
Importance of the PD-1/PD-L1 Axis for Malignant Transformation and Risk Assessment of Oral Leukoplakia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Collective
2.2. Detection of PD-L1 Expression by Quantitative Real Time Reverse Transcriptase Polymerase Chain Reaction (RT-qPCR)
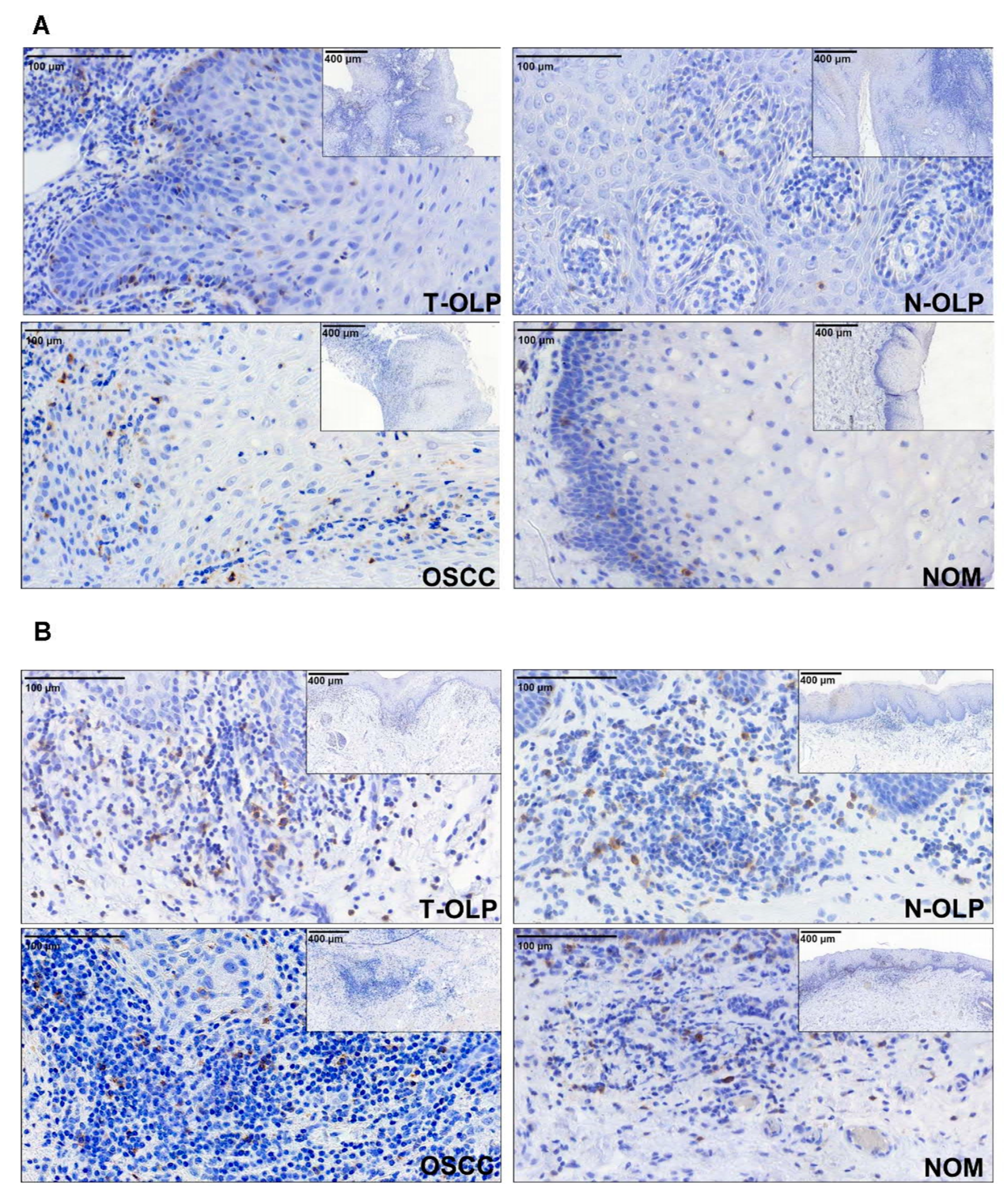
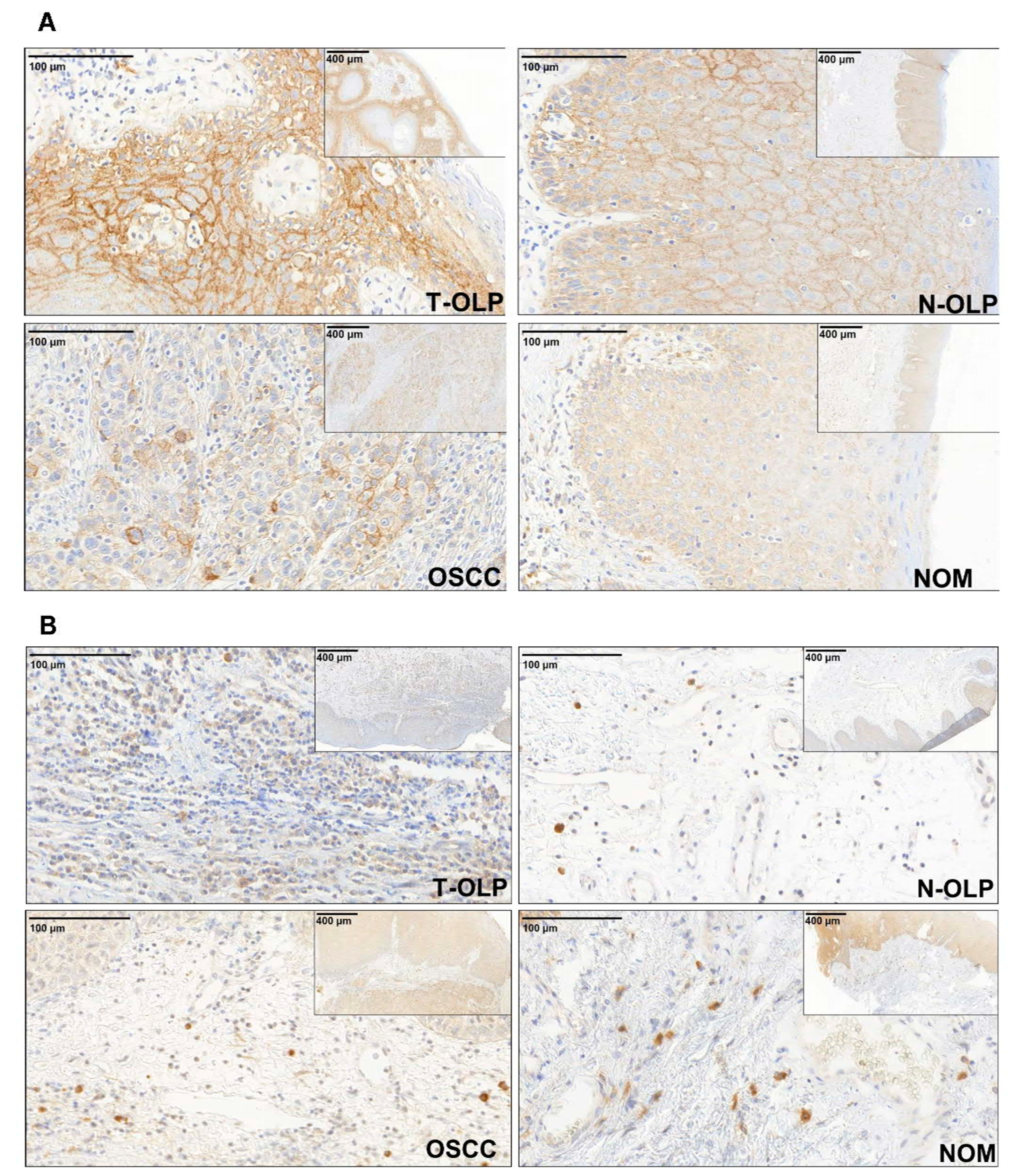
2.3. Detection and Quantitative Immunohistochemical Analysis of PD-1 and PD-L1 Expression by Immunohistochemistry
2.4. Statistics
3. Results
3.1. Demographic, Clinical and Histomorphologic Characteristics of the Study Groups
3.2. Descriptive Statistics of PD-1 and PD-L1 Expression in T-OLP, N- OLP, OSCC and NOM
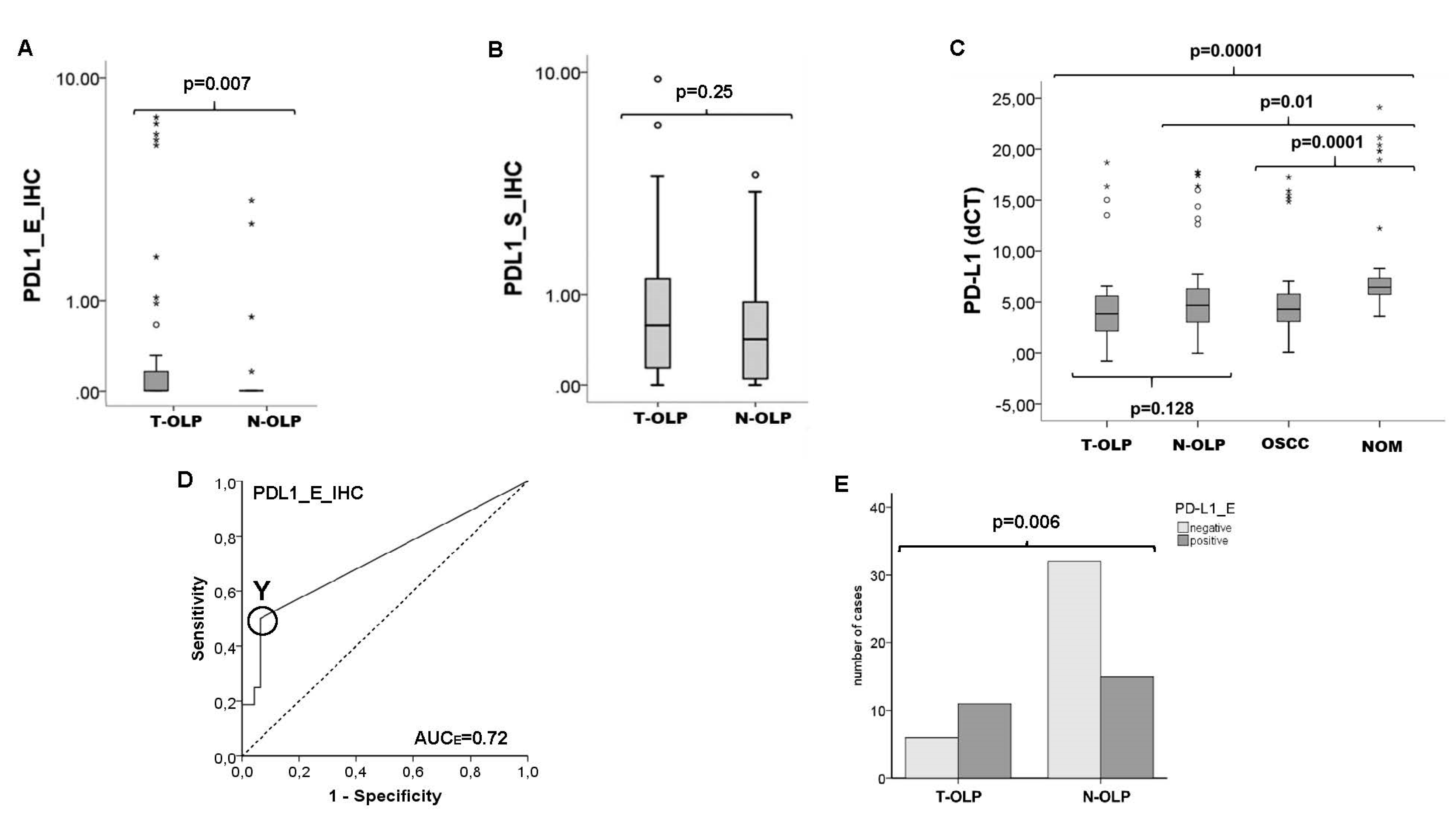
3.3. Comparison of Expression Rates between the Pathologically Altered Tissues and NOM
3.4. Comparison of T-OLP and N-OLP—Association between Overexpression of PD-1 and PD-L1 and Malignant Transformation
3.5. Association of Differential Expression Patterns with Histomorphological and Clinico-Histopathological Parameters
3.6. Inflammation in Relationship to Malignancy, Malignant Transformation and PD-1/PD-L1 Expression
3.6.1. Association between Inflammation and Malignancy or Malignant Transformation
3.6.2. Association between Inflammation and PD-L1 mRNA Expression
3.6.3. Association between Inflammation and Protein Expression of PD-1 and PD-L1
3.6.4. Association between Localization of the OLP with Malignant Transformation and PD-1/PD-L1 Expression
4. Discussion
4.1. Implication of Altered Checkpoint Expression in OLP
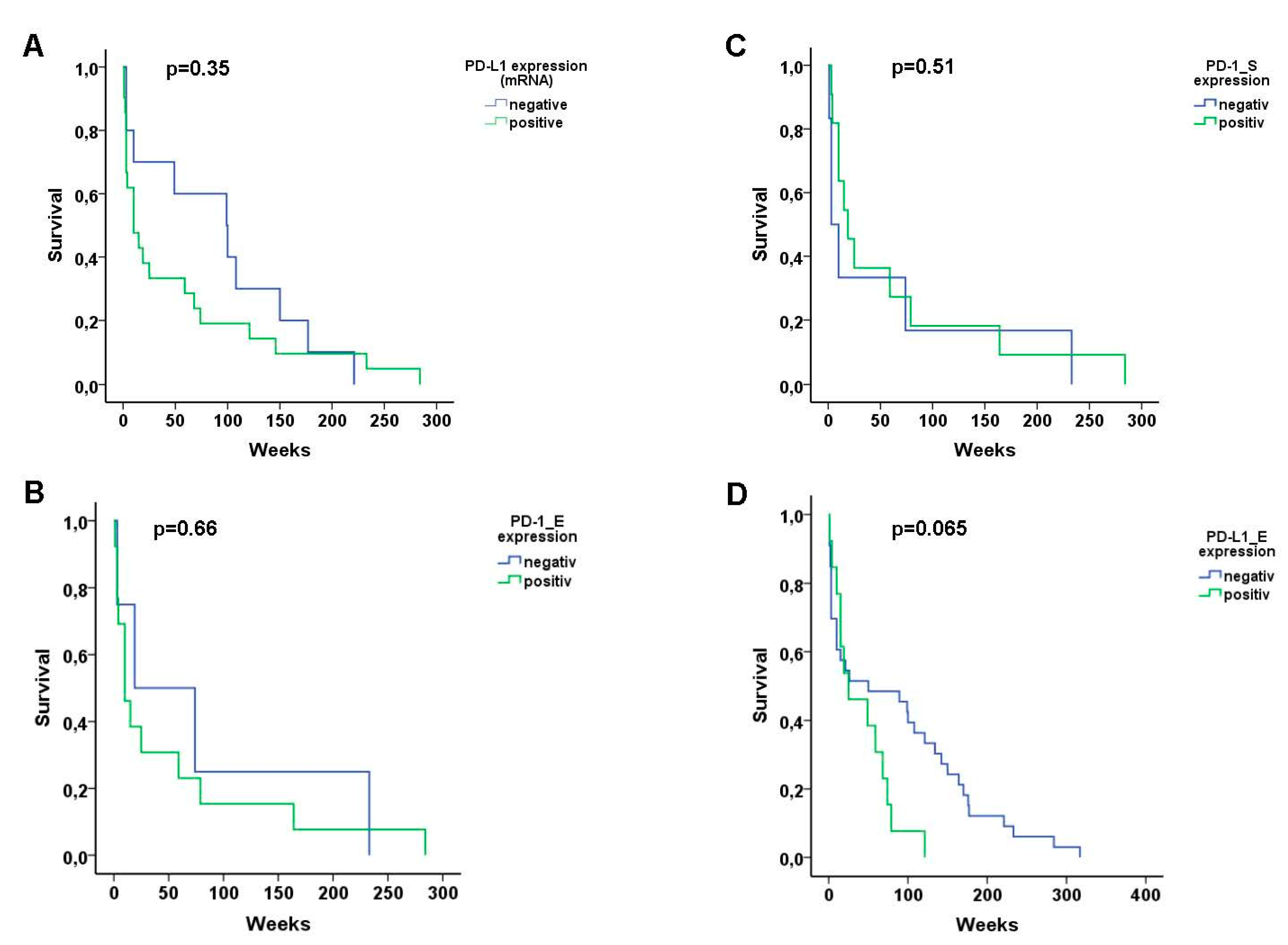
4.2. Predictive Value of Checkpoints in OLP
4.3. Therapeutic Potential
4.4. Association between Inflammation and Checkpoint Expression
4.5. Association between Localization of the OLP, Malignant Transformation and Immune Checkpoint Expression
4.6. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moskovitz, J.; Moy, J.; Ferris, R.L. Immunotherapy for Head and Neck Squamous Cell Carcinoma. Curr. Oncol. Rep. 2018, 20, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Cramer, J.D.; Burtness, B.; Ferris, R.L. Immunotherapy for head and neck cancer: Recent advances and future directions. Oral Oncol. 2019, 99, 104460. [Google Scholar] [CrossRef]
- Schoenfeld, J.D.; Hanna, G.J.; Jo, V.Y.; Rawal, B.; Chen, Y.H.; Catalano, P.S.; Lako, A.; Ciantra, Z.; Weirather, J.L.; Criscitiello, S.; et al. Neoadjuvant Nivolumab or Nivolumab Plus Ipili-mumab in Untreated Oral Cavity Squamous Cell Carcinoma: A Phase 2 Open-Label Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Uppaluri, R.; Campbell, K.M.; Egloff, A.M.; Zolkind, P.; Skidmore, Z.L.; Nussenbaum, B.; Paniello, R.C.; Rich, J.T.; Jackson, R.; Pipkorn, P.; et al. Neoadjuvant and Adjuvant Pem-brolizumab in Resectable Locally Advanced, Human Papillomavirus-Unrelated Head and Neck Cancer: A Multicenter, Phase II Trial. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 5140–5152. [Google Scholar] [CrossRef]
- Tang, H.; Liang, Y.; Anders, R.A.; Taube, J.M.; Qiu, X.; Mulgaonkar, A.; Liu, X.; Harrington, S.M.; Guo, J.; Xin, Y.; et al. PD-L1 on host cells is essential for PD-L1 block-ade-mediated tumor regression. J. Clin. Investig. 2018, 128, 580–588. [Google Scholar] [CrossRef] [Green Version]
- Wehrhan, F.; Weber, M.; Baran, C.; Agaimy, A.; Büttner-Herold, M.; Kesting, M.; Ries, J. PD1 expression and correlation with its ligands in oral cancer specimens and peripheral blood. J. Cranio Maxillofacial Surg. 2020. [Google Scholar] [CrossRef]
- Weber, M.; Wehrhan, F.; Baran, C.; Agaimy, A.; Büttner-Herold, M.; Preidl, R.; Neukam, F.W.; Ries, J. PD-L1 expression in tumor tissue and peripheral blood of patients with oral squamous cell carcinoma. Oncotarget 2017, 8, 112584–112597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, J.; Chen, X.-F.; Xu, M.-G.; Zhao, J. Relationship of programmed death ligand-1 expression with clinicopathological features and prognosis in patients with oral squamous cell carcinoma: A meta-analysis. Arch. Oral Biol. 2020, 114, 104717. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Wehrhan, F.; Baran, C.; Agaimy, A.; Büttner-Herold, M.; Kesting, M.; Ries, J. Prognostic significance of PD-L2 expression in patients with oral squamous cell carcinoma—A comparison to the PD-L1 expression profile. Cancer Med. 2019, 8, 1124–1134. [Google Scholar] [CrossRef]
- Wehrhan, F.; Büttner-Herold, M.; Hyckel, P.; Moebius, P.; Preidl, R.; Distel, L.; Ries, J.; Amann, K.; Schmitt, C.; Neukam, F.W.; et al. Increased malignancy of oral squamous cell carcinomas (oscc) is associated with macrophage polarization in regional lymph nodes—An immunohistochemical study. BMC Cancer 2014, 14, 522. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.; Moebius, P.; Büttner-Herold, M.; Amann, K.; Preidl, R.; Neukam, F.W.; Wehrhan, F. Macrophage polarisation changes within the time between diagnostic biopsy and tumour resection in oral squamous cell carcinomas—An immunohistochemical study. Br. J. Cancer 2015, 113, 510–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheifele, C.; Reichart, P.A. Oral leukoplakia in manifest squamous epithelial carcinoma. A clinical prospective study of 101 patients. MKG 1998, 2, 326–330. [Google Scholar] [PubMed]
- Sudbø, J.; Reith, A. Which putatively pre-malignant oral lesions become oral cancers? Clinical relevance of early targeting of high-risk individuals. J. Oral Pathol. Med. 2003, 32, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Reibel, J. Prognosis of Oral Pre-malignant Lesions: Significance of Clinical, Histopathological, and Molecular Biological Characteristics. Crit. Rev. Oral Biol. Med. 2003, 14, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, P. Dermatologie und Venerologie, 2nd ed.; Springer: Berlin, Germany, 2004. [Google Scholar]
- Warnakulasuriya, S.; Reibel, J.; Bouquot, J.; Dabelsteen, E. Oral epithelial dysplasia classification systems: Predictive value, utility, weaknesses and scope for improvement. J. Oral Pathol. Med. 2008, 37, 127–133. [Google Scholar] [CrossRef]
- Chatterjee, S.K.; Zetter, B.R. Cancer biomarkers: Knowing the present and predicting the future. Futur. Oncol. 2005, 1, 37–50. [Google Scholar] [CrossRef]
- Dionne, K.R.; Warnakulasuriya, S.; Zain, R.B.; Cheong, S.C. Potentially malignant disorders of the oral cavity: Current practice and future directions in the clinic and laboratory. Int. J. Cancer 2014, 136, 503–515. [Google Scholar] [CrossRef]
- Oliveira, L.; Ribeiro-Silva, A. Prognostic significance of immunohistochemical biomarkers in oral squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2011, 40, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Pitiyage, G.; Tilakaratne, W.M.; Tavassoli, M.; Warnakulasuriya, S. Molecular markers in oral epithelial dysplasia: Review. J. Oral Pathol. Med. 2009, 38, 737–752. [Google Scholar] [CrossRef]
- Rivera, C.; Oliveira, A.K.; Costa, R.A.P.; De Rossi, T.; Leme, A.F.P. Prognostic biomarkers in oral squamous cell carcinoma: A systematic review. Oral Oncol. 2017, 72, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Konings, H.; Stappers, S.; Geens, M.; De Winter, B.Y.; Lamote, K.; van Meerbeeck, J.P.; Specenier, P.; Vanderveken, O.M.; Ledeganck, K.J. A Literature Review of the Potential Di-agnostic Biomarkers of Head and Neck Neoplasms. Front. Oncol. 2020, 10, 1020. [Google Scholar] [CrossRef]
- Weber, M.; Wehrhan, F.; Baran, C.; Agaimy, A.; Büttner-Herold, M.; Öztürk, H.; Neubauer, K.; Wickenhauser, C.; Kesting, M.; Ries, J. Malignant transformation of oral leukoplakia is associated with macrophage polarization. J. Transl. Med. 2020, 18, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, D.; Gubin, M.M.; Schreiber, R.D.; Smyth, M.J. New insights into cancer immunoediting and its three component phas-es—Elimination, equilibrium and escape. Curr. Opin. Immunol. 2014, 27, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Vesely, M.D.; Kershaw, M.H.; Schreiber, R.D.; Smyth, M.J. Natural Innate and Adaptive Immunity to Cancer. Annu. Rev. Immunol. 2011, 29, 235–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagyuu, T.; Hatakeyama, K.; Imada, M.; Kurihara, M.; Matsusue, Y.; Yamamoto, K.; Obayashi, C.; Kirita, T. Programmed death ligand 1 (PD-L1) expression and tumor microenvironment: Implications for patients with oral precancerous lesions. Oral Oncol. 2017, 68, 36–43. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours; International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Brennan, M.; Migliorati, C.A.; Lockhart, P.B.; Wray, D.; Al-Hashimi, I.; Axéll, T.; Bruce, A.J.; Carpenter, W.; Eisenberg, E.; Epstein, J.B.; et al. Management of oral epithelial dysplasia: A review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, S19.e1–S19.e12. [Google Scholar] [CrossRef] [PubMed]
- McCall, M.N.; McMurray, H.R.; Land, H.; Almudevar, A. On non-detects in qPCR data. Bioinformatics 2014, 30, 2310–2316. [Google Scholar] [CrossRef]
- Sharpe, A.H.; Pauken, K.E. The diverse functions of the PD1 inhibitory pathway. Nat. Rev. Immunol. 2018, 18, 153–167. [Google Scholar] [CrossRef]
- Tan, J.; Chen, S.; Lu, Y.; Yao, D.; Xu, L.; Zhang, Y.; Yang, L.; Chen, J.; Lai, J.; Yu, Z.; et al. Higher PD-1 expression concurrent with exhausted CD8+ T cells in patients with de novo acute myeloid leukemia. Chin. J. Cancer Res. 2017, 29, 463–470. [Google Scholar] [CrossRef]
- Mattox, A.K.; Lee, J.; Westra, W.H.; Pierce, R.H.; Ghossein, R.; Faquin, W.C.; Diefenbach, T.J.; Morris, L.G.; Lin, D.T.; Wirth, L.J.; et al. PD-1 Expression in Head and Neck Squamous Cell Carcinomas Derives Primarily from Functionally Anergic CD4+ TILs in the Presence of PD-L1+ TAMs. Cancer Res. 2017, 77, 6365–6374. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-Y.; Yan, Y.-Y.; Li, J.-J.; Adhikari, R.; Fu, L.-W. PD-1/PD-L1 Based Combinational Cancer Therapy: Icing on the Cake. Front. Pharmacol. 2020, 11, 722. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Sánchez, F.J.; Lequerica-Fernández, P.; Suárez-Canto, J.; Rodrigo, J.P.; Rodriguez-Santamarta, T.; Domínguez-Iglesias, F.; García-Pedrero, J.M.; De Vicente, J.C. Macrophages in Oral Carcinomas: Relationship with Cancer Stem Cell Markers and PD-L1 Expression. Cancers 2020, 12, 1764. [Google Scholar] [CrossRef]
- Weber, M.; Büttner-Herold, M.; Hyckel, P.; Moebius, P.; Distel, L.; Ries, J.; Amann, K.; Neukam, F.W.; Wehrhan, F. Small oral squamous cell carcinomas with nodal lymphogenic metastasis show increased infiltration of M2 polarized macrophages—An immunohistochemical analysis. J. Cranio Maxillofacial Surg. 2014, 42, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.M.; Kato, S.; Bazhenova, L.; Patel, S.P.; Frampton, G.M.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol. Cancer Ther. 2017, 16, 2598–2608. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Liu, N.; Guan, X.; Wu, H.; Sun, Z.; Zeng, H. Immunosuppression Induced by Chronic Inflammation and the Progression to Oral Squamous Cell Carcinoma. Mediat. Inflamm. 2016, 2016, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lenouvel, D.; Gonzalez-Moles, M.A.; Ruiz-Avila, I.; Chamorro-Santos, C.; Gonzalez-Ruiz, L.; Gonzalez-Ruiz, I.; Ramos-García, P. Clinicopatho-logical and prognostic significance of PD-L1 in oral cancer: A preliminary retrospective immunohistochemistry study. Oral Dis. 2021, 27, 173–182. [Google Scholar] [CrossRef]
- Goncalves, A.S.; Mosconi, C.; Jaeger, F.; Wastowski, I.J.; Aguiar, M.C.F.; Silva, T.A.; Ribeiro-Rotta, R.F.; Lago Costa, N.; Carvalho Batista, A. Overexpression of immunomodulatory medi-ators in oral precancerous lesions. Hum Immunol. 2017, 78, 752–757. [Google Scholar] [CrossRef]
- Stasikowska-Kanicka, O.; Wagrowska-Danilewicz, M.; Danilewicz, M. CD8+ and CD163+ infiltrating cells and PD-L1 immu-noexpression in oral leukoplakia and oral carcinoma. APMIS 2018, 126, 732–738. [Google Scholar] [CrossRef]
- Chen, X.-J.; Tan, Y.-Q.; Zhang, N.; He, M.-J.; Zhou, G. Expression of programmed cell death-ligand 1 in oral squamous cell carcinoma and oral leukoplakia is associated with disease progress and CD8+ tumor-infiltrating lymphocytes. Pathol. Res. Pr. 2019, 215, 152418. [Google Scholar] [CrossRef]
- Kouketsu, A.; Sato, I.; Oikawa, M.; Shimizu, Y.; Saito, H.; Takahashi, T.; Kumamoto, H. Expression of immunoregulatory molecules PD-L1 and PD-1 in oral cancer and precancerous lesions: A cohort study of Japanese patients. J. Cranio Maxillofacial Surg. 2019, 47, 33–40. [Google Scholar] [CrossRef]
- Ries, J.; Agaimy, A.; Vairaktaris, E.; Gorecki, P.; Neukam, F.W.; Strassburg, L.H.; Nikenke, E. Detection of MAGE-A expression predicts ma-lignant transformation of oral leukoplakia. Cancer Investig. 2012, 30, 495–502. [Google Scholar] [CrossRef]
- Ries, J.; Agaimy, A.; Vairaktaris, E.; Kwon, Y.; Neukam, F.W.; Strassburg, L.H.; Nkenke, E. Evaluation of MAGE-A expression and grade of dysplasia for predicting malignant progression of oral leukoplakia. Int. J. Oncol. 2012, 41, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Lodi, G.; Franchini, R.; Warnakulasuriya, S.; Varoni, E.M.; Sardella, A.; Kerr, A.R.; Carrassi, A.; I MacDonald, L.C.; Worthington, H.V. Interventions for treating oral leukoplakia to prevent oral cancer. Cochrane Database Syst. Rev. 2016, 7, CD001829. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, J.; Yang, X.; Liu, Y.; Liu, Y.; Li, Y.; Sun, L.; Yang, X.; Niu, H. Bacillus Calmette–Guérin and anti-PD-L1 combination therapy boosts immune response against bladder cancer. Onco Targets Ther. 2018, 11, 2891–2899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin, A.M.; Baydar, D.E.; Hazir, B.; Babaoglu, B.; Bilen, C.Y. Prognostic significance of pre- and post-treatment PD-L1 expression in patients with primary high-grade non-muscle-invasive bladder cancer treated with BCG immunotherapy. World J. Urol. 2020, 38, 2537–2545. [Google Scholar] [CrossRef]
- Thoma, C. PD-L1 and BCG response prediction. Nat. Rev. Urol. 2020, 17, 8. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Xie, T.; Wang, B.; William, W.N.; Heymach, J.V.; El-Naggar, A.K.; Myers, J.N.; Caulin, C. PD-1 Blockade Prevents the Development and Progression of Carcinogen-Induced Oral Premalignant Lesions. Cancer Prev. Res. 2017, 10, 684–693. [Google Scholar] [CrossRef] [Green Version]
- Yao, S.; Chen, L. PD-1 as an Immune Modulatory Receptor. Cancer J. 2014, 20, 262–264. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Jiang, C.C.; Jin, L.; Zhang, X.D. Regulation of PD-L1: A novel role of pro-survival signalling in cancer. Ann. Oncol. 2016, 27, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.-Y.; Kuo, Y.-B.; Wu, T.-L.; Liao, C.-T.; Sun, Y.-C.; Yen, T.-C.; Chan, E.-C. Association and prognostic value of serum inflammation markers in patients with leukoplakia and oral cavity cancer. Clin. Chem. Lab. Med. 2013, 51, 1291–1300. [Google Scholar] [CrossRef]
- Rubert, A.; Bagán, L.; Bagán, J.V. Oral leukoplakia, a clinical-histopathological study in 412 patients. J. Clin. Exp. Dent. 2020, 12, e540–e546. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | T-OLP | N-OLP | OSCC | NOM | Total | |
|---|---|---|---|---|---|---|
| Number of Cases | 32 | 50 | 38 | 42 | 162 | |
| Sex | Male | 20 | 24 | 24 | - | - |
| Female | 12 | 14 | 18 | - | - | |
| Collective | Erlangen | 17 | 21 | 42 | - | - |
| Halle | 15 | 17 | 0 | - | - | |
| Mean Age/SD | 62/10.9 | 55/12.4 | 66/11.2 | 43/20.4 | - | |
| Age Range | 45–92 | 23–81 | 34–93 | 18–81 | - | |
| Localization | Tongue | 17 | 9 | - | - | - |
| Floor of mouth | 5 | 2 | - | - | - | |
| Lower jaw | 1 | 7 | - | - | - | |
| Upper jaw | 2 | 6 | - | - | - | |
| Buccal mucosa | 2 | 15 | - | - | - | |
| Vestibulum oris | 1 | 3 | - | - | - | |
| Oral cavity * | 4 | 8 | - | - | - | |
| Dysplasia | D0 | 17 | 37 | - | - | - |
| D1 | 6 | 11 | - | - | - | |
| D2 | 4 | 2 | - | - | - | |
| Group | T-OLP | N-OLP | OSCC | NOM | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PD-1 | PD-L1 | PD-1 | PD-L1 | PD-1 | PD-L1 | PD-1 | PD-L1 | PD-1 | PD-L1 | ||
| Number of Cases * | 17 | 46 | 50 | 53 | 21 | 45 | 20 | 20 | 108 | 164 | |
| Sex | Male | 9 | 29 | 25 | 27 | 11 | 28 | 10 | 10 | 55 | 94 |
| Female | 8 | 17 | 25 | 26 | 10 | 17 | 10 | 10 | 53 | 70 | |
| Collective | Erlangen | 5 | 27 | 30 | 31 | 9 | 26 | 20 | 20 | 64 | 104 |
| Halle | 12 | 19 | 20 | 22 | 12 | 19 | 0 | 0 | 44 | 60 | |
| Mean Age/SD | 56.5/15.1 | 53.7/12.6 | 60.9/14.8 | 43.1/19.8 | - | - | |||||
| Age Range | 45–93 | 23–81 | 38–93 | 18–81 | - | - | |||||
| PD-1 | PD-L1 | PD-1 | PD-L1 | PD-1 | PD-L1 | PD-1 | PD-L1 | ||||
| Dysplasia | D0 | 10 | 27 | 36 | 39 | - | - | - | - | ||
| D1 | 2 | 8 | 13 | 13 | - | - | |||||
| D2 | 2 | 6 | 1 | 1 | - | - | |||||
| D3 | 3 | 5 | 0 | 0 | - | - | |||||
| - | - | ||||||||||
| High Risk * | D0/D1 | 12 | 35 | 49 | 52 | - | - | ||||
| Low Risk * | D2/D3 | 5 | 11 | 1 | 1 | - | - | ||||
| Grading | G1 | - | 7 | 13 | - | - | - | ||||
| G2 | 8 | 18 | - | - | |||||||
| G3 | 5 | 11 | - | - | |||||||
| n.d. | 1 | 3 | - | - | |||||||
| T-Status * | T1-T2 | - | 18 | - | - | - | |||||
| T3-T4 | 2 | - | - | ||||||||
| n.d. | 1 | 8 | - | - | |||||||
| N-Status * | N0 | - | 10 | 18 | - | - | - | ||||
| N+ | 11 | 4 | - | - | |||||||
| UK | - | 23 | - | - | |||||||
| Inflammation | N-IF | 2 | 6 | 10 | 11 | 0 | 0 | 9 | 9 | - | - |
| M-IF | 5 | 17 | 24 | 25 | 2 | 7 | 11 | 11 | - | - | |
| Mo-IF | 7 | 16 | 13 | 13 | 14 | 31 | 0 | 0 | - | - | |
| S-IF | 3 | 5 | 3 | 3 | 5 | 7 | 0 | 0 | - | - | |
| n.d. | 2 | 1 | - | - | |||||||
| Clinical Stage * | Early | - | 17 | 30 | - | - | - | ||||
| Late | 3 | 8 | - | - | |||||||
| n.d. | 1 | 7 | - | - | |||||||
| Group | PD1 (ΔLI) | PD-L1 (ΔLI) | PD-L1 (∆CT) | |||
|---|---|---|---|---|---|---|
| Epithelial | Subepithelial | Epithelial | Subepithelial | Whole Tissue | ||
| T-OLP | Mean | 1.32 | 1.01 | 6.07 | 1.27 | 4.86 |
| SD | 1.58 | 1.46 | 15.58 | 1.91 | 4.67 | |
| N | 17 | 17 | 46 | 46 | 32 | |
| N-OLP | Mean | 0.3 | 0.26 | 0.62 | 0.69 | 6.47 |
| SD | 0.52 | 0.49 | 2.81 | 0.92 | 5.29 | |
| N | 50 | 50 | 53 | 53 | 50 | |
| OSCC | Mean | 0.37 | 0.25 | 10.38 | 0.47 | 5.76 |
| SD | 0.8 | 0.38 | 19.63 | 0.67 | 4.4 | |
| N | 21 | 21 | 45 | 45 | 38 | |
| NOM | Mean | 1 | 0.66 | 0.1 | 1.59 | 8.37 |
| SD | 1.21 | 1.1 | 0.42 | 1.73 | 5.32 | |
| N | 20 | 20 | 20 | 20 | 24 | |
| vs. NOM | p-Value MWU | FC Up/Down | AUC | p-Value (χ2) |
|---|---|---|---|---|
| RT qPCR (PD-L1) | ||||
| T-OLP | 0.0001 | 11.4 | 0.70 | 0.0001 |
| N-OLP | 0.001 | 3.8 | 0.65 | 0.01 |
| OSCC | 0.0001 | 8.9 | 0.77 | 0.0001 |
| IHC (PD-L1 epithelial) | ||||
| T-OLP | 0.04 | 60.14 | 0.617 | 0.03 |
| N-OLP | 0.703 | 6.27 | n.d | n.d |
| OSCC | 0.002 | 99.41 | 0.703 | 0.003 |
| IHC (PD-L1 subepithelial) | ||||
| T-OLP | 0.19 | 0.8/−1.3 | n.d | n.d |
| N-OLP | 0.014 | 0.44/−2.3 | 0.295 | n.d. |
| OSCC | 0.002 | 0.29/−3.4 | 0.233 | n.d. |
| IHC (PD-1 epithelial) | ||||
| T-OLP | 0.729 | 1.27 | n.d | n.d |
| N-OLP | 0.0001 | 0.29/−3.5 | 0.203 | n.d. |
| OSCC | 0.002 | 0.36/−2.8 | 0.194 | n.d. |
| IHC (PD-1 subepithelial) | ||||
| T-OLP | 0.55 | 1.52 | n.d | n.d |
| N-OLP | 0.014 | 0.40/−2.6 | 0.309 | n.d. |
| OSCC | 0.074 | 0.37/−2.8 | n.d | n.d |
| Target | p-Value MWU | FC | AUC | Sensitivity | Specificity | COP | p-Value (χ2) |
|---|---|---|---|---|---|---|---|
| T-OLP vs. N-OLP | |||||||
| PD-1_E (IHC) | 0.001 | 4.41 | 0.75 | 76.5 | 72.3 | 0.34 | 0.0001 |
| PD-1_S (IHC) | 0.005 | 3.83 | 0.78 | 76.5 | 66 | 0.18 | 0.002 |
| PD-L1 (qPCR) | 0.128 | 3.05 | n.d. | n.d. | n.d. | n.d. | n.d. |
| PD-L1_E (IHC) | 0.006 | 9.73 | 0.72 | 50.0 | 93.6 | 0.16 | 0.006 |
| PD-L1_S (IHC) | 0.25 | 1.83 | n.d. | n.d. | n.d. | n.d. | n.d. |
| DFS of Patients in Weeks (Mean 77.2) | |||
|---|---|---|---|
| Checkpoint | Expression | Range | Mean DFS |
| PD-L1-PCR | |||
| * COP = 5.027 | + | 1–284 | 52 |
| − | 3–221 | 92 | |
| PD-1_E | |||
| ** COP = 0.34 | + | 1–284 | 51.3 |
| − | 3–233 | 82.3 | |
| PD-1_S | |||
| ** COP = 0.18 | + | 3–284 | 61.1 |
| − | 1–233 | 54 | |
| PD-L1_E | |||
| ** COP = 0.16 | + | 1–121 | 39.1 |
| − | 1–317 | 86.3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ries, J.; Agaimy, A.; Wehrhan, F.; Baran, C.; Bolze, S.; Danzer, E.; Frey, S.; Jantsch, J.; Möst, T.; Büttner-Herold, M.; et al. Importance of the PD-1/PD-L1 Axis for Malignant Transformation and Risk Assessment of Oral Leukoplakia. Biomedicines 2021, 9, 194. https://doi.org/10.3390/biomedicines9020194
Ries J, Agaimy A, Wehrhan F, Baran C, Bolze S, Danzer E, Frey S, Jantsch J, Möst T, Büttner-Herold M, et al. Importance of the PD-1/PD-L1 Axis for Malignant Transformation and Risk Assessment of Oral Leukoplakia. Biomedicines. 2021; 9(2):194. https://doi.org/10.3390/biomedicines9020194
Chicago/Turabian StyleRies, Jutta, Abbas Agaimy, Falk Wehrhan, Christoph Baran, Stella Bolze, Eva Danzer, Silke Frey, Jonathan Jantsch, Tobias Möst, Maike Büttner-Herold, and et al. 2021. "Importance of the PD-1/PD-L1 Axis for Malignant Transformation and Risk Assessment of Oral Leukoplakia" Biomedicines 9, no. 2: 194. https://doi.org/10.3390/biomedicines9020194