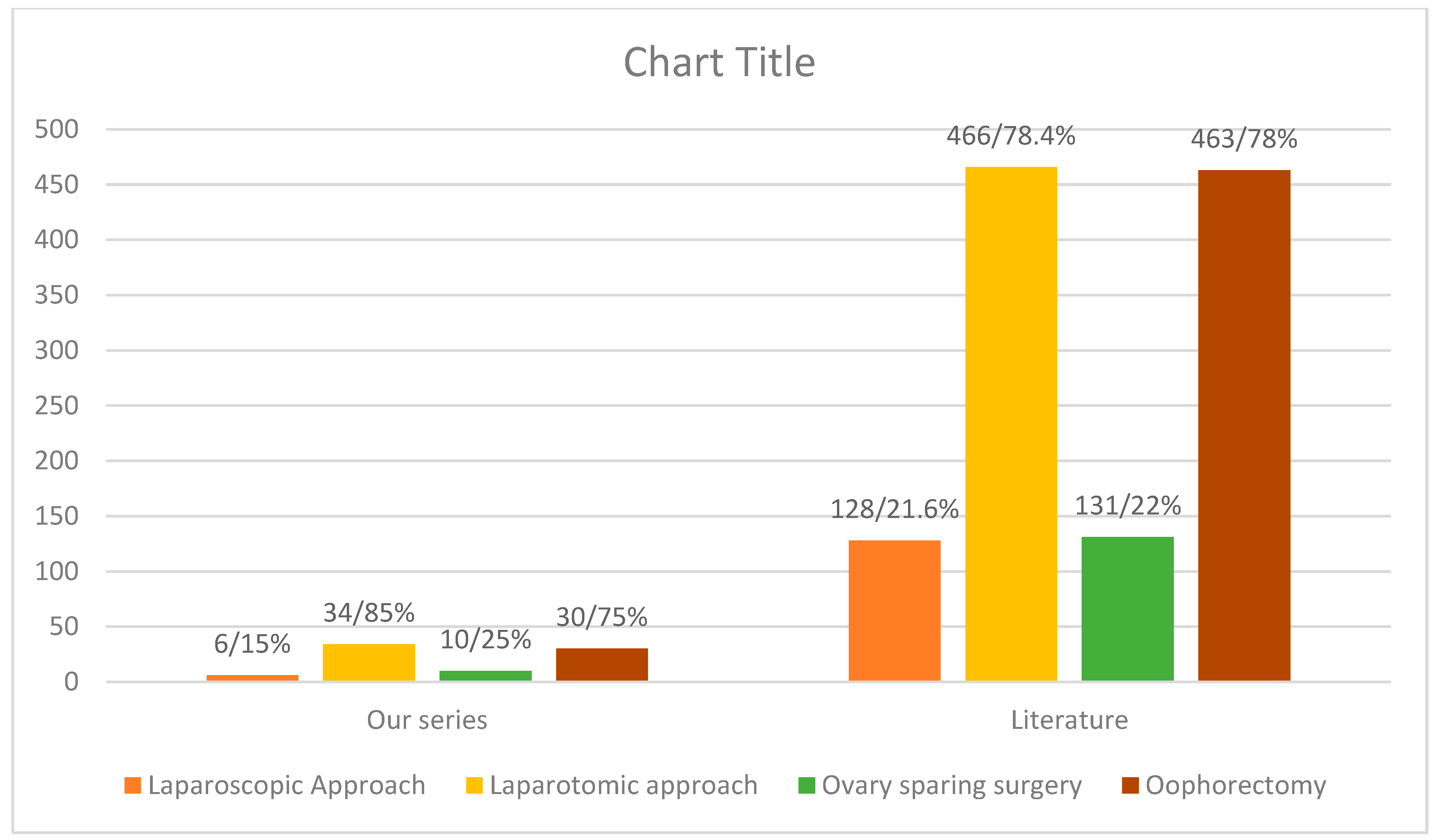
| Oophorectomy | 30 | 463 |
| Ovary-sparing surgery | 10 | 131 |
| Laparoscopic approach | 6 | 128 |
| Laparotomic approach | 34 | 466 |
| Acute abdominal pain | 12 | 506 |
| Chronic abdominal pain | 27 | 192 |
| Palpable mass | Not mentioned | 146 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkrozou, F.; Tsonis, O.; Vatopoulou, A.; Galaziou, G.; Paschopoulos, M. Ovarian Teratomas in Children and Adolescents: Our Own Experience and Review of Literature. Children 2022, 9, 1571. https://doi.org/10.3390/children9101571
Gkrozou F, Tsonis O, Vatopoulou A, Galaziou G, Paschopoulos M. Ovarian Teratomas in Children and Adolescents: Our Own Experience and Review of Literature. Children. 2022; 9(10):1571. https://doi.org/10.3390/children9101571
Chicago/Turabian StyleGkrozou, Fani, Orestis Tsonis, Anastasia Vatopoulou, Georgia Galaziou, and Minas Paschopoulos. 2022. "Ovarian Teratomas in Children and Adolescents: Our Own Experience and Review of Literature" Children 9, no. 10: 1571. https://doi.org/10.3390/children9101571