When Less Is More: Specific Capture and Analysis of Tumor Exosomes in Plasma Increases the Sensitivity of Liquid Biopsy for Comprehensive Detection of Multiple Androgen Receptor Phenotypes in Advanced Prostate Cancer Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Classification
2.2. Plasma Collection and Nucleic Acid Isolation
2.3. Digital PCR (dPCR) Analysis of Relevant Targets
2.4. Statistical Analysis
3. Results
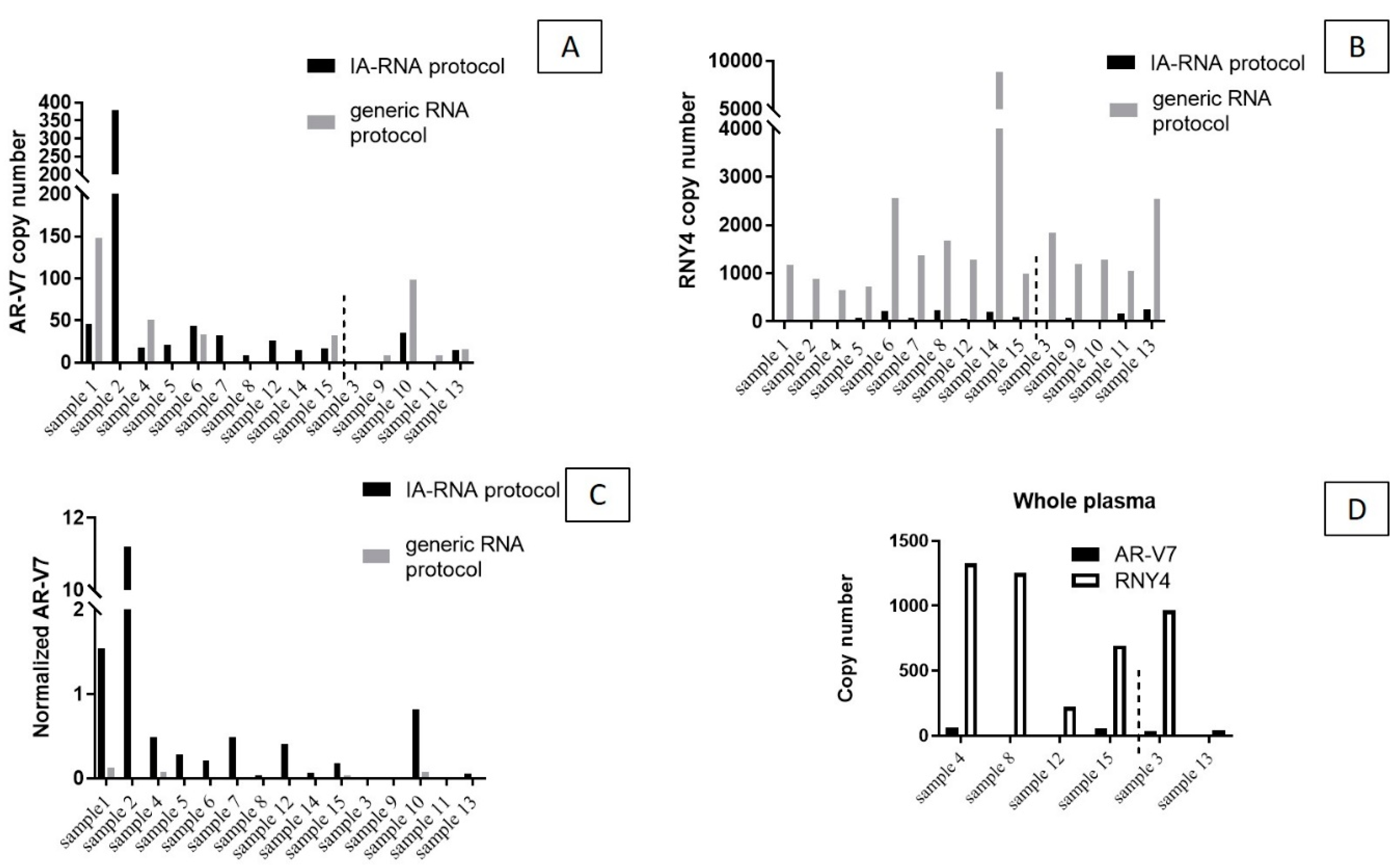
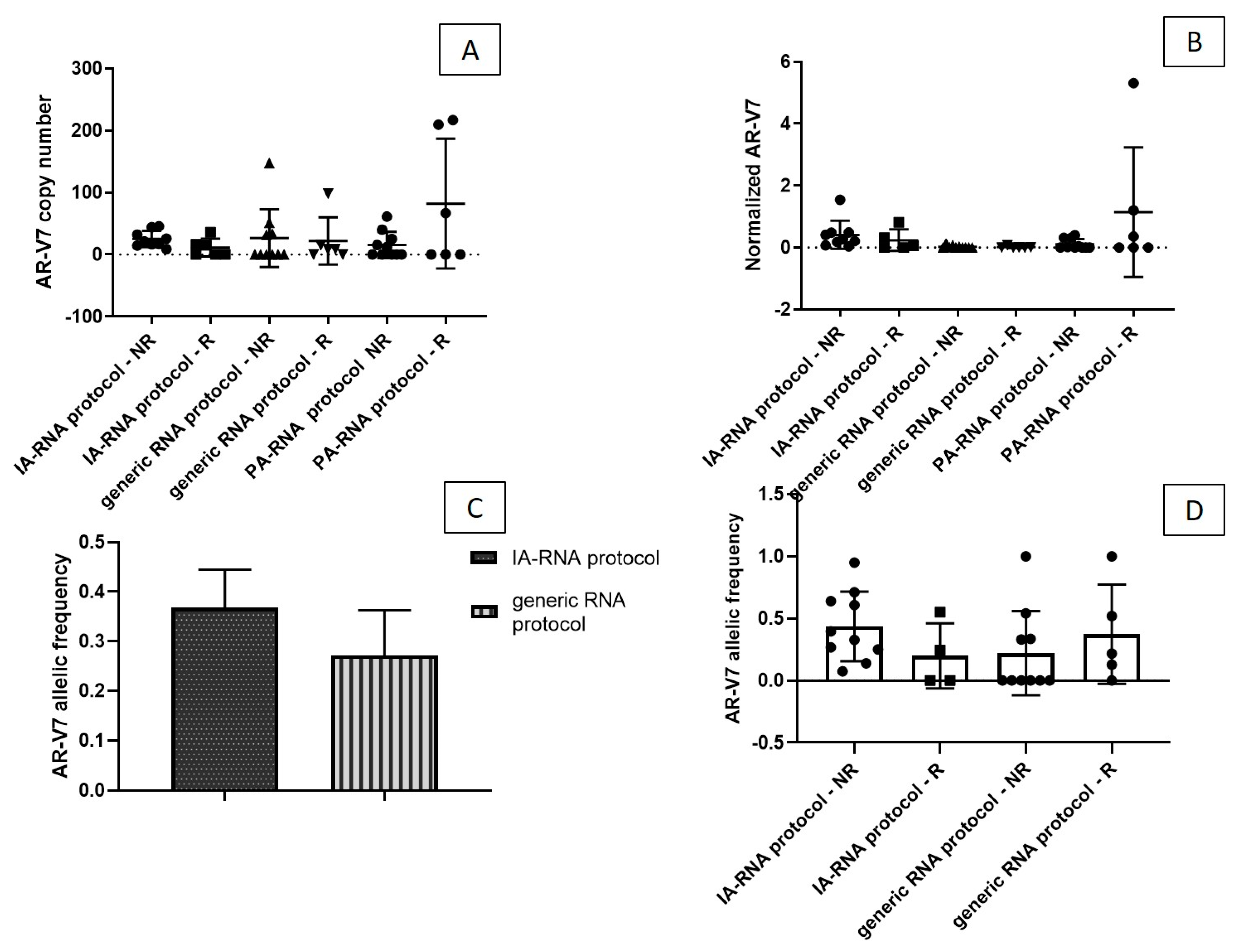
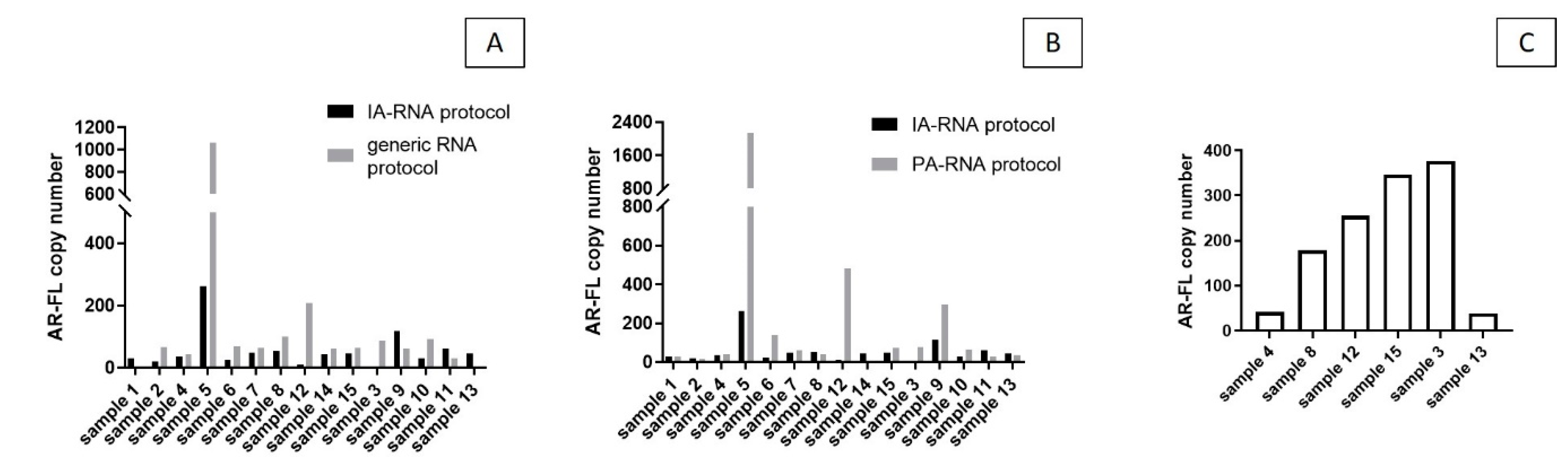
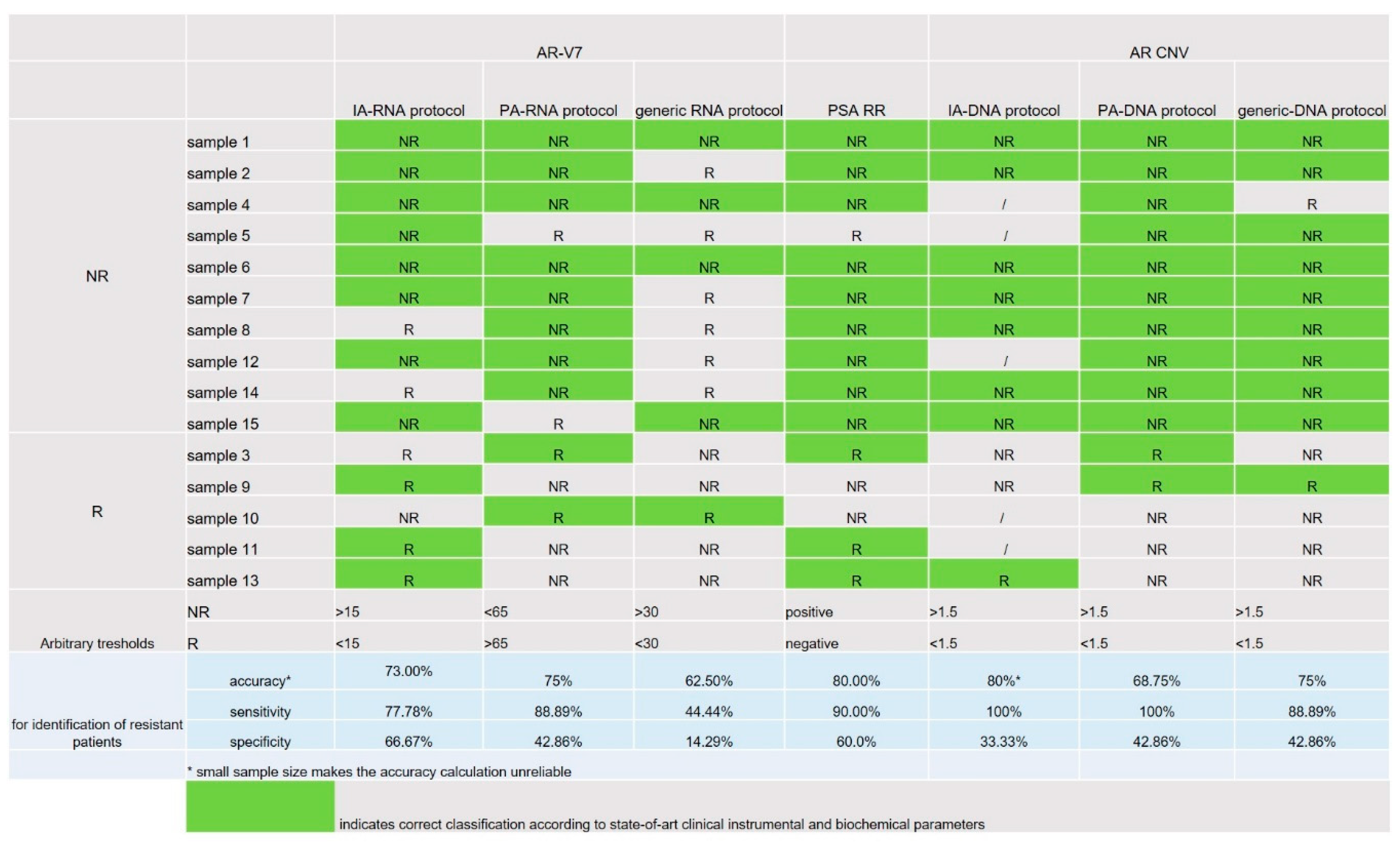
3.1. RNA Target—AR-V7
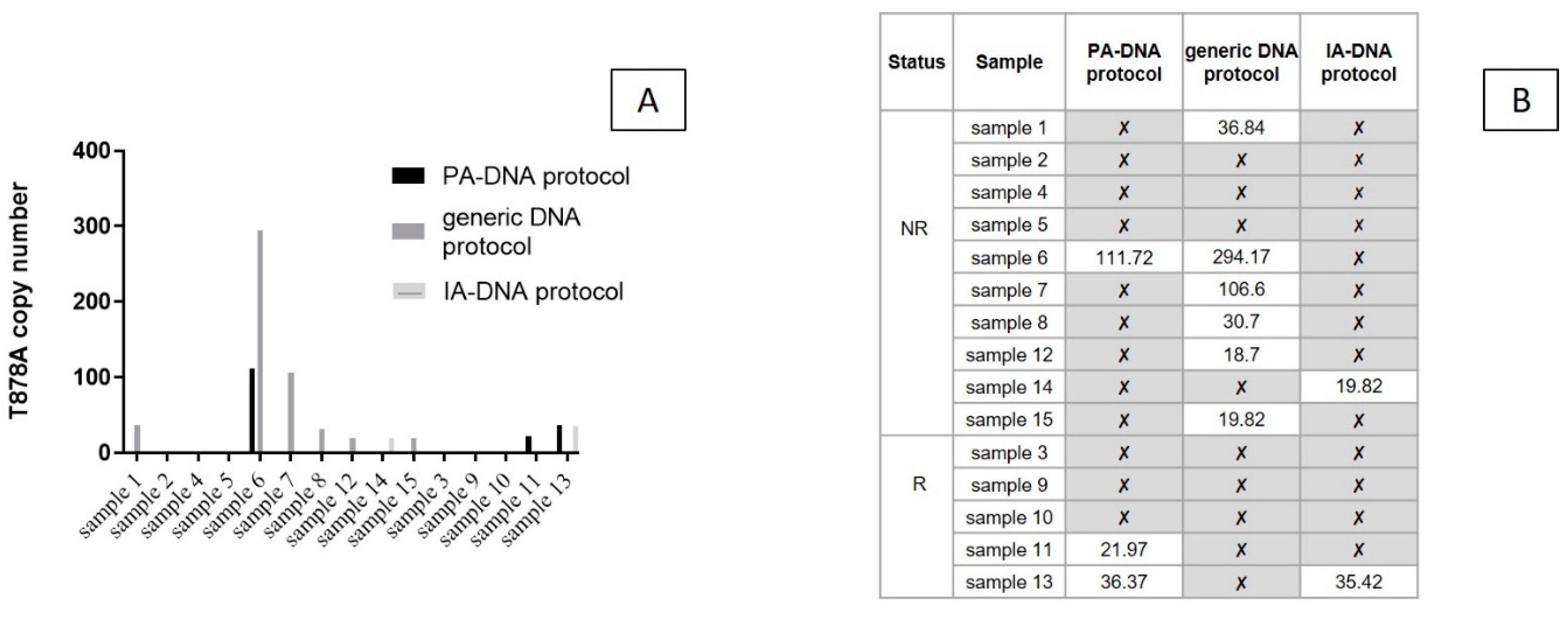
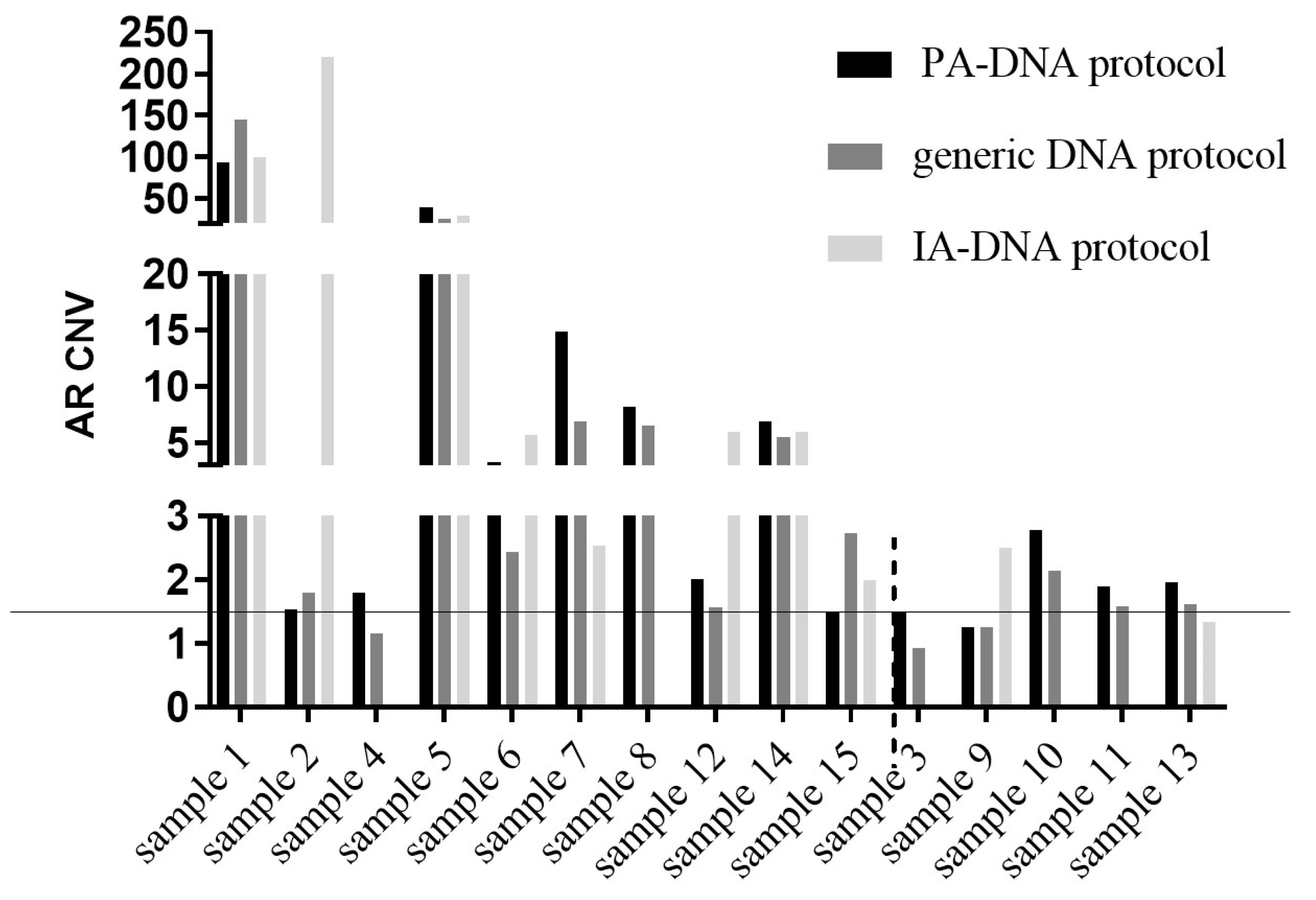
3.2. DNA Targets—AR T878A and AR Amplification
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vandekerkhove, G.; Struss, W.J.; Annala, M.; Kallio, H.M.L.; Khalaf, D.; Warner, E.W.; Herberts, C.; Ritch, E.; Beja, K.; Loktionova, Y.; et al. Circulating Tumor DNA Abundance and Potential Utility in De Novo Metastatic Prostate Cancer. Eur. Urol. 2019, 75, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Coleman, I.; Morrissey, C.; Zhang, X.; True, L.D.; Gulati, R.; Etzioni, R.; Bolouti, H.; Montgomery, B.; White, T.; et al. Substantial interindividual and limited intraindividual genomic diversity among tumors from men with metastatic prostate cancer. Nat. Med. 2016, 22, 369–378. [Google Scholar] [CrossRef]
- Jernberg, E.; Bergh, A.; Wikström, P. Clinical relevance of androgen receptor alterations in prostate cancer. Endocr. Connect. 2017, 6, R146–R161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, S.C.; Li, Y.; Dehm, S.M. Androgen receptor splice variants activate androgen receptor target genes andsupport aberrant prostate cancer cell growth independent of canonical androgen receptor nuclear localization signal. J. Biol. Chem. 2012, 287, 19736–19749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schweizer, M.T.; Yu, E.Y. AR-Signaling in Human Malignancies: Prostate Cancer and Beyond. Cancers 2017, 11, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kustanovich, A.; Schwartz, R.; Peretz, T.; Grinshpun, A. Life and death of circulating cell-free DNA. Cancer Biol. Ther. 2019, 20, 1057–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, E.K.; Tsui, N.B.; Lam, N.Y.; Chiu, R.W.; Yu, S.C.; Wong, S.C.; Lo, E.S.; Rainer, T.H.; Johnson, P.J.; Lo, Y.M. Presence of filterable and nonfilterable mRNA in the plasma of cancer patients and healthy individuals. Clin. Chem. 2002, 48, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Suraj, S.; Dhar, C.; Srivastava, S. Circulating nucleic acids: An analysis of their occurrence in malignancies. Biomed. Rep. 2017, 6, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhe, X.; Cher, M.L.; Bonfil, R.D. Circulating tumor cells: Finding the needle in the haystack. Am. J. Cancer Res. 2011, 1, 740–751. [Google Scholar] [PubMed]
- Di Meo, A.; Bartlett, J.; Cheng, Y.; Pasic, M.D.; Yousef, G.M. Liquid biopsy: A step forward towards precision medicine in urologic malignancies. Mol. Cancer 2017, 14, 80. [Google Scholar] [CrossRef] [PubMed]
- Del Re, M.; Crucitta, S.; Sbrana, A.; Rofi, E.; Paolieri, F.; Gianfilippo, G.; Galli, L.; Falcone, A.; Morganti, R.; Porta, C.; et al. AR-V7 and AR-FL expression is associated with clinical outcome: A translational study in patients with castrate resistant prostate cancer. BJU Int. 2019, 4. [Google Scholar] [CrossRef]
- Bernardi, S.; Foroni, C.; Zanaglio, C.; Re, F.; Polverelli, N.; Turra, A.; Morello, E.; Farina, M.; Cattina, F.; Gandolfi, L.; et al. Feasibility of tumor-derived exosome enrichment in the onco-hematology leukemic model of chronic myeloid leukemia. Int. J. Mol. Med. 2019, 44, 2133–2144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bathini, S.; Raju, D.; Badilescu, S.; Kumar, A.; Ouellette, R.J.; Ghosh, A.; Packirisamy, M. Nano–Bio Interactions of Extracellular Vesicles with Gold Nanoislands for Early Cancer Diagnosis. Research 2018, 2018, 3917986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonarakis, E.S.; Lu, C.; Wang, H.; Luber, B.; Nakazawa, M.; Roeser, J.C.; Chen, Y.; Nadal, R.; Chen, Y.; Fedor, H.L.; et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N. Engl. J. Med. 2014, 37, 1028–1038. [Google Scholar] [CrossRef] [Green Version]
- Driedonks, T.A.P.; Nolte-’t Hoen, E.N.M. Circulating Y-RNAs in Extracellular Vesicles and Ribonucleoprotein Complexes; Implications for the Immune System. Front. Immunol. 2019, 9, 3164–3178. [Google Scholar] [CrossRef]
- Salvi, S.; Casadio, V.; Conteduca, V.; Burgio, S.L.; Menna, C.; Bianchi, E.; Rossi, L.; Carretta, E.; Rossi, L.; Masini, C.; et al. Circulating cell-free AR and CYP17A1 copy number variations may associate with outcome of metastatic castration-resistant prostate cancer patients treated with abiraterone. Br. J. Cancer 2015, 112, 1717–1724. [Google Scholar] [CrossRef]
- Zhang, G.; Liu, X.; Li, J.; Ledet, E.; Alvarez, X.; Qi, Y.; Fu, X.; Sartor, O.; Dong, Y.; Zhang, H. Androgen receptor splice variants circumvent AR blockade by microtubule-targeting agents. Oncotarget 2015, 6, 23358–23371. [Google Scholar] [CrossRef] [Green Version]
- Francini, E.; Petrioli, R.; Rossi, G.; Laera, L.; Roviello, G. PSA response rate as a surrogatemarker for median overall survival in docetaxel-based first-line treatments for patients with metastatic castration-resistant prostate cancer: An analysis of 22 trials. Tumour Biol. 2014, 35, 10601–10607. [Google Scholar] [CrossRef]
- Facchini, G.; Caffo, O.; Ortega, C.; D’Aniello, C.; Di Napoli, M.; Cecere, M.; Cecere, S.C.; Della Pepa, C.; Crispo, A.; Maines, F.; et al. Very Early PSA Response to Abiraterone in mCRPC Patients: A Novel Prognostic Factor Predicting Overall Survival. Front. Pharmacol. 2016, 7, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Del Re, M.; Biasco, E.; Crucitta, S.; Derosa, L.; Rofi, E.; Orlandini, C.; Miccoli, M.; Galli, L.; Falcone, A.; Jenster, G.W.; et al. The Detection of Androgen Receptor Splice Variant 7 in Plasma-derived Exosomal RNA Strongly Predicts Resistance to Hormonal Therapy in Metastatic Prostate Cancer Patients. Eur. Urol. 2017, 71, 680–687. [Google Scholar] [CrossRef]
- Antonarakis, E.S.; Lu, C.; Luber, B.; Wang, H.; Chen, Y.; Zhu, Y.; Silberstein, J.L.; Taylor, M.N.; Maughan, B.L.; Denmeade, S.R.; et al. Clinical Significance of Androgen Receptor Splice Variant-7 mRNA Detection in Circulating Tumor Cells of Men With Metastatic Castration-Resistant Prostate Cancer Treated With First- and Second-Line Abiraterone and Enzalutamide. J. Clin. Oncol. 2017, 35, 2149–2156. [Google Scholar] [CrossRef]
- Takeuchi, T.; Okuno, Y.; Hattori-Kato, M.; Zaitsu, M.; Mikami, K. Detection of AR-V7 mRNA in whole blood may not predict the effectiveness of novel endocrine drugs for castration-resistant prostate cancer. Res. Rep. Urol. 2016, 8, 21–25. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.M.; Abdelmohsen, K.; Mustapic, M.; Kapogiannis, D.; Gorospe, M. RNA in extracellular vesicles. Wiley Interdiscip. Rev. RNA 2017, 8. [Google Scholar] [CrossRef]
- Wyatt, A.W.; Annala, M.; Aggarwal, R.; Beja, K.; Feng, F.; Youngren, J.; Foye, A.; Lloyd, P.; Nykter, M.; Beer, T.M.; et al. Concordance of Circulating Tumor DNA and Matched Metastatic Tissue Biopsy in Prostate Cancer. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [Green Version]
- Veldscholte, J.; Ris-Stalpers, C.; Kuiper, G.G.; Jenster, G.; Berrevoets, C.; Claassen, E.; van Rooij, H.C.; Trapman, J.; Brinkmann, A.O.; Mulder, E. A mutation in the ligand binding domain of the androgen receptor of human LNCaP cells affects steroid binding characteristics and response to anti-androgens. Biochem. Biophys. Res. Commun. 1990, 173, 534–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathkopf, D.E.; Smith, M.R.; Ryan, C.J.; Berry, W.R.; Shore, N.D.; Liu, G.; Higano, C.S.; Alumkal, J.J.; Hauke, R.; Tutrone, R.F.; et al. Androgen receptor mutations in patients with castration-resistant prostate cancer treated with apalutamide. Ann. Oncol. 2017, 28, 2264–2271. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, A.W.; Azad, A.A.; Volik, S.V.; Annala, M.; Beja, K.; McConeghy, B.; Haegert, A.; Warner, E.W.; Mo, F.; Brahmbhatt, S.; et al. Genomic Alterations in Cell-Free DNA and Enzalutamide Resistance in Castration-Resistant Prostate Cancer. JAMA Oncol. 2016, 2, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Steinestel, J.; Luedeke, M.; Arndt, A.; Schnoeller, T.J.; Lennerz, J.K.; Wurm, C.; Maier, C.; Cronauer, M.V.; Steinestek, K.; Schrader, A.J. Detecting predictive androgen receptor modifications in circulating prostate cancer cells. Oncotarget 2015, 10, 4213–4223. [Google Scholar] [CrossRef] [Green Version]
- Grasso, C.S.; Wu, Y.M.; Robinson, D.R.; Cao, X.; Dhanasekaran, S.M.; Khan, A.P.; Quist, M.J.; Jing, X.; Lonigro, R.J.; Brenner, J.C.; et al. The mutational landscape of lethal castration-resistant prostate cancer. Nature 2012, 487, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Cancer Genome Atlas Research Network. The Molecular Taxonomy of Primary Prostate Cancer. Cell 2015, 163, 1011–1025. [Google Scholar] [CrossRef]
- Beltran, H.; Prandi, D.; Mosquera, J.M.; Benelli, M.; Puca, L.; Cyrta, J.; Marotz, C.; Giannopoulou, E.; Chakravarthi, B.V.; Varambally, S.; et al. Divergent clonal evolution of castration-resistant neuroendocrine prostate cancer. Nat. Med. 2016, 22, 298–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annala, M.; Vandekerkhove, G.; Khalaf, D.; Taavitsainen, S.; Beja, K.; Warner, E.W.; Sunderland, K.; Kollmannsberger, C.; Eigl, B.J.; Finch, D.; et al. Circulating Tumor DNA Genomics Correlate with Resistance to Abiraterone and Enzalutamide in Prostate Cancer. Cancer Discov. 2018, 8, 444–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, Y.; Dehm, S.M. Androgen Receptor Rearrangement and Splicing Variants in Resistance to Endocrine Therapies in Prostate Cancer. Endocrinology 2017, 158, 1533–1542. [Google Scholar] [CrossRef] [PubMed]
- Hodara, E.; Morrison, G.; Cunha, A.; Zainfeld, D.; Xu, T.; Xu, Y.; Dempsey, P.W.; Pagano, P.C.; Bischoff, F.; Khurana, A. Multiparametric liquid biopsy analysis in metastatic prostate cancer. JCI Insight. 2019, 4. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Code | R/NR | Diagnosis Date | Previous Therapies | Therapy during Withdrawal | Observations | PSA before/after Treatment [ng/mL] |
|---|---|---|---|---|---|---|
| sample 1 | NR | 2012 | Bicalutamide + LHRH analog, Docetaxel + LHRH analog | Abiraterone | metastasis and biochemical progression after abiraterone treatment | 177/317 |
| sample 2 | NR | 2011 | Bicalutamide, LHRH analog | Abiraterone | several metastatic loci after abiraterone treatment | 546/812 |
| sample 3 | R | 2011 | Bicalutamide, LHRH analog, abiraterone | Docetaxel | steadiness of the disease | 812/658 |
| sample 4 | NR | 2001 | Bicalutamide, LHRH analog | Abiraterone | weak instrumental progression after abiraterone treatment | 4/151 |
| sample 5 | NR | 1999 | Bicalutamide + LHRH analog, Flutamide + LHRH analog, Zoledronic acid, Docetaxel, Enzalutamide + LHRH analog | Abiraterone | apparent steadiness of illness, but the patient reported a worsening of pain | 160/143 |
| sample 6 | NR | 2003 | Bicalutamide + LHRH analog, Abiraterone, Docetaxel + LHRH analog, | Cabaxitaxel | illness progression after cabaxitaxel treatment | 42/69 |
| sample 7 | NR | 2009 | Bicalutamide, LHRH analog, Zoledronic acid, Abiraterone, Docetaxel | Enzalutamide | metastasis and biochemical progression after enzalutamide treatment | 38/86 |
| sample 8 | NR | 2004 | Bicalutamide, LHRH analog | Abiraterone | instrumental progression after abiraterone treatment | 9.3/61.38 |
| sample 9 | R | 2006 | Bicalutamide, Bicalutamide + LHRH analog, LHRH analog, Abiraterone, Docetaxel | Enzalutamide | initial biochemical and instrumental response to enzalutamide | 58/125.15 |
| sample 10 | R | 2008 | Bicalutamide + LHRH analog, Zoledronic acid, Bicalutamide, Estramustine | Abiraterone | steadiness of the disease, despite the increase in PSA | 7,59/18 |
| sample 11 | R | 2010 | Bicalutamide, LHRH analog, Cyproterone acetate, Abiraterone, Docetaxel, Cabazitaxel | Enzalutamide | initial biochemical response to enzalutamide | 266/236 |
| sample 12 | NR | 2010 | Bicalutamide, LHRH analog, Cyproterone acetate, Abiraterone, Docetaxel, Cabazitaxel | Enzalutamide | instrumental and biochemical progression after abiraterone treatment | 266/554 |
| sample 13 | R | 2003 | Bicalutamide + LHRH analog, Bicalutamide, Cyproterone acetate, | Enzalutamide | biochemical and instrumental steadiness of the disease | 27/0.81 |
| sample 14 | NR | 2011 | LHRH analog, Bicalutamide, Enzalutamide, Docetaxel, | Radiometabolic therapy + LHRH analog | instrumental progression during treatment | 82/171 |
| sample 15 | NR | 2015 | bicalutamide + LHRH analog, radiotherapy | LHRH analog | instrumental and biochemical progression during treatment | 0.04/26 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foroni, C.; Zarovni, N.; Bianciardi, L.; Bernardi, S.; Triggiani, L.; Zocco, D.; Venturella, M.; Chiesi, A.; Valcamonico, F.; Berruti, A. When Less Is More: Specific Capture and Analysis of Tumor Exosomes in Plasma Increases the Sensitivity of Liquid Biopsy for Comprehensive Detection of Multiple Androgen Receptor Phenotypes in Advanced Prostate Cancer Patients. Biomedicines 2020, 8, 131. https://doi.org/10.3390/biomedicines8050131
Foroni C, Zarovni N, Bianciardi L, Bernardi S, Triggiani L, Zocco D, Venturella M, Chiesi A, Valcamonico F, Berruti A. When Less Is More: Specific Capture and Analysis of Tumor Exosomes in Plasma Increases the Sensitivity of Liquid Biopsy for Comprehensive Detection of Multiple Androgen Receptor Phenotypes in Advanced Prostate Cancer Patients. Biomedicines. 2020; 8(5):131. https://doi.org/10.3390/biomedicines8050131
Chicago/Turabian StyleForoni, Chiara, Natasa Zarovni, Laura Bianciardi, Simona Bernardi, Luca Triggiani, Davide Zocco, Marta Venturella, Antonio Chiesi, Francesca Valcamonico, and Alfredo Berruti. 2020. "When Less Is More: Specific Capture and Analysis of Tumor Exosomes in Plasma Increases the Sensitivity of Liquid Biopsy for Comprehensive Detection of Multiple Androgen Receptor Phenotypes in Advanced Prostate Cancer Patients" Biomedicines 8, no. 5: 131. https://doi.org/10.3390/biomedicines8050131