
Efficacy of Artificial Intelligence in the Categorisation of Paediatric Pneumonia on Chest Radiographs: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment and Risk of Bias
3. Results
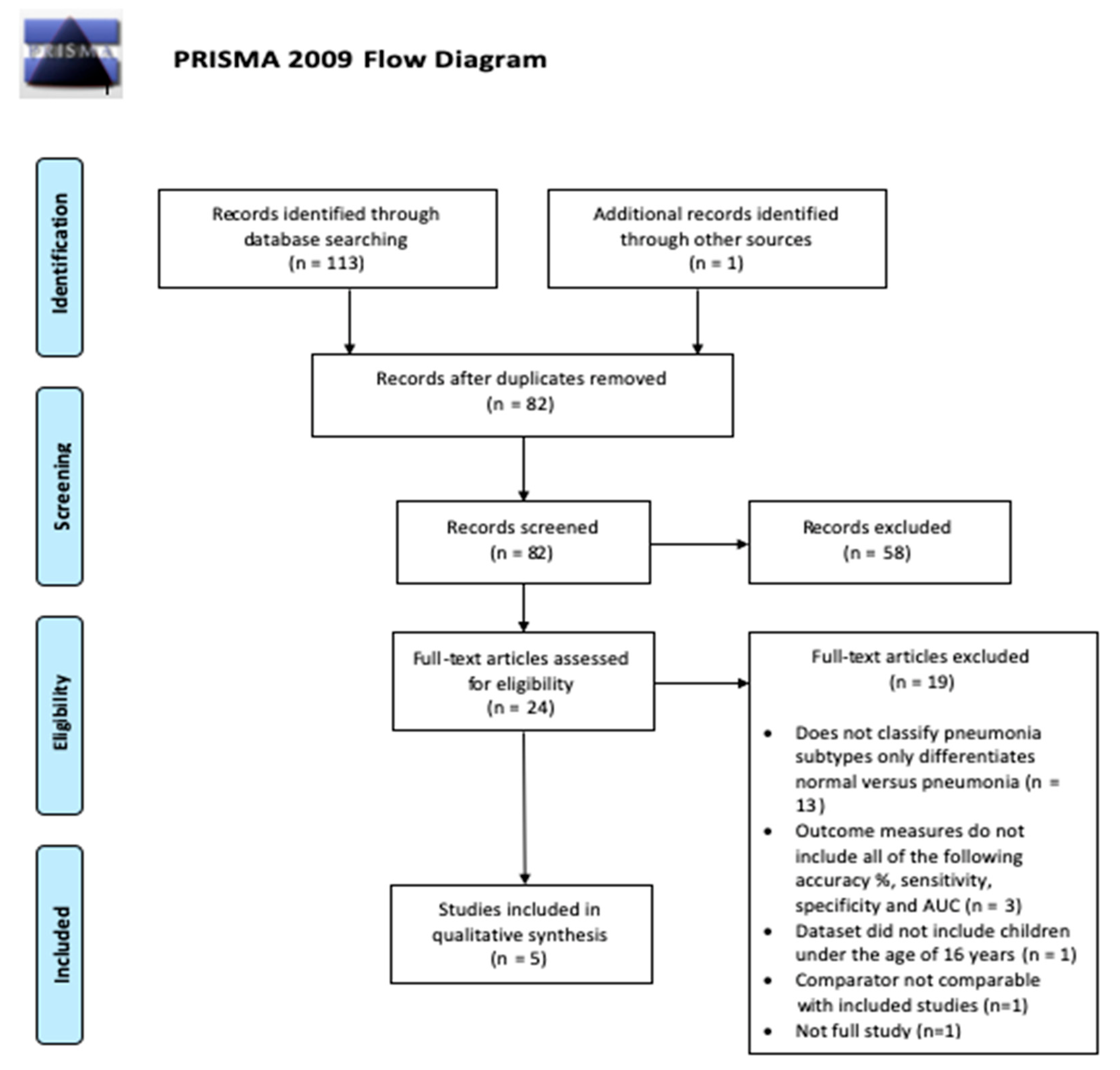
3.1. Study Selection
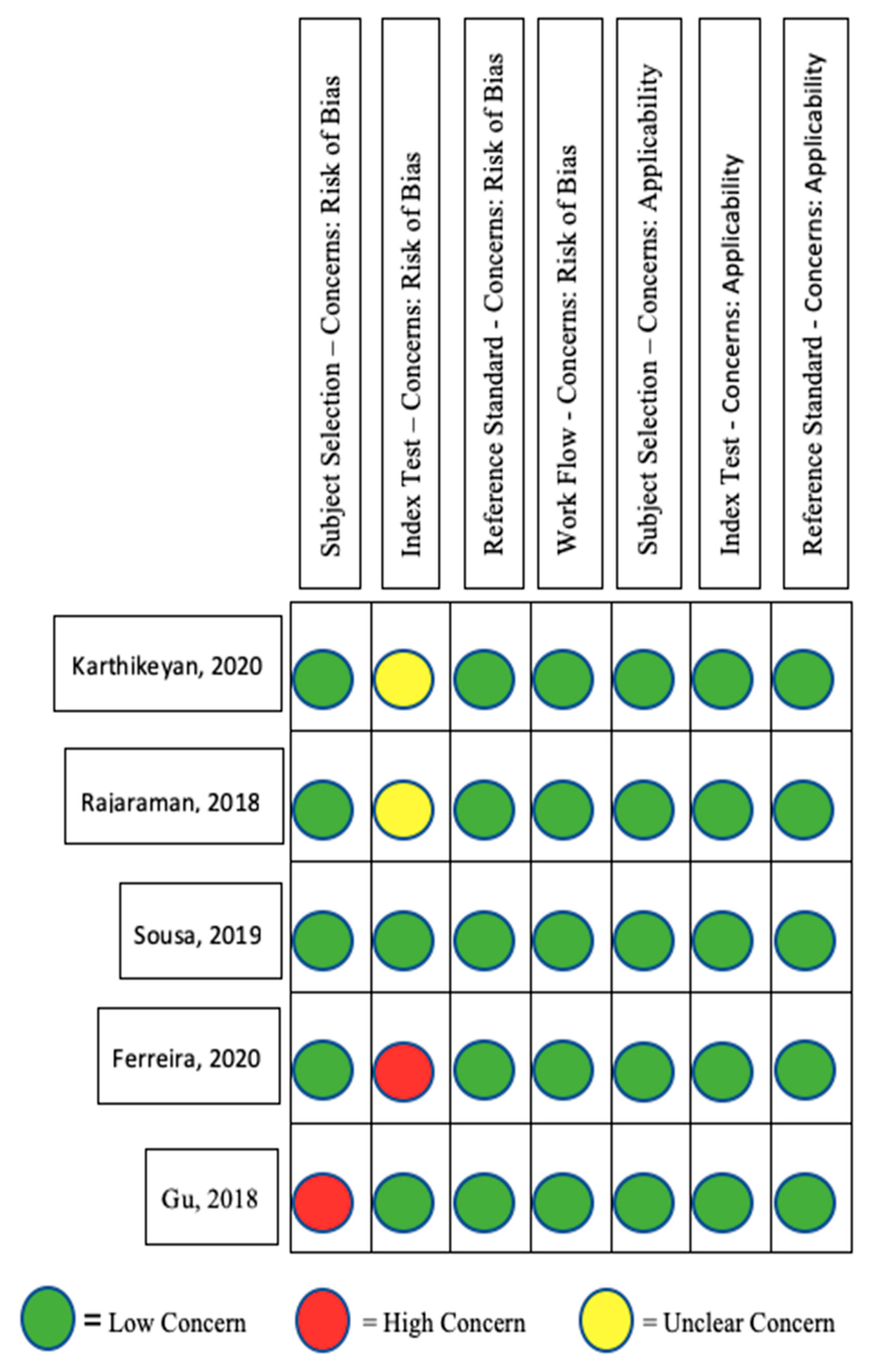
3.2. Study Quality Assessment
3.3. Study Characteristics
3.4. Diagnostic Accuracy of AI Algorithms in Distinguishing Viral Pneumonia from Bacterial Pneumonia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, B.; Kang, G.; Cheng, K.; Zhang, N. Attention-Guided Convolutional Neural Network for Detecting Pneumonia on Chest X-rays. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4851–4854. Available online: https://ieeexplore.ieee.org/document/8857277/ (accessed on 28 September 2022).
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Chumbita, M.; Cillóniz, C.; Puerta-Alcalde, P.; Moreno-García, E.; Sanjuan, G.; Garcia-Pouton, N.; Soriano, A.; Torres, A.; Garcia-Vidal, C. Can Artificial Intelligence Improve the Management of Pneumonia. J. Clin. Med. 2020, 9, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurade, A.; Dhanawade, S.; Shetti, S. Induced Sputum as a Diagnostic Tool in Pneumonia in Under Five Children—A Hospital-based Study. J. Trop. Pediatr. 2018, 64, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Rajaraman, S.; Candemir, S.; Kim, I.; Thoma, G.; Antani, S. Visualization and Interpretation of Convolutional Neural Network Predictions in Detecting Pneumonia in Pediatric Chest Radiographs. Appl. Sci. 2018, 8, 1715. [Google Scholar] [CrossRef] [Green Version]
- Franquet, T. Imaging of Community-acquired Pneumonia. J. Thorac. Imaging 2018, 33, 282–294. [Google Scholar] [CrossRef]
- Kowalski, M.L.; Agache, I.; Bavbek, S.; Bakirtas, A.; Blanca, M.; Bochenek, G.; Bonini, M.; Heffler, E.; Klimek, L.; Laidlaw, T.M.; et al. Diagnosis and management of NSAID—Exacerbated Respiratory Disease (N-ERD)—A EAACI position paper. Allergy 2019, 74, 28–39. [Google Scholar] [CrossRef] [Green Version]
- Longjiang, E.; Zhao, B.; Guo, Y.; Zheng, C.; Zhang, M.; Lin, J.; Luo, Y.; Cai, Y.; Song, X.; Liang, H. Using deep-learning techniques for pulmonary-thoracic segmentations and improvement of pneumonia diagnosis in pediatric chest radiographs. Pediatr. Pulmonol. 2019, 54, 1617–1626. [Google Scholar]
- Hurt, B.; Yen, A.; Kligerman, S.; Hsiao, A. Augmenting Interpretation of Chest Radiographs With Deep Learning Probability Maps. J. Thorac. Imaging 2020, 35, 285–293. [Google Scholar] [CrossRef]
- Smith-Bindman, R.; Lipson, J.; Marcus, R.; Kim, K.P.; Mahesh, M.; Gould, R.; Berrington de González, A.; Miglioretti, D.L. Radiation Dose Associated With Common Computed Tomography Examinations and the Associated Lifetime Attributable Risk of Cancer. Arch. Intern. Med. 2009, 169, 2078–2086. [Google Scholar] [CrossRef]
- Bolter, J.D. Turing’s Man: Western Culture in the Computer Age [Internet]; University of North Carolina Press: Chapel Hill, NC, USA, 1984; Available online: https://books.google.co.uk/books?id=4ZT6Th7CaDwC (accessed on 28 September 2022).
- Chahal, A.; Gulia, P. Machine Learning and Deep Learning. Int. J. Innov. Technol. Explor. Eng. 2019, 8, 4910–4914. [Google Scholar] [CrossRef]
- Ongsulee, P. Artificial intelligence, machine learning and deep learning. In Proceedings of the 2017 15th International Conference on ICT and Knowledge Engineering (ICT&KE) [Internet], Bangkok, Thailand, 22–24 November 2017; pp. 1–6. Available online: http://ieeexplore.ieee.org/document/8259629/ (accessed on 28 September 2022).
- Mathew, A.; Amudha, P.; Sivakumari, S. Deep Learning Techniques: An Overview. In Advanced Machine Learning Technologies and Applications [Internet]; Advances in Intelligent Systems and Computing; Hassanien, A.E., Bhatnagar, R., Darwish, A., Eds.; Springer: Singapore, 2021; Volume 1141, pp. 599–608. Available online: http://link.springer.com/10.1007/978-981-15-3383-9_54 (accessed on 28 September 2022).
- Bengio, Y. Deep Learning of Representations: Looking Forward. In Statistical Language and Speech Processing [Internet]; Lecture Notes in Computer Science; Dediu, A.H., Martín-Vide, C., Mitkov, R., Truthe, B., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; Volume 7978, pp. 1–37. Available online: http://link.springer.com/10.1007/978-3-642-39593-2_1 (accessed on 28 September 2022).
- Lodwick, G.S.; Haun, C.L.; Smith, W.E.; Keller, R.F.; Robertson, E.D. Computer Diagnosis of Primary Bone Tumors: A Preliminary Report. Radiology 1963, 80, 273–275. [Google Scholar] [CrossRef]
- Meyers, P.H.; Nice, C.M.; Becker, H.C.; Nettleton, W.J.; Sweeney, J.W.; Meckstroth, G.R. Automated Computer Analysis of Radiographic Images. Radiology 1964, 83, 1029–1034. [Google Scholar] [CrossRef]
- Winsberg, F.; Elkin, M.; Macy, J.; Bordaz, V.; Weymouth, W. Detection of Radiographic Abnormalities in Mammograms by Means of Optical Scanning and Computer Analysis. Radiology 1967, 89, 211–215. [Google Scholar] [CrossRef]
- Kruger, R.P.; Townes, J.R.; Hall, D.L.; Dwyer, S.J.; Lodwick, G.S. Automated Radiographic Diagnosis via Feature Extraction and Classification of Cardiac Size and Shape Descriptors. IEEE Trans. Biomed. Eng. 1972, 19, 174–186. [Google Scholar] [CrossRef]
- Kruger, R.P.; Thompson, W.B.; Turner, A.F. Computer Diagnosis of Pneumoconiosis. IEEE Trans. Syst. Man. Cybern. 1974, 4, 40–49. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Nishiyama, Y.; Sota, T.; Miyai, M.; Uchibe, T.; Yada, N.; Nishiyama, Y.; Kitagaki, H. Improvement in the Quantification of Striatal Tracer Uptake in Single-photon Emission Computed Tomography With 123I-ioflupane Using a Cadmium-zinc-telluride Semiconductor Camera. Shimane J. Med. Sci. 2017, 34, 35–40. [Google Scholar]
- Hadjiiski, L.; Sahiner, B.; Chan, H.-P. Advances in computer-aided diagnosis for breast cancer. Curr. Opin. Obstet. Gynecol. 2006, 18, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Hambrock, T.; Vos, P.C.; Hulsbergen–van de Kaa, C.A.; Barentsz, J.O.; Huisman, H.J. Prostate Cancer: Computer-aided Diagnosis with Multiparametric 3-T MR Imaging—Effect on Observer Performance. Radiology 2013, 266, 521–530. [Google Scholar] [CrossRef] [Green Version]
- Dromain, C.; Boyer, B.; Ferré, R.; Canale, S.; Delaloge, S.; Balleyguier, C. Computed-aided diagnosis (CAD) in the detection of breast cancer. Eur. J. Radiol. 2013, 82, 417–423. [Google Scholar] [CrossRef]
- Firmino, M.; Morais, A.H.; Mendoça, R.M.; Dantas, M.R.; Hekis, H.R.; Valentim, R. Computer-aided detection system for lung cancer in computed tomography scans: Review and future prospects. Biomed. Eng. Online 2014, 13, 41. [Google Scholar] [CrossRef] [Green Version]
- Mosquera-Lopez, C.; Agaian, S.; Velez-Hoyos, A.; Thompson, I. Computer-aided prostate cancer diagnosis from digitized histopathology: A review on texture-based systems. IEEE Rev. Biomed. Eng. 2014, 8, 98–113. [Google Scholar] [CrossRef] [PubMed]
- El Abbadi, N.K.; AL, J.; Taee, E. Breast Cancer Diagnosis by CAD. Int. J. Comput. Appl. 2014, 100, 25–29. [Google Scholar]
- Brown, M.S.; Lo, P.; Goldin, J.; Barnoy, E.; Kim, G.H.J.; McNItt-Gray, M.; Aberle, D.R. Toward clinically usable CAD for lung cancer screening with computed tomography. Eur. Radiol. 2014, 24, 2719–2728. [Google Scholar] [CrossRef] [PubMed]
- Mittal, A.; Kaur, M. Computer-aided-diagnosis in colorectal cancer: A survey of state of the art techniques. In Proceedings of the 2016 International Conference on Inventive Computation Technologies (ICICT), Coimbatore, India, 26–27 August 2016. [Google Scholar]
- Shariaty, F.; Mousavi, M. Application of CAD systems for the automatic detection of lung nodules. Inform. Med. Unlocked 2019, 15, 100173. [Google Scholar] [CrossRef]
- Chan, H.P.; Samala, R.K.; Hadjiiski, L.M. CAD and AI for breast cancer—Recent development and challenges. Br. J. Radiol. 2020, 93, 20190580. [Google Scholar] [CrossRef]
- Oliveira, S.P.; Neto, P.C.; Fraga, J.; Montezuma, D.; Monteiro, A.; Monteiro, J.; Ribeiro, L.; Gonçalves, S.; Pinto, I.M.; Cardoso, J.S. CAD systems for colorectal cancer from WSI are still not ready for clinical acceptance. Sci. Rep. 2021, 11, 14358. [Google Scholar] [CrossRef]
- Porto-Álvarez, J.; Barnes, G.T.; Villanueva, A.; García-Figueiras, R.; Baleato-González, S.; Zapico, E.H.; Souto-Bayarri, M. Digital Medical X-ray Imaging, CAD in Lung Cancer and Radiomics in Colorectal Cancer: Past, Present and Future. Appl. Sci. 2023, 13, 2218. [Google Scholar] [CrossRef]
- European Society of Radiology (ESR). What the radiologist should know about artificial intelligence—An ESR white paper. Insights Imaging 2019, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Frija, G.; Blažić, I.; Frush, D.P.; Hierath, M.; Kawooya, M.; Donoso-Bach, L.; Brkljačić, B. How to improve access to medical imaging in low- and middle-income countries ? Eclinicalmedicine 2021, 38, 101034. [Google Scholar] [CrossRef]
- Legido-Quigley, H.; Doering, N.; McKee, M. Challenges facing teleradiology services across borders in the European union: A qualitative study. Health Policy Technol. 2014, 3, 160–166. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Son, J.; Shin, J.Y.; Kim, H.D.; Jung, K.-H.; Park, K.H.; Park, S.J. Development and Validation of Deep Learning Models for Screening Multiple Abnormal Findings in Retinal Fundus Images. Ophthalmology 2020, 127, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Grewal, M.; Srivastava, M.M.; Kumar, P.; Varadarajan, S. RADnet: Radiologist level accuracy using deep learning for hemorrhage detection in CT scans. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 281–284. Available online: https://ieeexplore.ieee.org/document/8363574/ (accessed on 28 September 2022).
- Stephen, O.; Sain, M.; Maduh, U.J.; Jeong, D.-U. An Efficient Deep Learning Approach to Pneumonia Classification in Healthcare. J. Healthc. Eng. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Siddhartha, M.A.I. Versus M.D.—What happens when diagnosis is automated? The New Yorker, 27 March 2017; Annals of Medicine. [Google Scholar]
- The Economist. Images Aren’t Everything. Economists, 9 June 2018; Leaders Section. Available online: https://www.economist.com/leaders/2018/06/07/ai-radiology-and-the-future-of-work (accessed on 28 September 2022).
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.S.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying Medical Diagnoses and Treatable Diseases by Image-Based Deep Learning. Cell 2018, 172, 1122–1131.e9. [Google Scholar] [CrossRef]
- Gu, X.; Pan, L.; Liang, H.; Yang, R. Classification of Bacterial and Viral Childhood Pneumonia Using Deep Learning in Chest Radiography. In Proceedings of the 3rd International Conference on Multimedia and Image Processing—ICMIP 2018 [Internet], Guiyang, China, 16–18 March 2018; ACM Press: New York, NY, USA, 2018. Available online: http://dl.acm.org/citation.cfm?doid=3195588.3195597 (accessed on 28 September 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions [Internet], Version 6.3; Cochrane, 2022; Available online: www.training.cochrane.org/handbook (accessed on 28 September 2022).
- Critical Appraisal Skills Programme. CASP Diagnostic Study Checklist [Internet]. 2022. Available online: https://casp-uk.net/images/checklist/documents/CASP-Diagnostic-Study-Checklist/CASP-Diagnostic-Checklist-2018_fillable_form.pdf (accessed on 28 September 2022).
- Hung, K.; Montalvao, C.; Tanaka, R.; Kawai, T.; Bornstein, M.M. The use and performance of artificial intelligence applications in dental and maxillofacial radiology: A systematic review. Dentomaxillofac. Radiol. 2020, 49, 20190107. [Google Scholar] [CrossRef]
- Karthikeyan, M.P. An Efficient Deep Learning Approach to Pneumonia Classification in Healthcare. Int. J. Adv. Res. Sci. Technol. IJARST 2019, 2019, 4180949. Available online: https://ijarsct.co.in/Paper158.pdf (accessed on 28 September 2022).
- Ferreira, J.R.; Armando Cardona Cardenas, D.; Moreno, R.A.; de Fatima de Sa Rebelo, M.; Krieger, J.E.; Antonio Gutierrez, M. Multi-View Ensemble Convolutional Neural Network to Improve Classification of Pneumonia in Low Contrast Chest X-ray Images. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC) [Internet], Montreal, QC, Canada, 11 July 2020; pp. 1238–1241. Available online: https://ieeexplore.ieee.org/document/9176517/ (accessed on 28 September 2022).
- Sousa, G.G.B.; Fernandes, V.R.M.; de Paiva, A.C. Optimized Deep Learning Architecture for the Diagnosis of Pneumonia Through Chest X-rays. In Image Analysis and Recognition; Lecture Notes in Computer Science; Karray, F., Campilho, A., Yu, A., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; Volume 11663, pp. 353–361. Available online: http://link.springer.com/10.1007/978-3-030-27272-2_31 (accessed on 28 September 2022).
- Hoo, Z.H.; Candlish, J.; Teare, D. What is an ROC curve? Emerg. Med. J. 2017, 34, 357. [Google Scholar] [CrossRef] [Green Version]
- O’Grady, K.A.F.; Torzillo, P.J.; Frawley, K.; Chang, A.B. The radiological diagnosis of pneumonia in children. Pneumonia 2014, 5, 38–51. [Google Scholar] [CrossRef] [Green Version]
- McAllister, D.A.; Liu, L.; Shi, T.; Chu, Y.; Reed, C.; Burrows, J.; Adeloye, D.; Rudan, I.; Black, R.E.; Campbell, H.; et al. Global, regional, and national estimates of pneumonia morbidity and mortality in children younger than 5 years between 2000 and 2015: A systematic analysis. Lancet Glob. Health 2018, 7, e47–e57. [Google Scholar] [CrossRef] [Green Version]
- GBD 2015. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1133–1161. [Google Scholar] [CrossRef] [Green Version]
- Longjiang, E.; Zhao, B.; Liu, H.; Zheng, C.; Song, X.; Cai, Y.; Liang, H. Image-based deep learning in diagnosing the etiology of pneumonia on pediatric chest X-rays. Pediatr. Pulmonol. 2021, 56, 1036–1044. [Google Scholar]
- Shelmerdine, S.C.; Martin, H.; Shirodkar, K.; Shamshuddin, S.; Weir-McCall, J.R. Can artificial intelligence pass the Fellowship of the Royal College of Radiologists examination? Multi-reader diagnostic accuracy study. BMJ 2022, 379, e072826. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.Y.; Ramamurthy, N. A career in radiology. BMJ 2012, 345, e8142. [Google Scholar] [CrossRef]
- Gertych, A.; Zhang, A.; Sayre, J.; Pospiech-Kurkowska, S.; Huang, H. Bone age assessment of children using a digital hand atlas. Comput. Med. Imaging Graph. 2007, 31, 322–331. [Google Scholar] [CrossRef] [Green Version]
- Rajpurkar, P.; Irvin, J.; Bagul, A.; Ding, D.; Duan, T.; Mehta, H.; Yang, B.; Zhu, K.; Laird, D.; Ball, L.R.; et al. Mura: Large dataset for abnormality detection in musculoskeletal radiographs. arXiv 2017, arXiv:171206957. [Google Scholar]
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R.M. ChestX-Ray8: Hospital-Scale Chest X-Ray Database and Benchmarks on Weakly-Supervised Classification and Localization of Common Thorax Diseases. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR) [Internet], Honolulu, HI, USA, 21–26 July 2017; pp. 3462–3471. Available online: http://ieeexplore.ieee.org/document/8099852/ (accessed on 28 September 2022).
- Irvin, J.; Rajpurkar, P.; Ko, M.; Yu, Y.; Ciurea-Ilcus, S.; Chute, C.; Marklund, H.; Haghgoo, B.; Ball, R.; Shpanskaya, K.; et al. Chexpert: A large chest radiograph dataset with uncertainty labels and expert comparison. In Proceedings of the AAAI Conference on Artificial Intelligence, Honolulu, HA, USA, 27 January–1 February 2019; Volume 33, pp. 590–597. [Google Scholar]
- Johnson, A.E.; Pollard, T.J.; Berkowitz, S.J.; Greenbaum, N.R.; Lungren, M.P.; Deng, C.Y.; Mark, R.G.; Horng, S. MIMIC-CXR, a de-identified publicly available database of chest radiographs with free-text reports. Sci. Data 2019, 6, 317. [Google Scholar] [CrossRef] [Green Version]
- Halabi, S.S.; Prevedello, L.; Kalpathy-Cramer, J.; Mamonov, A.B.; Bilbily, A.; Cicero, M.; Pan, I.; Pereira, L.A.; Sousa, R.; Abdala, N.; et al. The RSNA pediatric bone age machine learning challenge. Radiology 2019, 290, 498–503. [Google Scholar] [CrossRef]
- Bustos, A.; Pertusa, A.; Salinas, J.M.; de la Iglesia-Vayá, M. PadChest: A large chest X-ray image dataset with multi-label annotated reports. Med. Image Anal. 2020, 66, 101797. [Google Scholar] [CrossRef]
- Selby, I. Automated Quality Control of Chest X-ray [Internet]. Oral Presentation Presented at: European Congress of Radiology 3 March 2023; Vienna. Available online: https://connect.myesr.org/?esrc_course=using-ai-for-quality-control-in-radiography (accessed on 28 September 2022).
- Ying, X. An Overview of Overfitting and its Solutions. J. Phys. Conf. Ser. 2019, 1168, 022022. [Google Scholar] [CrossRef]
- Whiteson, S.; Tanner, B.; Taylor, M.E.; Stone, P. Protecting against evaluation overfitting in empirical reinforcement learning. In Proceedings of the 2011 IEEE Symposium on Adaptive Dynamic Programming and Reinforcement Learning (ADPRL), Paris, France, 12–14 April 2011; pp. 120–127. Available online: http://ieeexplore.ieee.org/document/5967363/ (accessed on 28 September 2022).
- Dietterich, T. Overfitting and undercomputing in machine learning. ACM Comput. Surv. CSUR 1995, 27, 326–327. [Google Scholar] [CrossRef]
- Mutasa, S.; Sun, S.; Ha, R. Understanding artificial intelligence based radiology studies: What is overfitting? Clin. Imaging 2020, 65, 96–99. [Google Scholar] [CrossRef]
- Anderson, D.; Burnham, K. Model Selection and Multi-Model Inference, 2nd ed.; Springer: New York, NY, USA, 2004; Volume 63, p. 10. [Google Scholar]
- England, J.R.; Cheng, P.M. Artificial intelligence for medical image analysis: A guide for authors and reviewers. Am. J. Roentgenol. 2019, 212, 513–519. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, X.; Tang, X. Deep Learning Face Representation from Predicting 10,000 Classes. In Proceedings of the 2014 IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 1891–1898. [Google Scholar]
- Gonçalves, I.; Silva, S.; Melo, J.B.; Carreiras, J.M.B. Random Sampling Technique for Overfitting Control in Genetic Programming. In Genetic Programming; Moraglio, A., Silva, S., Krawiec, K., Machado, P., Cotta, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 218–229. [Google Scholar]
- Parmar, C.; Barry, J.D.; Hosny, A.; Quackenbush, J.; Aerts, H.J.W.L. Data Analysis Strategies in Medical Imaging. Clin. Cancer Res. 2018, 24, 3492–3499. [Google Scholar] [CrossRef] [Green Version]
- Chartrand, G.; Cheng, P.M.; Vorontsov, E.; Drozdzal, M.; Turcotte, S.; Pal, C.J.; Kadoury, S.; Tang, A. Deep Learning: A Primer for Radiologists. RadioGraphics 2017, 37, 2113–2131. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Into Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; MacKinnon, T. Artificial intelligence in fracture detection: Transfer learning from deep convolutional neural networks. Clin. Radiol. 2018, 73, 439–445. [Google Scholar] [CrossRef]
- Ha, R.; Mutasa, S.; Karcich, J.; Gupta, N.; Pascual Van Sant, E.; Nemer, J.; Sun, M.; Chang, P.; Liu, M.Z.; Jambawalikar, S. Predicting Breast Cancer Molecular Subtype with MRI Dataset Utilizing Convolutional Neural Network Algorithm. J. Digit. Imaging 2019, 32, 276–282. [Google Scholar] [CrossRef]
- Fry, H. Hello World: How to Be Human in the Age of the Machine [Internet]; Transworld, 2018; Available online: https://books.google.co.uk/books?id=72FCDwAAQBAJ (accessed on 28 September 2022).



{kind=link}
{kind=link}
| Author, Year | Algorithm Employed | Type of AI | Age of Participants (Years) | No. of Images (by Aetiology) | No. of Images Used in | Pre-Processing Methods | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normal | Pneumonia | Total | Training | Validation | Testing | |||||||
| Bacterial | Viral | Total | ||||||||||
| Gu et al., 2018 [44] |
| DL | 5.5 ± 4.2 | 0 | 2665 | 1848 | 4513 | 4513 | 3211 | 802 | 500 |
|
| Ferreira et al., 2020 [50] |
| DL | 1–5 | 1349 | 2538 | 1345 | 3883 | 5232 | 5232 | 0 | 624 |
|
| Sousa et al., 2019 [51] |
| DL | 1–5 | 1349 | 2538 | 1345 | 3883 | 5232 | 624 | 0 | 624 |
|
| Rajaraman et al., 2018 [5] |
| DL | 1–5 | 1349 | 2538 | 1345 | 3883 | 5232 | 5232 | 0 | 624 |
|
| Karthikeyan 2020 [49] |
| DL | 1–5 | 1341 | 2561 | 1345 | 3906 | 5247 | 4500 | 0 | 398 |
|
| Author, Year | Algorithm | Sensitivity | Specificity | Accuracy | AUC |
|---|---|---|---|---|---|
| Gu et al., 2018 [44] | AlexNet (DCNN ONLY) | 0.6322 ± 0.0023 | 0.7072 ± 0.0023 | 0.7360 ± 0.0023 | 0.7384 ± 0.0023 |
| GLCM Features | 0.6378 ± 0.0058 | 0.8980 ± 0.0062 | 0.7060 ± 0.0672 | 0.7060 | |
| Wavelet Features | 0.5612 ± 0.0065 | 0.8779 ± 0.0205 | 0.6769 ± 0.0100 | 0.6769 | |
| HOG Features | 0.5714 ± 0.0617 | 0.8651 ± 0.0664 | 0.7511 ± 0.0127 | 0.6930 | |
| All Handcrafted Features | 0.6213 ± 0.0482 | 0.8848 ± 0.0387 | 0.7640 ± 0.0330 | 0.7200 ± 0.0060 | |
| Fused Features (DCNN + all handcrafted features) | 0.5567 ± 0.0379 | 0.9267 ± 0.0301 | 0.7692 ± 0.0122 | 0.8234 ± 0.0014 | |
| Ferreira et al., 2020 [50] | VGG16 and Baseline Set | Not Stated | Not Stated | Not Stated | 0.85 |
| VGG16 and Set A | Not Stated | Not Stated | Not Stated | 0.88 | |
| VGG16 and Set B | Not Stated | Not Stated | Not Stated | 0.83 | |
| VGG16 and Set C (ensemble set) | 0.963 | 0.851 | 0.921 | 0.91 | |
| Inception V3 architecture | 0.886 | 0.909 | 0.907 | 0.940 | |
| Sousa et al., 2019 [51] | ‘Best generated model’ | 0.913 | 0.696 | 0.831 | 0.831 |
| Inception V3 architecture | 0.886 | 0.909 | 0.907 | 0.940 | |
| Rajaraman et al., 2018 [5] | Sequential CNN—Baseline | Not specified | 0.838 | 0.928 | 0.954 |
| Residual CNN—Baseline | Not specified | 0.784 | 0.897 | 0.921 | |
| Inception CNN—Baseline | Not specified | 0.714 | 0.854 | 0.901 | |
| Customised VGG16—Baseline | Not specified | 0.860 | 0.936 | 0.962 | |
| Sequential CNN—Cropped | Not specified | 0.838 | 0.928 | 0.956 | |
| Residual CNN—Cropped | Not specified | 0.798 | 0.908 | 0.933 | |
| Inception CNN—Cropped | Not specified | 0.730 | 0.872 | 0.919 | |
| Customised VGG16—Cropped | Not specified | 0.860 | 0.936 | 0.962 | |
| Karthikeyan, 2020 [49] | AlexNet | 0.94 | 0.845 | 0.90 | 0.89 |
| ResNet18 | 0.92 | 0.82 | 0.87 | 0.87 | |
| DenseNet201 | 0.96 | 0.94 | 0.95 | 0.952 | |
| SqueezeNet | 0.905 | 0.75 | 0.83 | 0.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Field, E.L.; Tam, W.; Moore, N.; McEntee, M. Efficacy of Artificial Intelligence in the Categorisation of Paediatric Pneumonia on Chest Radiographs: A Systematic Review. Children 2023, 10, 576. https://doi.org/10.3390/children10030576
Field EL, Tam W, Moore N, McEntee M. Efficacy of Artificial Intelligence in the Categorisation of Paediatric Pneumonia on Chest Radiographs: A Systematic Review. Children. 2023; 10(3):576. https://doi.org/10.3390/children10030576
Chicago/Turabian StyleField, Erica Louise, Winnie Tam, Niamh Moore, and Mark McEntee. 2023. "Efficacy of Artificial Intelligence in the Categorisation of Paediatric Pneumonia on Chest Radiographs: A Systematic Review" Children 10, no. 3: 576. https://doi.org/10.3390/children10030576