
School Mindfulness-Based Interventions for Youth, and Considerations for Anxiety, Depression, and a Positive School Climate—A Systematic Literature Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Synthesis
2.4. Quality Assessment
3. Results
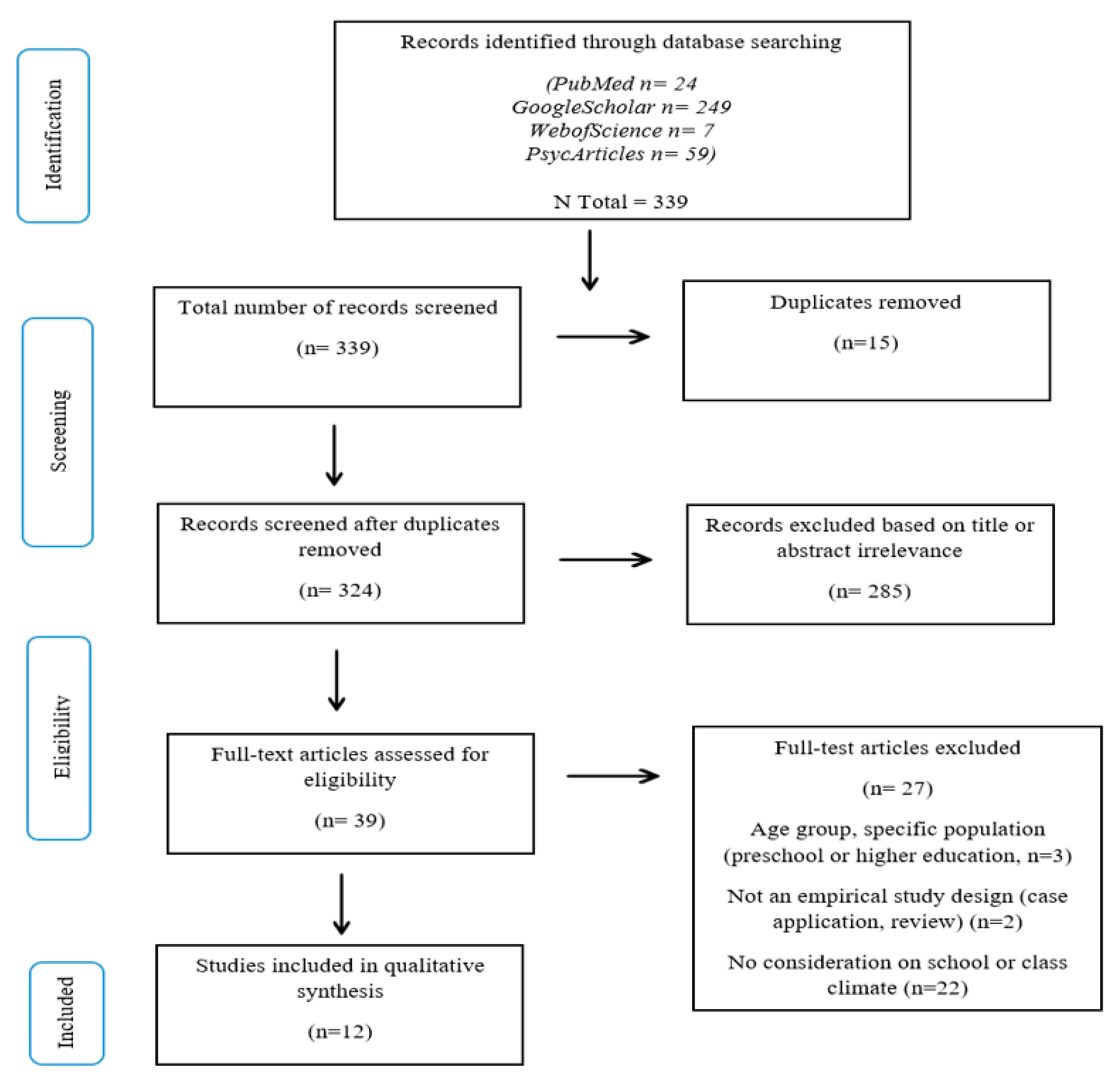
3.1. Study Selection and Characteristics

{kind=link}
| N° | Study | Country | Design | Population/Sample (N) | Intervention | Consideration for School & Class Climate |
|---|---|---|---|---|---|---|
| 1 | Waldemar et al., (2016) [47] | Brazil | Quasi-experimental design (pre/post-test measures) with inactive matched control group: MBI vs. control group Non-randomized | 5th grade (mean age 11.1) Elementary school N = 120 | M-SEL: Mindfulness—Social–Emotional Learning | Community: Yes Safety: Yes Academic: No Institution: No |
| 2 | Van de Weijer-Bergsma et al., (2012) [39] | Netherlands | RCT: MBI vs. wait list control group | Aged 8 to 12 years (mean age 9.92) Elementary school N = 199 | MindfulKids | Community: Yes Safety: Yes Academic: No Institution: Yes |
| 3 | Kielty et al., (2017) [49] | USA | One-group pre- and post-test pre-experimental design No control groups Longitudinal | Third grade (age not specified) elementary school N = 45 | Curricula designed by authors, based on Mindful Schools and MindUp | Community: Yes Safety: Yes Academic: No Institution: No |
| 4 | Schonert-Reichl et al., (2015) [41] | Canada | RCT with active control group: MBI vs. control group (SEL and Mind vs. Business as usual social responsibility program) | Aged 9 to 11 (mean age 11.16) Elementary school N = 99 | Social and Emotional Learning (SEL) combined with mindfulness based on MindUp intervention curricula | Community: Yes Safety: Yes Academic: Yes Institution: No |
| 5 | Bradley et al., (2018) [50] | USA | One-group pre- and post-test pre-experimental design No control group | Mean age 9.3 Elementary school N1 = 49 Teachers; N2 = 507 children | The Four Pillars of Well-Being | Community: Yes Safety: Yes Academic: No Institution: No |
| 6 | Parker et al., (2014) [40] | USA | RCT: MBI vs. wait list control group | Aged 9 to 11 years (mean age 10.09) Elementary school N = 111 | MasterMind | Community: Yes Safety: Yes Academic: Yes Institution: No |
| 7 | Wisner, Betsy (2014) [48] | USA | Exploratory study: pre- and post-test and mixed-method approach (concept mapping) No control group | High school grades 10, 11, 12 (mean age: 17.89) N = 35 | Mindfulness meditation (MM) | Community: Yes Safety: Yes Academic: No Institution: Yes |
| 8 | Kuyken et al., (2022) [42] | UK | Study protocol for cluster randomized controlled parallel group trial (inactive) | Aged 11 to 16 years old (students) N = 672 (teachers) N Schools = 85 (approx. 1000 students) | School-based mindfulness training (SBMT) | Community: Yes Safety: Yes Academic: Yes Institution: Yes |
| 9 | Lombas et al., (2019) [44] | Spain | Quasi-experimental design (pre/post-test measures) with controlled group (inactive) | (Mean age: 13.6 years, Grades 7, 8, 9, 10) N = 524 | Happy Classrooms Program (HCP) | Community: Yes Safety: Yes Academic: Yes Institution: No |
| 10 | Suárez-García et al., (2020) [46] | Spain | Quasi-experimental switching replications design (pre/post-test measures) with controlled group (inactive) | Aged between 7 and 10, 3rd year primary (mean age: 8.08) N = 73 (students) N = 5 (teachers) | Mindkeys training | Community: Yes Safety: Yes Academic: Yes Institution: No |
| 11 | Lauren Meyer & Katie Eklund (2020) [45] | USA | Quasi-experimental design (pre/post-test measures) with controlled group (wait list) | 4th grade and 5th grade elementary (mean age: 9.3) Students N = 296 Teachers N = 14 | Mindful Moments Intervention | Community: Yes Safety: Yes Academic: Yes Institution: No |
| 12 | Moreno-Gómez, Luna, & Cejudo, (2020) [43] | Spain | Quasi-experimental design (pre/post-test measures) with controlled group (inactive) | Aged 5 to 6 years (mean age: 5.69) N = 114 | Mindkinder | Community: Yes Safety: Yes Academic: Yes Institution: No |
| Quality Assessment Tools for Controlled Intervention Studies | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Randomization Method | Treatment Allocation Concealed | Blinding of Patients and Providers | Blind Assessors | No Base-Line Group Differ-rence | Drop-Out Rate >20% | Drop-Out Rate between Groups >15% | Treatment Protocol Adherence | Other Treatment Avoided or Similar |
| Van de Weijer-Bergsma et al. (2012) [39] | Good | Fair | Poor | NR | Good | Good | Good | Good | Good |
| Schonert-Reichl et al. (2015) [41] | Good | Fair | Poor | Good | Good | Good | Good | Good | Good |
| Parker et al. (2016) [40] | Good | Fair | Poor | NR | Good | Good | Good | Good | Good |
| Waldemar et al. (2016) [47] | NA | NA | Poor | NR | Good | Good | Good | Good | Good |
| Suárez-García et al. (2020) [46] | NA | NA | NR | NR | Good | Good | Good | Good | Good |
| Meyer & Eklund (2020) [45] | NA | NA | NR | NR | Good | Good | Good | Good | Good |
| Moreno et al. (2020) [43] | Good | Fair | NR | NR | Good | Good | Good | Good | Good |
| Lombas et al. (2019) [44] | NA | NA | Poor | NA | NR | NR | NR | Good | Good |
| Kuyken et al. (2022) [42] | Good | Fair | Poor | NR | Fair | Good | Good | Good | Good |
| Quality Assessment Tool for before–after (pre–post) studies | |||||||||
| Study | Study question | Eligibility criteria and population | Study participant representative of population of interest | 1. Enrolment of all eligible participants 2. Sample size | Inter-vention clearly described | 1. Outcome measure * 2. Blinding ** | Follow-up rate | 1. Statistical analysis and 2. Multiple outcome measures | Group-level interventions/individual level outcome efforts |
| Wisner, Betsy (2014) [48] | Good | Good | Good | 1. Fair 2. Poor | Good | 1. Fair 2. NR | Poor | 1. Good 2. Poor | Good |
| Kielty et al. (2017) [49] | Good | Good | Fair | 1. Fair 2. Fair | Fair | 1. Fair 2. NR | Poor | 1. Good 2. Poor | Good |
| Bradley et al. (2018) [50] | Good | Good | Good | 1. Fair 2. Good | Good | 1. Fair 2. NR | Poor | 1. Good 2. Fair | Good |
3.2. Quality of Included Studies
3.3. Participant Characteristics
3.4. Outcome Measures
3.4.1. School-Based Mindfulness Interventions
3.4.2. Stress & Anxiety
3.4.3. Depression
3.4.4. Emotional and Behavioral Regulation
3.4.5. Cognitive Abilities
3.4.6. Social Abilities
3.4.7. Mindfulness
3.4.8. Environment: School and Class Climates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kabat-Zinn, J. Mindfulness-based stress reduction (MBSR). Constr. Hum. Sci. 2003, 8, 73. [Google Scholar]
- Cullen, M. Mindfulness-based interventions: An emerging phenomenon. Mindfulness 2011, 2, 186–193. [Google Scholar] [CrossRef]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and commitment therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Linehan, M.M.; Schmidt, H.; Dimeff, L.A.; Craft, J.C.; Kanter, J.; Comtois, K.A. Dialectical behavior therapy for patients with borderline personality disorder and drug-dependence. Am. J. Addict. 1999, 8, 279–292. [Google Scholar] [PubMed]
- Segal, Z.V.; Teasdale, J.D.; Williams, J.M.; Gemar, M.C. The mindfulness-based cognitive therapy adherence scale: Inter-rater reliability, adherence to protocol and treatment distinctiveness. Clin. Psychol. Psychother. 2002, 9, 131–138. [Google Scholar] [CrossRef]
- Klatt, M.; Harpster, K.; Browne, E.; White, S.; Case-Smith, J. Feasibility and preliminary outcomes for move-into-learning: An arts-based mindfulness classroom intervention. J. Posit. Psychol. 2013, 8, 233–241. [Google Scholar] [CrossRef]
- Deplus, S.; Lahaye, M. La Pleine Conscience Chez L’enfant Et L’adolescent: Programs D’initiation et D’entraînement; Mardaga: Wavre, Belgium, 2015. [Google Scholar]
- Maloney, J.E.; Lawlor, M.S.; Schonert-Reichl, K.A.; Whitehead, J.A. A mindfulness-based social and emotional learning curriculum for school-aged children: The MindUP program. In Handbook of Mindfulness in Education; Springer: New York, NY, USA, 2016; pp. 313–334. [Google Scholar]
- Bishop, S.R.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.D.; Carmody, J.; Segal, Z.V.; Abbey, S.; Speca, M.; Velting, D.; et al. Mindfulness: A proposed operation definition. Clin. Psychol. Sci. Pract. 2004, 11, 230–241. [Google Scholar] [CrossRef]
- Chiesa, A.; Calati, R.; Serretti, A. Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clin. Psychol. Rev. 2011, 31, 449–464. [Google Scholar] [CrossRef]
- Jha, A.P.; Morrison, A.B.; Parker, S.C.; Stanley, E.A. Practice is protective: Mindfulness training promotes cognitive resilience in high-stress cohorts. Mindfulness 2017, 8, 46–58. [Google Scholar] [CrossRef]
- Hafenbrack, A.; Cameron, L.; Spreitzer, G.; Zhang, C.; Noval, L.; Shaffakat, S. Helping People by Being in the Present: Mindfulness Increases Prosocial Behavior. Organ. Behav. Hum. Decis. Process. 2020, 159, 21–38. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-based interventions for anxiety and depression. Psychiatr. Clin. 2017, 40, 739–749. [Google Scholar] [CrossRef]
- Guendelman, S.; Medeiros, S.; Rampes, H. Mindfulness and emotion regulation: Insights from neurobiological, psychological, and clinical studies. Front. Psychol. 2017, 8, 220. [Google Scholar] [CrossRef]
- Keng, S.L.; Smoski, M.J.; Robins, C.J. Effects of mindfulness on psychological health: A review of empirical studies. Clin. Psychol. Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef]
- Broderick, P.C.; Metz, S. Learning to BREATHE: A pilot trial of a mindfulness curriculum for adolescents. Adv. Sch. Ment. Health Promot. 2009, 2, 35–46. [Google Scholar] [CrossRef]
- Semple, R.J.; Lee, J. Mindfulness-based cognitive therapy for children. In Mindfulness-Based Treatment Approaches; Academic Press: Cambridge, MA, USA, 2014; pp. 161–188. [Google Scholar]
- Felver, J.C.; Celis-de Hoyos, C.E.; Tezanos, K.; Singh, N.N. A systematic review of mindfulness-based interventions for youth in school settings. Mindfulness 2016, 7, 34–45. [Google Scholar] [CrossRef]
- Van Loon, A.W.G.; Creemers, H.E.; Beumer, W.Y.; Okorn, A.; Vogelaar, S.; Saab, N.; Miers, A.C.; Westenberg, P.M.; Asscher, J.J. Can schools reduce adolescent psychological stress? A multilevel meta-analysis of the effectiveness of school-based intervention programs. J. Youth Adolesc. 2020, 49, 1127–1145. [Google Scholar] [CrossRef]
- McKeering, P.; Hwang, Y.S. A systematic review of mindfulness-based school interventions with early adolescents. Mindfulness 2019, 10, 593–610. [Google Scholar] [CrossRef]
- Devcich, D.A.; Rix, G.; Bernay, R.; Graham, E. Effectiveness of a mindfulness-based program on school children’s self-reported well-being: A pilot study comparing effects with an emotional literacy program. J. Appl. Sch. Psychol. 2017, 33, 309–330. [Google Scholar] [CrossRef]
- Maynard, B.R.; Solis, M.R.; Miller, V.L.; Brendel, K.E. Mindfulness-based interventions for improving cognition, academic achievement, behavior, and socioemotional functioning of primary and secondary school students. Campbell Syst. Rev. 2017, 13, 1–144. [Google Scholar] [CrossRef]
- Viafora, D.P.; Mathiesen, S.G.; Unsworth, S.J. Teaching mindfulness to middle school students and homeless youth in school classrooms. J. Child Fam. Stud. 2015, 24, 1179–1191. [Google Scholar] [CrossRef]
- Malboeuf-Hurtubise, C.; Lacourse, E.; Taylor, G.; Joussemet, M.; Ben Amor, L. A mindfulness-based intervention pilot feasibility study for elementary school students with severe learning difficulties: Effects on internalized and externalized symptoms from an emotional regulation perspective. J. Evid. Based Complement. Altern. Med. 2017, 22, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.T.; Degol, J.L. School climate: A review of the construct, measurement, and impact on student outcomes. Educ. Psychol. Rev. 2016, 28, 315–352. [Google Scholar] [CrossRef]
- Aldridge, J.M.; Fraser, B.J.; Fozdar, F.; Ala’i, K.; Earnest, J.; Afari, E. Students’ perceptions of school climate as determinants of wellbeing, resilience and identity. Improv. Sch. 2016, 19, 5–26. [Google Scholar] [CrossRef]
- Evans, I.M.; Harvey, S.T.; Buckley, L.; Yan, E. Differentiating classroom climate concepts: Academic, management and emotional environments. Kōtuitui. N. Z. J. Soc. Sci. Online 2009, 4, 131–146. [Google Scholar] [CrossRef]
- Jennings, P.A.; Greenberg, M.T. The prosocial classroom: Teacher social and emotional competence in relation to student and classroom outcomes. Rev. Educ. Res. 2009, 79, 491–525. [Google Scholar] [CrossRef]
- Meyer, L.N. A Change in Forecast: A Preliminary Analysis of the Effects of a Brief Mindfulness Intervention on Elementary School Class Climate; ProQuest LLC: Ann Arbor, MI, USA, 2018. [Google Scholar]
- Eisenberg, N.; Spinrad, T.L.; Eggum, N.D. Emotion-related self-regulation and its relation to children’s maladjustment. Annu. Rev. Clin. Psychol. 2010, 6, 495–525. [Google Scholar] [CrossRef]
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef]
- Poulin, P.A.; Mackenzie, C.S.; Soloway, G.; Karayolas, E. Mindfulness training as an evidenced-based approach to reducing stress and promoting well-being among human services professionals. Int. J. Health Promot. Educ. 2008, 46, 72–80. [Google Scholar] [CrossRef]
- Merrell, K.W.; Carrizales, D.C.; Feuerborn, L.C.; Gueldner, B.A.; Tran, O.K. Strong Kids Grades 6–8: A Social and Emotional Learning Curriculum; Paul H Brookes Publishing: Baltimore, MD, USA, 2007. [Google Scholar]
- Caballero, C.; Scherer, E.; West, M.R.; Mrazek, M.D.; Gabrieli, C.F.; Gabrieli, J.D. Greater mindfulness is associated with better academic achievement in middle school. Mind Brain Educ. 2019, 13, 157–166. [Google Scholar] [CrossRef]
- Galla, B.M.; Esposito, M.V.; Fiore, H.M. Mindfulness predicts academic diligence in the face of boredom. Learn. Individ. Differ. 2020, 81, 101864. [Google Scholar] [CrossRef]
- Mak, C.; Whittingham, K.; Cunnington, R.; Boyd, R.N. Efficacy of mindfulness-based interventions for attention and executive function in children and adolescents—A systematic review. Mindfulness 2018, 9, 59–78. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Van de Weijer-Bergsma, E.; Langenberg, G.; Brandsma, R.; Oort, F.J.; Bögels, S.M. The Effectiveness of a School-Based Mindfulness Training as a Program to Prevent Stress in Elementary School Children. Mindfulness 2014, 5, 238–248. [Google Scholar] [CrossRef]
- Parker, A.E.; Kupersmidt, J.B.; Mathis, E.T.; Scull, T.M.; Sims, C. The impact of mindfulness education on elementary school students: Evaluation of the Master Mind program. Adv. Sch. Ment. Health Promot. 2014, 7, 184–204. [Google Scholar] [CrossRef]
- Schonert-Reichl, K.A.; Oberle, E.; Lawlor, M.S.; Abbott, D.; Thomson, K.; Oberlander, T.F.; Diamond, A. Enhancing cognitive and social–emotional development through a simple-to-administer mindfulness-based school program for elementary school children: A randomized controlled trial. Dev. Psychol. 2015, 51, 52. [Google Scholar] [CrossRef]
- Kuyken, W.; Ball, S.; Crane, C.; Ganguli, P.; Jones, B.; Montero-Marin, J.; Nuthall, E.; Raja, A.; Taylor, L.; Tudor, K.; et al. Effectiveness and cost-effectiveness of universal school-based mindfulness training compared with normal school provision in reducing risk of mental health problems and promoting well-being in adolescence: The MYRIAD cluster randomised controlled trial. BMJ Ment. Health 2022, 25, 99–109. [Google Scholar] [CrossRef]
- Moreno-Gómez, A.; Luna, P.; Cejudo, J. Promoting school success through mindfulness-based interventions in early childhood. Rev. De Psicodidáctica Engl. Ed. 2020, 25, 136–142. [Google Scholar] [CrossRef]
- Lombas, A.S.; Jiménez, T.I.; Arguís-Rey, R.; Hernández-Paniello, S.; Valdivia-Salas, S.; Martín-Albo, J. Impact of the happy classrooms programme on psychological well-being, school aggression, and classroom climate. Mindfulness 2019, 10, 1642–1660. [Google Scholar] [CrossRef]
- Meyer, L.; Eklund, K. The impact of a mindfulness intervention on elementary classroom climate and student and teacher mindfulness: A pilot study. Mindfulness 2020, 11, 991–1005. [Google Scholar] [CrossRef]
- Suárez-García, Z.; Álvarez-García, D.; García-Redondo, P.; Rodríguez, C. The effect of a mindfulness-based intervention on attention, self-control, and aggressiveness in primary school pupils. Int. J. Environ. Res. Public Health 2020, 17, 2447. [Google Scholar] [CrossRef] [PubMed]
- Waldemar JO, C.; Rigatti, R.; Menezes, C.B.; Guimarães, G.; Falceto, O.; Heldt, E. Impact of a combined mindfulness and social–emotional learning program on fifth graders in a Brazilian public school setting. Psychol. Neurosci. 2016, 9, 79. [Google Scholar] [CrossRef]
- Wisner, B.L. An exploratory study of mindfulness meditation for alternative school students: Perceived benefits for improving school climate and student functioning. Mindfulness 2014, 5, 626–638. [Google Scholar] [CrossRef]
- Kielty, M.; Gilligan, T.; Staton, R.; Curtis, N. Cultivating mindfulness with third grade students via classroom-based interventions. Contemp. Sch. Psychol. 2017, 21, 317–322. [Google Scholar] [CrossRef]
- Bradley, C.; Cordaro, D.T.; Zhu, F.; Vildostegui, M.; Han, R.J.; Brackett, M.; Jones, J. Supporting improvements in classroom climate for students and teachers with the four pillars of wellbeing curriculum. Transl. Issues Psychol. Sci. 2018, 4, 245. [Google Scholar] [CrossRef]
- Diamond, A.; Barnett, W.S.; Thomas, J.; Munro, S. Preschool program improves cognitive control. Science 2007, 318, 1387–1388. [Google Scholar] [CrossRef]
- Kupersmidt, J.B.; Scull, T.M.; Austin, E.W. Media literacy education for elementary school substance use prevention: Study of media detective. Pediatrics 2010, 126, 525–531. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth, and Families: Burlington, VT, USA, 2001. [Google Scholar]
- Kendall, P.; Wilcox, L. Self-control in children: Development of a rating scale. J. Consult. Clin. Psychol. 1979, 47, 1020–1029. [Google Scholar] [CrossRef]
- Fleitlich, B.; Cortázar, P.G.; Goodman, R. 2000. Questionário de capacidades e dificuldades (SDQ). Infanto Rev. Neuropsiquiatr. Infanc. Adolesc. 2000, 8, 44–50. [Google Scholar]
- Salum, G.A.; Patrick, D.L.; Isolan, L.R.; Manfro, G.G.; Fleck, M.P. Youth Quality of Life Instrument-Research version (YQOL-R): Psychometric properties in a community sample. J. De Pediatr. 2012, 88, 443–448. [Google Scholar] [CrossRef]
- Mattos, P.; Serra-Pinheiro, M.A.; Rohde, L.A.; Pinto, D. A brazilian portuguese version of the MTA-SNAP-IV for the evaluation of ADHD and ODD symptoms. Rev. De Psiquiatr. Do Rio Gd. Do Sul 2006, 28, 290–297. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Diener, E.; Emmons, R.; Larsen, R.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 91–95. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; SAGE: Newbury Park, CA, USA, 1988; pp. 31–68. [Google Scholar]
- León, J.; Fernández, C.; Grijalvo, F.; Núñez, J. Assessing mindfulness: The Spanish version of the Mindfulness Attention Awareness Scale. Estud. De Psicol. 2013, 34, 175–184. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity, and repair: Exploring emotional intelligence using the trait meta mood scale. In Emotion, Disclosure, & Health; Pennebaker, J.W., Ed.; American Psychological Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Bryant, B.K. An index of empathy for children and adolescents. Child Dev. 1982, 53, 413–425. [Google Scholar] [CrossRef]
- Little, T.D.; Henrich, C.C.; Jones, S.M.; Hawley, P.H. Disentangling the “whys” from the “whats” of aggressive behavior. Int. J. Behav. Dev. 2003, 27, 122–133. [Google Scholar] [CrossRef]
- Vallerand, R.J.; Blais, M.R.; Brière, N.M.; Pelletier, L.G. Construction et validation de l’Échelle de Motivation en Éducation (EME). Can. J. Behav. Sci. 1989, 21, 323–349. [Google Scholar] [CrossRef]
- Moos, R.H.; Moos, B.S.; Trickett, E.J. FES, WES, CIES, CES. Escalas de Clima Social; TEA: Madrid, Spain, 1989. [Google Scholar]
- Davis, M. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Personal. Soc. Psychol. 1983, 44, 113–126. [Google Scholar] [CrossRef]
- Song, M. Two studies on the Resiliency Inventory (RI): Toward the Goal of Creating a Culturally Sensitive Measure of Adolescent Resilience. Unpublished. Doctoral Dissertation, Harvard University, Cambridge, MA, USA, 2003. [Google Scholar]
- Marsh, H.W. Age and sex effects in multiple dimensions of preadolescent self-concept. Aust. J. Psychol. 1985, 37, 197–204. [Google Scholar] [CrossRef]
- Kusché, C.A.; Greenberg, M.T.; Beilke, R. Seattle Personality Questionnaire for Young School-Aged Children; Unpublished Personality Questionnaire; Manuscript in Preparation; University of Washington, Department of Psychology: Seattle, WA, USA, 1988. [Google Scholar]
- Wentzel, K.R. Does being good make the grade? Social behavior and academic competence in middle school. J. Educ. Psychol. 1993, 85, 357–364. [Google Scholar] [CrossRef]
- Renshaw, T.L. Preliminary development and validation of the Mindful Student Questionnaire. Assess. Eff. Interv. 2017, 42, 168–175. [Google Scholar] [CrossRef]
- Furlong, M.J.; You, S.; Renshaw, T.L.; O’Malley, M.D.; Rebelez, J. Preliminary development of the positive experiences at school scale for elementary school students. Child Indic. Res. 2013, 6, 753–775. [Google Scholar] [CrossRef]
- Cattell, R.B.; Cattell, A.K.S. Factor G, Escala 1 y Escala 2; TEA Ediciones: Madrid, Spain, 1995. [Google Scholar]
- Thurstone, L.; Yela, M. CARAS-R: Test de Percepción de Diferencias Revisado; TEA Ediciones: Madrid, Spain, 2012. [Google Scholar]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [PubMed]
- Sink, C.A.; Spencer, L.R. Teacher version of the My class inventory-short form: An accountability tool for elementary school counselors. Prof. Sch. Couns. 2007, 11, 129–139. [Google Scholar] [CrossRef]
- Greco, L.A.; Baer, R.A.; Smith, G.T. Assessing mindfulness in children and adolescents: Development and validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychol. Assess. 2011, 23, 606. [Google Scholar] [CrossRef]
- Sink, C.A.; Spencer, L.R. My class inventory-short form as an accountability tool for elementary school counselors to measure classroom climate. Prof. Sch. Couns. 2005, 9, 37–48. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Cordaro, D.T.; Brackett, M.; Glass, L.; Anderson, C.L. Contentment: Perceived completeness across cultures and traditions. Rev. Gen. Psychol. 2016, 20, 221–223. [Google Scholar] [CrossRef]
- Burns, D.D. Ten Days to Self-Esteem: The Leader’s Manual; Quill/Harper Collins: New York, NY, USA, 1993. [Google Scholar]
- Tschannen-Moran, M.; Hoy, A.W. Teacher efficacy: Capturing an elusive construct. Teach. Teach. Educ. 2001, 17, 783–805. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Macdonald, S.; MacIntyre, P. The generic job satisfaction scale: Scale development and its correlates. Empl. Assist. Q. 1997, 13, 1–16. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Feldman, G.; Hayes, A.; Kumar, S.; Greeson, J.; Laurenceau, J.P. Mindfulness and emotion regulation: The development and initial validation of the Cognitive and Affective Mindfulness Scale Revised (CAMS-R). J. Psychopathol. Behav. Assess. 2007, 29, 177–190. [Google Scholar] [CrossRef]
- Frank, J.L.; Jennings, P.A.; Greenberg, M.T. Validation of the mindfulness in teaching scale. Mindfulness 2016, 7, 155–163. [Google Scholar] [CrossRef]
- Reynolds, C.R.; Kamphaus, R.W. Behavior Assessment System for Children, Manual; American Guidance Service, Inc.: Circle Pines, MN, USA, 1998. [Google Scholar]
- Garaigordobil, M.; Maganto, C. SPECI. Screening de problemas emocionales y de conducta infantil: Descripción y datos psicométricos. Int. J. Dev. Educ. Psychol. 2014, 4, 319–328. [Google Scholar]
- Jellesma, F.C.; Meerum Terwogt, M.; Reijntjes, A.H.; Rieffe, C.; Stegge, H. De vragenlijst Non-Productieve Denkprocessem voor Kinderen (NPDK). Kind Adolesc. 2005, 26, 368–378. [Google Scholar] [CrossRef]
- Rieffe, C.; Meerum Terwogt, M.; Kortonopoulou, K. Awareness of single and multiple emotions in high-functioning children with autism. J. Autism Dev. Disord. 2007, 37, 455–465. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Lepper, H.S. A measure of subjective happiness: Preliminary reliability and construct validation. Soc. Indic. Res. 1999, 46, 137–155. [Google Scholar] [CrossRef]
- Bodden, D.H.M.; Bögels, S.M.; Muris, P. The diagnostic Utility of the Screen for Child Anxiety Related Emotional Disorders-71 (SCARED-71). Behav. Res. Ther. 2009, 47, 418–425. [Google Scholar] [CrossRef]
- LaFreniere, P.J.; Dumas, J.E. Social competence and behavior evaluation in children ages 3 to 6 years: The short form (SCBE-30). Psychol. Assess. 1996, 8, 369–377. [Google Scholar] [CrossRef]
- Bruni, O.; Ottaviano, S.; Guidetti, V.; Romoli, M.; Innocenzi, M.; Cortesi, F.; Giannotti, F. The sleep disturbance scale for children (SDSC) construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J. Sleep Res. 1996, 5, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, S.H.; Winter, M.; Hox, J. Klasklimaatvragenlijst voor Leerkrachten [Class-Climate Questionnaire for Teachers]; Utrecht University, Langeveld Institute: Utrecht, The Netherland, 2007. [Google Scholar]
- Lickona, D.; Davidson, M. School as a Caring Community Profile-II; Unpublished Manuscript in Preparation; Center for the 4th and 5th Rs: Cortland, NY, USA, 2003. [Google Scholar]
- Brackett, M.A.; Rivers, S.E.; Maurer, M.; Elbertson, N.A.; Kremenitzer, J.P. Creating emotionally literate learning environments. Creat. Emot. Lit. Learn. Environ. 2011, 1–21. [Google Scholar] [CrossRef]
- Yoon, J.; Desmet, P.M.; Pohlmeyer, A.E. Embodied typology of positive emotions: The development of a tool to facilitate emotional granularity in design. In IASDR 2013: Proceedings of the 5th International Congress of International Association of Societies of Design Research “Consilience and Innovation in Design”, Tokyo, Japan, 26–30 August 2013; International Association of Societies of Design Research: Aalto, Finland, 2013. [Google Scholar]
- Porter, B.; Oyanadel, C.; Sáez-Delgado, F.; Andaur, A.; Peñate, W. Systematic Review of Mindfulness-Based Interventions in Child-Adolescent Population: A Developmental Perspective. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1220–1243. [Google Scholar] [CrossRef]
- Emerson, L.M.; De Diaz, N.N.; Sherwood, A.; Waters, A.; Farrell, L. Mindfulness interventions in schools: Integrity and feasibility of implementation. Int. J. Behav. Dev. 2020, 44, 62–75. [Google Scholar] [CrossRef]
- Ritvo, P.; Ahmad, F.; El Morr, C.; Pirbaglou, M.; Moineddin, R.; MVC Team. A mindfulness-based intervention for student depression, anxiety, and stress: Randomized controlled trial. JMIR Ment. Health 2021, 8, e23491. [Google Scholar] [CrossRef]
- Dunning, D.L.; Griffiths, K.; Kuyken, W.; Crane, C.; Foulkes, L.; Parker, J.; Dalgleish, T. Research review: The effects of mindfulness-based interventions on cognition and mental health in children and adolescents-a meta-analysis of randomized controlled trials. J. Child Psychol. Psychiatry 2018, 60, 244–258. [Google Scholar] [CrossRef]
- Odgers, C.L.; Jensen, M.R. Annual research review: Adolescent mental health in the digital age: Facts, fears, and future directions. J. Child Psychol. Psychiatry 2020, 61, 336–348. [Google Scholar] [CrossRef]
- Fulambarkar, N.; Seo, B.; Chesterman, A.; Rees, M.; Bausback, K.; Bunge, E. Meta-analysis on mindfulness-based interventions for adolescents’ stress, depression, and anxiety in school settings: A cautionary tale. Child Adolesc. Ment. Health 2023, 28, 307–317. [Google Scholar] [CrossRef]
- Reangsing, C.; Punsuwun, S.; Schneider, J.K. Effects of mindfulness interventions on depressive symptoms in adolescents: A meta-analysis. Int. J. Nurs. Stud. 2021, 115, 103848. [Google Scholar] [CrossRef]
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- Cohen, S. Social Relationships and Health. Am. Psychol. 2004, 59, 676–684. [Google Scholar] [CrossRef]
- Hwang, Y.S.; Bartlett, B.; Greben, M.; Hand, K. A systematic review of mindfulness interventions for in-service teachers: A tool to enhance teacher wellbeing and performance. Teach. Teach. Educ. 2017, 64, 26–42. [Google Scholar] [CrossRef]
- Laukkonen, R.; Leggett, J.M.I.; Gallagher, R.; Biddell, H.; Mrazek, A.; Slagter, H.; Mrazek, M. The Science of Mindfulness-Based Interventions and Learning: A Review for Educators; Organisation for Economic Co-Operation and Development: Paris, France, 2020. [Google Scholar]

| Implementation and Program Measures | Teacher Assessment Measures | Student Assessment Measures | ||
|---|---|---|---|---|
| Self-Reported | Teacher or Parent Reported | |||
| Parker et al., (2014) [40] | A trained observer rated each teacher’s fidelity of implementation in the three intervention classrooms. Teacher interview for intervention feasibility. | Executive functions: flanker fish task (Diamond et al., 2007) [51]; Intentions to Use Alcohol and Tobacco Scale (Kupersmidt, Scull, & Austin, 2010) [52] | Behavior and emotion regulation: Children’s Behavior Checklist Teachers’ Report Form (C-TRF) [53]; Self-Control Rating Scale (SCRS) [54] | |
| Waldemar et al., (2016) [47] | The Strengths and Difficulties Questionnaire—Child Version (SDQ-C) [55] (hyperactivity, emotional problems, conduct problems, interpersonal relationship, and prosocial behavior); The Youth Quality of Life Instrument (YQOL-R) [56] (personal, relational, environmental, and general); ADHD: The Swanson, Nolan and Pelham Questionnaire–IV (SNAP-IV) [57] | |||
| Lombas et al., (2019) [44] | Teacher Acceptability and Implementation Fidelity Questionnaire | Student Acceptability Questionnaire; Mindfulness (MAAS) [58]; Self-esteem: Rosenberg Self-Esteem Scale [59]; Satisfaction with life: Satisfaction with Life Scale [60]; Depressive symptomatology: Reduced Scale of Depressive Symptomatology [61]; Perceived stress: Perceived Stress Scale [62]; Basic psychological needs: Psychological Needs Satisfaction Scale in Education [63]; Emotional intelligence: Trait Meta-Mood Scale [64]; Empathy: Index of Empathy for Children and Adolescents [65]; School aggression: School Aggression Scale [66]; Academic motivation: Academic motivation according to self-determination theory [67] | Classroom Environment Scale [68] | |
| Schonert-Reichl et al., (2015) [41] | Survey on dosage of implementation | Executive functions: Flanker task and the hearts and flowers version of the dots task [51]; Cortisol salivatory measure; Empathy and perspective: Interpersonal Reactivity Index [69]; Resiliency inventory (RI) (optimism and emotional control subscales) [70]; The school self-concept scale from Marsh’s Self-Description Questionnaire,) [71]; Depression: Seattle Personality Questionnaire for Children [72]; Mindfulness: The Mindful Attention Awareness Scale adapted for children [58]; Social responsibility: subscale of the Social Goals Questionnaire [73]; Peer-nomination for prosociality and peer acceptance | Math grade for achievement measure | |
| Kielty et al., (2017) [49] | Qualitative surveys about experience and curriculum | Teacher Fidelity and Acceptability Measure created for this study. | Mindfulness Student Questionnaire [74]; Positive Experiences at School Scale [75] | |
| Suárez-García et al., (2020). [46] | The Factor G test (Scale 2—Form A), [76]; Test of Perception of Differences—Revised (CARAS-R) [77] | Evaluation System for Children and Adolescents—school teachers’ version (SENA), subscales: “Attention Problems”, “Hyperactivity-impulsivity”, “Aggression” | ||
| Lauren Meyer & Katie Eklund (2020) [45] | The Kentucky Inventory of Mindfulness [78]; My Class Inventory—Teacher Form [79] | Child and Adolescent Mindfulness Measure [80]; My Class Inventory—Short Form Revised [81] | ||
| Wisner, Betsy (2014) [48] | Concept mapping | Concept Mapping and Narrative Questionnaire | ||
| Bradley et al., (2018) [50] | Weekly Teacher Implementation Survey; Biannual Outcome Survey (battery of validated self-report measures) | The Maslach Burnout Inventory Educators Survey [82]; Ryff’s Scales of Psychological Well-Being [83]; The Positive Emotion Assessment of Contentment Scale [84]; The Relationship Satisfaction Scale [85]; The Teachers’ Sense of Efficacy Scale—Short Form [86]; The Self-Compassion Scale—Short Form [87]; The Generic Job Satisfaction [88]; The Perceived Stress Scale 10-Item Inventory [89]; The Cognitive and Affective Mindfulness Scale—Revised 10-item version [90]; Well-Being Survey | Mood Meter Report (emotion plotting tool) | |
| Kuyken et al., (2022) [42] | The Maslach Burnout Inventory Educators Survey [82]; The Teachers’ Sense of Efficacy Scale [86]; Five-Facet Mindfulness Questionnaire—Short Form [78]; Mindfulness in Teaching Scale [91]; Perceived Stress Scale, PSS [62]; Anxiety and depression (Patient Health Questionnaire); School Climate and Connectedness Survey | |||
| Moreno-Gómez, Luna, & Cejudo (2020) [43] | Behavior Assessment System for Children, second edition [92]; Screening of Emotional Problems and Child Behavior [93]; Average Kindergarten Grade in: (1) Self-knowledge and personal autonomy; (2) Environmental knowledge; (3) Languages: communication and representation. | |||
| Van de Weijer-Bergsma et al., (2012) [39] | The Dutch 10-item Non-Productive Thoughts Questionnaire for Children [94]; The Dutch 30-item Emotion Awareness Questionnaire revised [95]; The Dutch Sense of Coherence Questionnaire for Children Subjective Happiness Scale [96] | Dutch Screen for Child Anxiety-Related Emotional Disorders [97]; Social Competence and Behavior Evaluation [98]; Sleep Disturbance Scale for Children [99]; Teacher Report About Class Climate [100]; School as a Caring Community Profile II [101] | ||
| Study | Waldemar (2016) [47] | Schonert-Reichl (2015) [41] | Parker (2014) [40] | Van de Weijer-Bergsma (2012) [39] | Kielty (2017) [49] | Bradley (2018) [50] |
|---|---|---|---|---|---|---|
| Program | M-SEL | Master Mind | MindfulKids | Author Curricula Based on MindUp and MindfulSchools | The Four Pillars | |
| Theory | M-SEL: Mindfulness- Social–Emotional Learning | Positive Psychology SEL, Mindfulness (MindUp) | Mindfulness (MBSR, MBCT) | Mindfulness (MindfulSchools, MBSR, MBCT) | Mindfulness (MBSR, MBCT) | Positive Psychology, SEL, Mindfulness (MindUp) |
| Manual | Not available | Available for over 5 years | Available for over 5 years | Not available | Not available | Available less than 5 years |
| Delivery | Class by non-school trainer (therapist) | Class by non-school trainer and teachers | Class by teachers | Class by non-school trainer/authors | Class by non-school trainer/ authors | Class by teacher |
| Period/Intensity | 12 lessons—1 h long | 12 lessons, 1/week 4–50 min, daily 3 min core practice in class | 20 lessons, 4-week period, 1 lesson/day 15 min | 12 lessons, 6-week period, 2 lessons/week 30 min | 3-week period, 30 min lessons, 5 sessions, 1 booster session 1 year later | 1-year period, 20 min lesson every other week 15 lessons of Mindfulness, 10 lessons of community, 8 lessons of self-curiosity,10 lessons of contentment |
| Mindfulness | Mindfulness of breath—reflexive and playful mindfulness activities (mindfulness of eating, fishbowl technique for body awareness, mindful listening, nonjudgment/describing) & CASEL Skills (social emotional) | Breath awareness, psychoeducation, awareness of senses, home practices Kindness practices, group discussion, working on thoughts and emotions | Awareness of the body, breath and sensation, awareness of feelings, thoughts, relationships, Home practice, group discussions, mindful breathing | Bodily awareness, orienting attention, observing sounds and silence, curious attitude, awareness of breath, mindful eating, empathy, awareness of emotions and thoughts, non-judgmental awareness, being nonreactive | Psychoeducation, deep breathing and attention to thoughts, awareness of the body and of emotion | Self-awareness, mindful posture, mindfulness of breath, senses, thoughts, emotions, movement, orienting attention/concentration, self-compassion, psychoeducation |
| School and Class Climate | Safety: respect, recognizing and managing emotions, ethics, and responsibility. Community: empathy, positive relationships, collaboration. | Safety: belonging, caring. Community: understanding of others, performing acts of kindness for others, collectively engaging in community service learning activities. Academic: changing the ecology of the classroom environment, creating a positive classroom environment. | Safety: self-regulation by awareness, expression and modulation of emotion and behaviors, supportive school environment. Community: perspective taking Academic: Positive teacher–student interactions: mindful and accepting instruction giving. | Safety: respect, belonging. Community: social competence, friendly attention, friendship. Academic: class climate. Institution: student shaping of environment. | Safety: calmness, solving problems. Community: supportive relationships. | Safety: calmness, peacefulness well-being. Community: learning prosocial behaviors, altruism, empathy, compassion, forgiveness, taking perspective, self-acceptance. |
| School MBI programs—Part 2. | ||||||
| Study | Wisner (2014) [48] | Kuyken (2022) [42] | Moreno (2020) [43] | Suarez-Garcia (2020) [46] | Lombas (2019) [44] | Meyer (2020) [45] |
| Program | Mindfulness Meditation (MM) | School-Based Mindfulness Training (SBMT) | Mindkinder | Mindkeys Training | Happy Classrooms Program (HCP) | Mindful Moments Intervention |
| Theorization | MBSR | Author curricula based on MBCT-L | Author curricula based on Bakosh et al. (2015), Kabat-Zinn (2003), Gueldner & Feuerborn (2016), Carsley (2015), Poehlmann-Tynan et al. (2016) | Author curricula based on mindfulness practices and activities | Mindfulness and character strengths practices (Arguis et al. 2012) | Author curricula based on MBSR Kabat-Zinn (2003) |
| Manual | Not available | Not available | Not available | Not available | Available less than 5 years | Available than 5 years |
| Delivery | Class by mindfulness expert | Class by teachers after training | Class by a kindergarten teacher after training + assistance of an external instructor | Mindfulness daily activities by teacher after training + mindfulness expert | Class by a teacher after training | Class by teacher after training |
| Period/Intensity | 8 weeks, two to four times a week, 4-to-10 min activities | 10 lessons, 30 to 50 min each, over one school term | 6 months 6 weekly sessions of 15 min, same time and place each week. Beginning of the classes in different shifts. (4 weeks—12 h training course for teachers on mindfulness techniques) | 8 weeks, 1 h, once a week | 18 weeks, approximately 5 min, minimum periodicity of twice a week | 10-week 2 min mindfulness-based intervention 3 times a day |
| Mindfulness | Meditation in a stable posture; students were asked to observe the breath and to observe sensations in the body | Combination of psychoeducation, class discussion, and brief mindfulness practices. The program includes suggested home-based mindfulness practices at the end of each session, which are reviewed at the start of the next session | Audio-guided meditations; visualizations, using students’ imagination and their ability to abstract; visualization development of pedagogical and concentration dynamics using mandalas; corporal expression: students’ body awareness activities | Read and debate about mindfulness; breathing techniques (focusing attention); conscious attention to an activity; cultivating kindness and gratitude. (1) Sounding a singing bowl and silence; (2) Explanation of a breathing technique; (3) An attention to sound exercise; (4) Reading a story and a debate; (5) Week’s challenge; and (6) Sounding the singing bowl | Adapted meditation practices of focusing and monitoring attention, mindful movement, breathing exercises, mindful walking, body scan, mindful eating. + character strengths and well-being practices: development of appreciation of beauty, gratitude, hope, humor, and spirituality | 19 mindfulness-based movement, breathing, stretching, and body awareness exercises |
| School/ Class Climate | Safety: perceived enhancements in emotional coping reflect intrapersonal and psychosocial benefits. Calmer and more peaceful school climate with enhanced student engagement. Community: Accepting and supportive environment. Meditation helped teachers change their moods and improve stress management. Institution: perceived school climate benefits of meditation with regard to their school functioning. | Safety: better student engagement (self-efficacy) Community: teachers reported a respectful school climate, post-intervention and at 1-year follow up. Institution: better school leadership and involvement. | Safety: significant improvement in some indicators of school behavioral problems. Focusing on intrapersonal skills, such as the recognition of emotions, emotional and behavioral self-regulation, promotion of emotional well-being. Community: significant improvement in school adaptation. | Safety: Teacher and student well-being improvement, mainly through improvements in their capacity for emotional regulation and a reduction in stress. Community: Teacher stress reduction positively affects the relationship with students and classroom relationship management, contributing to an improved model of behavior for students. Academic: Available teacher training and resources of mindfulness for professional development. | Safety: potential reduction in school aggression, physical and relational. Community: improvements in relatedness. Academic: increases in factors relating to academic motivation. | Safety: higher ratings of satisfaction at post-intervention. Community: lower scores reported for friction and competitiveness, changes in reported friction and cohesion post-MBI. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monsillion, J.; Zebdi, R.; Romo-Desprez, L. School Mindfulness-Based Interventions for Youth, and Considerations for Anxiety, Depression, and a Positive School Climate—A Systematic Literature Review. Children 2023, 10, 861. https://doi.org/10.3390/children10050861
Monsillion J, Zebdi R, Romo-Desprez L. School Mindfulness-Based Interventions for Youth, and Considerations for Anxiety, Depression, and a Positive School Climate—A Systematic Literature Review. Children. 2023; 10(5):861. https://doi.org/10.3390/children10050861
Chicago/Turabian StyleMonsillion, Jessica, Rafika Zebdi, and Lucia Romo-Desprez. 2023. "School Mindfulness-Based Interventions for Youth, and Considerations for Anxiety, Depression, and a Positive School Climate—A Systematic Literature Review" Children 10, no. 5: 861. https://doi.org/10.3390/children10050861