
Sorry Parents, Children Consume High Amounts of Candy before and after a Meal: Within-Person Comparisons of Children’s Candy Intake and Associations with Temperament and Appetite
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design & Participants
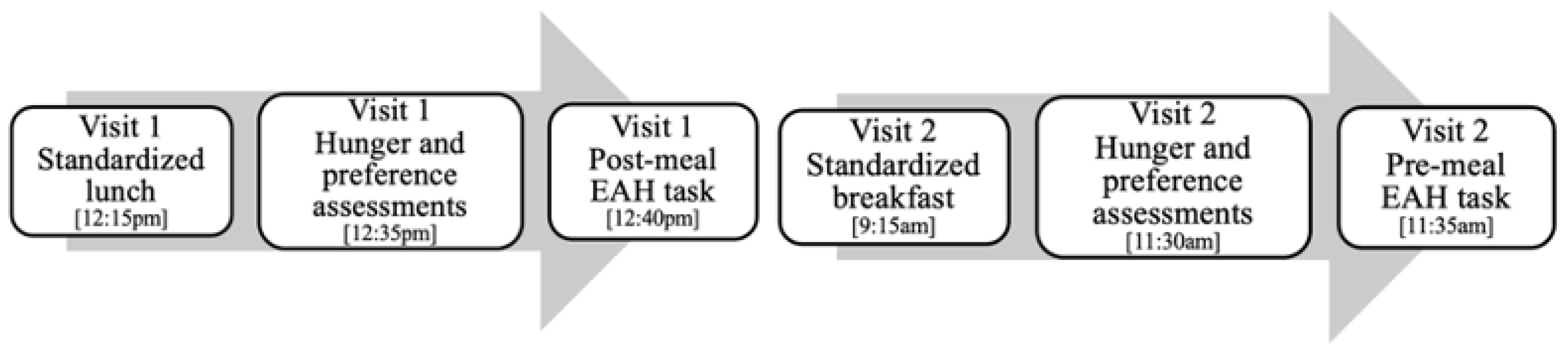
2.2. Procedure
2.3. Protocols
2.3.1. Post-Meal Candy Intake
2.3.2. Pre-Meal Candy Intake
2.4. Measures
2.4.1. Temperament
2.4.2. Appetitive Traits
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
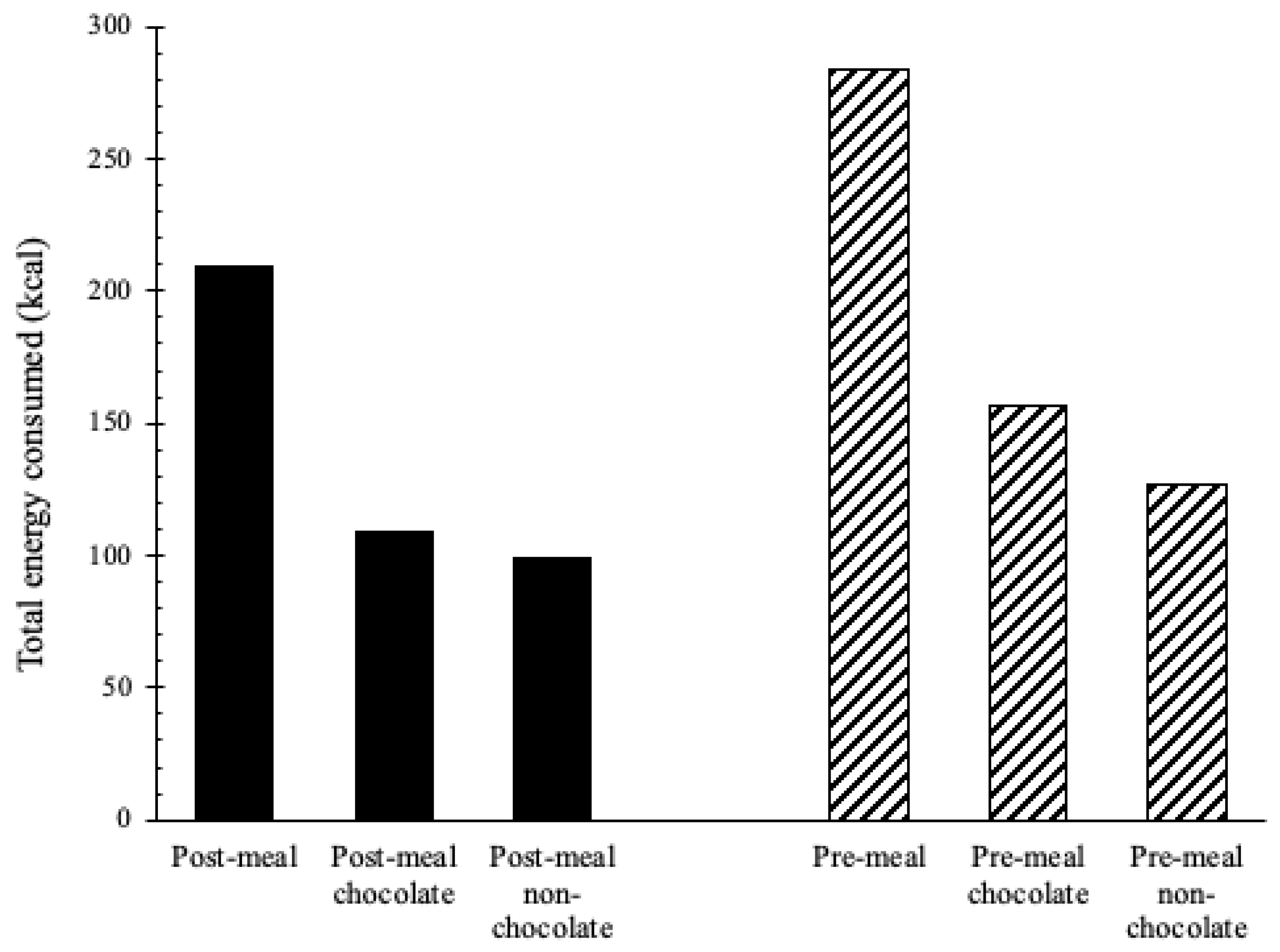
3.2. Candy Intake before and after a Meal
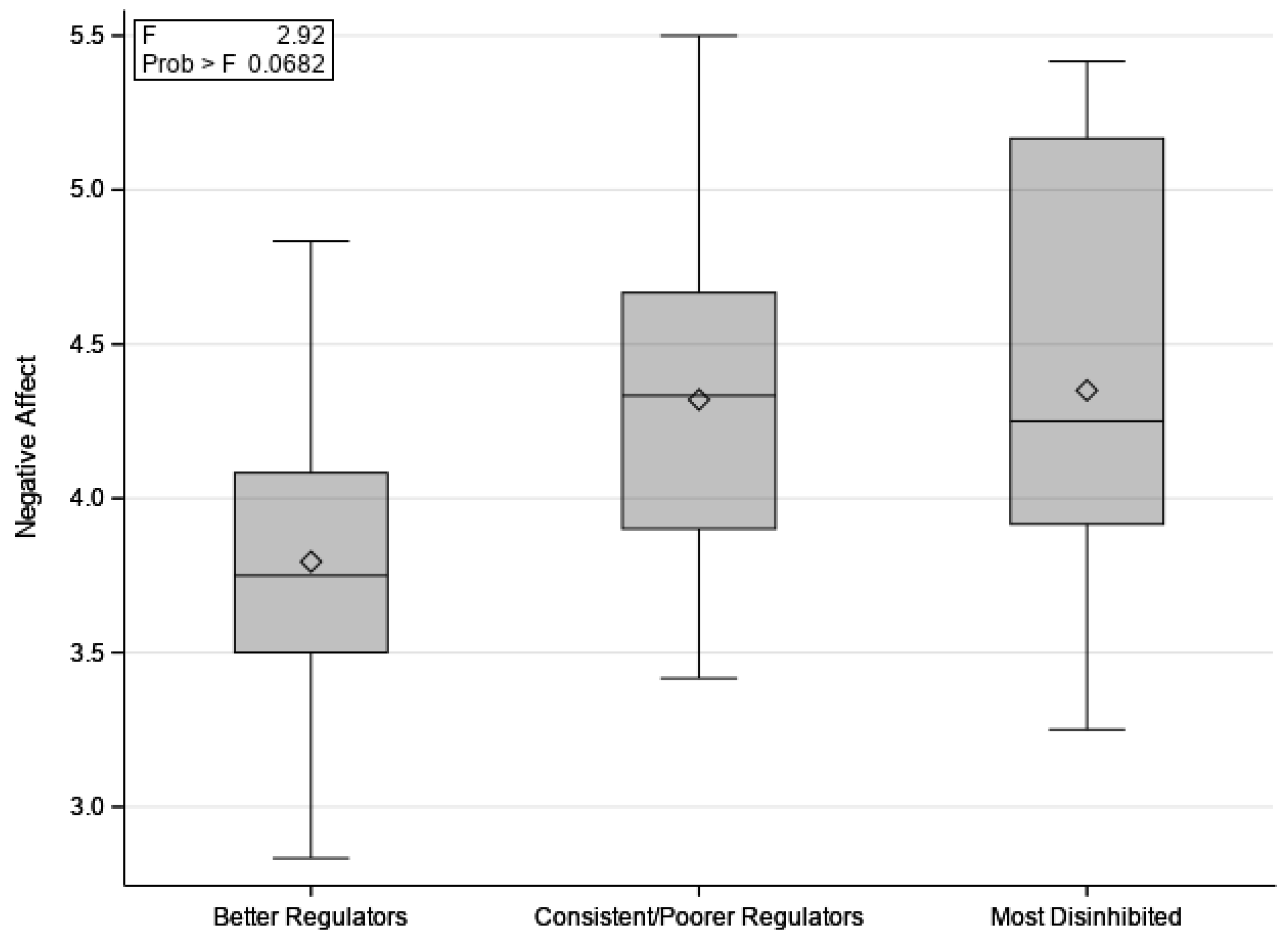
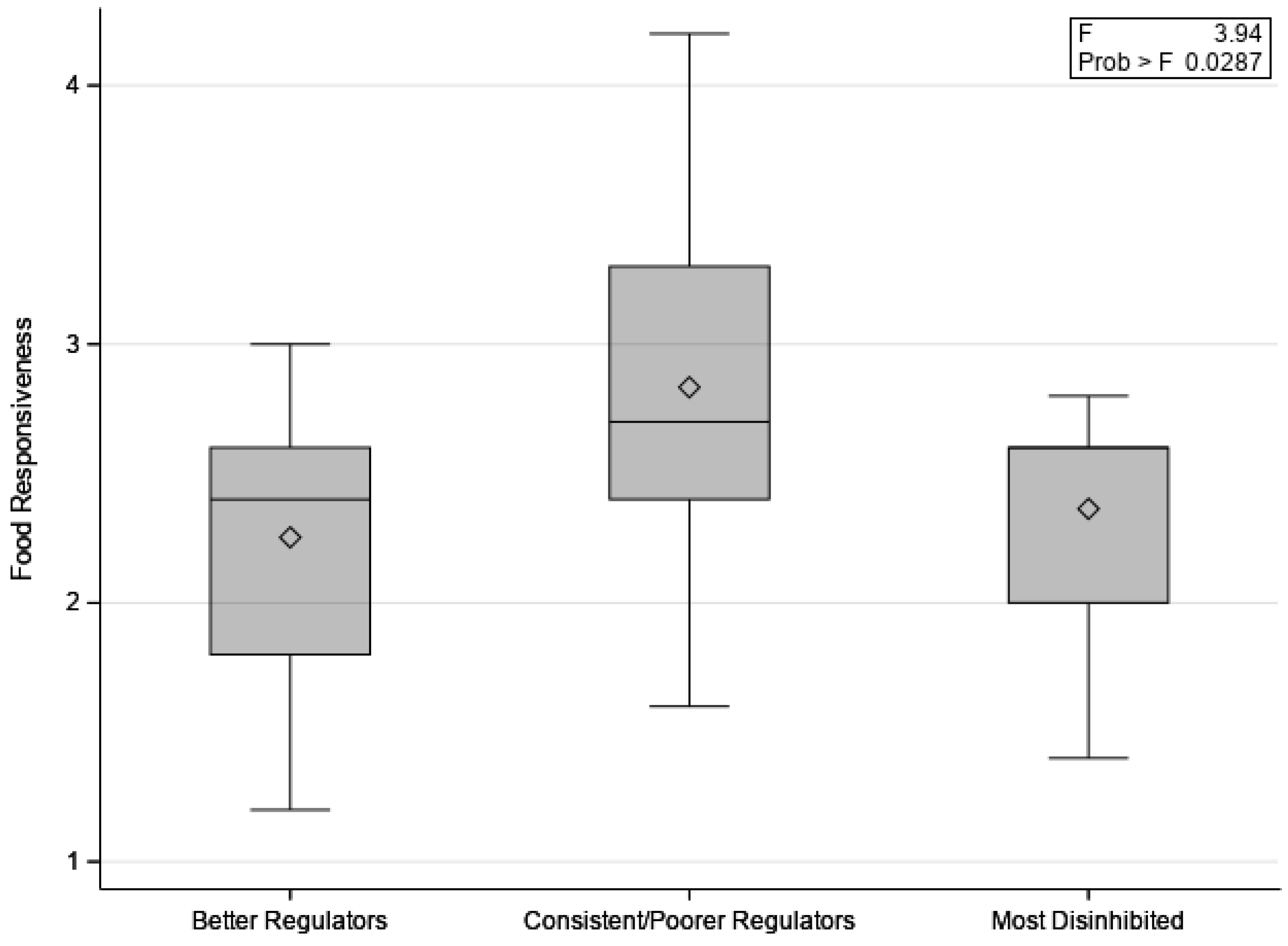
3.3. Differences in Candy Intake between Conditions and Associations with Temperament and Appetite
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kell, K.P.; Cardel, M.I.; Bohan Brown, M.M.; Fernández, J.R. Added Sugars in the Diet Are Positively Associated with Diastolic Blood Pressure and Triglycerides in Children. Am. J. Clin. Nutr. 2014, 100, 46–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.M.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement from the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicklas, T.A.; Yang, S.-J.; Baranowski, T.; Zakeri, I.; Berenson, G. Eating Patterns and Obesity in Children. Am. J. Prev. Med. 2003, 25, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Chi, D.L.; Scott, J.M. Added Sugar and Dental Caries in Children. Dent. Clin. N. Am. 2019, 63, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Fulgoni, V.L.; Cowan, A.E.; Gaine, P.C. Sources of Added Sugars in Young Children, Adolescents, and Adults with Low and High Intakes of Added Sugars. Nutrients 2018, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services Dietary Guidelines for Americans, 2020–2025. 9th Edition. 2020. Available online: https://www.dietaryguidelines.gov/ (accessed on 4 March 2022).
- Duyff, R.L.; Birch, L.L.; Byrd-Bredbenner, C.; Johnson, S.L.; Mattes, R.D.; Murphy, M.M.; Nicklas, T.A.; Rollins, B.Y.; Wansink, B. Candy Consumption Patterns, Effects on Health, and Behavioral Strategies to Promote Moderation: Summary Report of a Roundtable Discussion. Adv. Nutr. 2015, 6, 139S–146S. [Google Scholar] [CrossRef] [Green Version]
- Fisher, J.O.; Wright, G.; Herman, A.N.; Malhotra, K.; Serrano, E.L.; Foster, G.D.; Whitaker, R.C. “Snacks Are Not Food”. Low-Income, Urban Mothers’ Perceptions of Feeding Snacks to Their Preschool-Aged Children. Appetite 2015, 84, 61–67. [Google Scholar] [CrossRef]
- French, S.A.; Epstein, L.H.; Jeffery, R.W.; Blundell, J.E.; Wardle, J. Eating Behavior Dimensions. Associations with Energy Intake and Body Weight. A Review. Appetite 2012, 59, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Leung, C.Y.Y.; Lumeng, J.C.; Kaciroti, N.A.; Chen, Y.P.; Rosenblum, K.; Miller, A.L. Surgency and Negative Affectivity, but Not Effortful Control, Are Uniquely Associated with Obesogenic Eating Behaviors among Low-Income Preschoolers. Appetite 2014, 78, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pract. Res. 2007, 68, s1–s56. [Google Scholar]
- Ventura, A.K.; Worobey, J. Early Influences on the Development of Food Preferences. Curr. Biol. 2013, 23, R401–R408. [Google Scholar] [CrossRef]
- Freitas, A.; Albuquerque, G.; Silva, C.; Oliveira, A. Appetite-Related Eating Behaviours: An Overview of Assessment Methods, Determinants and Effects on Children’s Weight. Ann. Nutr. Metab. 2018, 73, 19–29. [Google Scholar] [CrossRef]
- Faith, M.S.; Carnell, S.; Kral, T.V.E. Genetics of Food Intake Self-Regulation in Childhood: Literature Review and Research Opportunities. Hum. Hered. 2013, 75, 80–89. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O.; Davison, K.K. Learning to Overeat: Maternal Use of Restrictive Feeding Practices Promotes Girls’ Eating in the Absence of Hunger. Am. J. Clin. Nutr. 2003, 78, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Lansigan, R.K.; Emond, J.A.; Gilbert-Diamond, D. Understanding Eating in the Absence of Hunger among Young Children: A Systematic Review of Existing Studies. Appetite 2015, 85, 36–47. [Google Scholar] [CrossRef] [Green Version]
- Rothbart, M.K.; Bates, J.E. Temperament. In Handbook of Child Psychology: Social, Emotional, and Personality Development, 6th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2006; Volume 3, pp. 99–166. ISBN 0-471-27290-6. [Google Scholar]
- Anzman-Frasca, S.; Stifter, C.A.; Birch, L.L. Temperament and Childhood Obesity Risk: A Review of the Literature. J. Dev. Behav. Pediatr. 2012, 33, 732–745. [Google Scholar] [CrossRef]
- Russell, C.G.; Russell, A. “Food” and “Non-Food” Self-Regulation in Childhood: A Review and Reciprocal Analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 33. [Google Scholar] [CrossRef]
- Drewnowski, A. Sensory Preferences for Fat and Sugar in Adolescence and Adult Life. Ann. N. Y. Acad. Sci. 1989, 561, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, S.; Fernández, M.C.; Cepeda-Benito, A.; Vila, J. Subjective and Physiological Reactivity to Chocolate Images in High and Low Chocolate Cravers. Biol. Psychol. 2005, 70, 9–18. [Google Scholar] [CrossRef]
- Standen-Holmes, J.E.; Liem, D.G. Chocolate and Children’s Food and Flavor Preferences. In Chocolate in Health and Nutrition; Watson, R.R., Preedy, V.R., Zibadi, S., Eds.; Nutrition and Health; Humana Press: Totowa, NJ, USA, 2013; pp. 491–503. ISBN 978-1-61779-803-0. [Google Scholar]
- Putnam, S.P.; Rothbart, M.K. Development of Short and Very Short Forms of the Children’s Behavior Questionnaire. J. Personal. Assess. 2006, 87, 102–112. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making Sense of Cronbach’s Alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiat. 2001, 42, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.C.; Gortmaker, S.L.; Sobol, A.M.; Kuntz, K.M. Estimating the Energy Gap among US Children: A Counterfactual Approach. Pediatrics 2006, 118, e1721–e1733. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of Obesity among Adults and Youth: United States, 2011–2014. NCHS Data Brief 2015, 219, 1–8. [Google Scholar]
- Coccia, C.; Lovan, P.; Macchi, A.; Coto, J.; Dick, A.S.; Graziano, P.A. How Much and What: Using a Buffet to Determine Self-Regulation of Food Intake among Young School-Age Children. Physiol. Behav. 2022, 249, 113745. [Google Scholar] [CrossRef]
- Kral, T.V.E.; Moore, R.H.; Chittams, J.; O’Malley, L.; Jones, E.; Quinn, R.J.; Fisher, J.O. Caloric Compensation and Appetite Control in Children of Different Weight Status and Predisposition to Obesity. Appetite 2020, 151, 104701. [Google Scholar] [CrossRef]
- Fisher, J.O.; Birch, L.L. Restricting Access to Palatable Foods Affects Children’s Behavioral Response, Food Selection, and Intake. Am. J. Clin. Nutr. 1999, 69, 1264–1272. [Google Scholar] [CrossRef] [Green Version]
- Savage, J.S. Development of a Theory-Based Questionnaire to Assess Structure and Control in Parent Feeding (SCPF). Int. J. Behav. Nutr. Phys. Act. 2017, 14, 9. [Google Scholar] [CrossRef] [Green Version]
- Moens, E.; Braet, C. Predictors of Disinhibited Eating in Children with and without Overweight. Behav. Res. Ther. 2007, 45, 1357–1368. [Google Scholar] [CrossRef]
- Grilo, C.M.; Masheb, R.M.; Wilson, G.T. Subtyping Binge Eating Disorder. J. Consult. Clin. Psychol. 2001, 69, 1066–1072. [Google Scholar] [CrossRef]
- Hetherington, M.M.; Rolls, B.J. Sensory-Specific Satiety: Theoretical Frameworks and Central Characteristics. In Why We Eat What We Eat: The psychology of Eating; American Psychological Association: Washington, DC, USA, 1996; pp. 267–290. ISBN 978-1-55798-366-4. [Google Scholar]
- Rischel, H.E.; Nielsen, L.A.; Gamborg, M.; Møller, P.; Holm, J.-C. Comparison of Sensory-Specific Satiety between Normal Weight and Overweight Children. Appetite 2016, 107, 486–493. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| F Value | p Value | R2 | |
|---|---|---|---|
| Negative Affect | 2.92 | 0.07 | 0.15 |
| Effortful Control | 1.84 | 0.18 | 0.10 |
| Surgency | 1.77 | 0.19 | 0.10 |
| Food Responsiveness | 3.94 | 0.03 | 0.18 |
| Satiety Responsiveness | 2.08 | 0.14 | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez, E.; Moore, A.M.; Rollins, B.Y.; Tovar, A.; Savage, J.S. Sorry Parents, Children Consume High Amounts of Candy before and after a Meal: Within-Person Comparisons of Children’s Candy Intake and Associations with Temperament and Appetite. Children 2023, 10, 52. https://doi.org/10.3390/children10010052
Hernandez E, Moore AM, Rollins BY, Tovar A, Savage JS. Sorry Parents, Children Consume High Amounts of Candy before and after a Meal: Within-Person Comparisons of Children’s Candy Intake and Associations with Temperament and Appetite. Children. 2023; 10(1):52. https://doi.org/10.3390/children10010052
Chicago/Turabian StyleHernandez, Erika, Amy M. Moore, Brandi Y. Rollins, Alison Tovar, and Jennifer S. Savage. 2023. "Sorry Parents, Children Consume High Amounts of Candy before and after a Meal: Within-Person Comparisons of Children’s Candy Intake and Associations with Temperament and Appetite" Children 10, no. 1: 52. https://doi.org/10.3390/children10010052