
Beyond Screen Time: The Different Longitudinal Relations between Adolescents’ Smartphone Use Content and Their Mental Health


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.1.1. Study Design
2.1.2. Recruitment
2.1.3. Ethical Issues
2.2. Measurements
2.2.1. Demographic Information
2.2.2. Smartphone Use Content
2.2.3. Well Being
2.2.4. Covariates
2.3. Analytic Procedure
3. Results
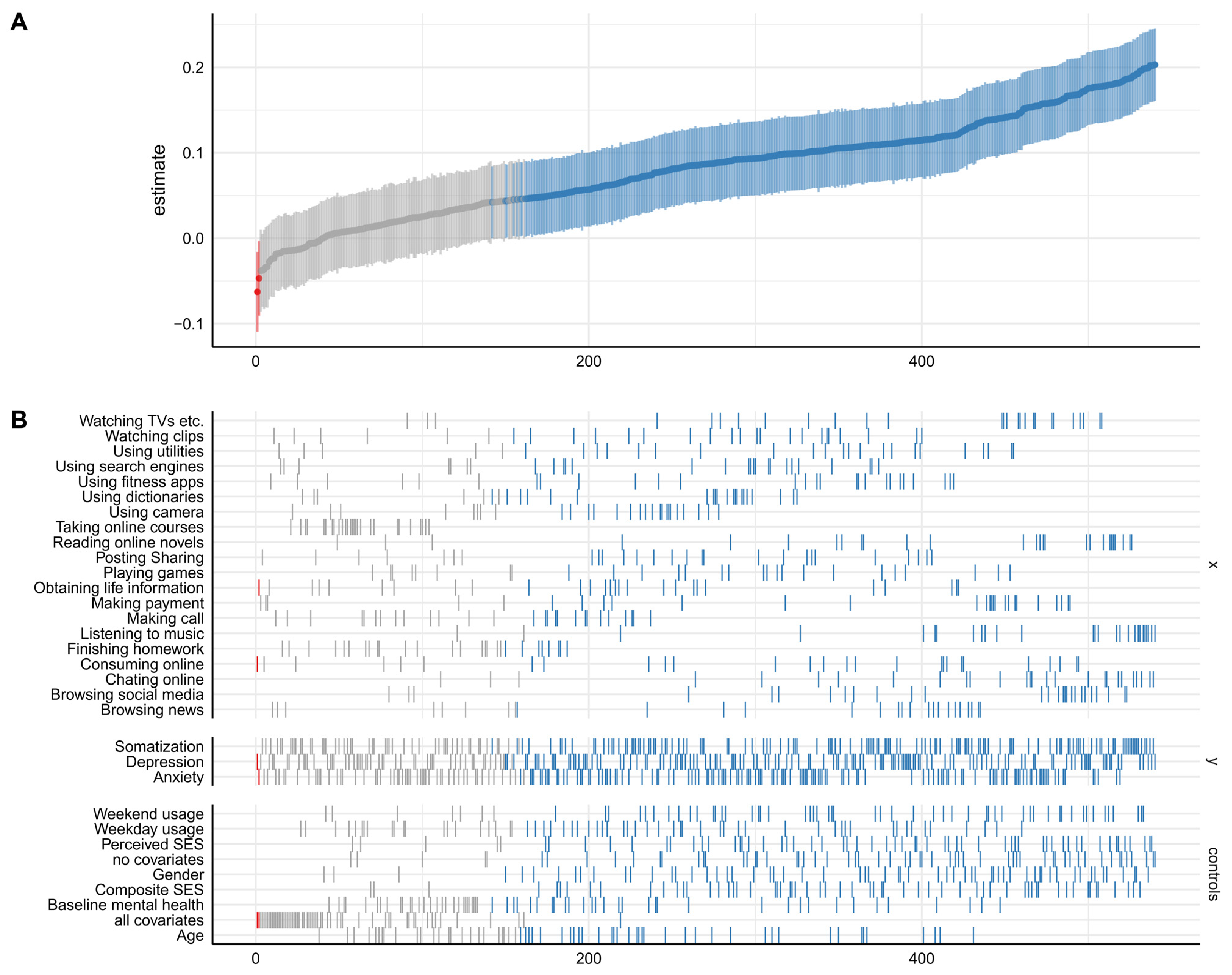
3.1. Identification of Specifications and Description of the Estimate
3.2. Statistical Inference
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statista Smartphone Users Worldwide 2016–2021. Available online: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/ (accessed on 20 March 2021).
- CNNIC. The 46th Statistical Reports on Internet Development in China; CNNIC: Beijing, China, 2020. [Google Scholar]
- Valkenburg, P.M.; Peter, J.; Schouten, A.P. Friend Networking Sites and Their Relationship to Adolescents’ Well-Being and Social Self-Esteem. Cyberpsychol. Behav. 2006, 9, 584–590. [Google Scholar] [CrossRef] [PubMed]
- George, M.J.; Jensen, M.R.; Russell, M.A.; Gassman-Pines, A.; Copeland, W.E.; Hoyle, R.H.; Odgers, C.L. Young Adolescents’ Digital Technology Use, Perceived Impairments, and Well-Being in a Representative Sample. J. Pediatr. 2020, 219, 180–187. [Google Scholar] [CrossRef]
- Orben, A.; Przybylski, A.K. The Association between Adolescent Well-Being and Digital Technology Use. Nat. Hum. Behav. 2019, 3, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Twenge, J.M. More Time on Technology, Less Happiness? Associations Between Digital-Media Use and Psychological Well-Being. Curr. Dir. Psychol. Sci. 2019, 28, 372–379. [Google Scholar] [CrossRef]
- Twenge, J.M. Why Increases in Adolescent Depression May Be Linked to the Technological Environment. Curr. Opin. Psychol. 2018, 32, 89–94. [Google Scholar] [CrossRef]
- Allen, M.S.; Vella, S.A. Screen-Based Sedentary Behaviour and Psychosocial Well-Being in Childhood: Cross-Sectional and Longitudinal Associations. Ment. Health Phys. Act. 2015, 9, 41–47. [Google Scholar] [CrossRef]
- Shakya, H.B.; Christakis, N.A. Association of Facebook Use with Compromised Well-Being: A Longitudinal Study. Am. J. Epidemiol. 2017, 185, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Riehm, K.E.; Feder, K.A.; Tormohlen, K.N.; Crum, R.M.; Young, A.S.; Green, K.M.; Pacek, L.R.; La Flair, L.N.; Mojtabai, R. Associations between Time Spent Using Social Media and Internalizing and Externalizing Problems among US Youth. JAMA Psychiatry 2019, 76, 1266–1273. [Google Scholar] [CrossRef]
- Schmiedeberg, C.; Schröder, J. Leisure Activities and Life Satisfaction: An Analysis with German Panel Data. Appl. Res. Qual. Life 2017, 12, 137–151. [Google Scholar] [CrossRef]
- Hartanto, A.; Quek, F.Y.X.; Tng, G.Y.Q.; Yong, J.C. Does Social Media Use Increase Depressive Symptoms? A Reverse Causation Perspective. Front. Psychiatry 2021, 12, 641934. [Google Scholar] [CrossRef]
- Odgers, C.L.; Jensen, M.R. Annual Research Review: Adolescent Mental Health in the Digital Age: Facts, Fears, and Future Directions. J. Child Psychol. Psychiatry Allied Discip. 2020, 61, 336–348. [Google Scholar] [CrossRef]
- George, M. The Importance of Social Media Content for Teens’ Risks for Self-Harm. J. Adolesc. Health 2019, 65, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Nesi, J.; Miller, A.B.; Prinstein, M.J. Adolescents’ Depressive Symptoms and Subsequent Technology-Based Interpersonal Behaviors: A Multi-Wave Study. J. Appl. Dev. Psychol. 2017, 51, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Aarts, A.A.; Anderson, J.E.; Anderson, C.J.; Attridge, P.R.; Attwood, A.; Axt, J.; Babel, M.; Bahník, Š.; Baranski, E.; Barnett-Cowan, M.; et al. Estimating the Reproducibility of Psychological Science. Science 2015, 349, aac4716. [Google Scholar] [CrossRef]
- Twenge, J.M.; Haidt, J.; Lozano, J.; Cummins, K.M. Specification Curve Analysis Shows That Social Media Use Is Linked to Poor Mental Health, Especially among Girls. Acta Psychol. 2022, 224, 103512. [Google Scholar] [CrossRef]
- Simonsohn, U.; Simmons, J.P.; Nelson, L.D. Specification Curve Analysis. Nat. Hum. Behav. 2020, 4, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- CNNIC. The 2019 National Study on Internet Use by Minors. Available online: http://www.cnnic.net.cn/n4/2022/0401/c116-1117.html (accessed on 20 May 2021).
- Kushlev, K. Media Technology and Well-Being: A Complementarity-Interference Model. In Handbook of Well-Being; Diener, E., Oishi, S., Tay, L., Eds.; DEF: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Kushlev, K.; Dwyer, R.; Dunn, E.W. The Social Price of Constant Connectivity: Smartphones Impose Subtle Costs on Well-Being. Curr. Dir. Psychol. Sci. 2019, 28, 347–352. [Google Scholar] [CrossRef]
- Hrastinski, S. A Theory of Online Learning as Online Participation. Comput. Educ. 2009, 52, 78–82. [Google Scholar] [CrossRef]
- Schafer, J.L.; Graham, J.W. Missing Data: Our View of the State of the Art. Psychol. Methods 2002, 7, 147–177. [Google Scholar] [CrossRef]
- Lai, X.; Nie, C.; Huang, S.; Li, Y.; Xin, T.; Zhang, C. Effect of Growth Mindset on Mental Health Two Years Later: The Role of Smartphone Use. Int. J. Environ. Res. Public Health 2022, 19, 3355. [Google Scholar] [CrossRef]
- Huang, S.; Lai, X.; Zhao, X.; Dai, X.; Yao, Y.; Zhang, C.; Wang, Y. Beyond Screen Time: Exploring the Associations between Types of Smartphone Use Content and Adolescents’ Social Relationships. Int. J. Environ. Res. Public Health 2022, 19, 8940. [Google Scholar] [CrossRef]
- Gardner, D.G.; Cummings, L.L.; Dunham, R.B.; Pierce, J.L. Single-Item versus Multiple-Item Measurement Scales: An Empirical Comparison. Educ. Psychol. Meas. 1998, 58, 898–915. [Google Scholar] [CrossRef]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for Depression in Well Older Adults: Evaluation of a Short Form of the CES-D. Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Gierk, B.; Kohlmann, S.; Kroenke, K.; Spangenberg, L.; Zenger, M.; Braḧler, E.; Loẅe, B. The Somatic Symptom Scale-8 (SSS-8): A Brief Measure of Somatic Symptom Burden. JAMA Intern. Med. 2014, 174, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.J.; Wang, L.L.; Yang, R.; Yang, X.J.; Zhang, L.G.; Guo, Z.C.; Chen, J.C.; Wang, J.Q.; Chen, J.X. Sleep Problems among Chinese Adolescents and Young Adults during the Coronavirus-2019 Pandemic. Sleep Med. 2020, 74, 39–47. [Google Scholar] [CrossRef]
- Yang, L.; Hu, Y.; Silventoinen, K.; Martikainen, P. Childhood Adversity and Depressive Symptoms among Middle-Aged and Older Chinese: Results from China Health and Retirement Longitudinal Study. Aging Ment. Health 2020, 24, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, L.; Lv, Y.; Liu, L.; Wang, Y.; Huntsinger, C.S. The Influence of Preschool Rural Migrant Composition on Rural Migrant Children’s Early Development in China. Int. J. Intercult. Relat. 2015, 49, 121–136. [Google Scholar] [CrossRef]
- Hässler, T.; Ullrich, J.; Bernardino, M.; Shnabel, N.; Van Laar, C.; Valdenegro, D.; Sebben, S.; Tropp, L.R.; Visintin, E.P.; González, R.; et al. A Large-Scale Test of the Link between Intergroup Contact and Support for Social Change. Nat. Hum. Behav. 2020, 4, 380–386. [Google Scholar] [CrossRef]
- Masur, P.K.; Scharkow, M. Specr: Statistical Functions for Conducting Specification Curve Analyses. 2020. Available online: https://masurp.github.io/specr/ (accessed on 20 May 2021).
- Orth, U.; Meier, L.L.; Bühler, J.L.; Dapp, L.C.; Krauss, S.; Messerli, D.; Robins, R.W. Effect Size Guidelines for Cross-Lagged Effects. Psychol. Methods 2022. [Google Scholar] [CrossRef]
- Orben, A.; Przybylski, A.K. Screens, Teens, and Psychological Well-Being: Evidence from Three Time-Use-Diary Studies. Psychol. Sci. 2019, 30, 682–696. [Google Scholar] [CrossRef]
- Delgado-Floody, P.; Caamaño-Navarrete, F.; Guzmán-Guzmán, I.P.; Jerez-Mayorga, D.; Martínez-Salazar, C.; Álvarez, C. Food Habits and Screen Time Play a Major Role in the Low Health Related to Quality of Life of Ethnic Ascendant Schoolchildren. Nutrients 2020, 12, 3489. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.G.; Marx, R.; Lipson, C.; Young, J. No More FOMO: Limiting Social Media Decreases Loneliness and Depression. J. Soc. Clin. Psychol. 2018, 37, 751–768. [Google Scholar] [CrossRef]
- Kim, H.H.S.; Ahn, S.J.G. How Does Neighborhood Quality Moderate the Association between Online Video Game Play and Depression? A Population-Level Analysis of Korean Students. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 628–634. [Google Scholar] [CrossRef]
- Cha, S.S.; Seo, B.K. Smartphone Use and Smartphone Addiction in Middle School Students in Korea: Prevalence, Social Networking Service, and Game Use. Health Psychol. Open 2018, 5, 2055102918755046. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H. Smartphone Use Patterns of Smartphone-Dependent Children. Child Health Nurs. Res. 2020, 26, 47–54. [Google Scholar] [CrossRef]
- Elhai, J.D.; Dvorak, R.D.; Levine, J.C.; Hall, B.J. Problematic Smartphone Use: A Conceptual Overview and Systematic Review of Relations with Anxiety and Depression Psychopathology. J. Affect. Disord. 2017, 207, 251–259. [Google Scholar] [CrossRef]
- Mesch, G.S. Parental Mediation, Online Activities, and Cyberbullying. Cyberpsychol. Behav. 2009, 12, 387–393. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Groups | Percentage (%) |
|---|---|---|
| Residence | City | 47% |
| Township | 15.3% | |
| Rural region | 37.7% | |
| Only child | Yes | 91% |
| No | 9% | |
| Mother’s education | <College | 90.5% |
| ≥College | 9.5% | |
| Father’s education | <College | 87.5% |
| ≥College | 11.4% | |
| Annual income | <50,000 ¥ 1 | 60.2% |
| 50,000–100,000 ¥ | 21.6% | |
| >100,000 ¥ | 19.2% |
| Abbreviation of SUC Items | M ± SD |
|---|---|
| 2.12 ± 0.82 |
| 2.07 ± 0.85 |
| 2.21 ± 0.80 |
| 2.16 ± 0.76 |
| 1.77 ± 0.78 |
| 2.16 ± 0.76 |
| 2.05 ± 0.70 |
| 2.28 ± 0.75 |
| 1.88 ± 0.82 |
| 1.64 ± 0.71 |
| 2.01 ± 0.83 |
| 2.17 ± 0.83 |
| 1.91 ± 0.91 |
| 2.16 ± 0.73 |
| 2.35 ± 0.89 |
| 2.06 ± 0.76 |
| 1.58 ± 0.72 |
| 2.30 ± 0.88 |
| 2.00 ± 0.83 |
| 1.99 ± 0.91 |
| Independent Variables | Median Point Estimate (β) | NSRPD |
|---|---|---|
| Watching TV, etc. | 0.14 *** | 24/27 * |
| Watching clips | 0.09 *** | 21/27 |
| Using utilities | 0.10 *** | 22/27 |
| Using search engines | 0.09 *** | 20/27 |
| Using fitness apps | 0.10 *** | 21/27 |
| Using dictionaries | 0.09 *** | 21/27 |
| Using cameras | 0.07 *** | 19/27 |
| Taking online courses | 0.01 | 0/27 |
| Reading online novels | 0.15 *** | 24/27 |
| Posting/sharing | 0.08 *** | 20/27 |
| Playing games | 0.09 *** | 19/27 * |
| Obtaining life information | 0.06 *** | 18/27 |
| Making payments | 0.14 *** | 22/27 |
| Making calls | 0.05 *** | 14/27 |
| Listening to music | 0.18 *** | 25/27 * |
| Finishing homework | 0.03 * | 8/27 |
| Consuming online | 0.10 *** | 21/27 |
| Chatting online | 0.15 *** | 24/27 * |
| Browsing social media | 0.16 *** | 24/27 |
| Browsing news | 0.11 *** | 19/27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.; Lai, X.; Li, Y.; Cui, Y.; Wang, Y. Beyond Screen Time: The Different Longitudinal Relations between Adolescents’ Smartphone Use Content and Their Mental Health. Children 2023, 10, 770. https://doi.org/10.3390/children10050770
Huang S, Lai X, Li Y, Cui Y, Wang Y. Beyond Screen Time: The Different Longitudinal Relations between Adolescents’ Smartphone Use Content and Their Mental Health. Children. 2023; 10(5):770. https://doi.org/10.3390/children10050770
Chicago/Turabian StyleHuang, Shunsen, Xiaoxiong Lai, Yajun Li, Yang Cui, and Yun Wang. 2023. "Beyond Screen Time: The Different Longitudinal Relations between Adolescents’ Smartphone Use Content and Their Mental Health" Children 10, no. 5: 770. https://doi.org/10.3390/children10050770