
Single-Stage Tibial Osteotomy for Correction of Genu Varum Deformity in Children
Abstract
:1. Introduction
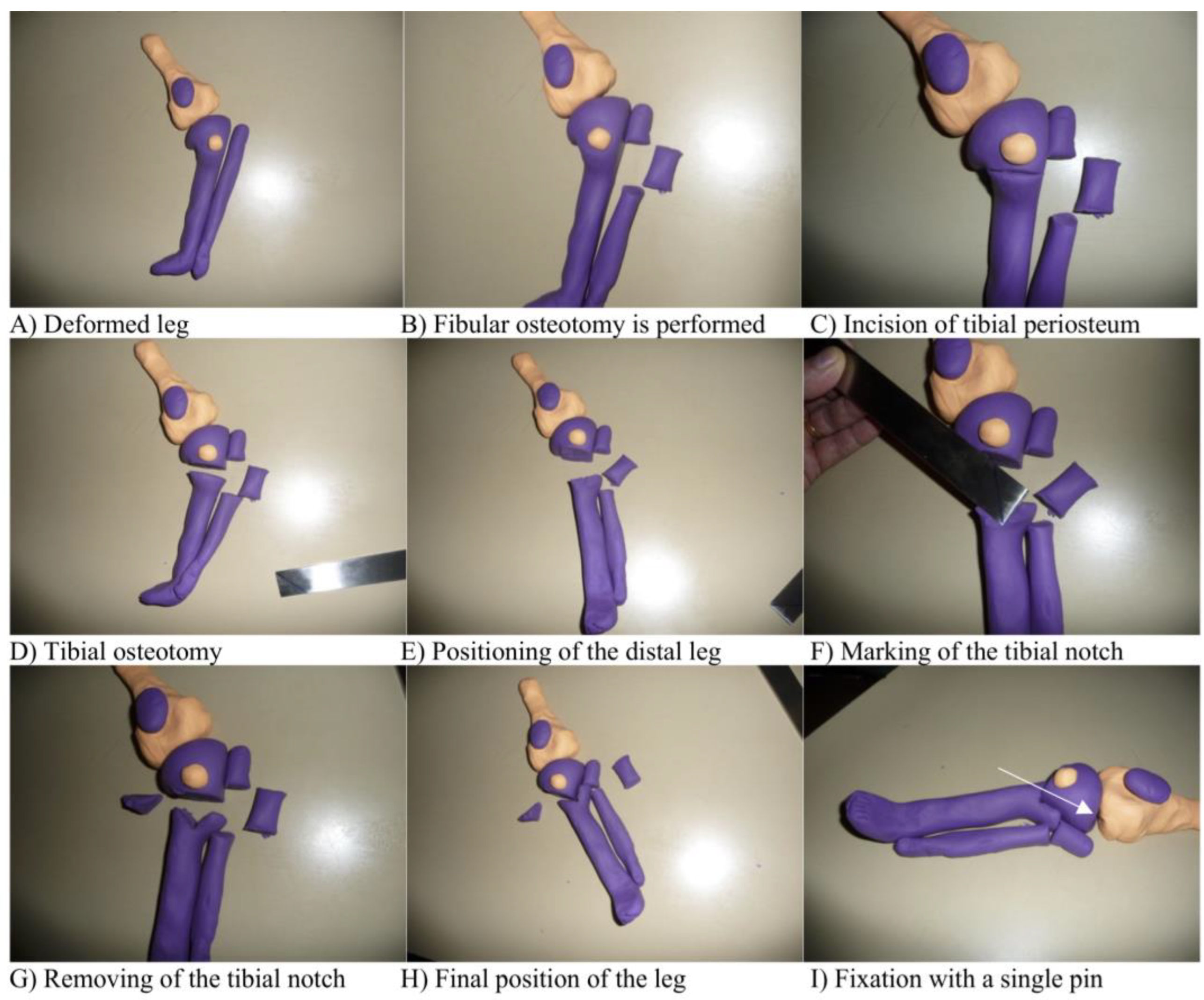
2. Materials and Methods
3. Results
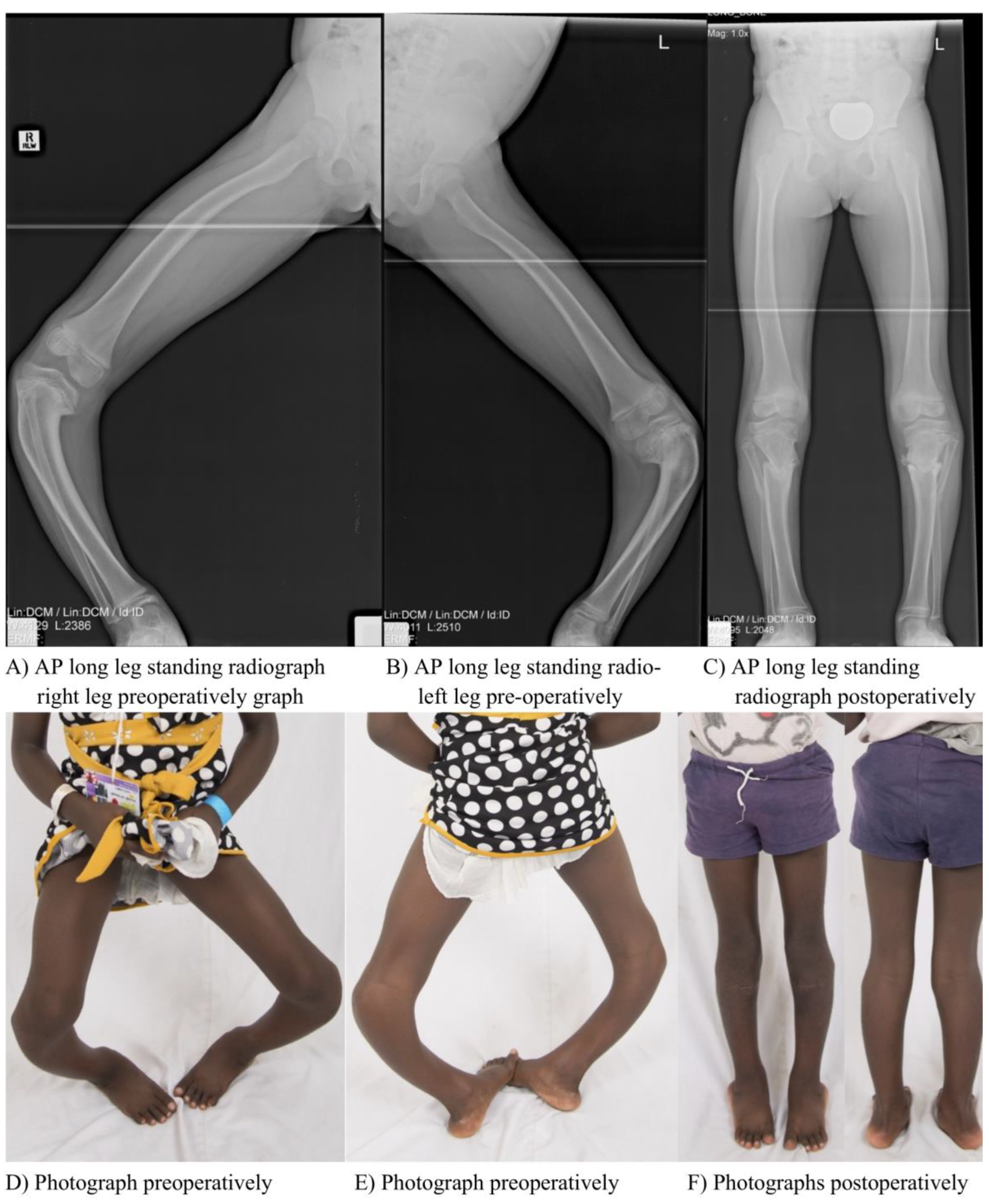
3.1. Clinical Results
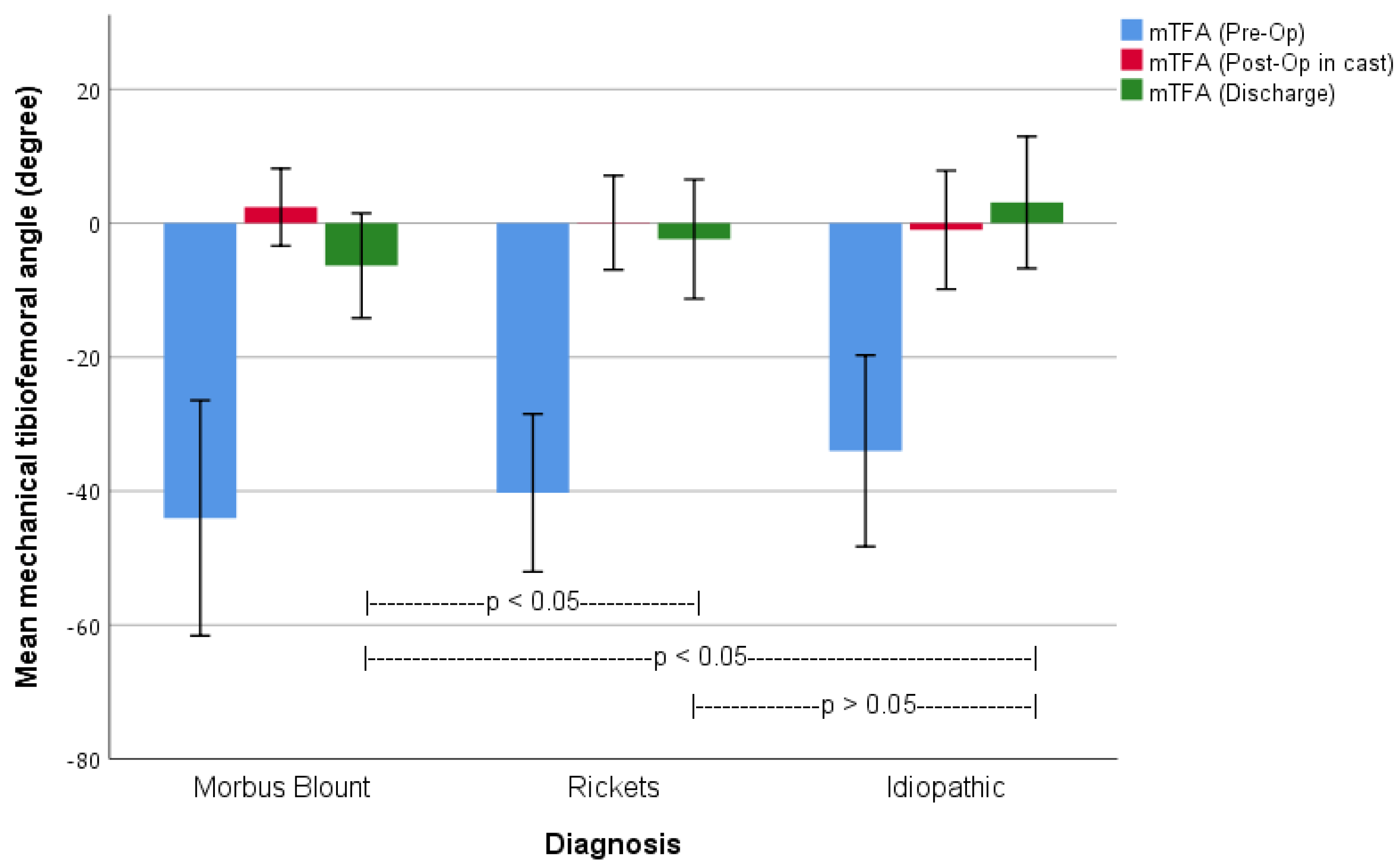
3.2. Radiographic Outcomes
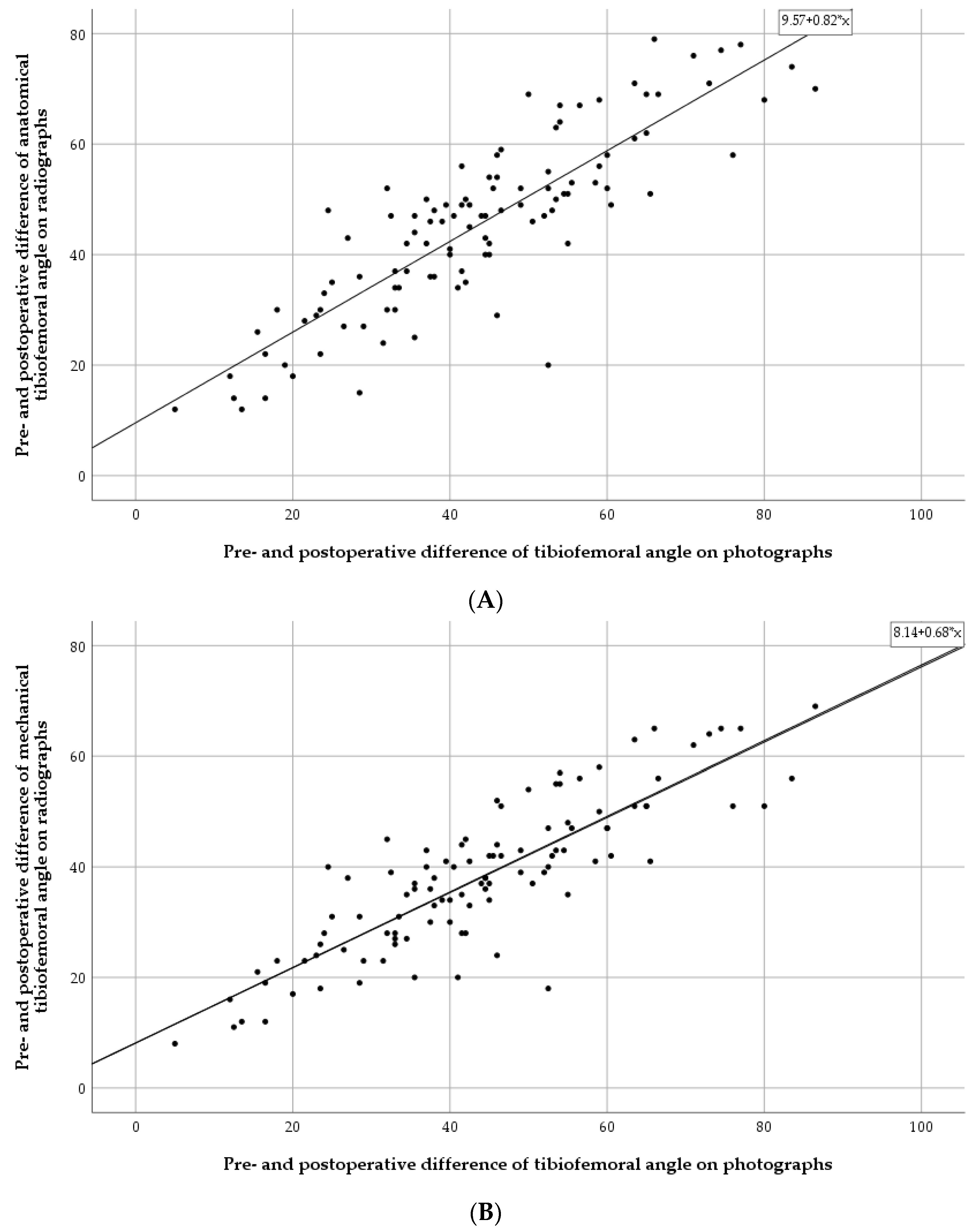
3.3. Photographic Measurements
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Study Approval of the Institutional Review Board of the NGO Mercy Ships

Appendix B. Patient Questionnaire Completed by Each Patient

Appendix C. Functional Assessment Completed for Each Patient by the Treating Physiotherapist

References
- Hefti, F. Kinderorthopädie in Der Praxis; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Hefti, F. Deviations in the axes of the lower extremities. Orthopäde 2000, 29, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Greene, W.B. Infantile tibia vara. J. Bone Jt. Surg. Am. 1993, 75, 130–143. [Google Scholar] [CrossRef]
- Sabharwal, S. Blount disease. J. Bone Jt. Surg. Am. 2009, 91, 1758–1776. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A. Nutritional rickets around the world. J. Steroid Biochem. Mol. Biol. 2013, 136, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, V.S.; Freeman, R.; Greenwood, C.L.; Summers, D.M.; Nigdikar, S.; Lavy, C.B.D.; Offiah, A.C.; Bishop, N.J.; Cashman, J.; Prentice, A. The aetiology of rickets-like lower limb deformities in Malawian children. Osteoporos. Int. 2016, 27, 2367–2372. [Google Scholar] [CrossRef]
- Catonné, Y. La maladie de Blount. In Cahiers D’Enseignement de la Société Française D’Orthopédie ET Traumatologie; Elsevier: Paris, France, 1997; pp. 147–163. [Google Scholar]
- Janoyer, M. Blount disease. Orthop. Traumatol. Surg. Res. 2019, 105, S111–S121. [Google Scholar] [CrossRef]
- Richards, B.S.; Katz, D.E.; Sims, J.B. Effectiveness of brace treatment in early infantile Blount’s disease. J. Pediatr. Orthop. 1998, 18, 374–380. [Google Scholar] [CrossRef]
- Sabharwal, S.; Lee, J., Jr.; Zhao, C. Multiplanar deformity analysis of untreated Blount disease. J. Pediatr. Orthop. 2007, 27, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, Y.; Kamegaya, M.; Kuniyoshi, K.; Moriya, H. Natural history of infantile tibia vara. J. Bone Jt. Surg. Br. 2002, 84, 263–268. [Google Scholar] [CrossRef]
- Loder, R.T.; Johnston, C.E., 2nd. Infantile tibia vara. J. Pediatr. Orthop. 1987, 7, 639–646. [Google Scholar] [CrossRef]
- Creo, A.L.; Thacher, T.D.; Pettifor, J.M.; Strand, M.A.; Fischer, P.R. Nutritional rickets around the world: An update. Paediatr. Int. Child Health 2017, 37, 84–98. [Google Scholar] [CrossRef]
- Ghanem, I.; Karam, J.A.; Widmann, R.F. Surgical epiphysiodesis indications and techniques: Update. Curr. Opin. Pediatr. 2011, 23, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.; Chmiel, J.S.; Almagor, O.; Felson, D.; Guermazi, A.; Roemer, F.; Lewis, C.E.; Segal, N.; Torner, J.; Cooke, T.D.; et al. The role of varus and valgus alignment in the initial development of knee cartilage damage by MRI: The Most study. Ann. Rheum. Dis. 2013, 72, 235–240. [Google Scholar] [CrossRef]
- Bowen, J.R.; Leahey, J.L.; Zhang, Z.-H.; Macewen, G.D. Partial epiphysiodesis at the knee to correct angular deformity. Clin. Orthop. Relat. Res. 1985, 198, 184–190. [Google Scholar] [CrossRef]
- Stevens, P.M. Guided growth for angular correction: A preliminary series using a tension band plate. J. Pediatr. Orthop. 2007, 27, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Vogt, B.; Schiedel, F.; Rodl, R. Guided growth in children and adolescents: Correction of leg length discrepancies and leg axis deformities. Orthopäde 2014, 43, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Rab, G.T. Oblique tibial osteotomy for Blount’s disease (tibia vara). J. Pediatr. Orthop. 1988, 8, 715–720. [Google Scholar] [CrossRef]
- Gilbody, J.; Thomas, G.; Ho, K. Acute versus gradual correction of idiopathic tibia vara in children: A systematic review. J. Pediatr. Orthop. 2009, 29, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.S.; Madan, S.S.; Ruchelsman, D.E.; Sala, D.A.; Lehman, W.B. Accuracy of correction of tibia vara: Acute versus gradual correction. J. Pediatr. Orthop. 2006, 26, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Phedy, P.; Siregar, P.U. Osteotomy for deformities in blount disease: A systematic review. J. Orthop. 2016, 13, 207–209. [Google Scholar] [CrossRef] [Green Version]
- Coogan, P.G.; Fox, J.A.; Fitch, R.D. Treatment of adolescent Blount disease with the circular external fixation device and distraction osteogenesis. J. Pediatr. Orthop. 1996, 16, 450–454. [Google Scholar] [CrossRef]
- Khanfour, A.A.; El-Rosasy, M. Late onset tibia vara. Acute correction strategy: Proper case selection and a simple external fixation technique. Acta Orthop. Belg. 2014, 80, 241–250. [Google Scholar]
- El-Rosasy, M.; Ayoub, M. Acute correction of proximal tibial deformities in adolescents using Ilizarov external fixator: Focal-dome versus straight-cut osteotomy. J. Pediatr. Orthop. B 2007, 16, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Rab, G.T. Oblique tibial osteotomy revisited. J. Child. Orthop. 2010, 4, 169–172. [Google Scholar] [CrossRef]
- Davis, C.A.; Maranji, K.; Frederick, N.; Dorey, F.; Moseley, C.F. Comparison of crossed pins and external fixation for correction of angular deformities about the knee in children. J. Pediatr. Orthop. 1998, 18, 502–507. [Google Scholar] [CrossRef]
- Meara, J.G.; Leather, A.J.M.; Hagander, L.; Alkire, B.C.; Alonso, N.; Ameh, E.A.; Bickler, S.W.; Conteh, L.; Dare, A.J.; Davies, J.; et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet 2015, 386, 569–624. [Google Scholar] [CrossRef] [PubMed]
- Paley, D.; Herzenberg, J.E.; Tetsworth, K.; McKie, J.; Bhave, A. Deformity planning for frontal and sagittal plane corrective osteotomies. Orthop. Clin. N. Am. 1994, 25, 425–465. [Google Scholar] [CrossRef]
- Levine, A.M.; Drennan, J.C. Physiological bowing and tibia vara. The metaphyseal-diaphyseal angle in the measurement of bowleg deformities. J. Bone Jt. Surg. Am. 1982, 64, 1158–1163. [Google Scholar] [CrossRef]
- Smith, S.L.; Beckish, M.L.; Winters, S.C.; Pugh, L.I.; Bray, E.W. Treatment of late-onset tibia vara using Afghan percutaneous osteotomy and orthofix external fixation. J. Pediatr. Orthop. 2000, 20, 606–610. [Google Scholar] [CrossRef]
- Chotigavanichaya, C.; Salinas, G.; Green, T.; Moseley, C.F.; Otsuka, N.Y. Recurrence of varus deformity after proximal tibial osteotomy in Blount disease: Long-term follow-up. J. Pediatr. Orthop. 2002, 22, 638–641. [Google Scholar] [CrossRef]
- LaMont, L.E.; McIntosh, A.L.; Jo, C.H.; Birch, J.G.; Johnston, C.E. Recurrence After Surgical Intervention for Infantile Tibia Vara: Assessment of a New Modified Classification. J. Pediatr. Orthop. 2019, 39, 65–70. [Google Scholar] [CrossRef]
- Sink, E.L.; Leunig, M.; Zaltz, I.; Gilbert, J.C.; Clohisy, J. Reliability of a complication classification system for orthopaedic surgery. Clin. Orthop. Relat. Res. 2012, 470, 2220–2226. [Google Scholar] [CrossRef]
- George, A.O. Skin diseases in tropical Africa: Medical, social, and economic implications. Int. J. Dermatol. 1988, 27, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Abraham, E.; Toby, D.; Welborn, M.; Helder, C.W.; Murphy, A. New Single-stage Double Osteotomy for Late-presenting Infantile Tibia Vara: A Comprehensive Approach. J. Pediatr. Orthop. 2019, 39, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Wesselsky, V.; Kitz, C.; Jakob, F.; Eulert, J.; Raab, P. Description and evaluation of operative deformity correction in calcium-deficiency rickets in Kaduna, northern Nigeria. Int. Orthop. 2016, 40, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Khanfour, A.A. A modified Puddu technique for the treatment of adolescent mild to moderate tibia vara. J. Pediatr. Orthop. B 2016, 25, 37–42. [Google Scholar] [CrossRef]
- Eamsobhana, P.; Kaewpornsawan, K.; Yusuwan, K. Do we need to do overcorrection in Blount’s disease? Int. Orthop. 2014, 38, 1661–1664. [Google Scholar] [CrossRef]
- Gkiokas, A.; Brilakis, E. Management of neglected Blount disease using double corrective tibia osteotomy and medial plateau elevation. J. Child. Orthop. 2012, 6, 411–418. [Google Scholar] [CrossRef]
- Ogbemudia, A.O.; Bafor, A.; Ogbemudia, P.E. Anterior posterior inverted-‘U’ osteotomy for tibia vara: Technique and early results. Arch. Orthop. Trauma Surg. 2011, 131, 437–442. [Google Scholar] [CrossRef]
- van Huyssteen, A.L.; Hastings, C.J.; Olesak, M.; Hoffman, E.B. Double-elevating osteotomy for late-presenting infantile Blount’s disease: The importance of concomitant lateral epiphysiodesis. J. Bone Jt. Surg. Br. 2005, 87, 710–715. [Google Scholar] [CrossRef]
- Beals, R.K.; Stanley, G. Surgical correction of bowlegs in achondroplasia. J. Pediatr. Orthop. B 2005, 14, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, R.D.; Quick, T.J.; Eastwood, D.M. Focal dome osteotomy for the correction of tibial deformity in children. J. Pediatr. Orthop. B 2005, 14, 340–346. [Google Scholar] [CrossRef] [PubMed]
- de Pablos, J.; Arbeloa-Gutierrez, L.; Arenas-Miquelez, A. Update on treatment of adolescent Blount disease. Curr. Opin. Pediatr. 2018, 30, 71–77. [Google Scholar] [CrossRef]
- Sabharwal, S.; Sabharwal, S. Treatment of Infantile Blount Disease: An Update. J. Pediatr. Orthop. 2017, 37 (Suppl. 2), S26–S31. [Google Scholar] [CrossRef] [PubMed]
- Pesenti, S.; Iobst, C.A.; Launay, F. Evaluation of the external fixator TrueLok Hexapod System for tibial deformity correction in children. Orthop. Traumatol. Surg. Res. 2017, 103, 761–764. [Google Scholar] [CrossRef]
- Putzeys, P.; Wilmes, P.; Merle, M. Triple tibial osteotomy for the correction of severe bilateral varus deformity in a patient with late-onset Blount’s disease. Knee Surg. Sport. Traumatol. Arthrosc. Off. J. ESSKA 2013, 21, 731–735. [Google Scholar] [CrossRef]
- Amer, A.R.A.L.; Khanfour, A.A. Evaluation of treatment of late-onset tibia vara using gradual angulation translation high tibial osteotomy. Acta Orthop. Belg. 2010, 76, 360–366. [Google Scholar] [PubMed]
- Petje, G.; Meizer, R.; Radler, C.; Aigner, N.; Grill, F. Deformity correction in children with hereditary hypophosphatemic rickets. Clin. Orthop. Relat. Res. 2008, 466, 3078–3085. [Google Scholar] [CrossRef]
- Fucentese, S.F.; Neuhaus, T.J.; Ramseier, L.E.; Exner, G.U. Metabolic and orthopedic management of X-linked vitamin D-resistant hypophosphatemic rickets. J. Child. Orthop. 2008, 2, 285–291. [Google Scholar] [CrossRef]
- Brooks, W.C.; Gross, R.H. Genu Varum in Children: Diagnosis and Treatment. J. Am. Acad. Orthop. Surg. 1995, 3, 326–335. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement | n | T1 1 Mean | Min | Max | SD | T2 2 Mean | Min | Max | SD | T3 3 Mean | Min | Max | SD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| mLDFA | 106 | 99.8 | 60 | 137 | 14.8 | 95.3 | 61 | 126 | 13.8 | 97.8 (p < 0.001) | 68 | 130 | 12.3 |
| mMPTA | 106 | 57.8 | 4 | 89 | 20.7 | 92.7 | 66 | 119 | 13.7 | 90.6 (p < 0.001) | 54 | 120 | 14.8 |
| JLCA | 106 | 6.6 | 0 | 26 | 5.6 | 5.8 | 0 | 27 | 4.7 | 5.1 (p > 0.05) | 0 | 17 | 3.4 |
| MDA | 87 | 26.9 | 0 | 75 | 16.0 | −7.2 | −33 | 48 | 14.7 | −5.1 (p < 0.001) | −30 | 67 | 16.4 |
| Plateau-angle | 102 | 38.5 | 2 | 74 | 15.7 | 38.3 | 1 | 74 | 16.8 | 37.6 (p > 0.05) | 3 | 70 | 16.6 |
| aTFA | 117 | −42.9 | −89 | −6 | 17.4 | 8.9 | −20 | 31 | 8.0 | 2.3 (p < 0.001) | −21 | 24 | 9.8 |
| mTFA | 116 | −42.1 | −85 | −12 | 15.5 | 1.2 | −20 | 17 | 6.6 | −4.3 (p < 0.001) | −30 | 13 | 8.9 |
| Clinical TFA | 109 | −35.7 | −85 | −5 | 15.5 | 2.0 (p < 0.001) | −16 | 15 | 7.0 | ||||
| Thigh-Foot-Angle | 83 | 39.1 IR | 110 IR | 17 ER | 22.5 | 3.1 IR (p < 0.001) | 50 IR | 40 ER | 15.3 | ||||
| TFA Photos | 111 | −44.6 | −100.5 | −8 | 19.8 | −0.5 (p < 0.001) | −55 | 20 | 11.2 |
| Influencing Factor | Unit | n | Crude Difference (95% CI) | Adjusted Difference (95% CI) | Adjusted Difference (95% CI) |
|---|---|---|---|---|---|
| Age | 115 | p = 0.002 | p = 0.024 1 | ||
| per year | −0.63 (−1.03; −0.24) | −0.42 1 (−0.78; −0.06) | |||
| mTFA (preoperative) | 115 | p < 0.001 | p < 0.001 2 | ||
| per degree | 0.30 (0.20; 0.39) | 0.282 (0.18; 0.37) | |||
| mTFA2 (in cast) | 115 | p < 0.001 | p < 0.001 2 | ||
| per degree | 0.47 (0.23; 0.70) | 0.46 2 (0.23; 0.68) | |||
| Diagnosis | |||||
| Blount disease | 57 | p < 0.001 | p = 0.071 2 | p = 0.035 3 | |
| −6.42 (−8.54; −4.30) | −4.0 2 (−8.37; 0.35) | 5.67 3 (0.40; 10.93) | |||
| Rickets | 29 | p = 0.011 | p = 0.040 2 | 0.036 3 | |
| 4.77 (1.11; 8.42) | 4.02 2 (0.18; 7.86) | 3.69 3 (0.25; 7.13) | |||
| Idiopathic | 20 | p < 0.001 | p = 0.001 2 | p = 0.005 3 | |
| 8.37 (4.21; 12.53) | 7.60 2 (3.22; 11.98) | 5.72 3 (1.74; 9.70) | |||
| Other | 12 | p = 0.101 | p = 0.195 2 | p = 0.327 3 | |
| −4.25 (−9.33; 0.84) | −3.43 2 (−8.65; 1.78) | −2.34 3 (−7.04; 2.37) |
| Measurement | N | T1 1 Mean | Min | Max | SD | T3 3 Mean | Min | Max | SD | T4 4 Mean | Min | Max | SD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| mLDFA | 9 | 112 | 99 | 125 | 8.0 | 107.1 | 95 | 121 | 8.3 | 102.1 | 89 | 123 | 11.1 |
| mMPTA | 9 | 72.4 | 65 | 82 | 5.3 | 102.1 | 94 | 117 | 6.8 | 103.1 | 89 | 121 | 8.9 |
| JLCA | 9 | 2.8 | 0 | 6 | 2.3 | 5.8 | 0 | 10 | 3.6 | 4.4 | 0 | 8 | 2.8 |
| MDA | 7 | 17.9 | 4 | 25 | 7.2 | −15.4 | −24 | −7 | 5.6 | −15.4 | −22 | −6 | 5.8 |
| Plateau-angle | 9 | 38 | 0 | 59 | 19.0 | 34.2 | 1 | 52 | 19.4 | 32.0 | 3 | 53 | 18.0 |
| aTFA | 9 | −39.4 | −53 | −12 | 12.5 | 5.2 | −7 | 17 | 8.7 | 10.6 | −6 | 26 | 11.9 |
| mTFA | 9 | −39.7 | −52 | −16 | 11.0 | −1.3 | −14 | 10 | 8.0 | 4 | −11 | 19 | 10.6 |
| Influencing Radiological Measurement | Crude Difference (95% CI) | Adjusted Difference (95% CI) |
|---|---|---|
| p < 0.001 | p < 0.001 1 | |
| aTFA | 0.82 (0.73; 0.92) | 0.84 1 (0.74; 0.93) |
| p < 0.001 | p < 0.001 1 | |
| mTFA | 0.68 (0.60; 0.77) | 0.701 (0.61; 0.78) |
| Grade | N | Listed Complications |
|---|---|---|
| Overall | 29 (23.4%) | |
| 1 | 24 (19.4%) | 7 patients with damaged skin integrity due to cast requiring local wound treatment |
| 1 patient with damaged skin integrity due to cast requiring local wound treatment and antibiotics | ||
| 2 patients with skin molds inside a cast | ||
| 1 patient with a wound infection requiring local wound treatment | ||
| 2 patients with a wound infection requiring local wound treatment and antibiotics | ||
| 1 patient with a wound break down requiring local wound treatment | ||
| 1 patient with excessive postoperative pain requiring opioids | ||
| 2 patients with postoperative urinary retention requiring catheterisation and antibiotics | ||
| 2 patients with a pin migration | ||
| 3 patients with feverish infections not associated to the surgical wound requiring antibiotics | ||
| 2 patients with temporary nerve irritations not requiring treatment | ||
| 2 patients with a fall after cast removal, one requiring no treatment and one requiring recasting for 4 weeks | ||
| 1d | 1 (0.8%) | 1 patient with a permanent peroneus lesion after ablation of the proximal fibular epiphysis requiring an ankle foot orthosis |
| 3 | 4 (3.2%) | 1 patient with a wound infection requiring antibiotics and revision surgery |
| 1 patient with a cast failure and excessive postoperative pain requiring a cast change in the OR | ||
| 1 patient with a loss of reduction requiring a cast change, pin removal and a wound cleaning in the OR | ||
| 1 patient with a vascular compromise requiring revision surgery with less correction angle, new placement of the pins and a cast change |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolbe, N.; Haydon, F.; Kolbe, J.; Dreher, T. Single-Stage Tibial Osteotomy for Correction of Genu Varum Deformity in Children. Children 2023, 10, 377. https://doi.org/10.3390/children10020377
Kolbe N, Haydon F, Kolbe J, Dreher T. Single-Stage Tibial Osteotomy for Correction of Genu Varum Deformity in Children. Children. 2023; 10(2):377. https://doi.org/10.3390/children10020377
Chicago/Turabian StyleKolbe, Nikolas, Frank Haydon, Johannes Kolbe, and Thomas Dreher. 2023. "Single-Stage Tibial Osteotomy for Correction of Genu Varum Deformity in Children" Children 10, no. 2: 377. https://doi.org/10.3390/children10020377