
Prenatal Predictors of Neurobehavioral Outcome in Children with Fetal Growth Restriction at 6 Years of Age: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Methods
2.1. Population
2.2. Parents’ Reports and Data Collection
2.3. Behavioral Assessment
2.4. Statistical Analysis
3. Results
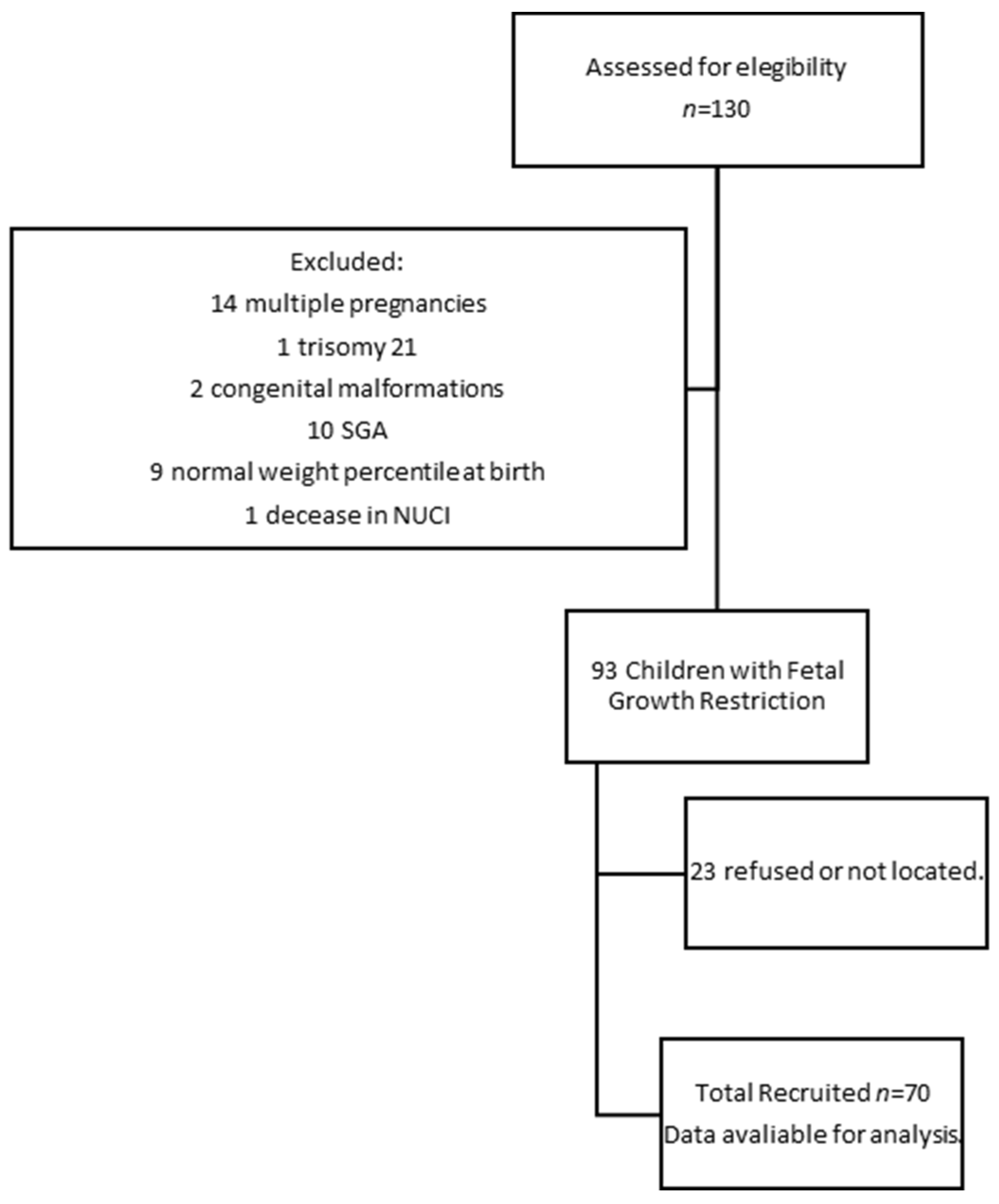
3.1. Population and Characteristics of Population Participants
3.2. Behavioral Outcomes at 6 Years of Age
3.3. Bivariant Analyses
3.4. Multivariate Analyses
4. Discussion
4.1. Regarding the Prevalence of Behavioral Disorders
4.2. Regarding the Prediction of Doppler Markers and Prematurity
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Figueras, F.; Gratacós, E. Update on the Diagnosis and Classification of Fetal Growth Restriction and Proposal of a Stage-Based Management Protocol. Fetal Diagn. Ther. 2014, 36, 86–98. [Google Scholar] [CrossRef]
- Lees, C.; Marlow, N.; Arabin, B.; Bilardo, C.M.; Brezinka, C.; Derks, J.B.; Duvekot, J.; Frusca, T.; Diemert, A.; Ferrazzi, E.; et al. Perinatal morbidity and mortality in early-onset fetal growth restriction: Cohort outcomes of the trial of randomized umbilical and fetal flow in Europe (TRUFFLE). Ultrasound Obstet. Gynecol. 2013, 42, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J.G.; Hornbuckle, J.; Vail, A.; Spiegelhalter, D.J.; Levene, M.; GRIT study group. Infant wellbeing at 2 years of age in the Growth Restriction Intervention Trial (GRIT): Multicentred randomised controlled trial. Lancet 2004, 364, 513–520. [Google Scholar] [PubMed]
- Costeloe, K.L.; Hennessy, E.M.; Haider, S.; Stacey, F.; Marlow, N.; Draper, E.S. Short term outcomes after extreme preterm birth in England: Comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ 2012, 345, e7976. [Google Scholar] [CrossRef] [PubMed]
- Simeoni, U.; Armengaud, J.-B.; Siddeek, B.; Tolsa, J.-F. Perinatal Origins of Adult Disease. Neonatology 2018, 113, 393–399. [Google Scholar] [CrossRef]
- Padilla, N.; Perapoch, J.; Carrascosa, A.; Acosta-Rojas, R.; Botet, F.; Gratacós, E. Twelve-month neurodevelopmental outcome in preterm infants with and without intrauterine growth restriction. Acta Paediatr. 2010, 99, 1498–1503. [Google Scholar] [CrossRef]
- Samuelsen, G.B.; Pakkenberg, B.; Bogdanović, N.; Gundersen, H.J.G.; Larsen, J.F.; Græm, N.; Laursen, H. Severe cell reduction in the future brain cortex in human growth–restricted fetuses and infants. Am. J. Obstet. Gynecol. 2007, 197, 56.e1–56.e7. [Google Scholar] [CrossRef]
- Tolsa, C.B.; Zimine, S.; Warfield, S.K.; Freschi, M.; Rossignol, A.S.; Lazeyras, F.; Hanquinet, S.; Pfizenmaier, M.; Hüppi, P.S. Early Alteration of Structural and Functional Brain Development in Premature Infants Born with Intrauterine Growth Restriction. Pediatr. Res. 2004, 56, 132–138. [Google Scholar] [CrossRef]
- Mallard, C.; Loeliger, M.; Copolov, D.; Rees, S. Reduced number of neurons in the hippocampus and the cerebellum in the postnatal guinea-pig following intrauterine growth-restriction. Neuroscience 2000, 100, 327–333. [Google Scholar] [CrossRef]
- Bruno, C.J.; Bengani, S.; Gomes, W.A.; Brewer, M.; Vega, M.; Xie, X.; Kim, M.; Fuloria, M. MRI Differences Associated with Intrauterine Growth Restriction in Preterm Infants. Neonatology 2017, 111, 317–323. [Google Scholar] [CrossRef]
- Fischi-Gómez, E.; Vasung, L.; Meskaldji, D.-E.; Lazeyras, F.; Borradori-Tolsa, C.; Hagmann, P.; Barisnikov, K.; Thiran, J.-P.; Hüppi, P.S. Structural Brain Connectivity in School-Age Preterm Infants Provides Evidence for Impaired Networks Relevant for Higher Order Cognitive Skills and Social Cognition. Cereb. Cortex 2015, 25, 2793–2805. [Google Scholar] [CrossRef] [PubMed]
- Padilla, N.; Junqué, C.; Figueras, F.; Sanz-Cortes, M.; Bargalló, N.; Arranz, A.; Donaire, A.; Figueras, J.; Gratacos, E. Differential vulnerability of gray matter and white matter to intrauterine growth restriction in preterm infants at 12 months corrected age. Brain Res. 2014, 1545, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dubois, J.; Benders, M.; Borradori-Tolsa, C.; Cachia, A.; Lazeyras, F.; Ha-Vinh Leuchter, R.; Sizonenko, S.V.; Warfield, S.K.; Mangin, J.F.; Hüppi, P.S. Primary cortical folding in the human newborn: An early marker of later functional development. Brain 2008, 131, 2028–2041. [Google Scholar] [CrossRef] [PubMed]
- Aarnoudse-Moens, C.S.H.; Weisglas-Kuperus, N.; van Goudoever, J.B.; Oosterlaan, J. Meta-Analysis of Neurobehavioral Outcomes in Very Preterm and/or Very Low Birth Weight Children. Pediatrics 2009, 124, 717–728. [Google Scholar] [CrossRef]
- Arpino, C.; Compagnone, E.; Montanaro, M.L.; Cacciatore, D.; De Luca, A.; Cerulli, A.; Di Girolamo, S.; Curatolo, P. Preterm birth and neurodevelopmental outcome: A review. Child’s Nerv. Syst. 2010, 26, 1139–1149. [Google Scholar] [CrossRef]
- Geva, R.; Eshel, R.; Leitner, Y.; Valevski, A.F.; Harel, S. Neuropsychological Outcome of Children with Intrauterine Growth Restriction: A 9-Year Prospective Study. Pediatrics 2006, 118, 91–100. [Google Scholar] [CrossRef]
- Geva, R.; Eshel, R.; Leitner, Y.; Fattal-Valevski, A.; Harel, S. Memory functions of children born with asymmetric intrauterine growth restriction. Brain Res. 2006, 1117, 186–194. [Google Scholar] [CrossRef]
- Gortner, L.; van Husen, M.; Thyen, U.; Gembruch, U.; Friedrich, H.-J.; Landmann, E. Outcome in preterm small for gestational age infants compared to appropriate for gestational age preterms at the age of 2 years: A prospective study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 110, S93–S97. [Google Scholar] [CrossRef]
- Guellec, I.; Lapillonne, A.; Renolleau, S.; Charlaluk, M.-L.; Roze, J.-C.; Marret, S.; Vieux, R.; Monique, K.; Ancel, P.-Y.; The EPIPAGE Study Group. Neurologic Outcomes at School Age in Very Preterm Infants Born with Severe or Mild Growth Restriction. Pediatrics 2011, 127, e883–e891. [Google Scholar] [CrossRef]
- Morsing, E.; Asard, M.; Ley, D.; Stjernqvist, K.; Marsal, K. Cognitive Function After Intrauterine Growth Restriction and Very Preterm Birth. Pediatrics 2011, 127, e874–e882. [Google Scholar] [CrossRef]
- Arcangeli, T.; Thilaganathan, B.; Hooper, R.; Khan, K.S.; Bhide, A. Neurodevelopmental delay in small babies at term: A systematic review. Ultrasound Obstet. Gynecol. 2012, 40, 267–275. [Google Scholar] [CrossRef]
- De Bie, H.M.A.; Oostrom, K.J.; Delemarre-van de Waal, H.A. Brain Development, Intelligence and Cognitive Outcome in Children Born Small for Gestational Age. Horm. Res. Paediatr. 2010, 73, 6–14. [Google Scholar] [CrossRef]
- Kulseng, S.; Jennekens-Schinkel, A.; Naess, P.; Romundstad, P.; Indredavik, M.; Vik, T.; Brubakk, A.M. Very-low-birthweight and term small-for-gestational-age adolescents: Attention revisited. Acta Paediatr. 2007, 95, 224–230. [Google Scholar] [CrossRef]
- Paz, I.; Laor, A.; Gale, R.; Harlap, S.; Stevenson, D.K.; Seidman, D.S. Term infants with fetal growth restriction are not at increased risk for low intelligence scores at age 17 years. J. Pediatr. 2001, 138, 87–91. [Google Scholar] [CrossRef]
- Savchev, S.; Sanz-Cortes, M.; Cruz-Martinez, R.; Arranz, A.; Botet, F.; Gratacos, E.; Figueras, F. Neurodevelopmental outcome of full-term small-for-gestational-age infants with normal placental function. Ultrasound Obstet. Gynecol. 2013, 42, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Sommerfelt, K. Cognitive development of term small for gestational age children at five years of age. Arch. Dis. Child. 2000, 83, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Theodore, R.F.; Thompson, J.M.D.; Waldie, K.E.; Becroft, D.M.O.; Robinson, E.; Wild, C.J.; Clark, P.M.; Mitchell, E.A.; Wild, C. Determinants of cognitive ability at 7 years: A longitudinal case–control study of children born small-for-gestational age at term. Eur. J. Pediatr. 2009, 168, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Marín, M.J.; Marín-Clavijo, J.; Blanco-Elena, J.A.; Jiménez-López, J.; González-Mesa, E. Brain Sparing Effect on Neurodevelopment in Children with Intrauterine Growth Restriction: A Systematic Review. Children 2021, 8, 745. [Google Scholar] [CrossRef]
- Benítez Marín, M.J.; Blanco Elena, J.A.; Marín Clavijo, J.; Jiménez López, J.; Lubián López, D.M.; González Mesa, E. Neurodevelopment Outcome in Children with Fetal Growth Restriction at Six Years of Age: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 11043. [Google Scholar] [CrossRef]
- Spittle, A.; Orton, J.; Anderson, P.J.; Boyd, R.; Doyle, L.W. Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants. Cochrane Database Syst. Rev. 2015, 2015, CD005495. [Google Scholar] [CrossRef]
- Robert Goodman. Available online: https://www.sdqinfo.org/a0.html (accessed on 1 December 2020).
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The Extended Version of the Strengths and Difficulties Questionnaire as a Guide to Child Psychiatric Caseness and Consequent Burden. J. Child Psychol. Psychiatry 1999, 40, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Español-Martín, G.; Pagerols, M.; Prat, R.; Rivas, C.; Sixto, L.; Valero, S.; Artigas, M.S.; Ribasés, M.; Ramos-Quiroga, J.A.; Casas, M.; et al. Strengths and Difficulties Questionnaire: Psychometric Properties and Normative Data for Spanish 5- to 17-Year-Olds. Assessment 2021, 28, 1445–1458. [Google Scholar] [CrossRef]
- Duncan, A.F.; Matthews, M.A. Neurodevelopmental Outcomes in Early Childhood. Clin. Perinatol. 2018, 45, 377–392. [Google Scholar] [CrossRef] [PubMed]
- Indredavik, M.S.; Vik, T.; Heyerdahl, S.; Kulseng, S.; Fayers, P.; Brubakk, A.M. Psychiatric symptoms and disorders in adolescents with low birth weight. Arch. Dis. Child-Fetal Neonatal Ed. 2004, 89, F445–F450. [Google Scholar] [CrossRef] [PubMed]
- Franz, A.P.; Bolat, G.U.; Bolat, H.; Matijasevich, A.; Santos, I.S.; Silveira, R.C.; Procianoy, R.S.; Rohde, L.A.; Moreira-Maia, C.R. Attention-Deficit/Hyperactivity Disorder and Very Preterm/Very Low Birth Weight: A Meta-analysis. Pediatrics 2018, 141, e20171645. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Hahn, C.-S.; Haynes, O.M. Social competence, externalizing, and internalizing behavioral adjustment from early childhood through early adolescence: Developmental cascades. Dev. Psychopathol. 2010, 22, 717–735. [Google Scholar] [CrossRef]
- Valcamonico, A.; Danti, L.; Frusca, T.; Soregaroli, M.; Zucca, S.; Abrami, F.; Tiberti, A. Absent end-diastolic velocity in umbilical artery: Risk of neonatal morbidity and brain damage. Am. J. Obstet. Gynecol. 1994, 170, 796–801. [Google Scholar] [CrossRef]
- Voßbeck, S.; de Camargo, O.K.; Grab, D.; Bode, H.; Pohlandt, F. Neonatal and neurodevelopmental outcome in infants born before 30 weeks of gestation with absent or reversed end-diastolic flow velocities in the umbilical artery. Eur. J. Pediatr. 2001, 160, 128–134. [Google Scholar] [CrossRef]
- Soregaroli, M.; Bonera, R.; Danti, L.; Dinolfo, D.; Taddei, F.; Valcamonico, A.; Frusca, T. Prognostic role of umbilical artery Doppler velocimetry in growth-restricted fetuses. J. Matern. Fetal Neonatal Med. 2002, 11, 199–203. [Google Scholar] [CrossRef]
- Kirsten, G.F.; van Zyl, J.I.; van Zijl, F.; Maritz, J.S.; Odendaal, H.J. Infants of Women with Severe Early Pre-Eclampsia: The Effect of Absent End-Diastolic Umbilical Artery Doppler Flow Velocities on Neurodevelopmental Outcome. Obstet. Gynecol. Surv. 2001, 56, 124–125. [Google Scholar] [CrossRef]
- Schreuder, A.M. Outcome at school age following antenatal detection of absent or reversed end diastolic flow velocity in the umbilical artery. Arch. Dis. Child-Fetal Neonatal Ed. 2002, 86, F108–F114. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.E.; Salavati, S.; Kooi, E.M.W.; Heijer, A.E.d.; Foreman, A.B.; Schoots, M.H.; Bilardo, C.M.; Scherjon, S.A.; Tanis, J.C.; Bos, A.F. Fetal Brain-Sparing, Postnatal Cerebral Oxygenation, and Neurodevelopment at 4 Years of Age Following Fetal Growth Restriction. Front. Pediatr. 2020, 8, 225. [Google Scholar] [CrossRef] [PubMed]
- Beukers, F.; Aarnoudse-Moens, C.S.H.; van Weissenbruch, M.M.; Ganzevoort, W.; van Goudoever, J.B.; van Wassenaer-Leemhuis, A.G. Fetal Growth Restriction with Brain Sparing: Neurocognitive and Behavioral Outcomes at 12 Years of Age. J. Pediatr. 2017, 188, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Van den Broek, A.J.M.; Kok, J.H.; Houtzager, B.A.; Scherjon, S.A. Behavioural problems at the age of eleven years in preterm-born children with or without fetal brain sparing: A prospective cohort study. Early Hum. Dev. 2010, 86, 379–384. [Google Scholar] [CrossRef]
- Hernandez-Andrade, E.; Figueroa-Diesel, H.; Jansson, T.; Rangel-Nava, H.; Gratacos, E. Changes in regional fetal cerebral blood flow perfusion in relation to hemodynamic deterioration in severely growth-restricted fetuses. Ultrasound Obstet. Gynecol. 2008, 32, 71–76. [Google Scholar] [CrossRef]
- Scherjon, S.A.; Oosting, H.; Smolders-DeHaas, H.; Zondervan, H.A.; Kok, J.H. Neurodevelopmental outcome at three years of age after fetal ‘brain-sparing’. Early Hum. Dev. 1998, 52, 67–79. [Google Scholar] [CrossRef]
- Stampalija, T.; Arabin, B.; Wolf, H.; Bilardo, C.M.; Lees, C.; Brezinka, C.; Derks, J.B.; Diemert, A.; Duvekot, J.J.; Ferrazzi, E.; et al. Is middle cerebral artery Doppler related to neonatal and 2-year infant outcome in early fetal growth restriction? Am. J. Obstet. Gynecol. 2017, 216, 521.e1–521.e13. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Birth weight less than the 3rd percentile | Structural and chromosomal abnormalities Multiple pregnancies Small for gestational age |
Birth weight less than the 10th percentile and abnormal Doppler study:
| |
| CPR = MCA-PI/UA-PI |
| Variables | n (%) | Mean ± SD |
|---|---|---|
| Separated parents | 21 (30) | |
| Maternal educational level | ||
| Primary school | 7 (10) | |
| Secondary school | 38 (54.3) | |
| Bachelor’s degree | 23 (32.9) | |
| Paternal educational level | ||
| Primary school | 18 (25.7) | |
| Secondary school | 36 (51.4) | |
| Bachelor’s degree | 13 (18.6) | |
| Maternal Unemployed status | 25 (35.7) | |
| Paternal Unemployed status | 8 (11.4) | |
| Socioeconomic status | ||
| Low | 10 (14.3) | |
| Middle | 54 (77.1) | |
| High | 4 (5.7) | |
| Smoker in pregnancy | 16 (22.9) | |
| Postpartum depression | 14 (20) | |
| Pre-eclampsia | 24 (34.3) | |
| Gestational age at diagnosis of FGR (mean) | 33.14 ± 4.31 | |
| Early onset | 23 (32.9) | |
| Late onset | 46 (65.7) | |
| Fetal weight at diagnosis | 1616.38 g ± 660.25 | |
| UA PI Percentile (mean) | 61.52 ± 27.94 | |
| Pathologic | 14 (20) | |
| MCA PI Percentile (mean) | 15.69 ± 22.68 | |
| Pathologic | 29 (41.4) | |
| CPR percentile (mean) | 14.18 ± 22.74 | |
| Pathologic | 35 (50) | |
| Vaginal delivery | 25 (35.7) | |
| Cesarean section | 45 (64.3) | |
| Gestational age at delivery | 35.61 ± 3.21 | |
| <28 weeks | 2 (2.9) | |
| 28–32 weeks | 10 (14.3) | |
| 32–37 weeks | 28 (40) | |
| >37 weeks | 30 (42.9) | |
| Pathological non-stressant test | 31 (44.3) | |
| Arterial blood cord pH | 7.27 ± 0.09 | |
| Birthweight (grams) | 1848.30 ± 589.74 | |
| Gender (female) | 37 (52.9) | |
| Head circumference at delivery (cm) | 30.26 ± 3.37 | |
| Breastfeeding | 52 (74.3) | |
| Days of NICU admission | 127 ± 26.78 | |
| Neonatal outcomes | ||
| ARDS | 22 (31.4) | |
| Neonatal sepsis | 14 (20) | |
| ROP | 6 (8.6) | |
| BPD | 4 (5.7) | |
| GMH | 3 (4.3) | |
| PDA | 6 (8.6) | |
| NEC | 3 (4.3) | |
| Intestinal perforation | 2 (2.9) | |
| Acute kidney failure | 2 (2.9) |
| SDQ Scales | Normal (%) | Borderline (%) | Abnormal (%) |
|---|---|---|---|
| Total difficulties | 70 | 15.7 | 14.3 |
| Emotional problems | 72.9 | 10 | 17.1 |
| Conduct problems | 62.9 | 25.7 | 11.4 |
| Hyperactivity | 61.4 | 8.6 | 30 |
| Peer problems | 78.6 | 11.4 | 10 |
| Prosocial | 95.7 | 2.9 | 1.4 |
| FGR Onset | Normal | Borderline | Abnormal | ||
|---|---|---|---|---|---|
| Total | E-O | 65.2 | 17.4 | 17.4 | n/s |
| L-O | 71.7 | 15.2 | 13 | ||
| Emotional | E-O | 65.2 | 21.7 | 13 | n/s |
| L-O | 76.1 | 4.3 | 19.6 | ||
| Conduct | E-O | 60.9 | 34.8 | 4.3 | n/s |
| L-O | 63 | 21.7 | 15.2 | ||
| Hyperactivity | E-O | 56.5 | 4.3 | 39.1 | n/s |
| L-O | 63 | 18.9 | 26.1 | ||
| Peer problems | E-O | 82.6 | 13 | 4.3 | n/s |
| L-O | 76.1 | 10.9 | 13 | ||
| Prosocial | E-O | 100 | 0 | 0 | n/s |
| L-O | 93.5 | 4.3 | 2.2 |
| UA | Normal (%) | Borderline (%) | Abnormal (%) | ||
|---|---|---|---|---|---|
| Total | Pathological | 64.3 | 14.3 | 21.4 | n/s |
| Normal | 74.5 | 13.7 | 11.8 | ||
| Emotional | Pathological | 64.3 | 14.3 | 21.4 | n/s |
| Normal | 74.5 | 9.8 | 15.7 | ||
| Conduct | Pathological | 64.3 | 28.6 | 7.1 | n/s |
| Normal | 64.7 | 23.5 | 11.8 | ||
| Hyperactivity | Pathological | 50 | 14.3 | 35.7 | n/s |
| Normal | 66.7 | 7.8 | 25.5 | ||
| Peer problems | Pathological | 78.6 | 14.3 | 7.1 | n/s |
| Normal | 80.4 | 7.8 | 11.8 | ||
| Prosocial | Pathological | 100 | 0 | 0 | n/s |
| Normal | 94.1 | 3.9 | 2 | ||
| MCA | |||||
| Total | Pathological | 69 | 17.2 | 13.8 | n/s |
| Normal | 80 | 13.3 | 6.7 | ||
| Emotional | Pathological | 69 | 13.8 | 17.2 | n/s |
| Normal | 80 | 6.7 | 13.3 | ||
| Conduct | Pathological | 62.1 | 31 | 6.9 | n/s |
| Normal | 70 | 16.7 | 13.3 | ||
| Hyperactivity | Pathological | 65.5 | 6.9 | 27.6 | n/s |
| Normal | 66.7 | 10 | 23.3 | ||
| Peer problems | Pathological | 75.9 | 10.3 | 13.8 | n/s |
| Normal | 83.3 | 10 | 6.7 | ||
| Prosocial | Pathological | 93.1 | 6.9 | 0 | n/s |
| Normal | 96.7 | 0 | 3.3 | ||
| CPR | |||||
| Total | Pathological | 60 | 22.9 | 17.1 | χ2(2, N = 70) = 6.36, p = 0.042 |
| Normal | 88.5 | 11.5 | 0 | ||
| Emotional | Pathological | 65.7 | 14.3 | 20 | n/s |
| Normal | 88.5 | 3.8 | 7.7 | ||
| Conduct | Pathological | 60 | 25.7 | 14.3 | n/s |
| Normal | 69.2 | 26.9 | 3.8 | ||
| Hyperactivity | Pathological | 57.1 | 11.4 | 31.4 | n/s |
| Normal | 73.1 | 3.8 | 23.1 | ||
| Peer problems | Pathological | 82.9 | 8.6 | 8.6 | n/s |
| Normal | 73.1 | 15.4 | 11.5 | ||
| Prosocial | Pathological | 97.1 | 0 | 2.9 | n/s |
| Normal | 92.3 | 7.7 | 0 |
| Model | Variables |
|---|---|
| 1 | Separated parents |
| Maternal and paternal educational level | |
| Maternal and paternal employment status | |
| Socioeconomic status | |
| 2 | Doppler measurements: |
| UA-PI percentile, MCA-PI percentile, and CPR percentile | |
| Birthweight percentile at delivery | |
| Gestational age at delivery | |
| 3 | Gender |
| Adverse neonatal outcomes | |
| Early child support | |
| Academic difficulties | |
| Nursery assistance |
| Model | Variables | Β | Standard Error | T | 95% CI | p | R2 | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| 1 | Maternal employment status | −2.97 | 1.31 | −2.26 | −5.60 | −0.355 | 0.027 | 0.077 |
| (Constant) | 12.95 | 1.06 | 12.18 | 10.82 | 15.08 | <0.001 | ||
| 2 | Birth-weight percentile | −0.659 | 0.279 | −2.36 | −1.21 | −0.100 | 0.022 | 0.089 |
| (Constant) | 11.26 | 0.697 | 16.15 | 9.86 | 12.66 | <0.001 | ||
| 3 | Need for early child support | 3.28 | 1.43 | 2.28 | 0.409 | 6.16 | 0.026 | 0.081 |
| (Constant) | 9.6 | 0.781 | 12.3 | 8.04 | 11.16 | <0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benítez Marín, M.J.; Blasco Alonso, M.; González Mesa, E. Prenatal Predictors of Neurobehavioral Outcome in Children with Fetal Growth Restriction at 6 Years of Age: A Retrospective Cohort Study. Children 2023, 10, 997. https://doi.org/10.3390/children10060997
Benítez Marín MJ, Blasco Alonso M, González Mesa E. Prenatal Predictors of Neurobehavioral Outcome in Children with Fetal Growth Restriction at 6 Years of Age: A Retrospective Cohort Study. Children. 2023; 10(6):997. https://doi.org/10.3390/children10060997
Chicago/Turabian StyleBenítez Marín, Mª José, Marta Blasco Alonso, and Ernesto González Mesa. 2023. "Prenatal Predictors of Neurobehavioral Outcome in Children with Fetal Growth Restriction at 6 Years of Age: A Retrospective Cohort Study" Children 10, no. 6: 997. https://doi.org/10.3390/children10060997