
Children’s Beliefs about Pain: An Exploratory Analysis

 , and
, and
Abstract
:
1. Introduction
1.1. Explanatory Styles
1.2. Current Study
1.3. Objectives
2. Materials and Methods
2.1. Overview
2.2. Recruitment
2.3. Assessments
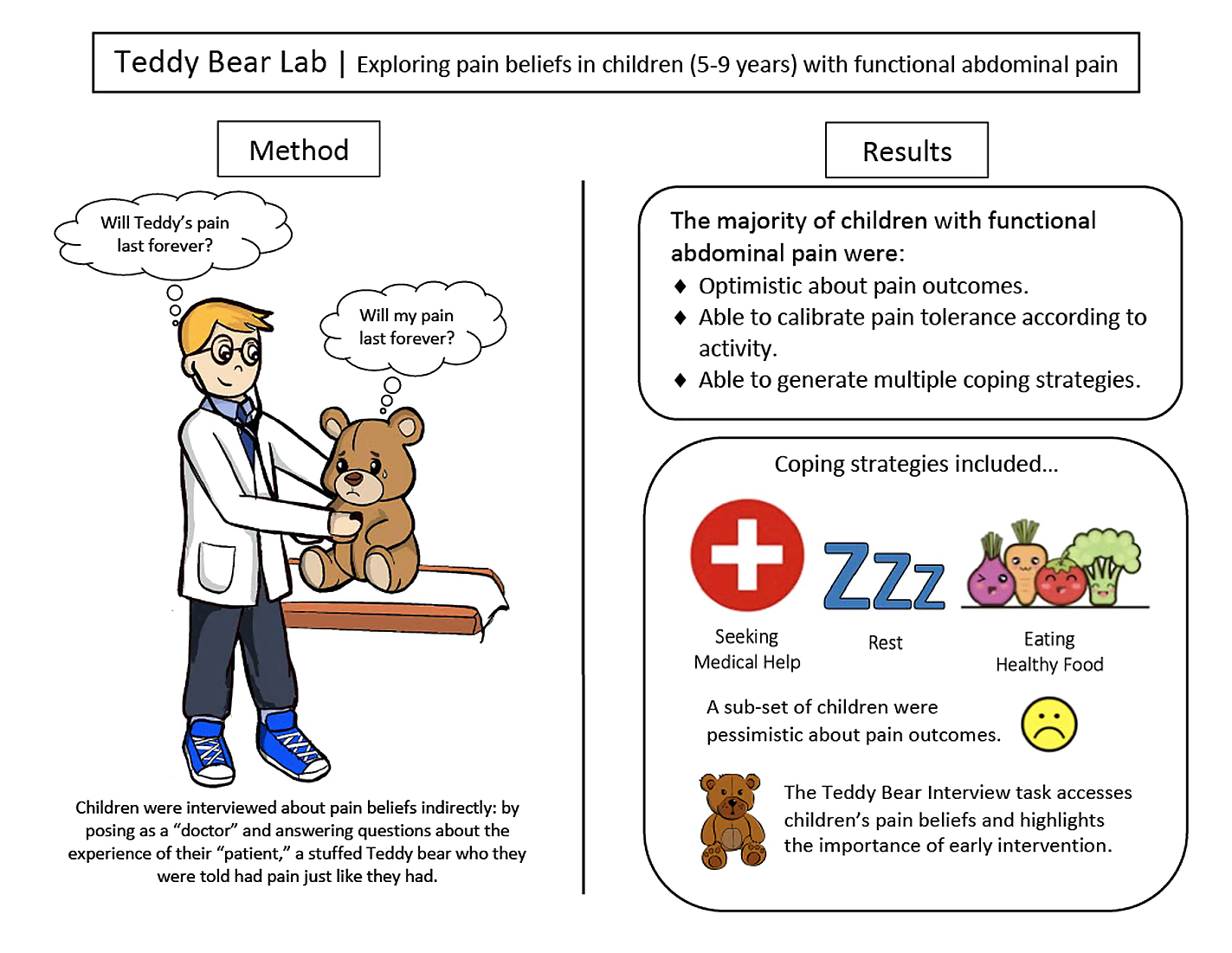
2.3.1. Teddy Bear Pain Interview
2.3.2. Tolerance of Pain in Diverse Contexts
2.3.3. Preschool Age Psychiatric Assessment (PAPA) Interview
2.3.4. Pain Diaries
2.3.5. Anxiety and Depressive Symptoms
2.4. Data Analysis
2.4.1. Quantitative
2.4.2. Qualitative
3. Results
3.1. Demographic Information of Teddy Bear Interview Sample
3.2. Baseline Beliefs by Age
3.3. Tolerance of Pain in Diverse Contexts
3.4. Associations with Pain
3.5. Qualitative Results
3.5.1. Pain Reduction Strategies
3.5.2. Pain Interference
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Can you point to Teddy’s pain?

- 2.
- How is Teddy feeling when he’s in pain?

- 3.
- Can you think of ways to make Teddy’s pain better?
- 4.
- Teddy has pain just like you. Point to the Teddy that shows how strong or weak you think Teddy is, compared to other Teddys.

- 5.
- Do you think Teddy will have the pain forever?
- 6.
- Do you think the pain will bother Teddy forever?
- 7.
- Do you think Teddy will get better at dealing with the pain?
- 8.
- When Teddy is a year older, how do you think Teddy will be feeling?
- 9.
- Does Teddy’s tummy pain cause problems at home?
- 10.
- Does Teddy’s tummy pain cause problems at school?
- 11.
- Does Teddy’s tummy pain stop him from having fun most of the time?
- 12.
- What kinds of things can Teddy still do, even when he is in pain? Do you think Teddy can still go to school with Tummy pain?
- 13.
- What is the most pain that Teddy can have and still go to school?

- 14.
- When Teddy goes to school with tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 15.
- Do you think Teddy can still play a favorite sport with tummy pain?
- 16.
- What is the most pain that Teddy can have and still play a favorite sport?

- 17.
- When Teddy plays a favorite sport with tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 18.
- Do you think Teddy can still play with a friend with tummy pain?
- 19.
- What is the most pain that Teddy can have and still play with friends?

- 20.
- When Teddy plays with his friends when he has tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 21.
- Do you think Teddy can still watch TV with tummy pain?
- 22.
- What is the most pain that Teddy can have and still watch TV?

- 23.
- When Teddy watches TV when he has tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 24.
- Do you think Teddy can still read a book with tummy pain?
- 25.
- What is the most pain that Teddy can have and still read a book?

- 26.
- When Teddy reads a book when he has tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 27.
- Do you think Teddy can still eat a favorite food with tummy pain?
- 28.
- What is the most pain that Teddy can have and still eat a favorite food?

- 29.
- When Teddy eats his favorite food with tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 30.
- Do you think Teddy can still eat a healthy food with tummy pain?
- 31.
- What is the most pain that Teddy can have and still eat a healthy food?

- 32.
- When Teddy eats a healthy food with tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 33.
- Can you think of another activity that Teddy’s pain gets in the way of?
- 34.
- Do you think Teddy can still do this activity with tummy pain?
- 35.
- What is the most pain that Teddy can have and still do this activity?

- 36.
- When Teddy does this activity with tummy pain, do you think he is weak, a little weak, in the middle, a little strong, or strong?

- 37.
- Is there anything else that is important for us to know about Teddy’s pain?
References
- Korterink, J.J.; Diederen, K.; Benninga, M.A.; Tabbers, M.M. Epidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-Analysis. PLoS ONE 2015, 10, e0126982. [Google Scholar] [CrossRef] [Green Version]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2016, 150, 1456–1468.e2. [Google Scholar] [CrossRef]
- Rasquin, A.; Di Lorenzo, C.; Forbes, D.; Guiraldes, E.; Hyams, J.S.; Staiano, A.; Walker, L.S. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2006, 130, 1527–1537. [Google Scholar] [CrossRef] [PubMed]
- Hotopf, M.; Carr, S.; Mayou, R.; Wadsworth, M.; Wessely, S. Why Do Children Have Chronic Abdominal Pain, and What Happens to Them When They Grow up? Population Based Cohort Study. BMJ 1998, 316, 1196–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelby, G.D.; Shirkey, K.C.; Sherman, A.L.; Beck, J.E.; Haman, K.; Shears, A.R.; Horst, S.N.; Smith, C.A.; Garber, J.; Walker, L.S. Functional Abdominal Pain in Childhood and Long-Term Vulnerability to Anxiety Disorders. Pediatrics 2013, 132, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, K.; Pearson, R.M.; Stein, A.; Fazel, M. The Predictive Value of Childhood Recurrent Abdominal Pain for Adult Emotional Disorders, and the Influence of Negative Cognitive Style. Findings from a Cohort Study. PLoS ONE 2017, 12, e0185643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Gontard, A.; Moritz, A.-M.; Thome-Granz, S.; Equit, M. Abdominal Pain Symptoms Are Associated with Anxiety and Depression in Young Children. Acta Paediatr. 2015, 104, 1156–1163. [Google Scholar] [CrossRef]
- Sweeney, P.D.; Anderson, K.; Bailey, S. Attributional Style in Depression: A Meta-Analytic Review. J. Personal. Soc. Psychol. 1986, 50, 974–991. [Google Scholar] [CrossRef]
- Ramchandani, P.G.; Fazel, M.; Stein, A.; Wiles, N.; Hotopf, M. The Impact of Recurrent Abdominal Pain: Predictors of Outcome in a Large Population Cohort. Acta Paediatr. 2007, 96, 697–701. [Google Scholar] [CrossRef]
- Abbott, R.A.; Martin, A.E.; Newlove-Delgado, T.V.; Bethel, A.; Whear, R.S.; Coon, J.T.; Logan, S. Recurrent Abdominal Pain in Children: Summary Evidence From 3 Systematic Reviews of Treatment Effectiveness. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.L.; van Tilburg, M.A.L. Functional Abdominal Pain in Childhood: Background Studies and Recent Research Trends. Pain Res. Manag. 2012, 17, 413–417. [Google Scholar] [CrossRef]
- Ramchandani, P.G.; Hotopf, M.; Sandhu, B.; Stein, A. The Epidemiology of Recurrent Abdominal Pain from 2 to 6 Years of Age: Results of a Large, Population-Based Study. Pediatrics 2005, 116, 46–50. [Google Scholar] [CrossRef]
- Birnie, K.A.; Ouellette, C.; Amaral, T.D.; Stinson, J.N. Mapping the Evidence and Gaps of Interventions for Pediatric Chronic Pain to Inform Policy, Research, and Practice: A Systematic Review and Quality Assessment of Systematic Reviews. Can. J. Pain 2020, 4, 129–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprenger, L.; Gerhards, F.; Goldbeck, L. Effects of Psychological Treatment on Recurrent Abdominal Pain in Children—A Meta-Analysis. Clin. Psychol. Rev. 2011, 31, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.L.; Langer, S.L.; Walker, L.S.; Romano, J.M.; Christie, D.L.; Youssef, N.; DuPen, M.M.; Feld, A.D.; Ballard, S.A.; Welsh, E.M.; et al. Cognitive-Behavioral Therapy for Children With Functional Abdominal Pain and Their Parents Decreases Pain and Other Symptoms. Am. J. Gastroenterol. 2010, 105, 946–956. [Google Scholar] [CrossRef] [Green Version]
- Groß, M.; Warschburger, P. Evaluation of a Cognitive–Behavioral Pain Management Program for Children with Chronic Abdominal Pain: A Randomized Controlled Study. Int. J. Behav. Med. 2013, 20, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Palermo, T.M.; Wilson, A.C.; Peters, M.; Lewandowski, A.; Somhegyi, H. Randomized Controlled Trial of an Internet-Delivered Family Cognitive–Behavioral Therapy Intervention for Children and Adolescents with Chronic Pain. Pain 2009, 146, 205–213. [Google Scholar] [CrossRef]
- Sanders, M.; Rebgetz, M.; Morrison, M.; Bor, W.; Gordon, A.; Dadds, M.; Shepherd, R. Cognitive-Behavioral Treatment of Recurrent Nonspecific Abdominal-Pain. J. Consult. Clin. Psychol. 1989, 57, 294–300. [Google Scholar] [CrossRef]
- Sanders, M.; Shepherd, R.; Cleghorn, G.; Woolford, H. The Treatment of Recurrent Abdominal-Pain in Children—A Controlled Comparison of Cognitive-Behavioral Family Intervention and Standard Pediatric Care. J. Consult. Clin. Psychol. 1994, 62, 306–314. [Google Scholar] [CrossRef]
- van der Veek, S.M.C.; Derkx, B.H.F.; Benninga, M.A.; Boer, F.; de Haan, E. Cognitive Behavior Therapy for Pediatric Functional Abdominal Pain: A Randomized Controlled Trial. Pediatrics 2013, 132, e1163–e1172. [Google Scholar] [CrossRef] [Green Version]
- Koopman, H.M.; Baars, R.M.; Chaplin, J.; Zwinderman, K.H. Illness through the Eyes of the Child: The Development of Children’s Understanding of the Causes of Illness. Patient Educ. Couns. 2004, 55, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S.; Girgus, J.S.; Seligman, M.E. Learned Helplessness in Children: A Longitudinal Study of Depression, Achievement, and Explanatory Style. J. Personal. Soc. Psychol. 1986, 51, 435–442. [Google Scholar] [CrossRef]
- Hietanen, J.K.; Glerean, E.; Hari, R.; Nummenmaa, L. Bodily Maps of Emotions across Child Development. Dev. Sci. 2016, 19, 1111–1118. [Google Scholar] [CrossRef]
- Zucker, N.; Mauro, C.; Craske, M.; Wagner, H.R.; Datta, N.; Hopkins, H.; Caldwell, K.; Kiridly, A.; Marsan, S.; Maslow, G.; et al. Acceptance-Based Interoceptive Exposure for Young Children with Functional Abdominal Pain. Behav. Res. Ther. 2017, 97, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.L.; Langer, S.L.; Walker, L.S.; Feld, L.D.; Whitehead, W.E. Relationship Between the Decision to Take a Child to the Clinic for Abdominal Pain and Maternal Psychological Distress. Arch. Pediatr. Adolesc. Med. 2006, 160, 961–965. [Google Scholar] [CrossRef] [Green Version]
- Walker, L.S.; Baber, K.F.; Garber, J.; Smith, C.A. A Typology of Pain Coping Strategies in Pediatric Patients with Chronic Abdominal Pain. Pain 2008, 137, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Langer, S.L.; Romano, J.M.; Levy, R.L.; Walker, L.S.; Whitehead, W.E. Catastrophizing and Parental Response to Child Symptom Complaints. Child. Health Care 2009, 38, 169–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miró, J.; Huguet, A.; Jensen, M.P. Pain Beliefs Predict Pain Intensity and Pain Status in Children: Usefulness of the Pediatric Version of the Survey of Pain Attitudes. Pain Med. 2014, 15, 887–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, A.L.; Walker, L.S.; Laird, K.T.; Shirkey, K.C.; Smith, C.A. Pediatric Pain Beliefs Questionnaire: Psychometric Properties of the Short Form. J. Pain 2016, 17, 1036–1044. [Google Scholar] [CrossRef] [Green Version]
- Walker, L.S.; Smith, C.A.; Garber, J.; Van Slyke, D.A. Development and Validation of the Pain Response Inventory for Children. Psychol. Assess. 1997, 9, 392–405. [Google Scholar] [CrossRef]
- De Los Reyes, A.; Augenstein, T.M.; Wang, M.; Thomas, S.A.; Drabick, D.A.G.; Burgers, D.E.; Rabinowitz, J. The Validity of the Multi-Informant Approach to Assessing Child and Adolescent Mental Health. Psychol. Bull. 2015, 141, 858–900. [Google Scholar] [CrossRef]
- Bloch, Y.H.; Toker, A. Doctor, Is My Teddy Bear Okay? The “Teddy Bear Hospital” as a Method to Reduce Children’s Fear of Hospitalization. Isr. Med. Assoc. J. 2008, 10, 597. [Google Scholar]
- Leonhardt, C.; Margraf-Stiksrud, J.; Badners, L.; Szerencsi, A.; Maier, R.F. Does the ‘Teddy Bear Hospital’ Enhance Preschool Children’s Knowledge? A Pilot Study with a Pre/Post-Case Control Design in Germany. J. Health Psychol. 2014, 19, 1250–1260. [Google Scholar] [CrossRef]
- Jebb, A.T.; Parrigon, S.; Woo, S.E. Exploratory Data Analysis as a Foundation of Inductive Research. Hum. Resour. Manag. Rev. 2017, 27, 265–276. [Google Scholar] [CrossRef]
- Drossman, D.A. The Functional Gastrointestinal Disorders and the Rome III Process. Gastroenterology 2006, 130, 1377–1390. [Google Scholar] [CrossRef]
- Herr, K.; Spratt, K.F.; Garand, L.; Li, L. Evaluation of the Iowa Pain Thermometer and Other Selected Pain Intensity Scales in Younger and Older Adult Cohorts Using Controlled Clinical Pain: A Preliminary Study. Pain Med. 2007, 8, 585–600. [Google Scholar] [CrossRef] [PubMed]
- Egger, H.L.; Angold, A. The Preschool Age Psychiatric Assessment (PAPA): A Structured Parent Interview for Diagnosing Psychiatric Disorders in Preschool Children. In Handbook of Infant, Toddler, and Preschool Mental Health Assessment; Oxford University Press: New York, NY, USA, 2004; pp. 223–243. ISBN 978-0-19-514438-3. [Google Scholar]
- Egger, H.L.; Erkanli, A.; Keeler, G.; Potts, E.; Walter, B.K.; Angold, A. Test-Retest Reliability of the Preschool Age Psychiatric Assessment (PAPA). J. Am. Acad. Child. Adolesc. Psychiatry 2006, 45, 538–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zucker, N.; Copeland, W.; Franz, L.; Carpenter, K.; Keeling, L.; Angold, A.; Egger, H. Psychological and Psychosocial Impairment in Preschoolers With Selective Eating. Pediatrics 2015, 136, e582–e590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, D.E.; Gross, H.E.; Stucky, B.D.; Thissen, D.; DeWitt, E.M.; Lai, J.S.; Amtmann, D.; Khastou, L.; Varni, J.W.; DeWalt, D.A. Development of Six PROMIS Pediatrics Proxy-Report Item Banks. Health Qual. Life Outcomes 2012, 10, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL: Measurement Model for the Pediatric Quality of Life Inventory. Med. Care 1999, 37, 126–139. [Google Scholar] [CrossRef]
- Kashikar-Zuck, S.; Carle, A.; Barnett, K.; Goldschneider, K.R.; Sherry, D.D.; Mara, C.A.; Cunningham, N.; Farrell, J.; Tress, J.; DeWitt, E.M. Longitudinal Evaluation of Patient Reported Outcomes Measurement Information Systems (PROMIS) Measures in Pediatric Chronic Pain. Pain 2016, 157, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, M. The Children’s Depression, Inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar] [PubMed]
- Varni, J.W.; Thissen, D.; Stucky, B.D.; Liu, Y.; Gorder, H.; Irwin, D.E.; DeWitt, E.M.; Lai, J.-S.; Amtmann, D.; DeWalt, D.A. PROMIS® Parent Proxy Report Scales: An Item Response Theory Analysis of the Parent Proxy Report Item Banks. Qual. Life Res. 2012, 21, 1223–1240. [Google Scholar] [CrossRef] [Green Version]
- Pope, C.; Ziebland, S.; Mays, N. Analysing Qualitative Data. BMJ 2000, 320, 114–116. [Google Scholar] [CrossRef]
- Dhroove, G.; Chogle, A.; Saps, M. A Million-Dollar Work-up for Abdominal Pain: Is It Worth It? J. Pediatr. Gastroenterol. Nutr. 2010, 51, 579–583. [Google Scholar] [CrossRef]
- Park, R.; Mikami, S.; LeClair, J.; Bollom, A.; Lembo, C.; Sethi, S.; Lembo, A.; Jones, M.; Cheng, V.; Friedlander, E.; et al. Inpatient Burden of Childhood Functional GI Disorders in the USA: An Analysis of National Trends in the USA from 1997 to 2009. Neurogastroenterol. Motil. 2015, 27, 684–692. [Google Scholar] [CrossRef]
- Hoekman, D.R.; Rutten, J.M.T.M.; Vlieger, A.M.; Benninga, M.A.; Dijkgraaf, M.G.W. Annual Costs of Care for Pediatric Irritable Bowel Syndrome, Functional Abdominal Pain, and Functional Abdominal Pain Syndrome. J. Pediatr. 2015, 167, 1103–1108.e2. [Google Scholar] [CrossRef] [PubMed]
- Youssef, N.N. Quality of Life for Children With Functional Abdominal Pain: A Comparison Study of Patients’ and Parents’ Perceptions. Pediatrics 2006, 117, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Bearden, D.J.; Waber, D.P.; Schreiber, J.E.; Mrakotsky, C. Functional Abdominal Pain Symptom Severity: Associations between Cognition and Emotion in a Pediatric Sample. Appl. Neuropsychol. Child. 2020. [Google Scholar] [CrossRef] [PubMed]
- Psihogios, A.M.; Baber, K. “Stop My Pain, but Don’t Send Me to School!” A Pediatric Case of Irritable Bowel Syndrome and School Absenteeism. Clin. Pract. Pediatr. Psychol. 2017, 5, 186–191. [Google Scholar] [CrossRef]
- Crombez, G.; Eccleston, C.; Van Damme, S.; Vlaeyen, J.W.S.; Karoly, P. Fear-Avoidance Model of Chronic Pain: The next Generation. Clin. J. Pain 2012, 28, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Tilburg, M.A.L.; Fortunato, J.E.; Squires, M.; Drossman, D.A.; Dalton, C.; Lichtman, S.; Whitehead, W.E. Impact of Eating Restriction on Gastrointestinal Motility in Adolescents With IBS. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 491–494. [Google Scholar] [CrossRef]
- Zucker, N.L.; Bulik, C.M. On Bells, Saliva, and Abdominal Pain or Discomfort: Early Aversive Visceral Conditioning and Vulnerability for Anorexia Nervosa. Int. J. Eat. Disord. 2020, 53, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, N.R.; Cohen, M.B.; Farrell, M.K.; Mezoff, A.G.; Lynch-Jordan, A.; Kashikar-Zuck, S. Concordant Parent-Child Reports of Anxiety Predict Impairment in Youth with Functional Abdominal Pain. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 312–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibler, R.C.; Beckmann, E.A.; Lynch-Jordan, A.M.; Kashikar-Zuck, S.; Mano, K.E.J. Characterizing Social and Academic Aspects of School Anxiety in Pediatric Chronic Pain. Clin. J. Pain 2019, 35, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Groenewald, C.B.; Giles, M.; Palermo, T.M. School Absence Associated With Childhood Pain in the United States. Clin. J. Pain 2019, 35, 525–531. [Google Scholar] [CrossRef]
- Sato, A.F.; Hainsworth, K.R.; Khan, K.A.; Ladwig, R.J.; Weisman, S.J.; Davies, W.H. School Absenteeism in Pediatric Chronic Pain: Identifying Lessons Learned From the General School Absenteeism Literature. Child. Health Care 2007, 36, 355–372. [Google Scholar] [CrossRef]
- Campo, J.V.; Bridge, J.; Ehmann, M.; Altman, S.; Lucas, A.; Birmaher, B.; Di Lorenzo, C.; Iyengar, S.; Brent, D.A. Recurrent Abdominal Pain, Anxiety, and Depression in Primary Care. Pediatrics 2004, 113, 817–824. [Google Scholar] [CrossRef] [Green Version]
- Malaty, H.M.; Abudayyeh, S.; Fraley, K.; Graham, D.Y.; Gilger, M.A.; Hollier, D.R. Recurrent Abdominal Pain in School Children: Effect of Obesity and Diet. Acta Paediatr. 2007, 96, 572–576. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptoms | Severity Level | Sample Average | |||
|---|---|---|---|---|---|
| Within Normal Limits | Mild | Moderate | Severe | ||
| Anxiety | 26.3% (10) | 15.8% (6) | 55.3% (21) | 2.6% (1) | M = 9.50 SD = 4.68 |
| Depression | 44.7% (17) | 21.1% (8) | 31.6% (12) | 2.6% (1) | M = 4.53 SD = 3.62 |
| Demographic | Duke Tummy Study (n = 107) | Teddy Bear Lab (n = 38) |
|---|---|---|
| Gender | Male: 43.9% (47) | Male: 39.5% (15) |
| Female: 56.1% (60) | Female: 60.5% (23) | |
| Age | M = 7.5 (SD = 1.4) | M = 7.2 (SD = 1.2) |
| Aged 5–6: 36.4% (39) | Aged 5–6: 39.5% (15) | |
| Aged 7–9: 63.6% (68) | Aged 7–9: 60.5% (23) | |
| White | 76.6% (82) | 84.2% (32) |
| Black | 12.2% (13) | 13.2% (5) |
| Asian | 1.9% (2) | 0% (0) |
| Mixed | 8.4% (9) | 2.6% (1) |
| Unknown Race | 0.9% (1) | 0% (0) |
| Hispanic | 4.7% (5) | 2.6% (1) |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Pain frequency | — | |||||||||||||
| 2. Morning pain intensity, parent rated | 0.46 ** | — | ||||||||||||
| 3. Morning pain intensity, child rated | 0.38 * | 0.80 ** | — | |||||||||||
| 4. Before dinner pain intensity, parent rated | 0.28 | 0.57 ** | 0.61 ** | — | ||||||||||
| 5. Before dinner pain intensity, child rated | 0.30 | 0.51 ** | 0.76 ** | 0.74 ** | — | |||||||||
| 6. Highest level of pain intensity, parent rated | 0.43 ** | 0.59 ** | 0.55 ** | 0.48 ** | 0.51 ** | — | ||||||||
| 7. How strong or weak do you think Teddy is, compared to other Teddys? | −0.07 | −0.04 | −0.22 | −0.12 | −0.18 | −0.06 | — | |||||||
| 8. Do you think Teddy will have the pain forever? | −0.02 | 0.10 | 0.11 | 0.29 | 0.21 | 0.36 * | 0.02 | — | ||||||
| 9. Do you think the pain will bother Teddy forever? | −0.23 | 0.11 | 0.03 | −0.06 | −0.02 | −0.06 | 0.05 | 0.25 | — | |||||
| 10. Do you think Teddy will get better at dealing with the pain? | −0.03 | 0.08 | 0.05 | 0.18 | 0.13 | −0.13 | −0.03 | −0.20 | 0.27 | — | ||||
| 11. When Teddy is a year older, how do you think Teddy will be feeling? | 0.16 | 0.13 | 0.15 | −0.16 | −0.11 | −0.11 | 0.10 | −0.38 * | −0.03 | 0.11 | — | |||
| 12. Does Teddy’s tummy pain cause problems at home? | −0.01 | −0.12 | 0.02 | 0.05 | 0.22 | 0.01 | 0.10 | 0.13 | 0.07 | 0.21 | 0.03 | — | ||
| 13. Does Teddy’s tummy pain cause problems at school? | −0.11 | −0.32* | −0.21 | −0.03 | 0.00 | −0.21 | 0.08 | −0.20 | −0.13 | −0.05 | −0.09 | 0.57 ** | — | |
| 14. Does Teddy’s tummy pain stop him from having fun most of the time? | 0.12 | −0.21 | −0.17 | −0.28 | −0.13 | −0.15 | −0.04 | −0.02 | −0.11 | −0.22 | −0.03 | 0.14 | 0.00 | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ives, L.T.; Stein, K.; Rivera-Cancel, A.M.; Nicholas, J.K.; Caldwell, K.; Datta, N.; Mauro, C.; Egger, H.; Puffer, E.; Zucker, N.L. Children’s Beliefs about Pain: An Exploratory Analysis. Children 2021, 8, 452. https://doi.org/10.3390/children8060452
Ives LT, Stein K, Rivera-Cancel AM, Nicholas JK, Caldwell K, Datta N, Mauro C, Egger H, Puffer E, Zucker NL. Children’s Beliefs about Pain: An Exploratory Analysis. Children. 2021; 8(6):452. https://doi.org/10.3390/children8060452
Chicago/Turabian StyleIves, Lindsay T., Kate Stein, Alannah M. Rivera-Cancel, Julia K. Nicholas, Kristen Caldwell, Nandini Datta, Christian Mauro, Helen Egger, Eve Puffer, and Nancy L. Zucker. 2021. "Children’s Beliefs about Pain: An Exploratory Analysis" Children 8, no. 6: 452. https://doi.org/10.3390/children8060452