
Bariatric Surgery in Adolescents: To Do or Not to Do?

 , , , ,
, , , ,  , and
, and
Abstract
:
1. Introduction
2. Methods
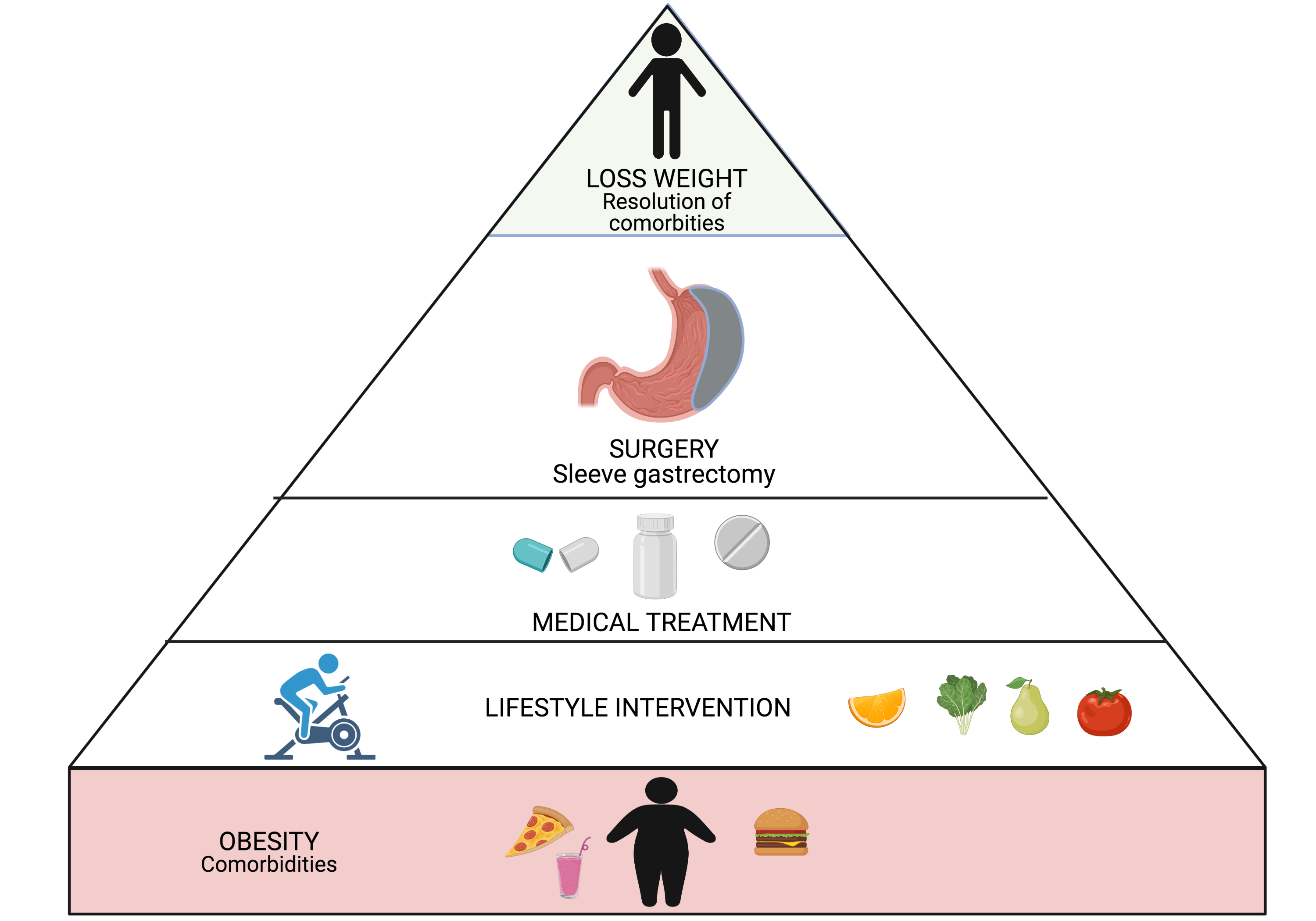
3. Obesity, Cardiometabolic Complications and Medical Treatment
4. Eligibility Criteria for Bariatric Surgery
- -
- at least 6 months of lifestyle treatment for weight loss in a specialized center
- -
- complete skeletal and sexual maturation
- -
- ability to give informed consent with adequate understanding of the procedure
- -
- ability to commit to comprehensive medical and psychological evaluation before and after surgery
- -
- willing to participate in a post-surgery multidisciplinary program
- -
- surgery access in a unit with specialist pediatric support
- Obesity that can treated with medical therapy.
- Substance abuse within the past year.
- Current or planned pregnancy within 12–18 months of the scheduled surgical procedure.
- Concomitant eating disorders.
- Medical, psychiatric, psychosocial issues interfering with postsurgical recommendations and required lifestyle modifications
5. Laparoscopic Sleeve Gastrectomy as Preferred Surgical Approach
6. Nutritional Status and Nutritional Risks
7. Weight Loss and Resolution of the Metabolic Comorbidities
8. Future Perspectives
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of obesity and severe obesity in US children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [Green Version]
- Center for Disease Control and Prevention. Available online: https://www.cdc.gov/nchs/products/index.htm (accessed on 2 April 2021).
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twig, G.; Tirosh, A.; Leiba, A.; Twig, G.; Tirosh, A.; Leiba, A.; Levine, H.; Ben-Ami Shor, D.; Derazne, E.; Haklai, Z.; et al. BMI at Age 17 Years and Diabetes Mortality in Midlife: A Nationwide Cohort of 2.3 Million Adolescents. Diabetes Care 2016, 39, 1996–2003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leopold, S.; Zachariah, J.P. Pediatric Obesity, Hypertension, Lipids. Curr. Treat Options Pediatr. 2020, 6, 62–77. [Google Scholar] [CrossRef] [PubMed]
- Mencin, A.A.; Lavine, J.E. Nonalcoholic fatty liver disease in children. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 151–157. [Google Scholar] [CrossRef]
- Bitners, A.C.; Sin, S.; Agrawal, S.; Lee, S.; Udupa, J.K.; Tong, Y.; Wootton, D.M.; Choy, K.R.; Wagshul, M.E.; Arens, R. Effect of sleep on upper airway dynamics in obese adolescents with obstructive sleep apnea syndrome. Sleep 2020, 43, zsaa071. [Google Scholar] [CrossRef]
- Kaczmarek, C.; Haller, D.M.; Yaron, M.J. Health-Related Quality of Life in Adolescents and Young Adults with Polycystic Ovary Syndrome: A Systematic Review. J. Pediatr. Adolesc. Gynecol. 2016, 29, 551–557. [Google Scholar] [CrossRef]
- Malhotra, S.; Czepiel, K.S.; Akam, E.Y.; Shaw, A.Y.; Sivasubramanian, R.; Seetharaman, S.; Stanford, F.C. Bariatric surgery in the treatment of adolescent obesity: Current perspectives in the United States. Expert Rev. Endocrinol. Metab. 2021, 21, 1–12. [Google Scholar]
- Park, K.H. Intervention for severely obese children and adolescents. J. Obes. Metab. Syndr. 2019, 28, 1–3. [Google Scholar] [CrossRef]
- Lennerz, B.S.; Wabitsch, M.; Lippert, H.; Wolff, S.; Knoll, C.; Weiner, R.; Manger, T.; Kiess, W.; Stroh, C. Bariatric surgery in adolescents and young adults—Safety and effectiveness in a cohort of 345 patients. Int. J. Obes. 2014, 38, 334–340. [Google Scholar] [CrossRef]
- Kelleher, D.C.; Merrill, C.T.; Cottrell, L.T.; Nadler, E.P.; Burd, R.S. Recent national trends in the use of adolescent inpatient bariatric surgery: 2000 through 2009. JAMA Pediatr. 2013, 167, 126–132. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, A.; Elahmedi, M.; Alqahtani, Y.A.; Al-Darwish, A. Endoscopic Sleeve Gastroplasty in 109 Consecutive Children and Adolescents with Obesity: Two-Year Outcomes of a New Modality. Am. J. Gastroenterol. 2019, 114, 1857–1862. [Google Scholar] [CrossRef]
- Cooiman, M.I.; Aarts, E.O.; Janssen, I.M.C.; Hazebroek, E.J.; Berends, F.J. Weight Loss, Remission of Comorbidities, and Quality of Life After Bariatric Surgery in Young Adult Patients. Obes. Surg. 2019, 29, 1851–1857. [Google Scholar] [CrossRef]
- Harvard T.H. Chan School of Public Health. Defining Childhood Obesity. Available online: https://www.hsph.harvard.edu/obesity-prevention-source/obesity-definition/defining-childhood-obesity/#References (accessed on 2 April 2021).
- Center for Disease Control and Prevention. Defining Childhood Obesity BMI for Children and Teens. Available online: https://www.cdc.gov/obesity/childhood/defining.html (accessed on 2 April 2021).
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Kansra, A.R.; Lakkunarajah, S.; Jay, M.S. Childhood and Adolescent Obesity: A Review. Front. Pediatr. 2021, 8, 581461. [Google Scholar] [CrossRef]
- Sangun, Ö.; Dündar, B.; Köşker, M.; Pirgon, Ö.; Dündar, N. Prevalence of metabolic syndrome in obese children and adolescents using three different criteria and evaluation of risk factors. J. Clin. Res. Pediatr. Endocrinol. 2011, 3, 70–76. [Google Scholar] [CrossRef]
- Cook, S.; Weitzman, M.; Auinger, P.; Nguyen, M.; Dietz, W.H. Pre-valence of a metabolic syndrome phenotype in adolescents: Findings from the third National Health and Nutrition Examination Survey, 1988–1994. Arch. Pediatr. Adolesc. Med. 2003, 157, 821–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Ferranti, S.D.; Gauvreau, K.; Ludwig, D.S.; Neufeld, E.J.; Newburger, J.W.; Rifai, N. Prevalence of the metabolic syndrome in American adolescents: Findings from the Third National Health and Nutrition Examination Survey. Circulation 2004, 110, 2494–2497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reisinger, C.; Nkeh-Chungag, B.N.; Fredriksen, P.M.; Goswami, N. The prevalence of pediatric metabolic syndrome—A critical look on the discrepancies between definitions and its clinical importance. Int. J. Obes. 2021, 45, 12–24. [Google Scholar] [CrossRef]
- Miller, J.M.; Kaylor, M.B.; Johannsson, M.; Bay, C.; Churilla, J.R. Prevalence of metabolic syndrome and individual criterion in US adolescents: 2001–2010 National Health and Nutrition Examination Survey. Metab. Syndr. Relat. Disord. 2014, 12, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Asghari, G.; Eftekharzadeh, A.; Hosseinpanah, F.; Ghareh, S.; Mirmiran, P.; Azizi, F. Instability of different adolescent metabolic syndrome definitions tracked into early adulthood metabolic syndrome: Tehran Lipid and Glucose Study (TLGS). Pediatr. Diabetes 2017, 18, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD. Health at a Glance. 2017. Available online: https://www.oecd.org/social/health-at-a-glance-19991312.htm (accessed on 2 April 2021).
- Al-Hamad, D.; Raman, V. Metabolic syndrome in children and adolescents. Transl. Pediatr. 2017, 6, 397–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Giuseppe, R.; Di Napoli, I.; Porri, D.; Cena, H. Pediatric Obesity and Eating Disorders Symptoms: The Role of the Multidisciplinary Treatment. A Systematic Review. Front. Pediatr. 2019, 7, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric obesity-assessment, treatment, and prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.B.; Nemeth, B.A.; Clark, R.R.; Peterson, S.E.; Eickhoff, J.; Carrel, A.L. Fitness is a stronger predictor of fasting insulin levels than fatness in overweight male middle-school children. J. Pediatr. 2007, 150, 383–387. [Google Scholar] [CrossRef]
- Martínez-Gómez, D.; Eisenmann, J.C.; Moya, J.M.; Gómez-Martínez, S.; Marcos, A.; Veiga, O.L. The role of physical activity and fitness on the metabolic syndrome in adolescents: Effect of different scores. The AFINOS Study. J. Physiol. Biochem. 2009, 65, 277–289. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, N.S.; Ruiz, J.R.; Oja, L.; Veidebaum, T.; Sjöström, M. Associations between physical activity, body fat, and insulin resistance (homeostasis model assessment) in adolescents: The European Youth Heart Study. Am. J. Clin. Nutr. 2008, 87, 586–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, J.J.; Eisenmann, J.C.; Norman, G.J.; Ortiz, K.A.; Young, P.C. Dietary fiber and nutrient density are inversely associated with the metabolic syndrome in USA adolescents. J. Am. Diet. Assoc. 2011, 111, 1688–1695. [Google Scholar] [CrossRef]
- Lin, Y.; Huybrechts, I.; Vereecken, C.; Mourati-dou, T.; Valtueña, J.; Kersting, M.; González-Gross, M.; Bolca, S.; Wärnberg, J.; Cuenca-García, M.; et al. Dietary fiber intake and its association with indicators of adiposity and serum biomarkers in European adolescents: The HELENA study. Eur. J. Nutr. 2014, 54, 771–782. [Google Scholar] [CrossRef]
- Dorgan, J.F.; Liu, L.; Barton, B.A.; Deshmukh, S.; Snetselaar, L.G.; Van Horn, L.; Stevens, V.J.; Robson, A.M.; Lasser, N.L.; Himes, J.H.; et al. Adolescent diet and metabolic syndrome in young women: Results of the Dietary Intervention Study in Children (DISC) follow-up study. J. Clin. Endocrinol. Metab. 2011, 96, E1999–E2008. [Google Scholar] [CrossRef]
- Kim, B.; Choi, H.N.; Yim, J.E. Effect of Diet on the Gut Microbiota Associated with Obesity. J. Obes. Metab. Syndr. 2019, 28, 216–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.N.; Mann, N.J.; Braue, A.; Mäkeläinen, H.; Varigos, G.A. A low-glycemic-load diet improves symptoms in acne vulgaris patients: A randomized controlled trial. Am. J. Clin. Nutr. 2007, 86, 107–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demol, S.; Yackobovitch-Gavan, M.; Shalitin, S.; Nagelberg, N.; Gillon-Keren, M.; Phillip, M. Low-carbohydrate (low & high-fat) versus 53 high-carbohydrate low-fat diets in the treatment of obesity in adolescents. Acta Paediatric 2009, 98, 346–351. [Google Scholar]
- Statovci, D.; Aguilera, M.; MacSharry, J.; Melgar, S. The impact of Western diet and nutrients on the microbiota and immune response at mucosal interfaces. Front. Immunol. 2017, 8, 838. [Google Scholar] [CrossRef] [Green Version]
- Cena, H.; Calder, P.C. Defining a Healthy Diet: Evidence for The Role of Contemporary Dietary Patterns in Health and Disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [Green Version]
- Calcaterra, V.; Regalbuto, C.; Porri, D.; Pelizzo, G.; Mazzon, E.; Vinci, F.; Zuccotti, G.; Fabiano, V.; Cena, H. Inflammation in Obesity-Related Complications in Children: The Protective Effect of Diet and Its Potential Role as a Therapeutic Agent. Biomolecules 2020, 10, 1324. [Google Scholar] [CrossRef]
- Patel, D.K.; Stanford, F.C. Safety and tolerability of new-generation anti-obesity medications: A narrative review. Postgrad. Med. 2018, 130, 173–182. [Google Scholar] [CrossRef]
- Flynn, J.T.; Kaelber, D.C.; Baker-Smith, C.M.; Blowey, D.; Carroll, A.E.; Daniels, S.R.; de Ferranti, S.D.; Dionne, J.M.; Falkner, B.; Flinn, S.K.; et al. Subcommittee on screening and management of high blood pressure in children. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 2017, 140, e20171904. [Google Scholar] [CrossRef] [Green Version]
- Inge, T.H.; Laffel, L.M.; Jenkins, T.M.; Marcus, M.D.; Leibel, N.I.; Brandt, M.L.; Haymond, M.; Urbina, E.M.; Dolan, L.M.; Zeitler, P.S. Teen–Longitudinal Assessment of Bariatric Surgery (Teen-LABS) and Treatment Options of Type 2 Diabetes in Adolescents and Youth (TODAY) Consortia. Comparison of Surgical and Medical Therapy for Type 2 Diabetes in Severely Obese Adolescents. JAMA Pediatr. 2018, 172, 452–460. [Google Scholar] [CrossRef]
- Czepiel, K.S.; Perez, N.P.; Campoverde Reyes, K.J.; Sabharwal, S.; Stanford, F.C. Pharmacotherapy for the Treatment of Overweight and Obesity in Children, Adolescents, and Young Adults in a Large Health System in the US. Front. Endocrinol. 2020, 11, 290. [Google Scholar] [CrossRef] [PubMed]
- Johnson, V.R.; Cao, M.; Czepiel, K.S.; Mushannen, T.; Nolen, L.; Stanford, F.C. Strategies in the Management of Adolescent Obesity. Curr. Pediatr. Rep. 2020, 8, 56–65. [Google Scholar] [CrossRef]
- Mastrandrea, L.D.; Witten, L.; Carlsson Petri, K.C.; Hale, P.M.; Hedman, H.K.; Riesenberg, R.A. Liraglutide effects in a paediatric (7-11 y) population with obesity: A randomized, double-blind, placebo-controlled, short-term trial to assess safety, tolerability, pharmacokinetics, and pharmacodynamics. Pediatr. Obes. 2019, 14, e12495. [Google Scholar] [CrossRef] [Green Version]
- Singhal, S.; Kumar, S. Current Perspectives on Management of Type 2 Diabetes in Youth. Children 2021, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- White, B.; Jamieson, L.; Clifford, S.; Shield, J.P.; Christie, D.; Smith, F.; Wong, I.C.; Viner, R.M. Adolescent experiences of anti-obesity drugs. Clin. Obes. 2015, 5, 116–126. [Google Scholar] [CrossRef] [Green Version]
- Rogovik, A.L.; Goldman, R.D. Pharmacologic treatment of pediatric obesity. Can. Fam. Physician 2011, 57, 195–197. [Google Scholar] [PubMed]
- Yanovski, J.A.; Krakoff, J.; Salaita, C.G.; McDuffie, J.R.; Kozlosky, M.; Sebring, N.G.; Reynolds, J.C.; Brady, S.M.; Calis, K.A. Effects of metformin on body weight and body composition in obese insulin-resistant children: A randomized clinical trial. Diabetes 2011, 60, 477–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy-Marchal, C.; Arslanian, S.; Cutfield, W.; Sinaiko, A.; Druet, C.; Marcovecchio, M.L.; Chiarelli, F. Insulin resistance in children: Consensus, perspective, and future directions. J. Clin. Endocrinol. Metab. 2010, 95, 5189–5198. [Google Scholar] [CrossRef] [Green Version]
- Daniels, S.R.; Greer, F.R.; Committee on Nutrition. Lipid screening and cardiovascular health in childhood. Pediatrics 2008, 122, 198–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung and Blood Institute. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: Summary report. Pediatrics 2011, 128, S213–S256. [Google Scholar] [CrossRef] [Green Version]
- Avis, H.J.; Vissers, M.N.; Stein, E.A.; Wijburg, F.A.; Trip, M.D.; Kastelein, J.J.; Hutten, B.A. A systematic review and meta-analysis of statin therapy in children with familial hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1803–1810. [Google Scholar] [CrossRef] [Green Version]
- Sinha, R.; Saha, A.; Samuels, J. American Academy of Pediatrics Clinical Practice Guidelines for Screening and Management of High Blood Pressure in Children and Adolescents: What is New? Indian Pediatr. 2019, 56, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Pratt, J.S.A.; Browne, A.; Browne, N.T.; Bruzoni, M.; Cohen, M.; Desai, A.; Inge, T.; Linden, B.C.; Mattar, S.G.; Michalsky, M.; et al. ASMBS pediatric metabolic and bariatric surgery guidelines, 2018. Surg. Obes. Relat. Dis. 2018, 14, 882–901. [Google Scholar] [CrossRef]
- Vlaev, I.; Taylor, M.J.; Taylor, D.; Gately, P.; Gunn, L.H.; Abeles, A.; Kerkadi, A.; Lothian, J.; Jreige, S.K.; Alsaadi, A.; et al. Testing a multicomponent lifestyle intervention for combatting childhood obesity. BMC Public Health 2021, 21, 824. [Google Scholar] [CrossRef]
- Michalsky, M.; Reichard, K.; Inge, T.; Pratt, J.; Lenders, C.; American Society for Metabolic and Bariatric Surgery. ASMBS pediatric committee best practice guidelines. Surg. Obes. Relat. Dis. 2012, 8, 1–7. [Google Scholar] [CrossRef]
- Fildes, A.; Charlton, J.; Rudisill, C.; Littlejohns, P.; Prevost, A.T.; Gulliford, M.C. Probability of an Obese Person Attaining Normal Body Weight: Cohort Study Using Electronic Health Records. Am. J. Public Health 2015, 105, e54–e59. [Google Scholar] [CrossRef] [Green Version]
- Ogle, S.B.; Dewberry, L.C.; Jenkins, T.M.; Inge, T.H.; Kelsey, M.; Bruzoni, M.; Pratt, J.S.A. Outcomes of Bariatric Surgery in Older Versus Younger Adolescents. Pediatrics 2021, 147, e2020024182. [Google Scholar] [CrossRef] [PubMed]
- Chopra, I.; Kamal, K.M. Factors associated with therapeutic goal attainment in patients with concomitant hypertension and dyslipidemia. Hosp. Pract. 2014, 42, 77–88. [Google Scholar] [CrossRef]
- Fiechtner, L.; Fonte, M.L.; Castro, I.; Gerber, M.; Horan, C.; Sharifi, M.; Cena, H.; Taveras, E.M. Determinants of Binge Eating Symptoms in Children with Overweight/Obesity. Child. Obes. 2018, 14, 510–517. [Google Scholar] [CrossRef]
- Treadwell, J.R.; Sun, F.; Schoelles, K. Systematic review and meta-analysis of bariatric surgery for pediatric obesity. Ann. Surg. 2008, 248, 763–776. [Google Scholar] [CrossRef]
- Roebroek, Y.G.M.; Pruijssers, S.R.; Bouvy, N.D.; van Heurn, E.L.W.E. Current Opinions and Practices of Bariatric Surgery in Adolescents: A Survey among Pediatric Surgeons. Eur. J. Pediatr. Surg. 2020, 30, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Beamish, A.J.; Reinehr, T. Should bariatric surgery be performed in adolescents? Eur. J. Endocrinol. 2017, 176, D1–D15. [Google Scholar] [CrossRef] [PubMed]
- Khidir, N.; El-Matbouly, M.A.; Sargsyan, D.; Al-Kuwari, M.; Bashah, M.; Gagner, M. Five-year Outcomes of Laparoscopic Sleeve Gastrectomy: A Comparison between Adults and Adolescents. Obes. Surg. 2018, 28, 2040–2045. [Google Scholar] [CrossRef]
- Stanford, F.C.; Mushannen, T.; Cortez, P.; Campoverde Reyes, K.J.; Lee, H.; Gee, D.W.; Pratt, J.S.; Boepple, P.A.; Bredella, M.A.; Misra, M.; et al. Comparison of Short and Long-Term Outcomes of Metabolic and Bariatric Surgery in Adolescents and Adults. Front. Endocrinol. 2020, 11, 157. [Google Scholar] [CrossRef]
- Steinhart, A.; Tsao, D.; Pratt, J.S.A. Pediatric Metabolic and Bariatric Surgery. Surg. Clin. N. Am. 2021, 101, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, N.; Antoniou, S.A.; Batterham, R.L.; Busetto, L.; Godoroja, D.; Iossa, A.; Carrano, F.M.; Agresta, F.; Alarçon, I.; Azran, C.; et al. Clinical practice guidelines of the European Association for Endoscopic Surgery (EAES) on bariatric surgery: Update 2020 endorsed by IFSO-EC, EASO and ESPCOP. Surg. Endosc. 2020, 34, 2332–2358. [Google Scholar] [CrossRef] [Green Version]
- Nobili, V.; Vajro, P.; Dezsofi, A.; Fischler, B.; Hadzic, N.; Jahnel, J.; Lamireau, T.; McKiernan, P.; McLin, V.; Socha, P.; et al. Indications and limitations of bariatric intervention in severely obese children and adolescents with and without nonalcoholic steatohepatitis: ESPGHAN Hepatology Committee Position Statement. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 550–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundy, D.A.P.; Silva, N.D.; Horton, S.; Jamison, D.T.; Patton, G.C. (Eds.) Child and Adolescent Health and Development, 3rd ed.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017. [Google Scholar]
- Cena, H.; Stanford, F.C.; Ochner, L.; Fonte, M.L.; Biino, G.; De Giuseppe, R.; Taveras, E.; Misra, M. Association of a history of childhood-onset obesity and dieting with eating disorders. Eat. Disord. 2017, 25, 216–229. [Google Scholar] [CrossRef]
- Goldschmidt, A.B.; Khoury, J.; Jenkins, T.M.; Bond, D.S.; Thomas, J.G.; Utzinger, L.M.; Zeller, M.H.; Inge, T.H.; Mitchell, J.E. Adolescent Loss-of-Control Eating and Weight Loss Maintenance After Bariatric Surgery. Pediatrics 2018, 141, e20171659. [Google Scholar] [CrossRef] [Green Version]
- Utzinger, L.M.; Gowey, M.A.; Zeller, M.; Jenkins, T.M.; Engel, S.G.; Rofey, D.L.; Inge, T.H.; Mitchell, J.E. Teen Loss of control eating and eating disorders in adolescents before bariatric surgery. Int. J. Eat. Disord. 2016, 49, 947–952. [Google Scholar] [CrossRef] [Green Version]
- Jarvholm, K.; Olbers, T.; Peltonen, M.; Marcus, C.; Dahlgren, J.; Flodmark, C.E.; Henfridsson, P.; Gronowitz, E.; Karlsson, J. Binge eating and other eating-related problems in adolescents undergoing gastric bypass: Results from a Swedish nationwide study (AMOS). Appetite 2018, 127, 349–355. [Google Scholar] [CrossRef]
- Austin, H.; Smith, K.; Ward, W.L. Psychological assessment of the adolescent bariatric surgery candidate. Surg. Obes. Relat. Dis. 2013, 9, 474–480. [Google Scholar] [CrossRef]
- Tagi, V.M.; Samvelyan, S.; Chiarelli, F. Treatment of Metabolic Syndrome in Children. Horm. Res. Pediatr. 2020, 93, 215–225. [Google Scholar] [CrossRef]
- Kheirvari, M.; Nikroo, N.D.; Jaafarinejad, H.; Farsimadan, M.; Eshghjoo, S.; Hosseini, S.; Anbara, T. The advantages and disadvantages of sleeve gastrectomy; clinical laboratory to bedside review. Heliyon 2020, 6, e03496. [Google Scholar] [CrossRef] [Green Version]
- Arman, G.A. Long-term (11+years) outcomes in weight, patient satisfaction, comorbidities, and gastroesophageal reflux treatment after laparoscopic sleeve gastrectomy. Surg. Obes. Relat. Dis. 2016, 12, 1778–1786. [Google Scholar] [CrossRef] [PubMed]
- Xanthakos, S.A.; Khoury, J.C.; Inge, T.H.; Jenkins, T.M.; Modi, A.C.; Michalsky, M.P.; Chen, M.K.; Courcoulas, A.P.; Harmon, C.M.; Brandt, M.L.; et al. Teen Longitudinal Assessment of Bariatric Surgery Consortium. Nutritional Risks in Adolescents After Bariatric Surgery. Clin. Gastroenterol. Hepatol. 2020, 18, 1070–1081. [Google Scholar] [CrossRef]
- Bondada, S.; Jen, H.C.; Deugarte, D.A. Outcomes of bariatric surgery in adolescents. Curr. Opin. Pediatr. 2011, 23, 552–556. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Kim, E.; Vu, S.; Phelan, M. Ten-year Outcomes of a Prospective Randomized Trial of Laparoscopic Gastric Bypass Versus Laparoscopic Gastric Banding. Ann. Surg. 2018, 268, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Inge, T.H.; Courcoulas, A.P.; Helmrath, M.A. Five-Year Outcomes of Gastric Bypass in Adolescents as Compared with Adults. Reply. N. Engl. J. Med. 2019, 381, e17. [Google Scholar] [PubMed]
- Oberbach, A.; Neuhaus, J.; Inge, T.; Kirsch, K.; Schlichting, N.; Blüher, S.; Kullnick, Y.; Kugler, J.; Baumann, S.; Till, H. Bariatric surgery in severely obese adolescents improves major comorbidities including hyperuricemia. Metabolism 2014, 63, 242–249. [Google Scholar] [CrossRef]
- Griggs, C.L.; Perez, N.P., Jr.; Goldstone, R.N.; Kelleher, C.M.; Chang, D.C.; Stanford, F.C.; Pratt, J.S. National Trends in the Use of Metabolic and Bariatric Surgery Among Pediatric Patients with Severe Obesity. JAMA Pediatr. 2018, 172, 1191–1192. [Google Scholar] [CrossRef]
- Nadler, E.P. Bariatric surgery and childhood obesity. Preface. Semin. Pediatr. Surg. 2014, 23, 1. [Google Scholar]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Higa, K.; Himpens, J.; Buchwald, H.; Scopinaro, N.I.F.S.O. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes. Surg. 2018, 28, 3783–3794. [Google Scholar] [CrossRef]
- Marnicola, G.; Gallo, C.; Hassan, C.; Raffaelli, M.; Costamagna, G.; Bove, V.; Pontecorvi, V.; Orlandini, B.; Boškoski, I. Laparoscopic sleeve gastrectomy versus endoscopic sleeve gastroplasty: A systematic review and meta-analysis. Endosc. Int. Open 2021, 9, E87–E95. [Google Scholar] [CrossRef]
- Durkin, N.; Desai, A.P. What Is the Evidence for Paediatric/Adolescent Bariatric Surgery? Curr. Obes. Rep. 2017, 6, 278–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaar, M.E. Thirty-day outcomes of sleeve gastrectomy versus Roux-en-Y gastric bypass: First report based on Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database. Surg. Obes. Relat. Dis. 2018, 14, 545–551. [Google Scholar] [CrossRef]
- Spaniolas, K.; Yang, J.; Zhu, C.; Maria, A.; Bates, A.T.; Docimo, S.; Talamini, M.; Pryor, A.D. Conversion of Adjustable Gastric Banding to Stapling Bariatric Procedures: Single- or Two-stage Approach. Ann. Surg. 2021, 273, 542–547. [Google Scholar] [CrossRef]
- Khorgami, Z.; Shoar, S.; Andalib, A.; Aminian, A.; Brethauer, S.A.; Schauer, P.R. Trends in utilization of bariatric surgery, 2010–2014: Sleeve gastrectomy dominates. Surg. Obes. Relat. Dis. 2017, 13, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Altieri, M.S.; DeMaria, E.J. Comment on: Standardized Reporting of Comorbidity Outcome After Bariatric Surgery: Low Compliance with the ASMBS Outcome Reporting Standards Despite Ease of Use. Surg. Obes. Relat. Dis. 2020, 16, 1682–1683. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.; Birch, D.W.; Shi, X.; Sharma, A.M.; Karmali, S. Effect of sleeve gastrectomy on gastroesophageal reflux disease: A systematic review. Surg. Obes. Relat. Dis. 2011, 7, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Dang, J.T.; Shelton, J.; Mocanu, V.; Sun, W.; Birch, D.W.; Karmali, S.; Switzer, N.J. Trends and Outcomes of Laparoscopic Sleeve Gastrectomy Between 2015 and 2018 in the USA and Canada. Obes. Surg. 2021, 31, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Pepper, V.K.; Rager, T.M.; Diefenbach, K.A.; Raval, M.V.; Teich, S.; Michalsky, M.P. Robotic vs. Laparoscopic Sleeve Gastrectomy in Adolescents; Reality or Hype. Obes. Surg. 2016, 26, 1912–1917. [Google Scholar] [CrossRef]
- Paulus, G.F.; de Vaan, L.E.; Verdam, F.J.; Bouvy, N.D.; Ambergen, T.A.; van Heurn, L.W. Bariatric surgery in morbidly obese adolescents: A systematic review and meta-analysis. Obes. Surg. 2015, 25, 860–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarr, M.G. Outcome of sleeve gastrectomy as a primary bariatric procedure. Br. J. Surg. 2014, 101, 668. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Brandt, M.L.; Wong, W.W.; Liu, Y.; Mehta, N.R.; Wilson, T.A.; Adolph, A.L.; Puyau, M.R.; Vohra, F.A.; Shypailo, R.J.; et al. Energetic adaptations persist after bariatric surgery in severely obese adolescents. Obesity 2015, 23, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, W.L.; Lewis, S.R.; Bagby, J.P.; Hilton, L.R.; Milad, M.; Bledsoe, S.E. Laparoscopic sleeve gastrectomy versus laparoscopic Roux-en-Y gastric bypass in the pediatric population: A MBSAQIP analysis. Surg. Obes. Relat. Dis. 2020, 16, 254–260. [Google Scholar] [CrossRef]
- Poliakin, L.; Roberts, A.; Thompson, K.J.; Raheem, E.; McKillop, I.H.; Nimeri, A. Outcomes of adolescents compared with young adults after bariatric surgery: An analysis of 227,671 patients using the MBSAQIP data registry. Surg. Obes. Relat. Dis. 2020, 16, 1463–1473. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, R.; Howell, M.H.; Chang, K.H.; Adrales, G.; Magnuson, T.; Schweitzer, M.; Nguyen, H. Robot-assisted versus laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy: A propensity score-matched comparative analysis using the 2015-2016 MBSAQIP database. Surg. Endosc. 2019, 33, 1600–1612. [Google Scholar] [CrossRef]
- Moore, J.M.; Haemer, M.A.; Fox, C.K. Lifestyle and Pharmacologic Management Before and After Bariatric Surgery. Semin. Pediatr. Surg. 2020, 29, 150889. [Google Scholar] [CrossRef] [PubMed]
- Cena, H.; De Giuseppe, R.; Biino, G.; Persico, F.; Ciliberto, A.; Giovanelli, A.; Stanford, F.C. Evaluation of eating habits and lifestyle in patients with obesity before and after bariatric surgery: A single Italian center experience. Springerplus 2016, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Price, P.H.; Kaizer, A.M.; Daniels, S.R.; Jenkins, T.M.; Inge, T.H.; Eckel, R.H. Physical Activity Improves Lipid and Weight-Loss Outcomes After Metabolic Bariatric Surgery in Adolescents with Severe Obesity. Obesity 2019, 27, 989–996. [Google Scholar] [CrossRef]
- Fruh, S.; Williams, S.; Hayes, K.; Hauff, C.; Hudson, G.M.; Sittig, S.; Graves, R.J.; Hall, H.; Barinas, J. A practical approach to obesity prevention: Healthy home habits. J. Am. Assoc. Nurse Pract. 2021. [Google Scholar] [CrossRef] [PubMed]
- Johnson Stoklossa, C.; Atwal, S. Nutrition care for patients with weight regain after bariatric surgery. Gastroenterol. Res. Pract. 2013, 2013, 256145. [Google Scholar] [CrossRef] [PubMed]
- Henfridsson, P.; Laurenius, A.; Wallengren, O.; Beamish, A.J.; Dahlgren, J.; Flodmark, C.-E.; Marcus, C.; Olbers, T.; Gronowitz, E.; Ellegard, L. Micronutrient intake and biochemistry in adolescents adherent or nonadherent to supplements 5 years after Roux-en-Y gastric bypass surgery. Surg. Obes. Relat. Dis. 2019, 15, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Inge, T.H.; Courcoulas, A.P.; Jenkins, T.M.; Michalsky, M.P.; Helmrath, M.A.; Brandt, M.L.; Harmon, C.M.; Zeller, M.H.; Chen, M.K.; Xanthakos, S.A.; et al. Weight Loss and Health Status 3 Years after Bariatric Surgery in Adolescents. N. Engl. J. Med. 2016, 374, 113–123. [Google Scholar] [CrossRef]
- Gonzalez-Gross, M.; Valtuena, J.; Breidenassel, C.; Moreno, L.A.; Ferrari, M.; Kersting, M.; De Henauw, S.; Gottrand, F.; Azzini, E.; Widhalm, K.; et al. Vitamin D status among adolescents in Europe: The Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2012, 107, 755–764. [Google Scholar] [CrossRef]
- Fiamenghi, V.I.; Mello, E.D. Vitamin D deficiency in children and adolescents with obesity: A meta-analysis. J. Pediatr. 2020, 97, 273–279. [Google Scholar] [CrossRef]
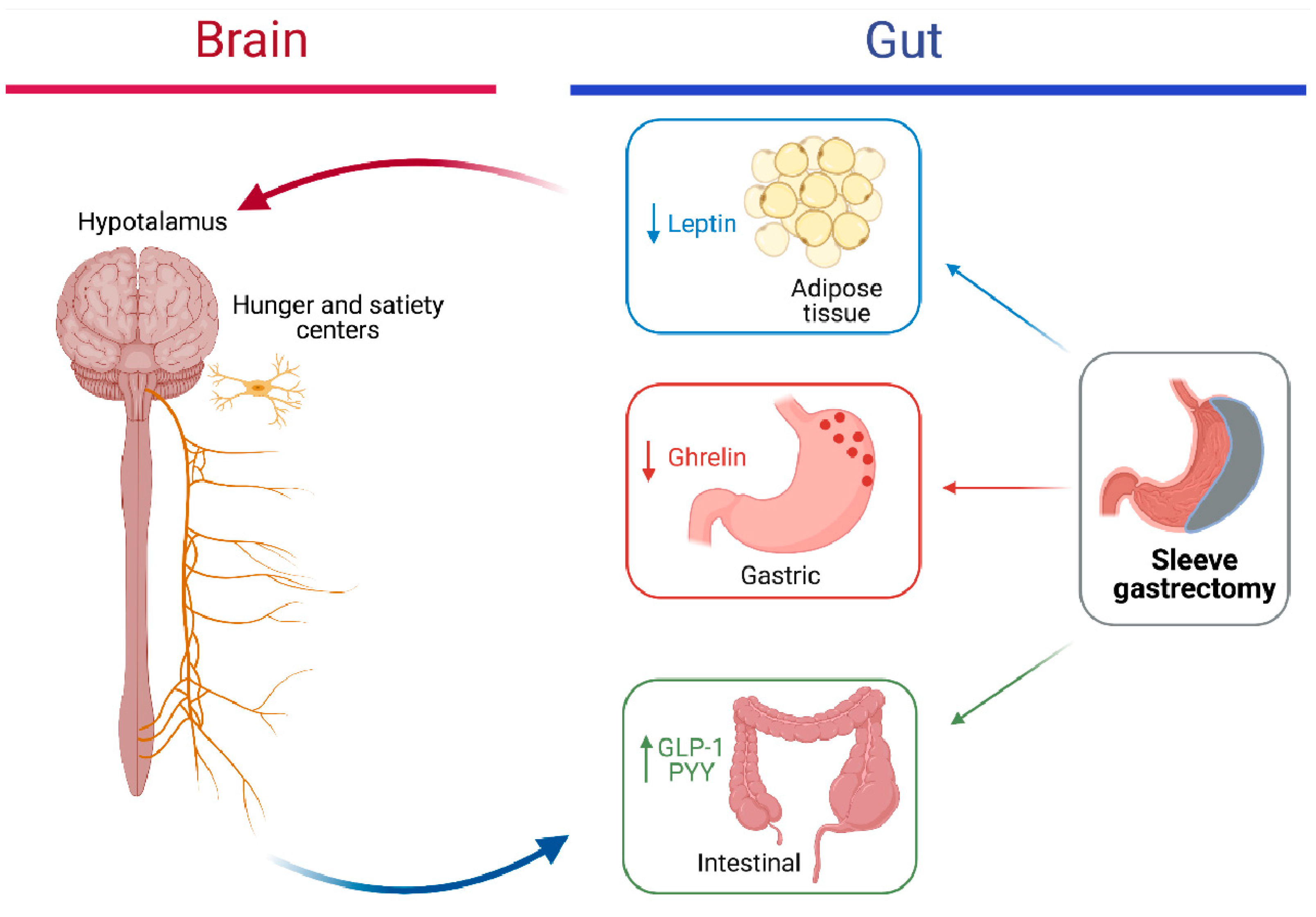
- Mans, E.; Serra-Prat, M.; Palomera, E.; Suñol, X.; Clavé, P. Sleeve gastrectomy effects on hunger, satiation, and gastrointestinal hormone and motility responses after a liquid meal test. Am. J. Clin. Nutr. 2015, 102, 540–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, Y.; Kim, H.J.; Lo Menzo, E.; Park, S.; Szomstein, S.; Rosenthal, R.J. Anemia, iron and vitamin B12 deficiencies after sleeve gastrectomy compared to Roux-en-Y gastric bypass: A meta-analysis. Surg. Obes. Relat. Dis. 2014, 10, 589–597. [Google Scholar] [CrossRef]
- Ruiz-Cota, P.; Bacardí-Gascón, M.; Jiménez-Cruz, A. Long-term outcomes of metabolic and bariatric surgery in adolescents with severe obesity with a follow-up of at least 5 years: A systematic review. Surg. Obes. Relat. Dis. 2019, 15, 133–144. [Google Scholar] [CrossRef]
- Goldberg, H.R.; Chin, V.L.; Zitsman, J.L.; Zhang, C.; Williams, K.M.; Oberfield, S.; Fennoy, I. Bariatric Surgery in Adolescents: Is Routine Nutrient Supplementation Sufficient to Avoid Anemia Following Bariatric Surgery? Nutr. Clin. Pract. 2017, 32, 502–507. [Google Scholar] [CrossRef]
- Elhag, W.; El Ansari, W.; Abdulrazzaq, S.; Abdullah, A.; Elsherif, M.; Elgenaied, I. Evolution of 29 Anthropometric, Nutritional, and Cardiometabolic Parameters Among Morbidly Obese Adolescents 2 Years Post Sleeve Gastrectomy. Obes. Surg. 2018, 28, 474–482. [Google Scholar] [CrossRef]
- Stein, J.; Stier, C.; Raab, H.; Weiner, R. Review article: The nutritional and pharmacological consequences of obesity surgery. Aliment. Pharmacol. Ther. 2014, 40, 582–609. [Google Scholar] [CrossRef]
- Sherf Dagan, S.; Tovim, T.B.; Keidar, A.; Raziel, A.; Shibolet, O.; Zelber-Sagi, S. Inadequate protein intake after laparoscopic sleeve gastrectomy surgery is associated with a greater fat free mass loss. Surg. Obes. Relat. Dis. 2017, 13, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Oudman, E.; Wijnia, J.W.; van Dam, M.; Biter, L.U.; Postma, A. Preventing Wernicke Encephalopathy After Bariatric Surgery. Obes. Surg. 2018, 28, 2060–2068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitfield, K.C.; Bourassa, M.W.; Adamolekun, B.; Bergeron, G.; Bettendorff, L.; Brown, K.H.; Cox, L.; Fattal-Valevski, A.; Fischer, P.R.; Frank, E.L.; et al. Thiamine deficiency disorders: Diagnosis, prevalence, and a roadmap for global control programs. Ann. N. Y. Acad. Sci. 2018, 1430, 3–43. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Alsulaim, H.A.; Canner, J.K.; Prokopowicz, G.P.; Steele, K.E. Prevalence and predictors of postoperative thiamine deficiency after vertical sleeve gastrectomy. Surg. Obes. Relat. Dis. 2018, 14, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Sugerman, H.J.; Sugerman, E.L.; DeMaria, E.J.; Kellum, J.M.; Kennedy, C.; Mowery, Y.; Wolfe, L.G. Bariatric surgery for severely obese adolescents. J. Gastrointest. Surg. 2003, 7, 102–108. [Google Scholar] [CrossRef]
- Black, J.A.; White, B.; Viner, R.M.; Simmons, R.K. Bariatric surgery for obese children and adolescents: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 634–644. [Google Scholar] [CrossRef]
- Ells, L.J.; Mead, E.; Atkinson, G.; Corpeleijn, E.; Roberts, K.; Viner, R.; Baur, L.; Metzendorf, M.I.; Richter, B. Surgery for the treatment of obesity in children and adolescents. Cochrane Database Syst. Rev. 2015, 6, CD011740. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, P.E.; Sawyer, S.M.; Laurie, C.; Brown, W.A.; Skinner, S.; Veit, F.; Paul, E.; Burton, P.R.; McGrice, M.; Anderson, M.; et al. Laparoscopic adjustable gastric banding in severely obese adolescents: A randomized trial. JAMA 2010, 303, 519–526. [Google Scholar] [CrossRef] [Green Version]
- Roberts, C.A. Physical and Psychological Effects of Bariatric Surgery on Obese Adolescents: A Review. Front. Pediatr. 2021, 8, 591598. [Google Scholar] [CrossRef]
- Thomas, S.; Schauer, P. Bariatric surgery and the gut hormone response. Nutr. Clin. Pract. 2010, 25, 175–182. [Google Scholar] [CrossRef]
- Sjöström, L.; Peltonen, M.; Jacobson, P.; Ahlin, S.; Andersson-Assarsson, J.; Anveden, Å.; Bouchard, C.; Carlsson, B.; Karason, K.; Lönroth, H.; et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA 2014, 311, 2297–2304. [Google Scholar] [CrossRef] [Green Version]
- Pareek, M.; Schauer, P.R.; Kaplan, L.M.; Leiter, L.A.; Rubino, F.; Bhatt, D.L. Metabolic Surgery: Weight Loss, Diabetes, and Beyond. J. Am. Coll. Cardiol. 2018, 71, 670–687. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M. Peripheral mechanisms in appetite regulation. Gastroenterology 2015, 148, 1219–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karamanakos, S.N.; Vagenas, K.; Kalfarentzos, F.; Alexandrides, T.K. Weight loss, appetite suppression, and changes in fasting and postprandial ghrelin and peptide-YY levels after Roux-en-Y gastric bypass and sleeve gastrectomy: A prospective, double blind study. Ann. Surg. 2008, 247, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-T.; Lu, Q.-C.; Wang, Q.; Wang, R.-C.; Zhang, Y.; Chen, H.-L.; Zhao, H.; Qian, H.-X. Role of the duodenum in regulation of plasma ghrelin levels and body mass index after subtotal gastrectomy. World J. Gastroenterol. 2008, 14, 2425–2429. [Google Scholar] [CrossRef] [PubMed]
- Kojima, S.; Ueno, N.; Asakawa, A.; Sagiyama, K.; Naruo, T.; Mizuno, S.; Inui, A. A role for pancreatic polypeptide in feeding and body weight regulation. Peptides 2007, 28, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Ramón, J.M.; Salvans, S.; Crous, X.; Puig, S.; Goday, A.; Benaiges, D.; Trillo, L.; Pera, M.; Grande, L. Effect of Roux-en-Y gastric bypass vs. sleeve gastrectomy on glucose and gut hormones: A prospective randomised trial. J. Gastrointest. Surg. 2012, 16, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Rehfeld, J.F. Incretin physiology beyond glucagon-like peptide 1 and glucose-dependent insulinotropic polypeptide: Cholecystokinin and gastrin peptides. Acta Physiol. 2011, 201, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, K.C. Gut hormones in gastric function. Bailliere Clin. Endocrinol. Metab. 1994, 8, 111–136. [Google Scholar] [CrossRef]
- Schrumpf, E.; Giercksky, K.E.; Nygaard, K.; Fausa, O. Gastrin secretion before and after gastric bypass surgery for morbid obesity. Scand. J. Gastroenterol. 1981, 16, 721–725. [Google Scholar] [CrossRef]
- Ferzli, G.S.; Dominique, E.; Ciaglia, M.; Bluth, M.H.; Gonzalez, A.; Fingerhut, A. Clinical improvement after duodenojejunal bypass for non-obese type 2 diabetes despite minimal improvement in glycemic homeostasis. World J. Surg. 2009, 33, 972–979. [Google Scholar] [CrossRef]
- Chambers, A.P.; Smith, E.P.; Begg, D.P.; Grayson, B.E.; Sisley, S.; Greer, T.; Sorrell, J.; Lemmen, L.; LaSance, K. Regulation of gastric emptying rate and its role in nutrient-induced GLP-1 secretion in rats after vertical sleeve gastrectomy. Am. J. Physiol. Endocrinol. Metab. 2014, 306, E424–E432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jimenez, A.; Casamitjana, R.; Viaplana-Masclans, J.; Lacy, A.; Vidal, J. GLP-1 action and glucose tolerance in subjects with remission of type 2 diabetes after gastric bypass surgery. Diabetes Care 2013, 36, 2062–2069. [Google Scholar] [CrossRef] [Green Version]
- Jimenez, A.; Mari, A.; Casamitjana, R.; Lacy, A.; Ferrannini, E.; Vidal, J. GLP-1 and glucose tolerance after sleeve gastrectomy in morbidly obese subjects with type 2 diabetes. Diabetes 2014, 63, 3372–3377. [Google Scholar] [CrossRef] [Green Version]
- Tsoli, M.; Chronaiou, A.; Kehagias, I.; Kalfarentzos, F.; Alexandrides, T.K. Hormone changes and diabetes resolution after biliopancreatic diversion and laparoscopic sleeve gastrectomy: A comparative prospective study. Surg. Obes. Relat. Dis. 2013, 9, 667–677. [Google Scholar] [CrossRef]
- Boggiano, M.M.; Chandler, P.C.; Oswald, K.D.; Rodgers, R.J.; Blundell, J.E.; Ishii, Y.; Beattie, A.H.; Holc, P.; Allison, D.B.; Schindler, M.; et al. PYY3-36 as an anti-obesity drug target. Obes. Rev. 2005, 6, 307–322. [Google Scholar] [CrossRef] [PubMed]
- Olivan, B.; Teixeira, J.; Bose, M.; Bawa, B.; Chang, T.; Summe, H.; Lee, H.; Laferrere, B. Effect of weight loss by diet or gastric bypass surgery on peptide YY3-36 levels. Ann. Surg. 2009, 249, 948–953. [Google Scholar] [CrossRef] [Green Version]
- Neary, M.T.; Batterham, R.L. Gut hormones: Implications for the treatment of obesity. Pharmacol. Ther. 2009, 124, 44–56. [Google Scholar] [CrossRef]
- Foschi, D.; Corsi, F.; Pisoni, L.; Vago, T.; Bevilacqua, M.; Asti, E.; Righi, I.; Trabucchi, E. Plasma cholecystokinin levels after vertical banded gastroplasty: Effects of an acidified meal. Obes. Surg. 2004, 14, 644–647. [Google Scholar] [CrossRef]
- Naslund, E.; Gryback, P.; Hellstrom, P.M.; Jacobsson, H.; Holst, J.J.; Theodorsson, E.; Backman, L. Gastrointestinal hormones and gastric emptying 20 years after jejunoileal bypass for massive obesity. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 387–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterli, R.; Steinert, R.E.; Woelnerhanssen, B.; Peters, T.; Christoffel-Courtin, C.; Gass, M.; Kern, B.; von Fluee, M.; Beglinger, C. Metabolic and hormonal changes after laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy: A randomized, prospective trial. Obes. Surg. 2012, 22, 740–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calcaterra, V.; Cena, H.; Fonte, M.L.; De Amici, M.; Vandoni, M.; Albanesi, M.; Pelizzo, G. Long-term Outcome after Robotic-assisted Gastroplication in Adolescents: Hunger Hormone and Food Preference Changes Two Case Reports. J. Clin. Res. Pediatr. Endocrinol. 2016, 8, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Cavin, J.B.; Couvelard, A.; Lebtahi, R.; Ducroc, R.; Arapis, K.; Voitellier, E.; Cluzeaud, F.; Gillard, L.; Hourseau, M.; Mikail, N.; et al. Differences in Alimentary Glucose Absorption and Intestinal Disposal of Blood Glucose After Roux-en-Y Gastric Bypass vs. Sleeve Gastrectomy. Gastroenterology 2016, 150, 454–464. [Google Scholar] [CrossRef] [Green Version]
- Inabnet, W.B.; Winegar, D.A.; Sherif, B.; Sarr, M.G. Early outcomes of bariatric surgery in patients with metabolic syndrome: An analysis of the bariatric outcomes longitudinal database. J. Am. Coll. Surg. 2012, 214, 550–556. [Google Scholar] [CrossRef]
- Schauer, P.R.; Bhatt, D.L.; Kirwan, J.P.; Wolski, K.; Brethauer, S.A.; Navaneethan, S.D.; Aminian, A.; Pothier, C.E.; Kim, E.S.; Nissen, S.E.; et al. STAMPEDE Investigators. Bariatric surgery versus intensive medical therapy for diabetes—3-year outcomes. N. Engl. J. Med. 2014, 370, 2002–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bueter, M.; Dubb, S.S.; Gill, A.; Joannou, L.; Ahmed, A.; Frankel, A.H.; Tam, F.W.; le Roux, C.W. Renal cytokines improve early after bariatric surgery. Br. J. Surg. 2010, 97, 1838–1844. [Google Scholar] [CrossRef]
- Viana, E.C.; Araujo-Dasilio, K.L.; Miguel, G.P.; Bressan, J.; Lemos, E.M.; Moyses, M.R.; de Abreu, G.R.; de Azevedo, J.L.; Carvalho, P.S.; Passos-Bueno, M.R.; et al. Gastric bypass and sleeve gastrectomy: The same impact on IL-6 and TNF-α. Prospective clinical trial. Obes. Surg. 2013, 23, 1252–1261. [Google Scholar] [CrossRef]
- Ay, L.; Kopp, H.P.; Brix, J.M.; Ay, C.; Quehenberger, P.; Schernthaner, G.H.; Pabinger, I.; Schernthaner, G. Thrombin generation in morbid obesity: Significant reduction after weight loss. J. Thromb. Haemost. 2010, 8, 759–765. [Google Scholar] [CrossRef]
- Blanco, D.G.; Funes, D.R.; Giambartolomei, G.; Lo Menzo, E.; Szomstein, S.; Rosenthal, R.J. Laparoscopic sleeve gastrectomy versus Roux-en-Y gastric bypass in cardiovascular risk reduction: A match control study. Surg. Obes. Relat. Dis. 2019, 15, 14–20. [Google Scholar] [CrossRef]
- Praveen Raj, P.; Gomes, R.M.; Kumar, S.; Senthilnathan, P.; Karthikeyan, P.; Shankar, A.; Palanivelu, C. The effect of surgically induced weight loss on nonalcoholic fatty liver disease in morbidly obese Indians: "NASHOST" prospective observational trial. Surg. Obes. Relat. Dis. 2015, 11, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Gumbau, V.; Bruna, M.; Canelles, E.; Guaita, M.; Mulas, C.; Basés, C.; Celma, I.; Puche, J.; Marcaida, G.; Oviedo, M.; et al. A prospective study on inflammatory parameters in obese patients after sleeve gastrectomy. Obes. Surg. 2014, 24, 903–908. [Google Scholar] [CrossRef]
- Michalsky, M.P.; Inge, T.H.; Jenkins, T.M.; Xie, C.; Courcoulas, A.; Helmrath, M.; Brandt, M.L.; Harmon, C.M.; Chen, M.; Dixon, J.B.; et al. Cardiovascular risk factors after adolescent bariatric surgery. Pediatrics 2018, 141, e20172485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalewski, P.K.; Olszewski, R.; Waledziak, M.S.; Maciej, S.; Janik, M.R.; Kwiatkowski, A.; Gałązka-Świderek, N.; Cichoń, K.; Brągoszewski, J.; Paśnik, K. Long-term outcomes of laparoscopic sleeve gastrectomy: A single-center, retrospective study. Obes. Surg. 2018, 28, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Braghetto, I.; Korn, O.; Burgos, A.; Figueroa, M. When should be converted laparoscopic sleeve gastrectomy to laparoscopic roux-en-y gastric bypass due to gastroesophageal reflux? ABCD Arq. Bras. Cir. Dig. 2021, 33, e1553. [Google Scholar] [CrossRef]
- Palma Dos Reis, C.R.; Serrano, F.; Fonseca, M.J.; Martins, A.T.; Campos, A.; McMahon, G.M.; Barros, H. The fetal origins of disease: A prospective cohort study on the association of preeclampsia and childhood obesity. J. Dev. Orig. Health Dis. 2021, 2, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.M. Current Issues in Bariatric Surgery for Adolescents with Severe Obesity: Durability, Complications, and Timing of Intervention. J. Obes. Metab. Syndr. 2020, 29, 4–11. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Cardiovascular Hypertension Dyslipidemia | Endocrinology Type II Diabetes Mellitus Precocious puberty Insulin resistance PCOS Menstrual irregularities |
| Gastrointestinal Gastroesophageal reflux disease Gallstones Non-alcoholic fatty liver disease | Orthopedics Slipped capital femoral epiphysis Ankle sprains Blount’s disease Arthritis Join pain Tibia vara Flat feet |
| Neurological Pseudotumor cerebri Headache | Renal Glomerulonephritis Nephrotic Syndrome |
| Respiratory Asthma Obstructive sleep apnea | Dermatological Acanthosis Nigricans Striae Hidradenitis Suppurativa |
| Psychological Depression Anxiety Poor-self-Esteem Poor Body Image Eating disorder Sleep Disturbance |
| International Diabetes Federation | IDEFICS Study | Cook et al. | de Ferranti et al. |
|---|---|---|---|
Waist circumference ≥90th percentile for age and sex associated with at least 2 of the following:
| ≥3 of the 4 following criteria:
| ≥3 of the 5 criteria below:
| ≥3 of the 5 criteria below:
|
| General Complications | Insufficient Weight Loss and Weight Regain |
|---|---|
| Surgical complications (mostly minor complications) | Acute post-operative
|
| Nutritional risks | Micronutrient deficiencies
Adverse bone density and bone microarchitectural changes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calcaterra, V.; Cena, H.; Pelizzo, G.; Porri, D.; Regalbuto, C.; Vinci, F.; Destro, F.; Vestri, E.; Verduci, E.; Bosetti, A.; et al. Bariatric Surgery in Adolescents: To Do or Not to Do? Children 2021, 8, 453. https://doi.org/10.3390/children8060453
Calcaterra V, Cena H, Pelizzo G, Porri D, Regalbuto C, Vinci F, Destro F, Vestri E, Verduci E, Bosetti A, et al. Bariatric Surgery in Adolescents: To Do or Not to Do? Children. 2021; 8(6):453. https://doi.org/10.3390/children8060453
Chicago/Turabian StyleCalcaterra, Valeria, Hellas Cena, Gloria Pelizzo, Debora Porri, Corrado Regalbuto, Federica Vinci, Francesca Destro, Elettra Vestri, Elvira Verduci, Alessandra Bosetti, and et al. 2021. "Bariatric Surgery in Adolescents: To Do or Not to Do?" Children 8, no. 6: 453. https://doi.org/10.3390/children8060453